Chapter 28, Part 1 Cardiology. Cardiac Physiology. Cardiovascular Anatomy
|
|
|
- Deborah Casey
- 6 years ago
- Views:
Transcription


1 Chapter 28, Part 1 Cardiology Part 1: Cardiovascular Anatomy & Physiology, ECG Monitoring, and Dysrhythmia Analysis 1 2 Cardiovascular Anatomy Coronary Circulation Cardiac Physiology The cardiac cycle consists of and Systole Diastole: Relaxation phase Systole: phase fraction: during each contraction, the ventricles eject about 2/3 of the blood it contains 3 4

2 Cardiac Physiology Cardiac Physiology Volume: amount ejected (70mL average) Stroke volume depends on: Preload Cardiac 5 6 Cardiac Physiology Cardiac Output = stroke volume X heart Heart function is regulated by the and parasympathetic nervous systems of the autonomic nervous system Each system secretes Sympathetic Nervous System Has 2 types of receptor fibers at the nerve endings: Alpha and Beta The chemical neurotransmitter of the SNS is These nerve endings are called 7 8
3 Terms Chronotropy: heart rate : contractile strength Dromotropy: rate of nervous conduction Cardiac Cell Groups Two types: Myocardial cells: responsible for generating the physical contraction of the heart muscle Specialized cells Coordinates rate and rhythm within the conduction system Do not contract 9 10 Cardiac Physiology Properties of the Cardiac Conductive System : Cells are capable of responding to electrical stimulus : Cells can transmit electrical impulses from cell to cell : Each cell can depolarize without any outside impulse : Cells have the ability to expand Cardiac Cell Characteristics Characteristic Cardiac Cells Function Excitability Pacemaker Cells Electrical Conductivity All Cells Electrical Conductivity All Cells Electrical Contractility Working Cells Mechanical 11 12
4 Pacemaker Cells Cardiac Physiology Cardiac Electrolytes: (Na+): depolarization Calcium (Ca++): depolarization and contractions (K+): repolarization Chloride (Cl-): Unsure (Mg++): Unsure Cardiac Depolarization Resting Potential ( ) : The normal electrical state of cardiac cells. Negatively charged Action Potential: The stimulation of myocardial cells, as evidenced by a change in the membrane electrical charge, that spreads across the myocardium Cardiac : a reversal of charges at a cell membrane so that the inside of the cell becomes positive in relation to the outside. Positively charged Cardiac Depolarization 15 16

5 Cardiac Physiology Cardiac Conductive System Components: Node Internodal Atrial Pathways Atrioventricular Node Atrioventricular Bundle of Left and Right Bundle Branches Fibers Cardiac Physiology Intrinsic Firing Rates of the Cardiac Conductive System SA Node: - bpm AV Node: - bpm Purkinje System: - bpm Electrocardiographic Monitoring The Electrocardiogram Positive and Negative Impulses Muscle tremors Shivering Patient Loose electrodes Hertz interference Machine malfunction 19 20
")
 avr, avl, avf V1 V6 Bipolar Lead")

6 Muscle Tremor Artifact 60 Cycle Interference The Electrocardiogram ECG Leads (Limb) Einthoven s Triangle Leads I, II, III - (Unipolar) avr, avl, avf V1 V6 Bipolar Lead Placement Sites Lead Positive Negative I Left Arm Right Arm II Left Leg Right Arm III Left Leg Left Arm 23 24



7 The Electrocardiogram (Page 1141) Lead Systems and Heart Surfaces The Electrocardiogram Routine Monitoring Information from a single lead shows: Rate &. to conduct an impulse The Electrocardiogram A single lead cannot: Identify/locate an. Identify deviation or chamber enlargement. Identify right-to-left differences in conduction. The quality or presence of action. 27 The Electrocardiogram ECG Paper Speed: mm/sec is normal Amplitude and Deflection: large boxes = 1 millivolt Each small square = seconds Each larger square = seconds 28
 29 30 The Electrocardiogram The Electrocardiogram")
8 The Electrocardiogram ECG Components: Wave Complex Wave Wave (rare) Isoelectric line: line with electrical activity The Electrocardiogram (flat) The Electrocardiogram The Electrocardiogram 31 32

