Asymptomatic Carotid Stenosis To Do or Not To Do
|
|
|
- Meghan Shields
- 6 years ago
- Views:
Transcription
1 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital
2
3 Principle Sources Seemant Chaturvedi M.D. University of Miami J. David Spence M.D., Western University, Ontario Canada
4 Topics of Discussion Epidemiology Clinical Correlates Landmark CEA studies Modern Medical Management of Carotid Stenosis recommendations Future of ACS (Asymptomatic Carotid Stenosis), Evaluation and Management
5 Prevalence Asymptomatic severe stenosis (>70%) in unselected patients 0-3.1% * In men > 70 years, 2-3% * In women > 70 years, roughly 1% * Higher rates in patients with DM * In USPSTF prevalence of high grade carotid stenosis fell from 1% (1992) to 0.5% (1998) likely secondary to improved medical management Ethnic Differences in Carotid Stenosis Native Americans > Caucasians > Hispanics > African Americans > Asians *De Weerd et al STROKE 2010, 41:
6 Methods for diagnosis U/S 70-80% accurate MRA CTA Conventional angiography Prior to intervention, 2 studies recommended and angiography used for discordant cases
7 How are patients identified Carotid bruits Contralateral symptomatic lesion Screening for surgical procedures (CABG, AAA surgery) Screening due to atherosclerotic disease elsewhere General screening not recommended by USPSTF (2014)
8 Clinical Manifestation Purely asymptomatic Cognitive dysfunction? Renewed interest Imaging evidence of silent brain infarction beyond ACS TIA or Stroke > 6 months earlier VB Symptoms
9 Risk for ACS Similar for CAD Age Male Smoking DM Hypertension High LDL Low HDL Likely Risks: Diet high in fat and cholesterol Sedentary Life Style Family History Mental/Social Stress
10 Risk stratification in ACS Clinical variables Age, gender and ethnicity Transcranial Doppler with embolus detection Plaque echolucency or ulceration Progression of stenosis MRI of the plaque (lipid core, intra-plaque hemorrhage)
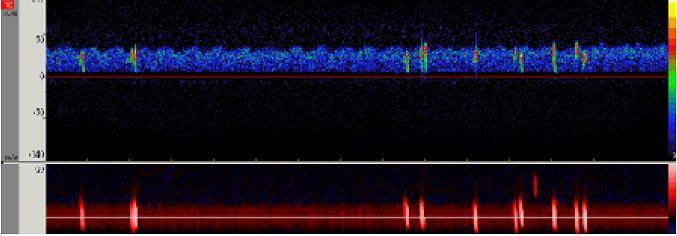
11 TCD microembolus detection 319 ACS patients studied between % had high intensity signals indicative of microemboli Stroke risk at 1 year No emboli 1% Emboli 15.6% Spence Stroke 2005,
12
13 Decline of microemboli with intensive medical therapy Prior to % After 2003 (intensive medical therapy) 3.7% Conclusion, reduction of microemboli equals reduction of stroke Spence, Arch Neurol, 2010, 67: 180-6
14
15 ACES Study (Asymptomatic Carotid Emboli Study) 467 patients with ACS studied with TCD looking for microembolus signal 16% had embolic signals (84% no embolic signal) 3.6% annual stroke rate if + for embolic signal 0.7% annual stroke rate if for embolic signal Conclusion - Embolic signal = Stroke No embolic signal = No stroke
16 ACES Study (cont.) Embolic signal plus plaque echolucency 37% had + plaque echolucency Echolucency predicts increase stroke rate Plaque echolucency plus microemboli additive risk Conclusion Combined studies can identify high risk group (8% per year) and low risk group (<1% per year) based on echolucency and microemboli on TCD Neurology 2011, 77:
17 Progression of Stenosis Categories 0-49%, 50-69%, 70-89%, 90-99%, 100% Progression of stenosis by 2 or 3 categories associated with ipsilateral stroke of TIA 1469 patients studied 50 patients showed (2.9%) progressed by 2 categories However, regression was as likely as progression Likely secondary to medical therapy Stroke 2014, 45:
18 Newer imaging techniques Will improve risk stratifications 3D U/S revealing plaque ulceration and plaque echolucency (increased fat content in plaque) Plaque MRI reveals intra-plaque hemorrhage PET Scan reveals plaque inflammation TCD with embolus detection grossly under utilized Stroke, 2014, 45:
19 Best medical management 2015 for ACS Antiplatelet agents (? Dual) Aggressive use of high potency statins; Rosuvastatin (Crestor), Ezetimibe (Zetia) Targeted blood pressure lowering (< 140 systolic, <130 in DM) ACE/ARB utilizations (? Additional protective effect beyond blood pressure control) Smoking cessation Risk factor control (DM, A1C control) Life style interventions (regular exercise and Mediterranean type diet)
20 History of CEA Where have we been? NASCET and ECST launched in 1980 s for symptomatic stenosis ACAS for asymptomatic stenosis ACST in 1990 s These studies resulted in sharp increase in CEA ~ 135,000 per year All studies done prior to aggressive medical therapy including statin use
