|
|
|
- Dustin Montgomery
- 6 years ago
- Views:
Transcription
1 Arrhythmology
2
 Slow cells which participate in conduction through SA and AV node 3) Pacemaker cells that create the electric signal.")
3 Cardiomyocytes Heart muscle consists of three types of cells: 1) Fast cells of working myocardium that make a contraction as a response to electric signal created in pacemaker cells most common type 2) Slow cells which participate in conduction through SA and AV node 3) Pacemaker cells that create the electric signal. Connection between two cells is maintained by desmosomes
4
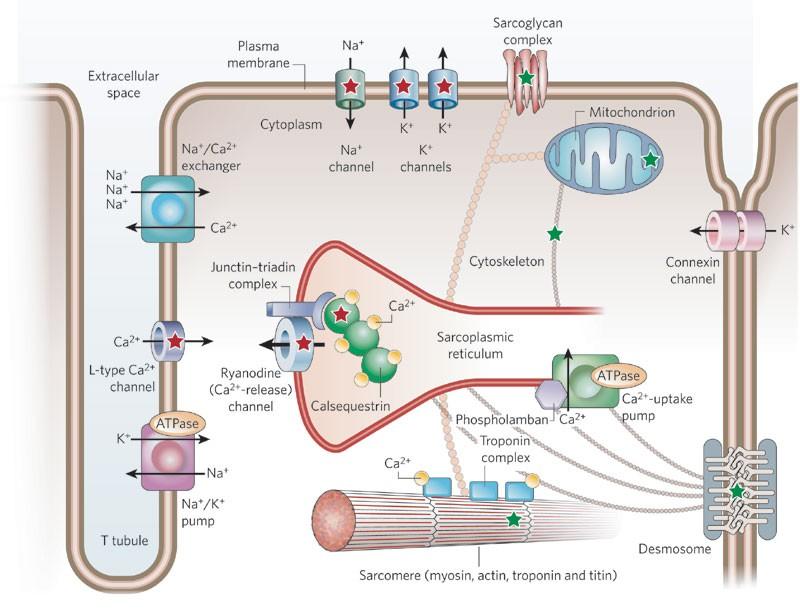
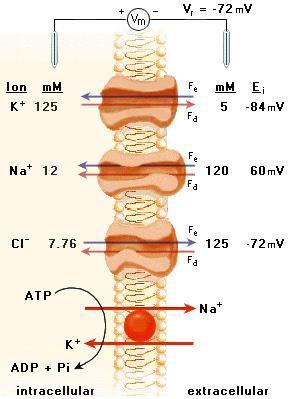
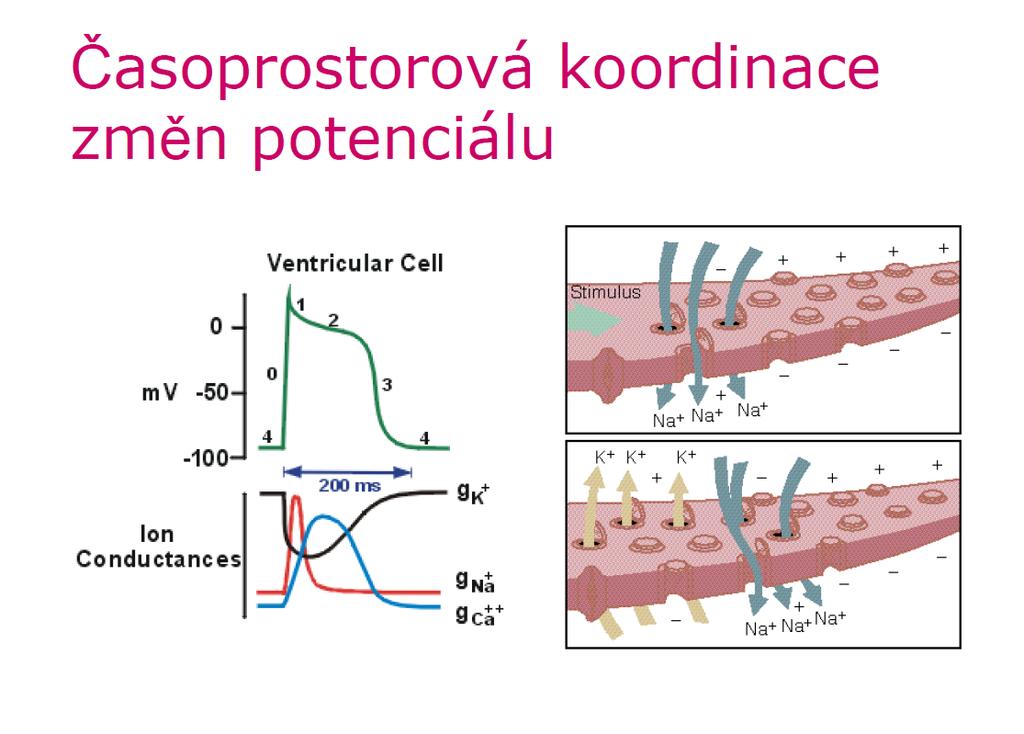
5 Mechanism of cardiomyocyte activity 1 Three cations present in both extra- and intracelular fluid participate in electrical activity of heart muscle: Na +, K + and Ca 2+. Na + and Ca 2+ are present mainly in ECF (Ca 2+ also in endoplasmic reticulum), K + in ICF During fast depolarisation of a cardiomyocyte (phase 0), voltage-gated gated sodium channels (I Na ) open at -65 mv. Subsequent influx of Na + leads to depolarisation up to +40 mv and closing of Na + channels. Phase 1 means partial repolarisation carried by diffusion of K + through specific ion channels (I to transient outward ) K + ions diffuse according to both electrical and chemical gradient. In the same time, Ca 2+ long-lasting lasting (I Ca-L ) channels are opened. During phase 0 to 2, heart muscle cell doesn t respond to any new electrical signal refractory period
6 Mechanism of cardiomyocyte activity 2 In phase 2 ( plateau ), prolonged depolarisation is maintained by the influx of Ca 2+ through I Ca-L channels. Unlike I Na or I to, I Ca-L channel is gated both by voltage and receptor mechanism, that responds to vegetative nervous signalisation. Ca 2+ binds to ryanodin receptor of sarcoplasmic reticulum, where it enhances the release of more Ca 2+ into the cytoplasm. Ca 2+ then binds troponin which changes its conformation and stops blocking the actin-myosin interaction. Contraction of muscle fibre follows as in other types of muscles. Another, delayed K + channel (I K ) is open. Finally, with closing of Ca 2+ channel, efflux of K + lowers the voltage inside the cardiomyocyte to the values during diastole (phase 3) Before next repolarisation, Na + ions are pumped outside the cell in exchange for K + by Na/K ATP-ase (3:2). Some Na + ions return inside the cell in change for Ca 2+ through specific exchanger Ca 2+ is also pumped into sarcoplasmic reticulum.the heart muscle gets to diastole
7
8
9