9 The Electrocardiogram The Electrocardiogram The Electrocardiogram The Electrocardiogram 35 36

10 Normal Time Intervals P R Interval (PRI) or P Q Interval (PQI) Seconds QRS Interval Seconds S T Segment Q T Interval Seconds Refractory Periods : Heart CAN beat again but without adequate pumping action : Heart CANNOT pump again S-T Segment Changes Elevation or depression of the S-T segment above or below the line Associated with Myocardial Infarctions Injury Interpretation of Rhythm Strips Always be and analytical. Memorize the rules for each dysrhythmia. Analyze a given rhythm strip according to a specific. Compare your analysis to the rules for each dysrhythmia. Identify the dysrhythmia by its similarity to established rules
11 Five-Step Procedure Five-Step Procedure 1. Analyze the (QRS). Over 100 = tachycardia Less than 60 = bradycardia 2. Analyze the. Regular or irregular? If irregular is it regularly irregular or irregularly irregular? ( ) 3. Analyze the -waves. Present? or inverted? 4. Analyze the interval to 0.20 is normal 5. Analyze the complex. Broad or narrow? Analyzing the Rate 6 seconds method Count the number of complexes in a 6 second interval ( large squares) and multiply by 10 Heart Rate Calculator Commercially available rulers Analyzing the Rate R-R Interval Only if heart rate is Measure duration between R waves in seconds and divide into Example: seconds = 92 bpm Count the number of large squares within the R-R interval and divide into Example: boxes = 86 bpm Count the number of small squares within the R-R interval and divide into 43 44
12 Analyzing the Rate Triplicate Method Used only with rhythms Locate an R wave that falls on a dark line bordering a large box. Then assign numbers corresponding with to the heart rate to the next dark lines to the right. The order is 300, 150, 100, 75, 60, and 50. The number that corresponds to the dark line closest to the of the next R wave is a rough estimate of the heart rate What is the Rate? Beats Per Minute small boxes between R waves 1500 divided by = What is the Rate? Analyzing the Rhythm? Irregular? Irregular? Irregular? Beats Per Minute small boxes between R waves divided by = 47 48
13 Is This Rhythm Regular? Is This Rhythm Regular? Analyzing the P Wave Analyze the P Waves Reflects depolarization Are P waves present? Are the P wave? Is there P wave per QRS complex? Are the P waves upright or? Do all P waves look alike? Present,, 1 per QRS, upright, all look 51 52
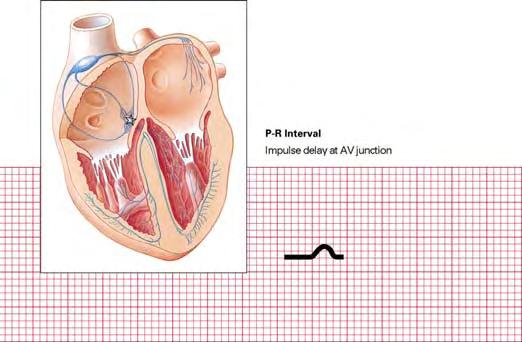
14 Analyze the P Waves Analyze the P Waves Present, regular, than 1 P wave for some QRS complexes,, all look alike Analyze the P Waves but not clear Analyzing the P-R Interval Time needed for atrial depolarization and conduction of the impulse to the AV node Normal is to seconds (3-5 small boxes) Measured from beginning of wave to beginning of wave Any deviation is abnormal 55 56
15 Analyze the P-R Interval Analyze the P-R Interval seconds Varies: to seconds Analyzing the QRS Complexes What is the QRS Duration? Do all the QRS complexes look alike? What is the QRS Normal duration is to seconds (narrow complexes) Anything longer than seconds is abnormal (broad complexes) seconds 59 60
16 What is the QRS Duration? Narrow Complexes: seconds Wide Complexes: seconds Normal Sinus Rhythm Rate: bpm Rhythm: P waves: normal,, only before each QRS complex PR Interval: - seconds QRS Complex: normal, duration of < seconds Normal Sinus Rhythm Rate: bpm Rhythm: Regular P Waves: normal, upright, only before each QRS complex P-R Interval: seconds QRS Duration: seconds Dysrhythmias 63 64
17 Dysrhythmias Dysrhythmia: any deviation from electrical rhythm : Absence of cardiac electrical activity Often used interchangeably with dysrhythmia Dysrhythmias Mechanism of Impulse Formation Foci Caused by increased automaticity When heart cells other than the pacemaker cells automatically Produces (abnormal) Beats Premature Ventricular contractions ( ) or premature atrial contractions ( ) Dysrhythmias Caused when disease or ischemia alters 2 branches of a pathway, slowing conduction in 1 branch and causing a unidirectional block in the other May be isolated beats or tachydysrhythmias Atrial fibrillation ( ) Paroxysmal supraventricular tachycardia ( ) Causes of Dysrhythmias Myocardial Ischemia, Necrosis, or Autonomic Nervous System Imbalance Distention of the Chambers of the Heart Blood Abnormalities Imbalances Trauma to the Myocardium 67 68
18 Causes of Dysrhythmias Drug Effects and Drug Toxicity Hypothermia Damage Idiopathic Events Occurrences Dysrhythmias Dysrhythmias in the healthy heart are of significance Most, if not all persons, have occasional dysrhythmias TREAT THE PATIENT, NOT THE Classification of Dysrhythmias Some classification methods of dysrhythmias include: Nature of Origin: changes in automaticity versus disturbances in conduction : major versus minor : life threatening versus non-life threatening of Origin: Where dysrhythmia is occurring (Most common) 71 Classification by Site of Origin Dysrhythmias Originating in the Node Dysrhythmias Originating in the Atria Dysrhythmias Originating Within the AV Junction (AV ) Dysrhythmias Sustained in or Originating in the AV Junction Dysrhythmias Originating in the Dysrhythmias Resulting from Disorders of 72

19 Dysrhythmias Originating in the SA Node Sinus Sinus Tachycardia Sinus Sinus 73 Rules of Interpretation: Sinus Bradycardia Description: results from slowing of the SA node Rate: Less than Rhythm: Pacemaker site: SA Node P Waves: and normal PRI: QRS: Normal 74 Sinus Bradycardia Sinus Bradycardia 75 76
20 Sinus Bradycardia Etiology Increased (vagal) tone, intrinsic disease of the SA node, drug effects. May be a normal finding in healthy, wellconditioned persons. Clinical Significance May result in decreased cardiac output, hypotension,, or CNS symptoms. In healthy, well-conditioned person, may have no significance. 77 Sinus Bradycardia Treatment: Generally unnecessary unless or ventricular irritability is present. If treatment is necessary, normally treated with and first; then external pacing, or chronotropic drug infusion such as Epi drip or Dopamine drip if Atropine is ineffective 78 Atropine Sulfate (1 of 4) Extracted from the deadly nightshade jimsonweed (parasympathetic) agent of the acetylcholine receptors is the main neurotransmitter used by the PNS Atropine lowers the "rest and digest" activity of all muscles and glands regulated by the Atropine Sulfate (2 of 4) Increases firing of node, conduction through AV node, opposes vagus nerve, blocks acetylcholine receptor sites, decreases bronchiole secretions. Indications: inadequate bradyarrythmias (other than high degree blocks), organophosphate poisonings, premedication prior to in pediatrics parasympathetic nervous system 79 80
21 Atropine Sulfate (3 of 4) Contraindications include allergic,, and 2 nd or 3 rd degree heart Side Effects: Dilated pupils, headache, nausea, vomiting, vision Atropine Sulfate (4 of 4) Adult Cardiac Dosage: mg IV push (bradycardia) repeated as needed every 3-5 minutes to a max of mg total dose Pediatric Cardiac Dosage: 0.01 to 0.03mg/kg with a minimum of mg and a maximum of 0.5mg per dose and a maximum of doses Dopamine (1 of 2) AKA: Drug Class: Sympathomimetic Given only via IV Actions: Increases cardiac contractility and causes peripheral Used regularly in prehospital setting Indication: Cardiogenic shock with hypotension and bradycardia resistant to Atropine and fluids Dopamine (2 of 2) Contraindications: tachyarrhythmias, V-Fib, Hypovolemia prior to fluid resuscitation Dosage: IV drip at - mcg/kg/min to maintain BP and or heart rate Most common range is 2-10mcg/kg/min Adverse Reactions: Ectopic beats, dyspnea, hypertension, palpitations, necrosis of skin with IV Over 20mcg/kg/min will shut off blood flow to kidneys and GI tract 84