21 250,000 Carotid Interventions worldwide Asymptomatic (%) Proportion Stented (%) US Europe UK Proportio n CEA Uncertainty about whether to intervene in asymptomatic patients as well as about choosing CEA vs. CAS
22 Absolute Benefits of CEA Symptomatic 70-99% - 8.5% absolute risk reduction Symptomatic 50-69% - 1.3% absolute risk reduction Asymptomatic - 1.2% absolute risk reduction Conclusion CEA in asymptomatic patients minimal value
23 Questions Remaining Value in Women Value in Elderly > 75 years of age Not well established in either group
24 Annual Stroke Rates with Carotid Stenosis Pre-Statin use: Symptomatic 70-90% (13%/yr) Asymptomatic 60-90% (2 2.5%/yr) Statin use: Percentage of patients on statins NASCET 14.5% (1980 s) ACE 28% (1990 s) ASCT 38% (2000 s) Statin use continuing to increase
25 AHA/ASA Guidelines for Primary Stroke Prevention 2014 Patients with ACS should be prescribed daily ASA and a statin. Patients should be screened for other treatable risk factors for stroke Class I It is reasonable to consider performing CEA in asymptomatic patients who have > 70% stenosis of ICA if the risks of perioperative stroke, MI and death is low (<3%). However it s effectiveness compared to contemporary best medical management alone is not well established.
26 ASA primary prevention Prophylactic CAS might be considered in highly selective patients with asymptomatic carotid stenosis (minimum, 60% by angiography, 70% by validated Doppler U/S) but it s effectiveness compared with medical therapy alone is not well established (Class IIb; level of evidence B.)
27 ASA primary prevention Selection of asymptomatic patients should be guided by co-morbid conditions and life expectancy Prophylactic CEA with M&M less than 3% can be useful in highly selected patients 3% threshold for complication rate may be high because of advances in medical therapy
28 AAN Choosing wisely recommendations Don t perform imaging of the carotid arteries for simple syncope Don t recommend CEA for asymptomatic stenosis unless the complication rate is <3%
29 CREST Trial (Carotid Revascularization Endarterectomy vs. Stent Trial) Stroke, Death, MI + ipsilateral stroke after 30 days CEA CAS 6.8 % 7.2% Stroke w/in 30 days 2.3% 4.1% MI w/in 30 days 2.3% 1.1% Peri-Procedural Stroke or Death in Asymptomatic CREST patients CAS 15 CEA 8
30 What about intensive medical therapy? There has never been a large multi-center study done to compare carotid revascularization + IMT vs. IMT alone Goals for IMT LDL < 70mb/dl SBP < 140 for Non-diabetics < 130 for DM Statins Dual anti-platelet therapy Life style management
31 Potential Risk Reductions Estimated with IMT High Potency Statins 33% RRR Dual Antiplatelet therapy 10-32% RRR B/P control % RRR Life Style Management % RRR Recent studies using modern medical therapy and risk stratification report stroke rates of.34% (Oxford Vascular Study); 0.3% (SMART); 0.7% (ACES) If confirmed by larger studies CAS/CEA will unlikely achieve these results SPARCL Trial, CHANCE Trial
32 Next generation of studies CREST 2 ECST 2 SPACE 2 ACST 2 All above studies will include best aggressive medical care arms
33 What might the future bring? Genetic Markers (Chromosome 9p21.3) Advanced imaging Bio-markers Risk stratification
34 Conclusions & Recommendations Asymptomatic carotid stenosis is uncommon in unselected patients Variety of diagnostic test available with variable reliability Risk stratification may be extremely useful Early studies suggest value of endarterectomy and possibly carotid stenting With intensive medical therapy the risk of stroke or death in patients with ACS appears below the risk of endarterectomy or stenting (SPENCE)
35 Conclusions & Recommendations Most ACS patients (approx. 90%) will be better off with medical therapy than either intervention (SPENCE) The few patients that may benefit from intervention can be identified with TCD w/ embolus detection and/or advanced imaging of the plaque (SPENCE) The vast majority of patients should be treated with IMT including high potency statins and ezetimible (Zetia), life style changes, dual antiplatelet and effective B/P control (SPENCE)
The argument against revascularization for asymptomatic carotid stenosis
 The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
CEA or CAS for asymptomatic carotid stenosis which patients benefit most?
 CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
CEA or CAS for asymptomatic carotid stenosis which patients benefit most? Alison Halliday Professor of Vascular Surgery University of Oxford Keynote Lecture, MAC, December 6 th 2018 Clinical/imaging characteristics
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis?
 for stroke prevention in patients with asymptomatic carotid stenosis?") How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
How good is current best medical therapy (BMT) for stroke prevention in patients with asymptomatic carotid stenosis? Dorothee Saur Department of Neurology University of Leipzig Disclosure for Dorothee
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2
 Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
Update on the only remaining Carotid Multicenter Randomised International Trial in the World:ACST-2 Alison Halliday MD Professor of Vascular Surgery University of Oxford Disclosure Statement of Financial
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered?
 TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
TCT 2009 San Francisco, California September 22, 2009 The Effectiveness of Medical Therapy for Severe Carotid Stenosis in Reducing Large-Vessel Embolic Stroke: Open Question or Question Answered? Michael
Stroke prevention in asymptomatic carotid stenosis. ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ
 Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Stroke prevention in asymptomatic carotid stenosis ΛΙΛΛΗΣ ΛΕΩΝΙΔΑΣ Καρδιολόγος Επιστημονικός Συνεργάτης Α Καρδιολογικής Κλινικής ΑΠΘ ΠΓΝΘ ΑΧΕΠΑ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας
Carotid Artery Disease How the Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient
 Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Carotid Artery Disease How the 2014-2015 Data Will Influence Management The Symptomatic vs. the Asymptomatic Patient Christopher J. White, MD, MSCAI, FACC, FAHA, FESC Professor and Chair of Medicine Ochsner
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS. Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford
 Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
Current Status and Perspectives of ACST-2, CREST-2, ECST-2 and ACTRIS Richard Bulbulia Co-Principal Investigator ACST-2 University of Oxford Two BIG questions in carotid research Question #1 Should we
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease
 The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
The most important recommendations from the 2017 ESVS/ESC guideline on the management of carotid artery disease GJ de Borst Department of Vascular Surgery RECOMMENDATION GRADING CRITERIA What is new
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
MEET Θ symptomatic patients. K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany
 MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
MEET Θ 2006 Why I stent asymptomatic and symptomatic patients K. Mathias Department of Radiology Teaching Hospital of Dortmund - Germany Evidence for treating symptomatic patients symptomatic patients
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention
 How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
How to Choose Between Carotid Stenting and Carotid Endarterectomy for Stroke Prevention Christopher J. White MD, MSCAI Chief of Medical Services, Professor and Chairman of Medicine Ochsner Medical Center
Spontaneous embolisation on TCD and carotid plaque features
 Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Spontaneous embolisation on TCD and carotid plaque features J. David Spence Stroke Prevention & Atherosclerosis Research Centre Robarts Research Institute London, Canada dspence@robarts.ca www.imaging.robarts.ca/sparc
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
ESC Heart & Brain Workshop
 ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
ESC Heart & Brain Workshop The role of vascular surgeon in stroke prevention Barbara Rantner, MD, PhD, Department of Vascular Surgery, Medical University Innsbruck, Innsbruck, Austria Supported by Bayer,
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
The argument against revascularization for asymptomatic carotid stenosis