10 Pacemaker cells In pacemaker cells, sympathicus- and parasympathicus- controlled sodium, potassium and calcium channels remain open during the diastole, leading into continual loss of negative voltage up to -65mV, when fast depolarisation begins. Pacemaker cells are present in SA node, AV node and Purkinje fibres
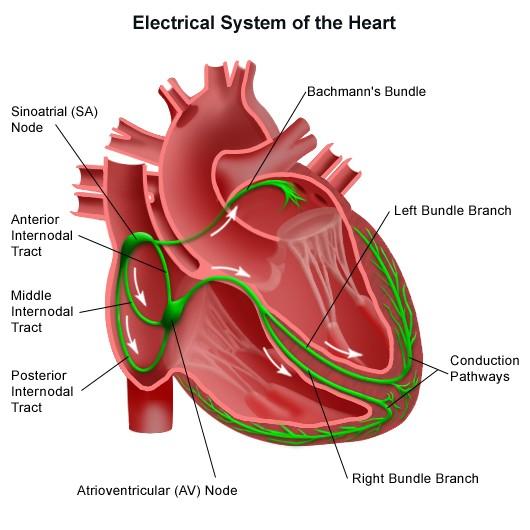
11 Normal conduction within the heart Aorta According to Katzung's Basic & Clinical Pharmacology. McGraw-Hill Medical; 9 edition (December 15, 2003) VC M / 1 SA node Atrial myocardium AV node 1 SA node Bundle of His AV node Purk. fibre Bundle of His ventricle ECG P T U Purkinje fibre QRS Time (s) 0.6
12 Sinoatrial (SA) node Group of pacemaker cells located in the right atrium Under normal circumstances it serves as primary pacemaker of the heart It spontaneously generates electrical impulses at a rate of 60-90/min The SA node is richly innervated by both sympaticus and parasympaticus, which modify the SA node rate and thus heart frequency
13 Atrial conduction system Bachmann s bundle conducts action potentials to the left atrium Internodal tracts (anterior, middle and posterior) run from SA node to AV node, converging near the coronary sinus. Atrial automacity foci are present within the atrial conduction system
14 Atrioventricular (AV) node Area of specialized tissue located between atria and ventricles, near the coronary sinus and tricuspid valve. It serves as secondary pacemaker and is the only way of electric connection between the atria and the ventricles under normal circumstances. AV node consists of 3 zones: AN (atria-nodus), N (nodus) and NH (nodus- His). In AN zone, the conduction gets slower, as there is less sodium channels and slower depolarisation N zone is formed by nodal cells with low voltage (-50mV) slow cells. These cells do not contain sodium channels, their depolarisation is then mediated by Ca 2+. The conduction delays by about 0,12s there. The Ca 2+ I Ca L receptors are influenced by the sympathicus and the parasympathicus. In NH zone, the nuber of sodium channels increase again. The cells of NH zone can take over the function of pacemaker, in the case if no signal from upper parts of the conduction system is present. Its rate is slower than that of SA node: 40-60/min Ca-
15 Bundle of His Part of cardiac tissue specialized for fast electrical conduction that leads the signal from AV-node to working myocardium of the ventricles. After its short course, the Bundle of His branches ito right and left bundle branch (Tawara branches). Right bundle branch is long and thin, thus more vulnerable than the left one Left bundle branch is then divided into the left anterior and left posterior fascicle
, without innervation Jan Evangelista Purkyně (1787-1869), 1869), Czech")
16 Purkinje fibres Terminal part of the conduction system Tertiary pacemaker idioventricular rhythm (20-40/min), without innervation Jan Evangelista Purkyně ( ), 1869), Czech physiologist
17 12-leads ECG (uses 10 electrodes) Electrode placement: RA: On the right arm, avoiding bony prominences. LA: In the same location that RA was placed, but on the left arm this time. RL: On the right leg, avoiding bony prominences. LL: In the same location that RL was placed, but on the left leg this time. V1: In the fourth intercostal space (between ribs 4 & 5) just to the right of the sternum (breastbone). V2: In the fourth intercostal space (between ribs 4 & 5) just to the left of the sternum. V3: Between leads V2 and V4. V4: In the fifth intercostal space (between ribs 5 & 6) in the mid-clavicular line (the imaginary line that extends down from the midpoint of the clavicle (collarbone). V5: Horizontally even with V4, but in the anterior axillary line. (The anterior axillary line is the imaginary line that runs down from the point midway between the middle of the clavicle and the lateral end of the clavicle; the lateral end of the collarbone is the end closer to the arm.) V6: Horizontally even with V4 and V5 in the midaxillary line. (The midaxillary line is the imaginary line that extends down from the middle of the patient s armpit.)

18 12-leads ECG electrode placement


19 Evaluation of electrical signal: Eindhoven s triangle

20 Normal ECG curve
21 Normal Sinus Rhythm Implies normal sequence of conduction, originating in the sinus node and proceeding to the ventricles via the AV node and His-Purkinje system. EKG Characteristics: Regular narrow-complex rhythm Rate bpm Each QRS complex is proceeded by a P wave P wave is upright in lead II & downgoing in lead avr
22 rhythm sinus 60-90/min other junctional 40-60/min idioventricular 30-40/min atrial fibrilation atrial flutter Description of ECG description of waves and intervals electrical axis of the heart action regular irregular frequency normal 60 90/min tachycardia >90/min bradycardia <60/min
, ventricular (V) Mechanism early after depolarisation (EAD), delayed after depolarisation (DAD), re-entry")
23 Arrhythmias: Electrophysiological abnormalities arising from the impairment of the impulse 1. genesis (origin), 2. conduction, 3. both previous Arrhythmias are defined by exclusion - i.e., any rhythm that is not a normal sinus rhythm (NSR, bpm) is an arrhythmia With respect to the Frequency bradyarrythmias vs. tachyarrhythmias Localization supraventricular (SV), ventricular (V) Mechanism early after depolarisation (EAD), delayed after depolarisation (DAD), re-entry
24 Mechanism of Arrhythmia Abnormal heart pulse formation 1. Sinus pulse 2. Ectopic pulse 3. Triggered activity Abnormal heart pulse conduction 1. Reentry 2. Conduct block
25 Possible causes of arrhytmia Vegetative nervous system disorder (nervous lability, compensation of heart failure, shock, anxiety) Ischaemia, hypoxia and reperfusion, ph disorders Disorders of iont balance Disorders of myocardium hypertrophy, dilatation, amyloidosis, scar aftar acute myoacrdial infarction Inflammation Drugs (β-blockers, digitalis, antiarrhytmics) General state (trauma, endokrinopathy..) Genetic causes (ion channel mutations) Aberrant conduction bundle of KENT (WPW syndrom aberrant track between the atria and the ventricles bypassing the AV-node
 Supraventricular (SV) - SV extrasystoles atrial, junction - atrial tachycardia, flutter, fibrillation - AV node re-entry tachycardia (AVNRT) - AV re-entry tachycardia")
26 Brady- and tachyarrhythmias: 1. Bradyarrhythmias - SA block - sick-sinus syndrome - AV block 2. Tachyarrhythmias a) Supraventricular (SV) - SV extrasystoles atrial, junction - atrial tachycardia, flutter, fibrillation - AV node re-entry tachycardia (AVNRT) - AV re-entry tachycardia (Wolf-Parkinson-White syndrome) b) Ventricular - ventricular extrasystoles - ventricular tachycardia - flutter/fibrillation
27 Badyarrhythmias
28 Recognizing altered automaticity on EKG Gradual onset and termination of the arrhythmia. The P wave of the first beat of the arrhythmia is typically the same as the remaining beats of the arrhythmia (if a P wave is present at all).
29 Decreased Automaticity Sinus Bradycardia

30 Sinus Bradycardia HR< 60 bpm; every QRS narrow, preceded by p wave Can be normal in well-conditioned athletes HR can be<30 bpm in children, young adults during sleep, with up to 2 sec pauses
31 Sinus bradycardia - etiologies Normal aging 15-25% Acute MI, esp. affecting inferior wall Hypothyroidism, infiltrative diseases (sarcoid, amyloid) Hypothermia, hypokalemia SLE, collagen vasc diseases Situational: micturation, coughing Drugs: beta-blockers, blockers, digitalis, calcium channel blockers, amiodarone, cimetidine, lithium


32 Increased/Abnormal Automaticity Sinus tachycardia Ectopic atrial tachycardia Junctional tachycardia
33 Sinus tachycardia - etiologies Fever Hyperthyroidism Effective volume depletion Anxiety Pheochromocytoma Sepsis Anemia Exposure to stimulants (nicotine, caffeine) or illicit drugs Hypotension and shock Pulmonary embolism Acute coronary ischemia and myocardial infarction Heart failure Chronic pulmonary disease Hypoxia

34 Sinus Arrhythmia Variations in the cycle lengths between p waves/ QRS complexes Will often sound irregular on exam Normal p waves, PR interval, normal, narrow QRS
35 Sinus arrhythmia Usually respiratory--increase in heart rate during inspiration Exaggerated in children, young adults and athletes decreases with age Usually asymptomatic, no treatment or referral Can be non-respiratory, often in normal or diseased heart, seen in digitalis toxicity Referral may be necessary if not clearly respiratory, history of heart disease
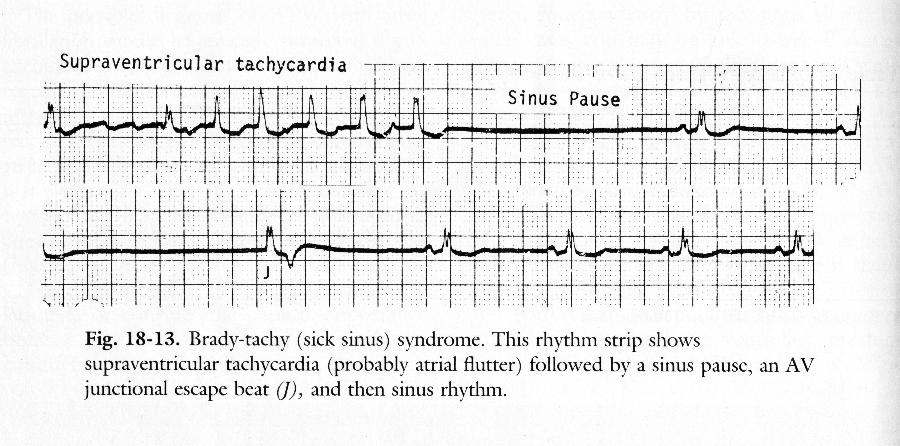
36 Sick Sinus Syndrome All result in bradycardia Sinus bradycardia (rate of ~43 bpm) with a sinus pause Often result of tachy-brady syndrome: where a burst of atrial tachycardia (such as afib) is then followed by a long, symptomatic sinus pause/arrest, with no breakthrough junctional rhythm.
37 Sick Sinus Syndrome - etiology Often due to sinus node fibrosis, SNode arterial atherosclerosis, inflammation (Rheumatic fever, amyloid, sarcoid) Occurs in congenital and acquired heart disease and after surgery Hypothyroidism, hypothermia Drugs: digitalis, lithium, cimetidine, methyldopa, reserpine, clonidine, amiodarone Most patients are elderly, may or may not have symptoms
38

39 Triggered activity Long QT a bradycardia
40 2. Delayed afterdepolarization (DAD)
41 Mechanism of Reentry
42 Mechanism of Reentry
43 Reentrant Rhythms AV nodal reentrant tachycardia (AVNRT) AV reentrant tachycardia (AVRT) Orthodromic Antidromic Atrial flutter Atrial fibrillation Ventricular tachycardia
44 Recognizing reentry on EKG Abrupt onset and termination of the arrhythmia. The P wave of the first beat of the arrhythmia is different from the remaining beats of the arrhythmia (if a P wave is present at all).

45 Example of AVNRT
46 Mechanism of AVNRT
47 Atrial Flutter Most cases of atrial flutter are caused by a large reentrant circuit in the wall of the right atrium EKG Characteristics: Biphasic sawtooth flutter waves at a rate of ~ 300 bpm Flutter waves have constant amplitude, duration, and morphology through the cardiac cycle There is usually either a 2:1 or 4:1 block at the AV node, resulting in ventricular rates of either 150 or 75 bpm

48 Unmasking of Flutter Waves Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 7th ed., In the presence of 2:1 AV block, the flutter waves may not be immediately apparent. These can be brought out by administration of adenosine.
49 Atrial Fibrillation Atrial fibrillation is caused by numerous wavelets of depolarization spreading throughout the atria simultaneously, leading to an absence of coordinated atrial contraction. This kind of rhythm is present in up to 5% of adult population, mostly in older age. It is often connected with other diseases of the heart (ischaemic haert disease, heart failure. Atrial fibrillation is important because it can lead to: Hemodynamic compromise Systemic embolization Symptoms
50 Atrial Fibrillation ECG Characteristics: Absent P waves Presence of fine fibrillatory waves which vary in amplitude and morphology Irregularly irregular ventricular response
51 Ventricular arrhythmia
 and has different")
52 Ventricular extrasystoles (VES) Is caused by either reentrant signaling or enhanced automaticity in some ectopic focus The QRS complex is enlarged (>120ms) and has different shape


53 Coupling of VES Premature ventricular beats occurring after every normal beat are termed ventricular bigeminy, if 2 normal QRS complexes are folloved by VES, we speak of ventricular trigeminy. Two VES grouped together are called a couplet, three a triplet. Runs longer than 3 VES is referred as ventricular tachycardia
54 What is this arrhythmia? Ventricular tachycardia Ventricular tachycardia is usually caused by reentry, and most commonly seen in patients following myocardial infarction.

55 Polymorphic ventricular tachycardia torsades de pointes Is connected with prolonged QT interval. The place of origin of the beats is moving that leads into different shape of QRS

56 Ventricular fibrillation (lethal condition)
57 Conduction Block
58 Rhythms Produced by Conduction Block AV Block (relatively common) 1 st degree AV block Type 1 2 nd degree AV block Type 2 2 nd degree AV block 3 rd degree AV block SA Block (relatively rare)
59 Atrioventricular Block AV block is a delay or failure in transmission of the cardiac impulse from atrium to ventricle. Etiology: Atherosclerotic heart disease; myocarditis; rheumatic fever; cardiomyopathy; drug toxicity; electrolyte disturbance, collagen disease, lev s disease.
60 1 st Degree AV Block The Alan E. Lindsay ECG Learning Center ; ECG Characteristics: Prolongation of the PR interval, which is constant All P waves are conducted

61 2 nd Degree AV Block Type 1 (Wenckebach) EKG Characteristics: Progressive prolongation of the PR interval until a P wave is not conducted. As the PR interval prolongs, the RR interval actually shortens Type 2 EKG Characteristics: Constant PR interval with intermittent failure to conduct

62 3 rd Degree (Complete) AV Block EKG Characteristics: No relationship between P waves and QRS complexes Relatively constant PP intervals and RR intervals Greater number of P waves than QRS complexes
63 SA arrest with compensatory AV activity When the activity of SA node is stopped, AV node takes over the role of pacemaker. Very similar type of arrhythmia is SA block: Pacing in SA node is generated, but not conducted to the myocardium+
64 Intraventricular Block Intraventricular conduction system: 1. Right bundle branch 2. Left bundle branch 3. Left anterior fascicular 4. Left posterior fascicular
65 Intraventricular Block Etiology: Myocarditis, valve disease, cardiomyopathy, CAD, hypertension, pulmonary heart disease, drug toxicity, Lenegre disease, Lev s disease et al. Manifestation: Single fascicular or bifascicular block is asymptom; tri-fascicular block may have dizziness; palpitation, syncope and Adams-stokes stokes syndrome
66 Premature contractions The term premature contractions are used to describe non sinus beats. Common arrhythmia The morbidity rate is 3-5%
67 Atrial premature contractions (APCs) APCs arising from somewhere in either the left or the right atrium. Causes: rheumatic heart disease, CAD, hypertension, hyperthyroidism, hypokalemia Symptoms: many patients have no symptom, some have palpitation, chest incomfortable. Therapy: Needn t therapy in the patients without heart disease. Can be treated with ß-blocker, propafenone, moricizine or verapamil.
68 Ventricular Premature Etiology: Contractions (VPCs) 1. Occur in normal person 2. Myocarditis, CAD, valve heart disease, hyperthyroidism, Drug toxicity (digoxin, quinidine and anti-anxiety anxiety drug) 3. electrolyte disturbance, anxiety, drinking, coffee
69 Pre-excitation excitation syndrome (W-P-W W syndrome) There are several type of accessory pathway 1. Kent: adjacent atrial and ventricular 2. James: adjacent atrial and his bundle 3. Mahaim: adjacent lower part of the AVN and ventricular Usually no structure heart disease, occur in any age individual
70 WPW syndrome Manifestation: Palpitation, syncope, dizziness Arrhythmia: 80% tachycardia is AVRT, 15-30% is AFi, 5% is AF, May induce ventricular fibrillation

71 Wolff-Parkinson White Syndrome (WPW) is a condition in which the heart beats too fast due to abnormal, extra electrical pathways between the heart s atrium and ventriculum.
72 Thank you for your attention
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Paroxysmal Supraventricular Tachycardia PSVT.
 Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
Atrial Tachycardia; is the name for an arrhythmia caused by a disorder of the impulse generation in the atrium or the AV node. An area in the atrium sends out rapid signals, which are faster than those
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
Paramedic Rounds. Tachyarrhythmia's. Sean Sutton Dallas Wood
 Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Paramedic Rounds Tachyarrhythmia's Sean Sutton Dallas Wood Objectives At the end of this session, the paramedic will be able to: State the key components of the cardiac conduction pathway, along with the
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Cardiac Arrhythmias. Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company
 Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
Cardiac Arrhythmias Cathy Percival, RN, FALU, FLMI VP, Medical Director AIG Life and Retirement Company The Cardiovascular System Three primary functions Transport of oxygen, nutrients, and hormones to
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Pathologic ECG. Adelina Vlad, MD PhD
 Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Pathologic ECG Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze the morphology and
Module 1: Introduction to ECG & Normal ECG
 Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
Module 1: Introduction to ECG & Normal ECG Importance of Correct anatomical positions Measurements & Morphologies ONLY accurate if Precise anatomical positions adhered to Standardised techniques are used
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ELECTROCARDIOGRAPHY (ECG)
") ELECTROCARDIOGRAPHY (ECG) The heart is a muscular organ, which pumps blood through the blood vessels of the circulatory system. Blood provides the body with oxygen and nutrients, as well as assists in
ELECTROCARDIOGRAPHY (ECG) The heart is a muscular organ, which pumps blood through the blood vessels of the circulatory system. Blood provides the body with oxygen and nutrients, as well as assists in
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
THE CARDIOVASCULAR SYSTEM. Heart 2
 THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
THE CARDIOVASCULAR SYSTEM Heart 2 PROPERTIES OF CARDIAC MUSCLE Cardiac muscle Striated Short Wide Branched Interconnected Skeletal muscle Striated Long Narrow Cylindrical PROPERTIES OF CARDIAC MUSCLE Intercalated
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Pediatrics. Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment. Overview
 Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Pediatrics Arrhythmias in Children: Bradycardia and Tachycardia Diagnosis and Treatment See online here The most common form of cardiac arrhythmia in children is sinus tachycardia which can be caused by
Introduction. Circulation
 Introduction Circulation 1- Systemic (general) circulation 2- Pulmonary circulation carries oxygenated blood to all parts of the body carries deoxygenated blood to the lungs From Lt. ventricle aorta From
Introduction Circulation 1- Systemic (general) circulation 2- Pulmonary circulation carries oxygenated blood to all parts of the body carries deoxygenated blood to the lungs From Lt. ventricle aorta From
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Lecture outline. Electrical properties of the heart. Automaticity. Excitability. Refractoriness. The ABCs of ECGs Back to Basics Part I
 Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
Lecture outline The ABCs of ECGs Back to Basics Part I Meg Sleeper VMD, DACVIM (cardiology) University of Florida Veterinary School Electrical properties of the heart Action potentials Normal intracardiac
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Where are the normal pacemaker and the backup pacemakers of the heart located?
 CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
CASE 9 A 68-year-old woman presents to the emergency center with shortness of breath, light-headedness, and chest pain described as being like an elephant sitting on her chest. She is diagnosed with a
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
BASIC PRINCIPLES OF ECG INTERPRETATION
 Chapter 1 BASIC PRINCIPLES OF ECG INTERPRETATION Cardiac rhythm analysis may be accomplished informally via cardiac monitoring and more diagnostically via a 12-lead electrocardiogram (ECG). An electrocardiogram
Chapter 1 BASIC PRINCIPLES OF ECG INTERPRETATION Cardiac rhythm analysis may be accomplished informally via cardiac monitoring and more diagnostically via a 12-lead electrocardiogram (ECG). An electrocardiogram
a lecture series by SWESEMJR
 Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Arrhythmias Automaticity- the ability to depolarize spontaneously. Pacemakers: Sinoatrial node: 70 bpm AV-nodal area: 40 bpm His-Purkinje: 20-40 bpm it Mechanisms of arrhythmias 1. Increased automaticity
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1
 usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1") If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
If the P wave > 0.12 sec( 3 mm) usually in any lead. Notched P wave usually in lead I,aVl may be lead II Negative terminal portion of P wave in V1, 1 mm depth and 3 mm width( most specific) Since Mitral
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Cardiac Telemetry Self Study: Part One Cardiovascular Review 2017 THINGS TO REMEMBER
 Please review the above anatomy of the heart. THINGS TO REMEMBER There are 3 electrolytes that affect cardiac function o Sodium, Potassium, and Calcium When any of these electrolytes are out of the normal
Please review the above anatomy of the heart. THINGS TO REMEMBER There are 3 electrolytes that affect cardiac function o Sodium, Potassium, and Calcium When any of these electrolytes are out of the normal
PATIENT S NAME, DATE/TIME,
 ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
ECG and Arrhythmias Dec, 1 st 2014 Doctor Mohammad Jarrah References: - Lecture and Slides - ECG Made Easy - Davidson Principles of Medicine - First Aid Cases for the USMLE Step 1 - Mini-OSCE Archive ECG
KNOW YOUR ECG. G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada
 KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
Chapter 20 (2) The Heart
 The Heart") Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
Chapter 20 (2) The Heart ----------------------------------------------------------------------------------------------------------------------------------------- Describe the component and function of
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Appendix. Table 1: Causes for abnormal axis deviation Left axis deviation
 Appendix Table 1: Causes for abnormal axis deviation Left axis deviation Normal variant (2 5%) Left anterior fascicular block Left ventricular hypertrophy Inferior wall myocardial infarction Primum atrial
Appendix Table 1: Causes for abnormal axis deviation Left axis deviation Normal variant (2 5%) Left anterior fascicular block Left ventricular hypertrophy Inferior wall myocardial infarction Primum atrial
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida
 S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
Conduction disorders
 Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Conduction disorders L.V. Bogun, N.I. Yabluchansky, F.M. Abdueva, O.Y. Bichkova, A.N. Fomich, P.A. Garkavyi, A.L. Kulik, N.V. Lysenko, N.V. Makienko, L.A. Martimyanova, I.V. Soldatenko, E.E. Tomina Department
Cardiac Cycle. Each heartbeat is called a cardiac cycle. First the two atria contract at the same time.
 The Heartbeat Cardiac Cycle Each heartbeat is called a cardiac cycle. First the two atria contract at the same time. Next the two ventricles contract at the same time. Then all the chambers relax. http://www.youtube.com/watch?v=frd3k6lkhws
The Heartbeat Cardiac Cycle Each heartbeat is called a cardiac cycle. First the two atria contract at the same time. Next the two ventricles contract at the same time. Then all the chambers relax. http://www.youtube.com/watch?v=frd3k6lkhws
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CARDIOVASCULAR SYSTEM
 CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
CARDIOVASCULAR SYSTEM Overview Heart and Vessels 2 Major Divisions Pulmonary Circuit Systemic Circuit Closed and Continuous Loop Location Aorta Superior vena cava Right lung Pulmonary trunk Base of heart
ARRHYTHMIAS. Zuzana Charvátová
 ARRHYTHMIAS Zuzana Charvátová 24. 10. 2017 ARRHYTMIAS = abnormalities of heart rhythm presence of any heart rhythm different from physiologic sinus rhythm various spectrum of clinical importance A. myocardial
ARRHYTHMIAS Zuzana Charvátová 24. 10. 2017 ARRHYTMIAS = abnormalities of heart rhythm presence of any heart rhythm different from physiologic sinus rhythm various spectrum of clinical importance A. myocardial
ECG WORKBOOK. Rohan Jayasinghe
 ECG WORKBOOK Rohan Jayasinghe Contents Preface vii Foreword viii Acknowledgements ix The author x Reviewers xi Section 1 Basics of the ECG 1 Section 2 ECG-based diagnosis: pathology by ECG 21 Section 3
ECG WORKBOOK Rohan Jayasinghe Contents Preface vii Foreword viii Acknowledgements ix The author x Reviewers xi Section 1 Basics of the ECG 1 Section 2 ECG-based diagnosis: pathology by ECG 21 Section 3
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
V. TACHYCARDIAS Rapid rhythm abnormalities
 V. TACHYCARDIAS Rapid rhythm abnormalities Tachyarrhythmias currently account for up to 350,000 deaths annually in the US. In addition to these clearly dangerous rhythm disturbances, other forms of more
V. TACHYCARDIAS Rapid rhythm abnormalities Tachyarrhythmias currently account for up to 350,000 deaths annually in the US. In addition to these clearly dangerous rhythm disturbances, other forms of more
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017
 CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.