22 Epinephrine Drip AKA: Drug Class: Sympathomimetic Effects: increases cardiac rate, contractility, force, increase electrical activity of heart, increases BP IV Drip dosage is - mcg/min Epi is discussed further later Rules of Interpretation: Sinus Tachycardia Description: results from an increased rate of the node Rate: Greater than Rhythm: Regular Pacemaker Site: SA Node P-Waves: Upright and PRI: Normal QRS: Normal Sinus Tachycardia Sinus Tachycardia 87 88
23 Sinus Tachycardia Etiology Results from an increased rate of SA node discharge. Potential causes include exercise, fever, anxiety, hypovolemia, anemia, pump failure, increased tone, hypoxia, or hypothyroidism. Clinical Significance Decreased cardiac output for rates > Very rapid rates can precipitate ischemia or infarct. Sinus Tachycardia Treatment Treatment is directed at the underlying. MI, shock, fear, stress, etc No are normally given for sinus tach in the field Rules of Interpretation: Sinus Dysrhythmia Description: results from a variation of the interval Rate: - Rhythm: Pacemaker Site: SA Node P-Waves: Upright and normal PRI: Normal QRS: Normal Sinus Dysrhythmia 91 92

24 Sinus Dysrhythmia Sinus Dysrhythmia Etiology Often a normal finding, sometimes related to the respiratory cycle. May be caused by enhanced tone. Clinical Significance Normal. Occurs in almost everyone Treatment Typically, required Sinus Arrest Description: occurs when the sinus node fails to discharge, resulting in short periods of cardiac. This standstill can persist until pacemaker cells lower in the conduction system discharge ( beats) or until the sinus node resumes discharging Rules of Interpretation: Sinus Arrest Rate: Normal to Rhythm: Irregular Pacemaker Site: Node P-Waves: and normal PRI: Normal QRS: Normal 95 96

25 Sinus Arrest Sinus Arrest Sinus Arrest Etiology Occurs when the sinus node fails to discharge. May result from ischemia of the SA node, toxicity, excessive vagal tone, or degenerative fibrotic disease. Clinical Significance Frequent or prolonged episodes may decrease cardiac output and cause Prolonged episodes may result in escape rhythms. Sinus Arrest Treatment None if patient is Treat symptomatic
26 Dysrhythmias Originating in the Atria Wondering Atrial Pacemaker Multifocal Atrial Tachycardia Premature Contractions Paroxysmal Supraventricular Tachycardia Atrial Atrial Wandering Atrial Pacemaker Description: the transfer of pacemaker sites from the sinus node to other latent pacemaker sites in the atria and AV junction. Often more than one site will be present, causing variation in the R-R interval and P waves Rules of Interpretation: Wandering Atrial Pacemaker Wandering Atrial Pacemaker Rate: Usually normal (60-100) Rhythm: Slightly Pacemaker Site: varies among the SA node, atrial tissue, and the AV junction P-Waves: Variable or PRI: Varies, depending on site of impulse QRS: normal

27 Wandering Atrial Pacemaker Wandering Atrial Pacemaker 105 Etiology Variant of sinus dysrhythmia, which is a natural phenomenon in the very young or old. May also be caused by heart disease or atrial dilation. Clinical Significance None, but may be precursor to other atrial dysrhythmias. Treatment Typically, required. 106 Multifocal Atrial Tachycardia Description: usually seen in acutely ill patients. Significant disease is seen in about 60% of these patients. Certain medications used to treat lung diseases (Theophylline, ) may worsen the condition. 3 different P waves are noticed, indicating various ectopic foci. Rules of Interpretation: Multifocal Atrial Tachycardia Rate: Greater than Rhythm: Pacemaker Site: Ectopic sites in atria P-Waves: Organized, non-sinus, with at least different forms PRI: QRS: Varies depending on AV node s refractory status when impulse begins

28 Multifocal Atrial Tachycardia Multifocal Atrial Tachycardia 109 Etiology Often seen in acutely ill patients. May result from pulmonary disease, metabolic disorders, ischemic heart disease, or recent. Clinical Significance Presence of multifocal atrial tachycardia often indicates a serious underlying illness. Treatment Treat the underlying. 110 Premature Atrial Contractions Description: result from a single electrical impulse originating in the atria of the SA node, which causes a depolarization of the heart before the next expected sinus beat. Interrupts the normal Premature Atrial Contractions Creates a non-compensatory in the underlying rhythm. Pause following an ectopic beat where the SA node is and the normal cadence is interrupted


29 Rules of Interpretation: Premature Atrial Contractions Premature Atrial Contractions Rate: Depends on underlying rhythm Rhythm: Usually regular except for Pacemaker Site: Ectopic focus in the atrium P-Waves: Occurs than expected PRI: Varies depending on focus Near SA node = 0.12 or less Near AV node = 0.12 or more QRS: Usually PACs Premature Atrial Contractions Etiology Single electrical impulse originating outside the SA node. May result from use of caffeine, tobacco, or alcohol, sympathomimetic drugs, ischemic heart disease, hypoxia, or digitalis toxicity, or may be. Clinical Significance. Presence of PACs may be a precursor to other atrial dysrhythmias
30 Premature Atrial Contractions Treatment if asymptomatic. Treat symptomatic patients by administering highflow oxygen and establishing access. Paroxysmal Supraventricular Tachycardia Description: PSVT occurs when rapid atrial depolarization overrides the node. Often occurs with sudden onset, may last minutes to hours, and terminates. Can be life threatening Rules of Interpretation: PSVT Supraventricular Tachycardia Rate: - Rhythm: Pacemaker Site: In Atria, outside the SA node P-Waves: Normally in preceding T-Wave PRI: Usually normal (but normally buried) QRS: Normal

31 PSVTs Supraventricular Tachycardia Etiology: Rapid atrial depolarization overrides the node. May be precipitated by, overexertion, smoking, caffeine Supraventricular Tachycardia Clinical Significance: May be tolerated well by healthy patients for periods. Marked reduction in cardiac can precipitate angina, hypotension, or congestive heart failure. May be life threatening Treatment of SVT Treatment may include one or more of the following: Maneuvers Therapy
32 Vagal Maneuvers Vagal Maneuvers stimulate the nerve which may slow the conduction through the SA Node There are several types of vagal maneuvers: Forced expiration against a closed glottis Bearing down as if to move bowels ( Maneuver) Immersion of face in ice water ( reflex) 125 Vagal Maneuvers artery massage Contraindicated in patients with carotid (sound of turbulent blood flow) Contraindicated in patients with known cerebrovascular disease carotid artery disease 126 Adenosine (Adenocard) Pharmacological Therapy for Supraventricular Tachycardia Slows conduction through the node Contraindications: -Allergic -2 nd or 3 rd degree -Wolfe-Parkinson-White Syndrome
33 Dosage: Adenosine (Adenocard) mg rapid IVP immediately followed by fluid bolus of 10-15cc If needed, repeat dosage (after 1-2 minutes) mg rapid IVP immediately followed by fluid bolus Adverse Reactions: dizziness, facial flushing, SOB Causes a brief period of Verapimil AKA:, Calan Channel Blocker Contraindications: Allergies Shock Patients receiving beta blockers Dosage: to mg Can be repeated once in minutes at a dose of 5 to 10mg Verapimil Adverse Reactions: Dizziness Headache AV Blocks Electrical Therapy for SVTs Used for hemodynamically unstable patients Consider sedation prior if conscious and Systolic BP above (Diazepam) 5-10mg IVP (Versed) 2-5mg IVP (Lorazepam) 1-4mg SIVP
34 Electrical Therapy for SVTs Treatment Summary for SVTs Synchronized cardioversion starting at 100J or biphasic equivalent. If unsuccessful, increase as directed by medical control Normally, J, J, J, J (or biphasic equivalent) Do not if patient converts Stable Patients Maneuvers Drug Therapy Adenosine Verapimil Electrical Shock Unstable Patients Electrical Shock Synchronized cardioversion beginning at J Drug Therapy Atrial Flutter Description: results from rapid atrial reentry circuit and an node that cannot conduct all impulses through to the ventricles. The AV node may allow impulses in a 1:1 (rare), 2:1, 3:1 or 4:1 ratio or even greater resulting is a discrepancy between and rates. Rules of Interpretation: Atrial Flutter Rate: Atrial rate of -. Ventricle rate varies Rhythm: Usually regular Pacemaker Site: Atria; outside the SA node P waves: Flutter (F-waves) are present. pattern PR Interval: Usually normal QRS Complex:
. Atrial Flutter Clinical Significance Generally well tolerated.")
35 Atrial Flutter Atrial Flutter Atrial Flutter Etiology: Results when the node cannot conduct all the impulses. Impulses may be conducted in fixed or ratios. Usually associated with organic disease such as congestive heart failure (rarely seen with ). Atrial Flutter Clinical Significance Generally well tolerated. Rapid ventricular rates may compromise cardiac output and result in. May occur in conjunction with atrial
36 Treatment of Atrial Flutter Note: A-Flutter is NOT normally treated prehospital) Electrical Therapy Consider if ventricular rate > and symptomatic. Consider sedation with synchronized cardioversion starting at 100J. Treatment of Atrial Flutter Pharmacological Therapy Diltiazem (Cardizem) Verapamil, Digoxin, beta-blockers, and Quinidine. These drugs may not be commonly carried. If rate is above bpm, consider sedation and Atrial Fibrillation Description: results from multiple areas of within the atria or from multiple ectopic foci bombarding the node which cannot handle all of the incoming impulses. AV conduction is and highly variable Rules of Interpretation: Atrial Fibrillation (A-Fib) Rate: Atrial rate of -. Ventricular rate varies greatly Rhythm: irregular Pacemaker Site: numerous ectopic foci in atria (Outside the SA node) P-Waves: discernable PRI: none QRS: Normal

37 Atrial Fibrillation (A-Fib) Atrial Fibrillation (A-Fib) Atrial Fibrillation (A-Fib) Etiology Results from multiple foci; AV conduction is random and highly variable. Often associated with underlying heart disease. Clinical Significance Atria fail to contract effectively, reducing cardiac. Well tolerated with normal ventricular rates. High or low ventricular rates can result in cardiac. 147 Treatment of A-Fib Note: A-fib is not normally treated prehospital unless rate is above 150 Electrical Therapy Consider if ventricular rate > 150 and. Consider sedation and synchronized cardioversion starting at - J then 300J and 360J. 148
 AV Blocks Locations: At the Node At the Bundle of Below the Bundle of His 149 150 AV Blocks The electrical impulses are or blocked as it")
38 Treatment of A-Fib Pharmacological Therapy Diltiazem ( ) Verapamil, Digoxin, beta blockers, and Quinidine. (heparin or warfarin). Dysrhythmias Originating Within the AV Junction (AV Blocks) AV Blocks Locations: At the Node At the Bundle of Below the Bundle of His AV Blocks The electrical impulses are or blocked as it passes through the AV node Can be caused by pathology of the AV junctional tissue or by a physiological block such as with or A- Flutter Classifications of AV Blocks -Degree AV Block Type I Second-Degree AV Block Mobitz I Type II Second-Degree AV Block Mobitz II -Degree AV Block
39 First Degree AV Block Description: First degree AV block is a in conduction at the level of the AV node rather than an actual block. First degree AV block is NOT a itself, but a condition superimposed upon another rhythm. The rhythm must also be identified Rules of Interpretation: First Degree AV Block Rate: depends on underlying Rhythm: Usually Pacemaker Site: SA node or atria P-Waves: normal P-R interval: greater than seconds QRS: Usually less than seconds First Degree AV Block First Degree AV Block Interpretation Keys Every is caused by a P-wave. But, the PRI is consistently greater than 0.20 seconds and One wave for each QRS

40 First Degree AV Block First Degree AV Block 157 Etiology Delay in the conjunction of an impulse through the AV node. May occur in hearts, but often indicative of ischemia at the AV junction. Clinical Significance Usually not significant, but new onset may precede a more block. 158 First Degree AV Block Treatment Generally, none required other than. Avoid drugs that may further AV conduction. Type I Second Degree AV Block AKA: Mobitz I or Wenckebach Description: an block at the level of the AV node Produces a pattern which the intervals become progressively longer until an impulse is blocked. Cycle is repetitive and the P-P interval is Pattern may be constant or variable

41 Type I Second Degree AV Block Keys to Interpretation: PRI until a QRS drops out Each is caused by a P-Wave Rules of Interpretation: Type I Second Degree AV Block Rate: is normal, Ventricular is normal to slow Rhythm: Atrial is regular. Ventricular is irregular Pacemaker Site: node or atria P-Waves: normal. Some P-waves are NOT followed by complexes QRS: Usually less than 0.12 seconds Type I Second Degree AV Block Type I Second Degree AV Block
42 Type I Second Degree AV Block Etiology Delay increases until an impulse is. Indicative of ischemia at the AV junction. Clinical Significance Frequently dropped beats can result in compromise. Type I Second Degree AV Block Treatment Generally, none required other than observation. Avoid drugs that may further slow AV conduction. Treat symptomatic. : 0.5mg repeated as needed every - minutes up to a max of 3mg total dose External Pacing if Atropine is unsuccessful Type II Second Degree AV Block AKA: Mobitz II, or infranodal Description: an intermittent block characterized by P wave that are not conducted to the ventricles, but associated lengthening of the P-R interval before the dropped beats Type II Second Degree AV Block Keys to Interpretation: More waves than QRS but every QRS is caused by a P wave is constant for conducted beats

43 Rules of Interpretation: Type II Second Degree AV Block Type II Second Degree AV Block Rate: is normal. Ventricular is slow Rhythm: regular or Pacemaker Site: SA node or atria P-Waves: normal, some P-waves not followed by QRS PRI: constant for conducted beats, may be greater than seconds QRS: Normal or greater than 0.12 seconds Type II Second Degree AV Block 171 Type II Second Degree AV Block Etiology Intermittent block of impulses. Usually associated with or septal necrosis. Clinical Significance May compromise cardiac output and is indicative of MI. Often develops into AV blocks. 172
44 Type II Second Degree AV Block Treatment Avoid drugs that may further slow AV conduction. Treat symptomatic bradycardia. Atropine should be given May increase atrial but worsen block Consider transcutaneous pacing. 173 Third Degree AV Block AKA: Complete Heart Block Description: the absence of conduction between the atria and the ventricles resulting from complete electrical block at or below the node The pacemaker, located below the atria, paces the heart 174 Third Degree AV Block Keys to Interpretation: More P wave than QRS Each QRS is caused by a P-wave Both the P-waves and QRS rhythm is but unassociated Rules of Interpretation: Third Degree AV Block Rate: Atrial is normal. Ventricular is - Rhythm: Both atrial and ventricular rate is regular. Pacemaker Site: SA node and AV junction or PRI: no relationship between P waves and R waves QRS: greater than if pacemaker is ventricular; less than 0.12 if pacemaker is junctional

45 Third Degree AV Block Third Degree AV Block Third Degree AV Block Etiology Absence of conduction between the atria and the ventricles. Results from, digitalis toxicity, or degeneration of the conductive system. Clinical Significance Severely compromised cardiac. 179 Third Degree AV Block Treatment Pacemaker insertion is treatment Transcutaneous for acutely symptomatic patients. Treat symptomatic. should NOT be given May increase atrial rate but worsen block Avoid drugs that may further slow AV conduction. 180
46 Dysrhythmias Sustained or Originating in the AV Junction Dysrhythmias: Premature Junctional Junctional Complexes and Rhythm Accelerated Junctional Rhythm Paroxysmal Junctional Tachycardia Characteristics: P Waves in Lead II PRI of < Seconds Normal QRS Complex Duration 181 Premature Junctional Contractions Description: PJCs result from a single electrical impulse originating in the AV node that occurs before the next expected beat. A PJC can result in a compensatory pause or a -compensatory pause. Compensatory pause: the pause following an ectopic beat where the node is unaffected and the cadence of the heart is uninterrupted 182 Rules of Interpretation: PJC PJC Rate: depends on rhythm Rhythm: depends on underlying rhythm Pacemaker Site: ectopic focus in the AV junction P-Waves: flat or. May occur QRS PRI: Normal if P occurs before QRS QRS: usually

47 PJC 185 PJCs Etiology Single electrical impulse originating in the node. May occur with use of caffeine, tobacco, alcohol, sympathomimetic drugs, ischemic heart disease, hypoxia, or digitalis toxicity, or may be idiopathic. Clinical Significance Limited, frequent PJCs may precursor other junctional dysrhythmias. Treatment usually required. 186 Junctional Escape Complexes and Rhythms Description: results when the rate of the primary pacemaker (SA Node) is slower than that of the AV node. The AV node then becomes the. AV node fires at it s intrinsic rate: - Safety mechanism that prevents cardiac Rules of Interpretation: Junctional Escape Complexes and Rhythms Rate: Rhythm: irregular in single occurrence, regular in junctional escape rhythm Pacemaker Site: Junction P-Waves: inverted,, or after QRS PRI: Normal if before QRS QRS: Usually

48 Junctional Escape Complexes and Rhythms Junctional Rhythm Junctional Escape Complexes and Rhythms Etiology Results when the AV node becomes the pacemaker. Results from increased tone, pathologically slow SA discharges, or heart block. Clinical Significance Slow rate may cardiac output, precipitating angina and other problems. 191 Junctional Escape Complexes and Rhythms Treatment: None if the patient remains. Treat symptomatic episodes with or pacing as indicated. 192

49 Accelerated Junctional Rhythm Description: results from increased automaticity in the AV junction, causing the AV junction to discharge faster than its rate. As the rate increases, the AV node overrides the node. The rate is not, technically, a but because it is faster than its intrinsic rate of the AV junction, it is considered accelerated. Rules of Interpretation: Accelerated Junctional Rhythm Rate: - Rhythm: Pacemaker Site: AV Junction P-Waves: Inverted,, or after QRS complexes PRI: Normal if present and occurs before QRS QRS: Accelerated Junctional Rhythm Accelerated Junctional Rhythm
50 Accelerated Junctional Rhythm Etiology Results from increased in the AV junction. Often occurs due to ischemia of the AV junction. Clinical Significance Usually well tolerated, but for other dysrhythmias. Treatment generally required in the prehospital setting. 197 Paroxysmal Junctional Tachycardia Description: develops when rapid AV junctional depolarization overrides the SA node. Often occurs with sudden onset ( ) May last minutes or hours. May be caused by increased automaticity of a single AV nodal focus or by a phenomenon at the AV node. Sometimes indistinguishable from due to rapid rate 198 Rules of Interpretation: Paroxysmal Junctional Tachycardia Paroxysmal Junctional Tachycardia Rate: - Rhythm: Regular Pacemaker Site: AV Junction P-Waves: Inverted, absent, or QRS PRI: Normal if occurs before QRS QRS:
51 Paroxysmal Junctional Tachycardia 201 Paroxysmal Junctional Tachycardia Etiology Rapid AV junction depolarization overrides the node. Occurs with or without heart disease. May be precipitated by stress, overexertion, smoking, or ingestion. Clinical Significance May be well tolerated for brief periods. Decreased cardiac output will result from prolonged episodes, which may precipitate angina, hypotension, or congestive heart failure. 202 Paroxysmal Junctional Tachycardia Treatment: Same as Maneuvers Pharmacological Therapy Verapamil Electrical Therapy Use if rate is > 150 and patient is hemodynamically unstable. Synchronized cardioversion starting at J. 203 Dysrhythmias Originating in the Ventricles Ventricular Escape Complexes and Rhythms Accelerated Rhythm Premature Ventricular Contractions Ventricular Related Dysrhythmia Ventricular Fibrillation Artificial Rhythm 204
52 Ventricular Escape Complexes and Rhythms AKA: rhythm Description: results either when impulses from higher pacemakers fail to reach the ventricles or when the discharge rate of higher pacemakers become less than that of the ventricles ( - bpm). Serves to prevent cardiac 205 Rules of Interpretation: Ventricular Escape Complexes and Rhythms Rate: (sometimes less) Rhythm: escape complex is. Escape rhythm is regular Pacemaker Site: Ventricle P-Waves: PRI: QRS: Greater than seconds and bizarre in morphology 206 Ventricular Escape Rhythm Ventricular Escape Complexes and Rhythms Etiology mechanism to prevent cardiac standstill. Results from failure of other foci or highdegree block. Clinical Significance cardiac output, possibly to life-threatening levels

53 Ventricular Escape Complexes and Rhythms Treatment: For perfusing rhythms, administer and/or TCP (Pacing). For nonperfusing rhythms, follow pulseless electrical activity ( ) protocols. Accelerated Idioventricular Rhythm Etiology A subtype of ventricular escape rhythm that frequently occurs with. Ventricular escape rhythm with a rate of. Clinical Significance May cause cardiac output if the rate slows Accelerated Idioventricular Rhythm Accelerated Idioventricular Rhythm Treatment: Does not usually require treatment unless the patient becomes hemodynamically. Primary goal is to treat the underlying
54 Premature Ventricular Contractions Description: A is a single ectopic impulse arising from an irritable focus in either ventricle that occurs earlier than the next expected beat. May result from increased automaticity in the cell The altered sequence of ventricular depolarization results in a and bizarre QRS and may cause the T-wave to occur in the opposite direction of the QRS. 213 Premature Ventricular Contractions Pause following a PVC is Occasionally, an interpolated beat occurs when a PVC falls between two sinus beats without interrupting the rhythm If more than 1 PVC occurs, each can be classified as Unifocal or Unifocal: from the same foci (looks alike) Multifocal: from different sites (look different) 214 Groups of PVCs : Every other beat is a PVC Trigeminy: Every third beat is a PVC Quadrageminy: Every fourth beat is a PVC : Two consecutive PVCs Triplet: or more consecutive PVCs Runs of V-Tach: group of or more consecutive PVCs Rules of Interpretation: PVCs Rate: Depends on underlying rhythm Rhythm: Normally. Interrupts underlying rhythm Pacemaker Site: P-Waves: PRI: None QRS: Greater than and bizarre



55 PVCs Unifocal PVCs Multifocal PVCs PVC Couplets


56 PVC Triplets Bigeminy PVCs Etiology Single ectopic impulse resulting from an irritable focus in either Causes may include myocardial ischemia, increased tone, hypoxia, idiopathic causes, acid base disturbances, imbalances, or as a normal variation of the ECG. PVCs May occur in Bigeminy, trigeminy, or quadrigeminy. and triplets. Runs of

57 PVCs Clinical Significance: Malignant PVCs: More than /minute, R on T phenomenon, couplets or runs of ventricular tachycardia, PVCs, or PVCs associated with chest pain. Ventricles do not adequately, causing decreased cardiac output. Treatment of Non-Malignant PVCs Non-malignant PVCs do not usually require treatment in patients without a cardiac history. Most people have PVCs Cardiac patient with nonmalignant PVCs Administer oxygen and establish access Watch EKG closely Treatment of Malignant PVCs R on T phenomenon Treatment of PVCs is normally performed for on phenomenon and symptomatic patients Two drugs to treat PVCs: Do NOT mix anti-dysrhythmics
58 Lidocaine for Malignant PVCs mg/kg IV bolus. If PVCs are not suppressed, repeat doses of - mg/kg to max dose of mg/kg. If PVCs are suppressed, administer lidocaine drip - mg/min. the dose in patients with decreased output or decreased hepatic function and patients > 70 years old. If patient is allergic to Lidocaine, consider Amiodarone 229 Lidocaine Antidysrhythmic (Sodium channel blocker) Contraindications: Allergic or allergic to Indications: V-fib, PVCs, V-Tach A bolus should be followed with a drip if Lidocaine Drip: usually mixed gm/250cc and is run at 2-4mg/min Side Effects: Dizziness, drowsiness, N/V, sensation of heat/cold, numbness 230 Amiodarone (Cordarone) Amiodarone is an alternative to Lidocaine Newer drug with proven success Amiodarone is an antiarrhythmic (Calcium Channel ) Long life Indications: Wide Complex Tachycardia, V-Fib, V-Tach, Supraventricular Tachycardia, Rapid A-Fib Contraindications: Allergic,, Bradycardia 231 Amiodarone (Cordarone) Effects: Inhibits abnormal Increases refractory period at all sites Slows and node rate Causes peripheral 232
59 Amiodarone (Cordarone) Side Effects: Can produce hypotension or Worsens Parestesias (numbness and tingling) Tremor Amiodarone (Cordarone) Initial Dosage (For non per): mg IV push Repeated (if needed) at mg in 3-5 minutes ½ dose (150mg) for perfusing rhythm over 10 minutes Amiodarone (Cordarone) Maintenance Dosage: IV Drip: - mg/min Drip must be in glass or Viaflex bag Glass container is good for 24 hours Viaflex bag is good for hours Amiodarone drips normally not established in setting Notify ER that Amiodarone was given 235 Ventricular Tachycardia V-Tach Description: or more ventricular contractions in succession with a rate of bpm or faster. Overrides the node. May be present with or without a Monomorphic V-Tach: all complexes appear the (Most common). Polymorphic V-Tach: complexes have different sizes and shapes. (Torsade de Pointes) 236
60 Rules of Interpretation: V-Tach V-Tach Rate: - Rhythm: usually regular Pacemaker site: P-Waves: If present, not associated with QRS PRI: QRS: greater than seconds and bizarre V-Tach V-Tach Etiology: 3 or more ventricular complexes in succession at a rate of >. Causes include myocardial ischemia, increased sympathetic tone,, idiopathic causes, acid base disturbances, or electrolyte imbalances. VT may appear or polymorphic
61 V-Tach Clinical Significance: Decreased output, possibly to life-threatening levels. May deteriorate into ventricular. Treatment of V-Tach Perfusing patient: Administer and establish IV access. Consider immediate synchronized starting at 100J for hemodynamically patients. (normally 100J, 200J, 300J, 360J or biphasic equivalent) Sedate if necessary Treatment of V-Tach Perfusing Patient (Cont d) mg IV over 10 minutes. Repeated once at 150mg, OR mg/kg IV Mixing of antiarrhythmics is NOT recommended Administer repeat doses of Lidocaine 0.5 1mg/kg to the max dose of 3.0 mg/kg, or until VT is suppressed. (Lidocaine if conversion) 243 V-Tach Treatment Summary Conscious Patient BLS, IV Drugs Amiodarone Lidocaine Synchronized Cardioversion Sedation? 100J, 200J, 300J, 360J Unconscious Patient With a Pulse BLS, IV Synchronized Cardioversion 100J, 200J, 300J, 360J Drugs Amiodarone Lidocaine 244
 Magnesium sulfate 1 2 g diluted in 100 ml D5W over 1 2 minutes is drug of choice.")
62 Treatment of V-Tach Non-Perfusing Patients (No Pulse): Treat as Ventricular (V-Fib) Torsade de Pointes Typically occurs in nonsustained bursts. Prolonged - interval during breaks. QRS rates from RR interval highly. Treatment Do not treat as standard VT ( not indicated) Magnesium sulfate 1 2 g diluted in 100 ml D5W over 1 2 minutes is drug of choice. Amiodarone mg Torsade de Pointes Ventricular Fibrillation (V-Fib) Description: a ventricular rhythm usually resulting from the presence of many reentry circuits within the ventricles. No ventricular polarization or depolarization May be or course CANNOT produce a


63 Rules of Interpretation: V-Fib Rate: no organized rhythm Rhythm: no organized rhythm Pacemaker Site: numerous ectopic foci throughout the P-Waves: Usually absent PRI: QRS: V-Fib V-Fib Fine V-Fib
64 Course V-Fib V-Fib Etiology Wide variety of causes, often resulting from advanced artery disease. Clinical Significance dysrhythmia with no cardiac output and no organized electrical pattern Treatment of V-Fib Initiate CPR for 2 minutes unless witnessed or CPR has been in progress for 2 minutes or more. Defibrillate once at J (or biphasic equivalent) Continue CPR without checking or ECG Establish access and then control the airway Treatment of V-Fib Administer Epinephrine 1:10,000 every minutes for duration of arrest. Administer second-line drugs such as Lidocaine, Amiodarone, or Magnesium Sulfate. Do NOT mix Consider 40 IU IV instead of 1 st or 2 nd dose of Epinephrine (one time only)
65 Epinephrine 1:10,000 agonist (Adrenalin) Stimulates both alpha and beta adrenergic Alpha Receptors: Peripheral (arteries and veins) Bronchoconstriction Beta Receptors: Epinephrine 1:10,000 Increase of cardiac contractility and thus increasing cardiac output and heart rate Relaxing of muscles in bronchi Dilation of arteries Epinephrine 1:10,000 Epinephrine is mostly beta with some alpha Increases cardiac and automaticity Dilates passageways Decreases resistance to electrical shock Dilates coronary arteries peripheral blood vessels 259 Epinephrine 1:10,000 Indications: ALL cardiac arrests, allergic reactions, severe asthma attacks Contraindications: None in cardiac arrest Adult Dosage: mg every - minutes for duration of arrest Side effects: none in cardiac arrest Normally supplied as mg in cc of solvent in syringes 260
66 Vasopressin AKA: Pitressin, ADH (Anti-Diuretic Hormone) Synthetic Pituitary Hormone Indication: V-Fib, pulseless V-Tach Actions: vasoconstrictor Decreases to electrical shock Has no cardiac stimulatory properties Useful when heart is over Vasopressin Contraindications: None in V-Fib or Pulseless V-Tach Dosage: units IV push Currently, no dosage Used instead of or round of Epi Asystole Description: Cardiac The of all cardiac electrical activity CANNOT produce a pulse Flat Line : However, very rarely Rules of Interpretation: Asystole Rate: No electrical activity Rhythm: No electrical activity Pacemaker Site: No electrical activity P-Waves: PRI: QRS:

67 Asystole Asystole Asystole Etiology Primary event in cardiac arrest, resulting from massive myocardial infarction, ischemia, and necrosis. outcome of ventricular fibrillation. Clinical Significance Asystole results in cardiac arrest. Poor for resuscitation. 267 Treatment for Asystole Administer CPR and manage the airway. Confirm in Lead Treat for ventricular fibrillation if there is any doubt about the underlying rhythm. Epinephrine mg every - minutes for duration Consider causes: 6 H s and 5 T s Possibly sodium. 268
68 6 H s Hypovolemia Hydrogen Ion- Acidosis Hyper/Hypokalemia Hypothermia Causes of Asystole 5 T s Tablets (OD) Tension Pneumothorax Thrombosis (Cardiac), pulmonary (PE) Artificial Pacemaker Rhythm Description: results from stimulation of the heart by an artificial pacemaker Rate Pacemakers: fire continuously at a preset rate; regardless of heart s own electrical activity Pacemakers: Monitors heart s electrical activity and only fires if heart rate drops below a preset rate Artificial Pacemaker Rhythm Pacemakers stimulate only the right ventricle resulting in a rhythm that resembles an idioventricular rhythm chambered pacemakers stimulate the atria first and then the ventricles Usually inserted in patients with severe symptomatic Rules of Interpretation: Artificial Pacemaker Rhythm Rate: varies with rate of pacemaker Rhythm: regular if pacing regularly Pacemaker Site: Depends on electrode placement P-Waves: produced by ventricular pacemaker. Sinus P- waves may be seen but are unassociated with QRS. Pacemaker may be visible QRS: greater than seconds, bizarre



69 Artificial Pacemaker Rhythm Atrial Pacemaker Rhythm Ventricular Pacemaker Rhythm Dual Chamber Pacemaker Rhythm
70 Artificial Pacemaker Rhythm Etiology Single vs. dual chamber pacemakers. Fixed-rate vs. demand pacemakers. Clinical Significance Used in patients with a chronic high- grade heart block, sick sinus syndrome, or severe symptomatic bradycardia. Pacemaker may NOT be seen. Obtain history in any patient who presents with broad QRS rhythms Artificial Pacemaker Rhythm Problems with Pacemakers failure pacers Displaced Use a to turn unit off if needed (contact medical control first) Artificial Pacemaker Rhythm Management Considerations: Identify patients with pacemakers. Treat the. Use an pacemaker if malfunctioning Try to avoid placing d-fib pads (or paddles) on pacemaker site The only way to confirm that a pacemaker is working correctly is to assure pulse corresponds with 279 Pulseless Electrical Activity (PEA) Formerly called electrical mechanical dissociation ( ) Characteristics Electrical impulses are present, but with no accompanying mechanical contractions of the. Treat the patient, not the. ECG could show ANY rhythm that is normally a perfusing rhythm 280
71 Treatment of PEA Prompt recognition and early treatment. 1 mg every 3 5 minutes. Identify and treat underlying of PEA. 6 H s and 5 T s (same as asystole) Treatment of Underlying Causes of PEA/Asystole Condition Treatment Hypovolemia Cardiac Tamponade Pericardiosentesis Tension Pneumothorax Oxygen/Intubation Sodium Bicarbonate Hypoglycemia D50W Dysrhythmias Resulting from Disorders of Conduction Categories of Conductive Disorders: Blocks Disturbances of Ventricular Conduction Syndromes Disturbances of Ventricular Conduction Conduction: a single supraventricular beat conducted through the ventricles in a delayed manner Branch Block: disorder in which all supraventricular beats are conducted through the ventricles in a delayed manner


72 Bundle Branch Block Can involve either the left or right bundle branch If both branches are involved, then a degree block exists Causes Ischemia or necrosis of a bundle branch PAC or that reaches one of the bundle branches in a refractory period Causes wide complexes with P- waves present 285 Left Bundle Branch Block 286 Pre-Excitation Syndromes Excitation by an impulse that bypasses the AV node Most common is Wolf-Parkinson-White ( ) Syndrome Characterized by a short and a long duration. Upstroke of the QRS often has a slur called a wave Treatment is to treat underlying rhythm Pre-Excitation Syndromes


 Atrial Fibrillation (Ventricular rate <")
73 Wolf-Parkinson-White Syndrome (WPW) ECG Changes Due to Electrolyte Abnormalities and Hypothermia Hyperkalemia: Tall Suspect in patients with a history of renal failure. Hypokalemia: Prominent waves Hypothermia wave ( J wave) T wave inversion, sinus bradycardia, atrial fib or flutter, AV blocks, PVCs, VF, asystole J-Wave 291 Classifications of Cardiac Rhythms Class I Rhythms: Not treated Sinus Rhythm Class II Rhythms: Not routinely treated by EMS Sinus Wandering Premature atrial contractions Atrial Flutter (Ventricular rate < 150bpm) Atrial Fibrillation (Ventricular rate < 150bpm) Premature Ventricular Contractions (<5 per minute) 292
74 Classifications of Cardiac Rhythms Class II Rhythms: Not routinely treated by EMS (Continued): Premature junctional complex rhythm Accelerated junctional rhythm Junctional tachycardia (ventricular rate < 150) degree AV block degree AV block, type I (Wenckebach) (ventricular rate < 150) Classifications of Cardiac Rhythms Class III: Treated by EMS to prevent rhythm becoming Class IV: Supraventricular Tachycardia (ventricular rate > 150) 2 nd Degree AV block, Type Degree AV block Classifications of Cardiac Rhythms Class III (Continued): Premature Ventricular Contractions, if: Patients Runs of V-Tach on Phenomenon PVCs Classifications of Cardiac Rhythms Class IV: Must be treated in pre-hospital setting, or death will result: Ventricular Fibrillation (VF or V-Fib) Ventricular Tachycardia (VT or V-Tach) Pulseless Electrical Activity ( )
75 Treating Cardiac Dysrhythmias Determine that there is a true need to treat the dysrhythmia before treating it Obtain a chief BEFORE treating the dysrhythmia Most importantly.. TREAT THE PATIENT, NOT THE MONITOR 297
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Basic EKG Interpretation. Nirja Parikh, PT, DPT
 Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Basic Dysrhythmia Interpretation
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms
 Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Paramedic Rounds. Tachyarrhythmia's. Sean Sutton Dallas Wood
 Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
COURSE DESCRIPTION. Rev 2.0 7/2013. Page 1 of 26
 COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
Basic ECG Interpretation Module Notebook
 Basic ECG Interpretation Module Notebook ECG_Notebook_04.27.05 Page 1 of 142 Basic ECG Interpretation Table of Contents Module Objectives... 3 Module Outline... 6 Lesson I... 6 Lesson II... 8 Lesson III...
Basic ECG Interpretation Module Notebook ECG_Notebook_04.27.05 Page 1 of 142 Basic ECG Interpretation Table of Contents Module Objectives... 3 Module Outline... 6 Lesson I... 6 Lesson II... 8 Lesson III...
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Cardiology Part 2. Practice Test A
 Cardiology Part 2 Practice Test A The following practice exam is comprised of all multiple-choice questions. Select the response that MOST appropriately answers the question. The questions are designed
Cardiology Part 2 Practice Test A The following practice exam is comprised of all multiple-choice questions. Select the response that MOST appropriately answers the question. The questions are designed
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Chapter 20 (2) The Heart
 The Heart") Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
CORONARY ARTERIES HEART
 CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2
Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2
8/20/2012. Learning Outcomes (Cont d)
") 1 2 3 4 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2 Identify premature junctional complexes
1 2 3 4 Electrocardiography for Healthcare Professionals Chapter 7: Junctional Dysrhythmias Learning Outcomes 7.1 Describe the various junctional dysrhythmias 7.2 Identify premature junctional complexes
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Cardiology. Objectives. Chapter
 1:44 M age 1121 Chapter Cardiology Objectives art 1: Cardiovascular natomy and hysiology, ECG Monitoring, and Dysrhythmia nalysis (begins on p. 1127) fter reading art 1 of this chapter, you should be able
1:44 M age 1121 Chapter Cardiology Objectives art 1: Cardiovascular natomy and hysiology, ECG Monitoring, and Dysrhythmia nalysis (begins on p. 1127) fter reading art 1 of this chapter, you should be able
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG Interpretation and Clinical Significance
 Confirming Pages ECG Interpretation and Clinical Significance Chapter Outline 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 5.9 5.10 Learning Outcomes Key Terms Introduction (p. 114) Identifying the Components of the
Confirming Pages ECG Interpretation and Clinical Significance Chapter Outline 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 5.9 5.10 Learning Outcomes Key Terms Introduction (p. 114) Identifying the Components of the
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Electrical Conduction
 Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
Sinoatrial (SA) node Electrical Conduction Sets the pace of the heartbeat at 70 bpm AV node (50 bpm) and Purkinje fibers (25 40 bpm) can act as pacemakers under some conditions Internodal pathway from
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017
 CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.
Antiarrhythmic Drugs 1/31/2018 1
 Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
5AB Dysrhythmia Interpretation tation and Management Review Please complete and return by:
 1 5AB Dysrhythmia Interpretation tation and Management Review 2014 RN Please complete and return by: Overview 2 This review begins with a discussion of the physiology of cardiac conduction, and then covers
1 5AB Dysrhythmia Interpretation tation and Management Review 2014 RN Please complete and return by: Overview 2 This review begins with a discussion of the physiology of cardiac conduction, and then covers
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
Electrocardiography for Healthcare Professionals Kathryn A. Booth Thomas O Brien Chapter 5: Rhythm Strip Interpretation and Sinus Rhythms Learning Outcomes 5.1 Explain the process of evaluating ECG tracings
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
Practical Approach to Arrhythmias
 Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Cardiac Arrhythmias in Sleep
 Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most