 The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
The argument against revascularization for asymptomatic carotid stenosis Seemant Chaturvedi, MD, FAHA, FAAN Professor of Clinical Neurology Vice-Chair for VA Programs Univ. of Miami Miller School of Medicine
Approach to the Patient with Carotid Artery Disease
 Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Approach to the Patient with Carotid Artery Disease Michael R. Jaff, DO, FACP, FACC Director, Vascular Medicine Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Statement Within
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective)
") Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Endarterectomy vs. Carotid artery Stenting (Surgeon Perspective) T-Woei Tan, MD, FACS, RPVI Assistant Professor of Surgery Vascular and Endovascular Surgery Louisiana State University Health -
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor
 Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC
 CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
CNSF Meeting, Victoria, BC. June 2017 Contemporary Carotid Imaging and Approach to Treatment: Course Notes Thursday, June 22, 2017 David M. Pelz, MD, FRCPC A. Objectives 1. To understand the current imaging
LARGE ARTERY DISEASE pathophysiology of ischemic insults. ISCHEMIC STROKE & TIA main etiologies
 תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
תאריך בדיקה- 27.1.04 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
ISCHEMIC STROKE & TIA main etiologies
 דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
דופלקס עורקי צוואר - משמעות בגיל הקשיש דר' יונתן שטרייפלר מנהל היחידה הנוירולוגית מרכז רפואי רבין - בי"ח השרון תאריך בדיקה- 27.1.04 ISCHEMIC STROKE & TIA main etiologies Large vessel (artery) disease -
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy
 13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
13 th Annual Angioplasty Summit TCT Asia Pacific Seoul, Korea April 24, 2008 Which Patients Are Good Candidates for Carotid Artery Stenting or Carotid Endarterectomy Michael R. Jaff, DO, FACP, FACC Associate
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
CAROTID STENTING A 2009 UPDATE. Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital
 CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
CAROTID STENTING A 2009 UPDATE Hoang Duong, MD Director of Interventional Neuroradiology Memorial Regional Hospital TREATMENT FOR CAROTID STENOSIS Best medical management Antiplatelet therapy Antihypertensive
Prise en charge du polyvasculaire
 Prise en charge du polyvasculaire Dépistage et prise en charge des sténoses carotidiennes Serge Kownator Centre cardiologique et Vasculaire - Thionville Disclosure Statement of Financial Interest I currently
Prise en charge du polyvasculaire Dépistage et prise en charge des sténoses carotidiennes Serge Kownator Centre cardiologique et Vasculaire - Thionville Disclosure Statement of Financial Interest I currently
I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease
 I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease Alonso Collar, M.D. F.A.C.S. Chief of Surgery Chair Cardiovascular Surgery Sparrow Hospital Lansing, MI I want Medical Therapy for
I want Medical Therapy for my ASYMPTOMATIC patients with Carotid Disease Alonso Collar, M.D. F.A.C.S. Chief of Surgery Chair Cardiovascular Surgery Sparrow Hospital Lansing, MI I want Medical Therapy for
CardioLucca2014. Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee. Fabrizio Tomai
 CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
CardioLucca2014 Fare luce sulla scelta ottimale del trattamento nella rivascolarizzazione delle stenosi carotidee Fabrizio Tomai European Hospital e Aurelia Hospital Roma Treatment of Carotid Artery Disease
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Stenting Versus
 Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Carotid Artery Stenting Versus Carotid Endarterectomy Seong-Wook Park, MD, PhD, FACC,, Seoul, Korea Stroke & Carotid artery stenosis Stroke & Carotid artery stenosis Cerebrovascular disease is one of the
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
Carotid Artery Stent: Is it ready for prime time?
 2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
2010 CATH LAB SYMPOSIUM Carotid Artery Stent: Is it ready for prime time? Luis F. Tami, MD, FACC, FSCAI Interventional Cardiology and Vascular Medicine Memorial Regional Hospital August 2010 CAE and CAS
ESC Heart & Brain Workshop
 ESC Heart & Brain Workshop Carotid Stenosis - selecting the high risk patients for intervention Alison Halliday, Professor of Vascular Surgery, University of Oxford 20 th January 2018, Prague ESC Workshop
ESC Heart & Brain Workshop Carotid Stenosis - selecting the high risk patients for intervention Alison Halliday, Professor of Vascular Surgery, University of Oxford 20 th January 2018, Prague ESC Workshop
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
The Great Swedish Debate. Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund
 The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
The Great Swedish Debate Håkan Pärsson Department Vascular Surgery Helsingborgs Lasarett, University Lund My Disclosures Trying to bribe the moderators What do my patients expect? Balanced information
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Emboli detection to evaluate risk of stroke
 Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Emboli detection to evaluate risk of stroke Background: Improved methods are required to identify patients with asymptomatic carotid stenosis at high risk for stroke. Whether surgery is beneficial for
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Update : Carotid Stenting and Current Trial Data
 Update : Carotid Stenting and Current Trial Data J. Michael Bacharach, MD, MPH, FACC, FSCAI Section Head, Vascular Medicine and Vascular Intervention North Central Heart Institute, Sioux Falls, South Dakota
Update : Carotid Stenting and Current Trial Data J. Michael Bacharach, MD, MPH, FACC, FSCAI Section Head, Vascular Medicine and Vascular Intervention North Central Heart Institute, Sioux Falls, South Dakota
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions. No Disclosures. Prevalence >70% Asymptomatic ICA Stenosis*
 How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
FRANK J. VEITH MAC TH MUNICH VASCULAR CONF
 UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
UPDATE ON THE NORTH AMERICAN RCTs CREST 2 & ACST 1: WILL CAS SURVIVE AS AN ALTERNATIVE TO BMT OR CEA? FRANK J. VEITH 6 TH MUNICH VASCULAR CONF MAC - 2016 MUNICH DECEMBER 1, 2016 I HAVE NO FINANCIAL CONFLICTS
Best Medical Therapy for asymptomatic carotid disease
 Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Best Medical Therapy for asymptomatic carotid disease Richard Bulbulia Consultant Vascular Surgeon and Co-PI ACST-2 MRC Population Health Research Unit CTSU, Nuffield Department of Population Health University
Non-Selective Carotid Artery Ultrasound Screening in Patients Undergoing Coronary Artery Bypass Grafting: Is It Necessary?
 Non-Selective Carotid Artery Ultrasound Screening in Patients Undergoing Coronary Artery Bypass Grafting: Is It Necessary? Khalil Masabni, Joseph F. Sabik III, Sajjad Raza, Theresa Carnes, Hemantha Koduri,
Non-Selective Carotid Artery Ultrasound Screening in Patients Undergoing Coronary Artery Bypass Grafting: Is It Necessary? Khalil Masabni, Joseph F. Sabik III, Sajjad Raza, Theresa Carnes, Hemantha Koduri,
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Octogenarians Must Be Treated With CAS
 Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Some Octogenarians Must Be Treated With CAS LN Hopkins, MD E Levy MD, Adnan Siddiqui,, MD, PhD Rod Samuelson MD J Mocco MD LN Hopkins, MD Potential Conflicts Consultant & research support: Boston Scientific,
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA
 Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
4/14/2018 DYSLIPIDEMIA CASES. Mary Malloy, MD. I have nothing to disclose
 DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Screening for Asymptomatic Carotid Artery Stenosis: A Systematic Review and Meta-Analysis for the U.S. Preventive Services Task Force
 Evidence Synthesis Number 111 Screening for Asymptomatic Carotid Artery Stenosis: A Systematic Review and Meta-Analysis for the U.S. Preventive Services Task Force Prepared for: Agency for Healthcare Research
Evidence Synthesis Number 111 Screening for Asymptomatic Carotid Artery Stenosis: A Systematic Review and Meta-Analysis for the U.S. Preventive Services Task Force Prepared for: Agency for Healthcare Research
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
TCD in Subclavian Steal Syndrome
 ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Prevention of MACROvascular Complications of Diabetes
 Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
Carotid Artery Stenting
 Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
Carotid Artery Stenting Natural history of the carotid stenosis Asymptomatic 80% carotid stenosis - 6% risk of stroke / year Symptomatic carotid stenosis have 10% risk of CVA at one year and 40% at 5 years
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
ICSS Safety Results NOT for PUBLICATION. June 2009 ICSS ICSS ICSS ICSS. International Carotid Stenting Study: Main Inclusion Criteria
 Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
Safety Results NOT for The following slides were presented to the Investigators Meeting on 22/05/09 and most of them were also presented at the European Stroke Conference on 27/05/09 They are NOT for in
ASYMPTOMATIC CAROTID STENOSIS WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS
 CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS") WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
BULgarian Carotid Artery Stenting versus Surgery Study (BULCASSS): Randomized single center trial
: Randomized single center trial") BULgarian Carotid Artery Stenting versus Surgery Study (): Randomized single center trial Ivo Petrov, M. Konteva, H. Dimitrov, K. Kichukov Tokuda Hospital Sofia Cardiology Department Background Carotid
BULgarian Carotid Artery Stenting versus Surgery Study (): Randomized single center trial Ivo Petrov, M. Konteva, H. Dimitrov, K. Kichukov Tokuda Hospital Sofia Cardiology Department Background Carotid
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine