Acute Coronary Syndrome refers to any
|
|
|
- Barbara Weaver
- 6 years ago
- Views:
Transcription



1 IMPACTING THE CLOTTING CASCADE: PRACTICE IMPLICATIONS FOR ANTICOAGULANT AND ANTIPLATELET PHARMACOLOGY Cynthia L. Webner DNP, CCNS, ACNPC-AG, CCRN-CMC, CHFN NTI Class Code A75m462 Acute Coronary Syndrome refers to any rupture of plaque or thrombotic event that leads to symptomatic ischemia or infarction. 2 STEMI NSTE-ACS 1

* NSTE Abciximab (Repro) ADP Receptor Blockers Clopidogrel Prasugrel Ticagrelor Thromboxane A 2 Inhibitor ASA VTE:")
2 3 Drugs Used to Alter Clotting in ACS Fibrinolytics STEMI tpa Alteplase Retaplase Tenecteplase Streptokinase (no longer used) Anticoagulants o STEMI / NSTE-ACS o Unfractionated Heparin o Low Molecular Weight Heparin o Direct Thrombin Inhibitor o Factor Xa Inhibitor (IV/SQ) Antiplatelets STEMI / NSTE-ACS GP IIb/ IIIa Inhibitors Eptifibitide (Integrelin)* NSTE Tirofiban (Aggrastat)* NSTE Abciximab (Repro) ADP Receptor Blockers Clopidogrel Prasugrel Ticagrelor Thromboxane A 2 Inhibitor ASA VTE: PE / DVT 2

3 Long Term Drugs Used in VTE VTE no Cancer Dabigatran Rivaroxaban Apixaban Edoxaban Warfarin Low Molecular Weight Heparin VTE with Cancer Low Molecular Weight Heparin Warfarin Dabigatran Rivaroxaban Apixaban Edoxaban Fibrinolytic therapy recommended for PE with hypotension systemic versus catheter directed. Parenteral anticoagulation may be used initially. 6 Atrial Fibrillation Lack of coordinated atrial activity (no consistent P waves) Irregular, chaotic atrial f waves Irregularly irregular ventricular response 3
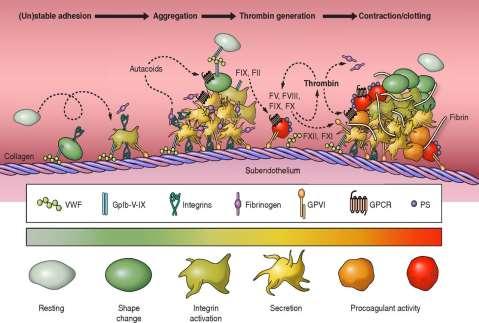
4 7 Anticoagulants in Cardiac Disorders Warfarin Vitamin K antagonist Dabigatran Direct thrombin inhibitor Rivaroxaban Factor Xa inhibitor Apixaban Factor Xa inhibitor Edoxaban Factor Xa inhibitor 8 Clot Formation: Clotting Cascade Initiated by vascular injury and direct exposure to collagen Site of activated platelet Site of endothelial damage Subendothelial layer where collogen is exposed From initiation to a clot is 2-6 minutes Measured by APTT Initiated by endothelial release (secondary to tissue injury) of thromboplastin tissue factor From initiation to clot is 15 to 20 seconds Measured by Protime 4
5 9 The Clotting Cascade Intrinsic Pathway Extrinsic Pathway XII XIIa Thromboplastin Tissue Factor III VII Activated platelets Endo damage Exposed collagen XI XIa Activated platelets Endo /tissue damage VIIa Common Pathway IX X IXa Xa Phospholipid Calcium VIIIa Va X II Prothrombin IIa Thrombin Fibrinogen Fibrin Fibrin Stable Clot 10 The Clotting Cascade Intrinsic Pathway XII XIIa XI XIa Warfarin IX IXa Fondaparinox Rivaroxaban Apixaban Edoxaban Extrinsic Pathway TF III VII VIIa Common Pathway UFH LMWH X Xa II Prothrombin Fibrinogen Va IIa Thrombin Fibrin X Bivalrudin Dibigitran Lirudin Argatroban Fibrin Stable Clot 5

6 11 Unfractionated Heparin Works in the intrinsic and common pathway Antithrombin activator that inhibits factors Xa and IIa (thrombin) Antithrombin III lyses factor Xa and thrombin and inhibits clotting When heparin binds with antithrombin III the inhibition is increased 1000 times Concern that unfractionated heparin results in platelet activation - although thrombin is a strong platelet activator and heparin is an antithrombin drug Anticoagulation is almost instant ½ life relatively short Antidote: Protamine 1 mg per 100 units In NSTEMI: continue for 48 hours or until PCI 12 6
7 Unfractionated Heparin Dosing Initial load of 60 u/kg IV Maximum 4000U Initial infusion is 12u/kg/hr Maximum is 1000 u/hr Continue 48 hours or until PCI is performed Prophylaxis 5000 u SC q8-12 hours Acute DVT or PE Initial load of 80 u/kg IV Alternative 5000U Initial infusion is 18u/kg/hr Alternative is 1000 u/hr Use of unfractionated heparin in atrial fibrillation is off label 14 More About Heparin Different dose and aptt for ACS versus venous thrombotic event aptt (activated partial thromboplastin time) is used to monitor effectiveness and safety Goal is aptt 1.5-2Xs the control Weight based heparin dosing reaches goal 90% of time compared to 77% with standard therapy OR Anti factor Xa levels IU/ml Baseline aptt, PT/INR, platelets and CBC Increased bleeding can occur with renal failure Heparin has dual clearance mechanism 7
8 15 Complications of Heparin Bleeding Mild thrombocytopenia HIT 1 Mild thrombocytopenia occurs in 10-20% of patients Severe thrombocytopenia HIT 2 occurs in 1-2% of patients Heparin Induced Thrombocytopenia (HIT) Platelet aggregation resulting in venous or arterial thrombosis (HITT Thrombocytopenia with thrombosis) Determining patients at risk is unpredictable Generally occurs 5 to 10 days after initiation of heparin Could be sooner if recent exposure to heparin DC heparin if platelets fall below 100,000 (or > 50% reduction from baseline) Severe thrombocytopenia is due to an immune response More on Heparin Induced Thrombocytopenia 16 Immune system forms antibodies against heparin when bound to protein platelet factor 4 [PF4] antibodies bind to PF4-heparin complexes and induce platelet activation Immunoassay identify antibodies against PF4 Detected in ELISA testing Function Assay Heparin-induced platelet aggregation assay (HIPA) Platelet activation test HIT antibodies are usually IgG class Take 5 days to form IgG antibodies associated with platelet activation and increased thrombin generation Antibodies not necessarily associated with thrombotic risk Can disappear 3 months after exposure Antibodies bind to platelets and trigger the development of thrombosis. 8
9 17 Treatment of HIT 1. Discontinue and avoid all heparin. 2. Give a non-heparin alternative anticoagulant: Direct thrombin inhibitors. 3. Postpone warfarin pending substantial platelet count recovery (give vitamin K if warfarin has already been started). Warfarin is associated with protein C deficiency and increased risk for microthrombosis 4. Avoid platelet transfusions leads to platelet activation. 5. Test for HIT antibodies (ELISA and washed assay) 6. Investigate for lower-limb deep-vein thrombosis. 18 Low Molecular Weight Heparin Enoxaparin, dalteparin, tinzaparin, and nadroparin Smaller in size Antithrombin by inhibiting factor Xa Causes less inactivation of thrombin and less bleeding than standard heparin More predictable anticoagulant response No need to monitor APTT Anti Xa levels can be drawn 4 hours after SQ dose Lower incidence of heparin induced thrombocytopenia Less platelet activation concern than with UFH 9
10 19 Low Molecular Weight Heparin Can be self administered with Sub Q administration ½ life 4-6 hours Protamine reverses 60% of drug effect Renal failure results in increased risk of bleeding because LMWH is renally cleared Special dosing for chronic renal insufficiency with enoxaparin 20 Enoxaparin Dosing Prevention of DVT 40 mg SC daily in most situations 30 mg SC daily for renal adjustment (CR Clearance < 30 ml/min) NSTE-ACS (or as adjunct in STEMI) 1 mg/kg SC q12 hours 1mg/kg SC daily if CR Clearance < 30 ml/min IV loading dose of 30 mg in select patients Continued for duration of stay or until PCI Embolism with Atrial Fib 1 mg/kg SC q12 hours Venous thrombosis / DVT 1mg/kg SC q12 or 1.5 mg/kg daily depending of specific circumstances 10
11 Enoxaparin Administration Full length of 27 gauge ½ needle (prepackaged) should be injected Skin fold held until needle withdrawn Use anterolateral or posterorlateral walls of abdomen Rotate sites frequently Do not massage site 22 Direct Thrombin Inhibitor Ability to inactivate fibrin bound thrombin Less binding to plasma proteins, therefore more reliable anticoagulation effect Indications HIT /HITT Approved in NSTE-ACS (Use only in patients with early invasive strategy) / PCI Non inferior to heparin with a GPIIb/IIIa with less bleeding Monitor in the cath lab with ACT Lipirudin / desirudin (hirudin) Argatroban Bivalirudin* 0.10 mg/kg loading 0.25 mg/kg per hour Until diagnostic angiography or PCI is performed 11
12 23 Synthetic Factor Xa Inhibitor Fondaparinux (Arixtra) Neutralizes Factor Xa and interrupts the clotting cascade Does not inhibit thrombin No reported HIT / HITT Indications Venous thromboembolism and PE DVT prophylaxis ACS Contraindicated in severe renal dysfunction No laboratory monitoring is needed PT/aPTT not sensitive No antidote (Recombinant factor VIIa can help reverse anticoagulation effect) Synthetic Factor Xa Inhibitor DVT Prophylaxis: 2.5mg SC once daily in adults > 50 kg ACS 2.5 mg SC daily for duration of hospital stay up to 8 days or until time of revascularization If STEMI an initial dose 2.5mg should be given IV before starting daily SC Cannot be used as sole anticoagulant during PCI add DTI or UH Acute DVT or PE weight based for between 5mg and 10mg SC daily Can use as a bridge for 5-7 days if warfarin is long term anticoagulation choice Start warfarin on day 1 or 2 but continue Fondaparinux for at least 24 hours after therapeutic INR is achieved 12
13 26 13

14 27 New Dual Antiplatelet Therapy Guidelines Update STEMI PCI NSTE CABG Stable Ischemic CAD Non Cardiac Surgery Figure 1. Master Treatment Algorithm for Duration of P2Y 12 Inhibitor Therapy in Patients With CAD Treated With DAPT ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. 14


15 Figure 2. Treatment Algorithm for Duration of P2Y 12 Inhibitor Therapy in Patients Treated With PCI ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. Figure 3. Treatment Algorithm for Management and Duration of P2Y 12 Inhibitor Therapy in Patients Undergoing CABG ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. 15


16 Figure 4. Treatment Algorithm for Duration of P2Y 12 Inhibitor Therapy in Patients With SIHD (Without ACS Within the Past Several Years) ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. Figure 5. Treatment Algorithm for Duration of P2Y 12 Inhibitor Therapy in Patient With Recent ACS (NSTE-ACS or STEMI) ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. 16
17 Figure 6. Treatment Algorithm for the Timing of Elective Noncardiac Surgery in Patients With Coronary Stents ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. Factors Used to Calculate a 34 DAPT Score Variable Points Age 75 y -2 Age 65 to <75 y -1 Age <65 y 0 Current cigarette smoker Diabetes mellitus 1 MI at presentation 1 1 A score of 2 is associated with a favorable benefit/risk ratio for prolonged DAPT while a score of <2 is associated with an unfavorable benefit/risk ratio. Prior PCI or prior MI Stent diameter <3 mm Paclitaxel-eluting stent CHF or LVEF <30% Saphenous vein graft PCI Levine GN, Bittl JA, Brindis RG, et al. ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease. J Am Coll Cardiol ; doi= /j.jacc
18 35 Aspirin Diminishes platelet reactivity Produces rapid clinical antithrombotic effect caused by immediate and near-total inhibition of thromboxane A2 production (released with vascular injury). Thromboxane A2 is a potent vasocontrictor Inhibits COX1 and COX2 NSAIDS reversibly bind to COX1 preventing inhibition by ASA and may cause prothromotic events Inhibits the endothelium s production of prostaglandin I 2 which decreases platelet aggregation and induces vasodilation. Prostaglandin I 2 is also involved in inflammation. Reduces mortality Increase myocardial oxygen supply Use in ACS Administered as soon as possible after presentation Initial dose: 162 mg to 325 mg chewed (non-enteric coated) Long Term: 81 mg daily If ASA intolerant load with clopidogrel and then daily dose 36 P2Y 12 Receptor Inhibitors / ADP Receptor Blockers Clopidogrel (Plavix) 600 mg initial dose 75 mg daily Prasugrel (Effient) 60 mg initial dose 10mg daily Contraindicated: > 75, < 60 kg, previous TIA, CVA Ticagrelor (Brilinta) 180mg initial dose 90mg twice daily Not to be given with ASA doses > 100mg Adenosine Diphosphate (ADP) - Stored in platelets and released upon platelet activation ADP interacts with P2Y 12 chemoreceptors to enhance adhesiveness and aggregation of platelets through the activation of the GP IIb/IIIa pathway 18
19 37 P2Y 12 Receptor Inhibitors / ADP Receptor Blockers Thienopyridines Clopidogrel Prasugrel Non thienopyridine Ticagrelor 38 Thienopyridines Thienopyridines are a class of ADP / P2Y 12 receptor blockers Clopidogrel (Plavix) Prasugrel (Effient) Irreversibly inhibits P2Y 12 receptor 19
20 Clopidogrel Indications Alternative to ASA therapy in those who cannot take ASA Option in NSTE-ACS for the second antiplatelet agent Ticagrelor and prasugrel have upgraded indications Recommended agent in elective PCI with bare metal stent 40 Clopidogrel Issue of Non Responders ACCF/AHA Clopidogrel Clinical Alert FDA Boxed Warning March 2010 Role of genotype testing or routine platelet function testing Class II b recommendation pending results of randomized controlled clinical trials. Prodrug 2 step process Involves several CYP450 isoenzymes CYP2C19 isoenzyme responsible for almost half of the first step formation 3 major genetic polymorphisms are associated with loss of function Observational studies have shown an association between an increased risk of adverse cardiovascular events and the presence of one nonfunctioning allele 20
21 41 Clopidogrel and PPIs 11/8/2010: Expert Consensus Document Using proton pump inhibitors (PPIs) and antiplatelet drugs (thienopyridines) together is an appropriate way of treating patients with cardiovascular (CV) disease who are at high risk of upper gastrointestinal (GI) bleeds, despite recent concerns about an adverse interaction between these two types of drugs, according to an Expert Consensus Document released jointly today by the American College of Cardiology (ACC), the American College of Gastroenterology (ACG), and the American Heart Association (AHA). 42 Clopidogrel and PPIs 2012: World Journal of Gastroenterology Because PPI induced risk reduction clearly overweighs the possible adverse cardiovascular risk in patients with high risk of gastrointestinal bleeding, combination of clopidogrel with the less CYP2C19 inhibiting pantoprazole should be recommended. Several pharmacodynamic studies found a significant decrease of the clopidogrel platelet antiaggregation effect for omeprazole, but not for pantoprazole. More recent RCT and retrospective co-hort studies have not resulted in same concerns with PPIs as observational studies suggested. 21
22 43 Prasugrel TRITON TIMI 38 Trail 13,608 patients with moderate to high risk ACS all referred for PCI; 3,534 STEMI Randomized to clopidogrel 300mg load and 75mg daily or prasurgrel 60mg load and 10mg daily Median follow up 14 ½ months Prasugrel (compared to Clopidogrel) associated with Significant 2.2% reduction in absolute risk and a 19% reduction in relative risk in the composite endpoint of death due to CV disease, nonfatal MI, or nonfatal stroke during the follow up period Significant increase in TIMI major hemorrhage (1.8% vs 2.4%) Prasugrel approved 2009 Wiviott et al., Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2007; 357: Prasugrel TRILOGY Prasugrel versus clopidogrel in patients with NSTEMI or unstable angina who were not treated with PCI 7,243 patients No statistically significant difference in primary outcome (composite of: death from cardiovascular causes, myocardial infarction, or stroke) among patients under the age of 75 years A weak trend toward a reduced risk in the prasugrel group after 12 months (P = 0.07) Rates of severe and intracranial bleeding were similar in the two groups in all age groups. This is different than TRITON TIMI 38. Dose was adjusted in Trilogy for weight < 60 kg and age > 75 years. Conclusion: More research needed Higher recommendation for prasugrel in NSTE over clopidogrel in early invasive option only 22
23 45 Take Away Prasugrel Points Less concern with PPI administration Less concern regarding non responders Prodrug but not as dependent on CYP2C19 isoenzyme Only used in patients with planned PCI No benefit to administration before the time of angiography Increased bleeding risk > 75 years old <60 KG Cannot be used: Previous CVA / TIA 46 Ticagrelor (Non-Thienopyridine) Reversibly binds to P2Y 12 receptor Not a PRO drug: does not requiring metabolic activation FDA approved July 2011 Prevention of thrombotic events in patients with acute coronary syndromes. Loading dose 180 mg then 90 mg twice daily Contraindicated in history of intracranial bleeding, active pathological bleeding, severe hepatic impairment Higher recommendation for ticagrelor in NSTE over clopidogrel in either ischemia guided or early invasive option 23
24 47 Clopidogrel versus Ticagrelor PLATO trial Better anti-ischemic effect compared to clopidogrel No significant increase in major bleeding Faster onset and shorter duration than clopidogrel (known as reversible mode of action) BID dosing is a potential concern for compliance North American effect thought to be due to higher dose ASA Must not be given with maintenance ASA doses > 100mg Although shorter ½ life recommendation to be held 5 days before surgery. Wallentin, L. et al., Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med; 361: Take Aways NOVEL ORAL ANTICOAGULANTS NOAC 24
25 49 Anticoagulants in Cardiac Disorders Warfarin Vitamin K antagonist Dabigatran Direct thrombin inhibitor Rivaroxaban Factor Xa inhibitor Apixaban Factor Xa inhibitor Edoxaban Factor Xa inhibitor 50 CHA 2 DS 2 VASc to Prevent Stroke in AF C HF or LVEF < 35% H Hypertension A 2 < 65 (0), 65 to 74 (1), and > 75 (2) D Diabetes Mellitus S 2 Stroke, TIA, or Thromboembolism (2) VA Vascular Disease Sc Gender (Female = 1) 25
26 51 Point 1 In assessing risk of stroke in a patient with nonvalvular AF, the writing committee recommends (Class I) the usage of the CHA 2 DS 2 -VASc (C=congestive heart failure; H=hypertension; A 2 =age 75 years [doubled]; D=diabetes mellitus; S 2 =stroke, transient ischemic attack, or thromboembolism (doubled); V=vascular disease; A=age years; Sc=sex category, i.e., female gender) score, as opposed to the CHADS 2 score. 52 Point 2 For nonvalvular AF patients with a history of stroke or transient ischemic attack, or a CHA 2 DS 2 -VASc score 2, oral anticoagulation is recommended (Class I). Options for oral anticoagulation include warfarin, dabigatran, rivaroxaban, and apixaban. 26
27 53 Point 3 For patients with nonvalvular AF and a CHA 2 DS 2 -VASc score of 0, it is reasonable to omit antithrombotic therapy (Class IIa). 54 Point 4 The following options may be considered with a patient with nonvalvular AF and a CHA 2 DS 2 -VASc score of 1: no antithrombotic therapy, oral anticoagulation, or aspirin (Class IIb). 27
28 55 Point 5 None of the new novel oral anticoagulants (dabigatran, rivaroxaban, or apixaban) are recommended to be used in patients with AF and a mechanical or bioprosthetic heart valve (Class III harm). 56 Point 6 Oral anticoagulation should be prescribed to patients with hypertrophic cardiomyopathy and AF irrespective of the CHA 2 DS 2 -VASc score (Class I). 28
29 57 Preventing Thromboembolism Warfarin established as gold standard Eliminates excess rates of ischemic stroke, reduces stroke severity and reduces post stroke mortality Target INR of Superior to ASA and ASA plus clopidogrel Warfarin in atrial fibrillation in stable CAD Warfarin in atrial fibrillation post ACS / PCI 58 Oral anticoagulants with predictable doseresponse relationship: No lab monitoring of coagulation status needed 29
30 59 Drug Dabigatran A Fib Study RE-LY trial (Connolly et al, 2009) Highlights: Note all studies tested for primary endpoint of stroke (ischemic and hemorrhagic) and systemic embolism 150 mg BID superior to warfarin (p< 0.001) (stroke / systemic embolism) Ischemic stroke and hemorrhagic stroke both lower Rate of major bleeding same (potential concern for GI bleeding) Did not test approved 75 mg dose 32 to 33% of patients with CHADS2 score > 2 Rivaroxaban ROCKET AF (Patel et al., 2011) Non-inferiority of rivaroxaban (P<0.001) (stroke / systemic embolism) No significant difference in the risk of major bleeding, intracranial and fatal bleeding occurred less frequently in the rivaroxaban group 87% to 86.9% had CHADS2 score > 3 Drug Abixaban A Fib Study ARISTOTLE (Granger et al., 2011.) Highlights: Note all studies tested for primary endpoint of stroke (ischemic and hemorrhagic) and systemic embolism Primary objective: Found to be non inferior to warfarin (p = <0.001) Secondary objective: Found to be superior to warfarn (p= 0.01) Major bleeding: Statistically less with apixaban (p<0.001) Interesting: No statistical difference in ischemic stroke. Edoxaban ENGAGE AF- TIMI 48 Non-inferior to warfarin (P = < 0.001) for high dose and (P = 0.005) for low dose Significantly lower rates of bleeding & CV death compared to warfarin at both doses (Not less GI bleeding) 30
31 61 Newer Oral Agents Generic Peak Plasma Level Elimination Half-life Clearance Dabigatran 1.5 hours 12 to 18 hours Mostly by kidneys Rivaroxaban 3 hours 5-9 hours (up 11 to 13 hours if > 75 years old) Hepatic and renal excretion Abixaban 3-4 hours 8 to 15 hours 25% cleared by the kidneys Edoxaban 1-2 hours hours Concern in patients with normal renal function Generic Trade Name Class Dabigatran Pradaxa Direct thrombin inhibitor Rivaroxaban Xarelto Factor Xa inhibitor Abixaban Eliquis Factor Xa inhibitor Dosing for Atrial Fibrillation 150 mg PO BID 75 mg PO BID with Cr. Cl. 15 to 30 ml/minute CrCl: < 15 ml/m not recommended Dose 20 mg PO daily CrCl: ml/m 15 mg BID CrCl: < 15 ml/m not recommended ESRD: Avoid Dose: 5 mg BID Dose: 2.5 mg BID with any two of the following > 80 years of age Creatinine > 1.5 mg/dl Weight < 60 kg 62 Edoxaban Savaysa Factor Xa inhibitor 60 mg daily for Cr. Cl. > 50 to < mg daily for Cr. Cl. 15 to 50 CrCl: > 95 ml/m do not use ENGAGE AF-TIMI 48 31
32 Generic Trade Name Class Dabigatran Pradaxa Direct thrombin inhibitor Rivaroxaban Xarelto Factor Xa inhibitor Abixaban Eliquis Factor Xa inhibitor Edoxaban Savaysa Factor Xa inhibitor Dosing VTE / DVT Prophylaxis VTE: 150mg BID AFTER 5-10 days of parenteral anticoagulation DVT Prophylaxis: 110mg initial dose then 220 mg daily VTE: 15 mg BID x 21 days then 20mg daily DVT Prophylaxis: 10mg daily CrCl: < 30 ml/min Do not use CrCl:> 30 ml/min and > 65 years decrease dose VTE:10 mg BID x 7 days then 5mg BID after 6 months 2.5mg BID. Patients with serum creatinine > 2.5 mg/dl or CrCl <25 ml/m were excluded from clinical trials VTE: 60 mg daily AFTER days of parenteral anticoagulation < 60 kg 30mg daily CrCl: ml/m 30 mg daily CrCl: < 15 ml/m not recommended CrCl: < 30 ml/min in age > 65 years not recommended Hold Times for Newer Oral Agents 64 Surgery with high risk for bleeding (i.e. CABG) Dabigatran 3 to 5 days. For urgent cases until clotting times are normal or until four half-lives has passed Hold times for surgery are dependent on renal function DO NOT USE INR. Can be falsely elevated Rivaroxaban / Apixaban Renal impairment Cr. Cl.: > 50 = 3 days Cr. Cl. < 50 = 4 days Liver impairment Mild: 2 days Mod: At least 4 days Severe: At least 7 days Surgery Low Bleeding Risk Minimum hold time for low risk surgery and normal renal function is > 24 hours Renal impairment Cr. Cl.: > 50 = 1 days Cr. Cl. < 50 = 3 days Liver impairment Mild: 1 day Mod: At least 2 days Severe: At least 5 days Edoxaban Not specifically addressed in product information. Minimum hold time of at least 24 hours 32
33 Assessment of Bleeding Risk 65 Dabigatran Bleeding risk can be assessed by an ecarin clotting time if available If not available, a PTT can be assessed to determine clearance of the drug because dabigatran has been shown to prolong aptt (aptt not used for quantitative assessment) > 2 x upper normal limit 12 to 24 hours after drug may be indicative of high risk for bleeding Thrombin time is most sensitive test. Diluted thrombin time (DTT) is a quantitative test (calibrated Hemoclot ) Rivaroxaban Apixaban Edoxaban PT may provide qualitative assessment of presence of factor Xa; not sensitive for quantitative anticoagulation effect Point of care INR should not be used to gauge anticoagulation effects Chromogenic assay can provide quantitative assessment not widely available, not fully studied, not recommended at this time 66 Antidotes Dabigatran 19 October 2015FDA Approves Praxbind (idarucizumab), Specific Reversal Agent for Pradaxa (dabigatran etexilate) Two 2.5g doses administered no more than 15 minutes aparts Factor Xa Inhibitors Andexanet alfa breakthrough therapy desgination by FDA; orphan drug status Thrombin generation restored in 100% vs 11% of the participants (P<0.001) within 2 to 5 minutes. Should have FDA decision August 16 th 33

34 67 68 Preoperative Discontinuation Time Frames for Drugs Impacting Coagulation Drug Aspirin Clopidogrel Prasugrel Ticagrelor Discontinuation Time Frame Not discontinued in patients with ACS. Reasonable to continue 81mg in all patients up to surgery. > 5 days prior to surgery; 3 days prior to off pump CABG may be acceptable; at least 24 hours prior to urgent surgery > 7 days prior to surgery > 5 days prior to surgery, 24 to 36 hours if urgent surgery Tirofiban and Eptifibatide Abciximab Warfarin Dabigatran Rivaroxaban Apixaban Unfractionated heparin Low molecular weight heparin Fondaparinux Bivalirudin 2 to 4 hours prior to surgery 12 to 24 hours prior to surgery 4 to 5 days prior to surgery 5 days 2 to 4 days based on age and renal function. Longer hold times for hepatic impairment. > 2 days Continued up until time of surgery in patients with ischemia. Discontinued 4 hours prior to surgery when used for bridging. 18 to 24 hours prior to surgery At least 48 hours prior to surgery 1 to 2 hours, can be given up to the time of surgery if necessary Sources: Ballantyne, 2013a; Ballantyne, 2013b; Lexicomp, 2013; Ferraris et al., 2012; Ferraris et al., 2011; Hillis et al., 2011; Bojar,



35 My Vision: 69 Practice with Joy. Impact every patient and family on their journey and provide safe passage by meeting them where they are, connecting with them in a meaningful way, and delivering care with wisdom and intention. - Karen 70 BE THE BEST THAT YOU CAN BE EVERY DAY. YOUR PATIENTS ARE COUNTING ON IT! Handouts are available on NTI Network and at 35
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation Management Around Endoscopy: GI Perspective. Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017
 Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Anticoagulation Management Around Endoscopy: GI Perspective Nathan Landesman, DO FACOI Flint Gastroenterology Associates October 11, 2017 EDUCATIONAL OBJECTIVES Understand risks of holding anticoagulation
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Antiplatelets and Anticoagulants. Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center
 Antiplatelets and Anticoagulants Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center Mechanism 2 http://www.medicinehack.com/2011/07/virchows-triad.html Mechanism 3 http://drtedwilliams.net/kb/index.php?pagename=coagulation%20cascade
Antiplatelets and Anticoagulants Helen Leung, PharmD PGY1 Pharmacy Resident Memorial Hermann-Texas Medical Center Mechanism 2 http://www.medicinehack.com/2011/07/virchows-triad.html Mechanism 3 http://drtedwilliams.net/kb/index.php?pagename=coagulation%20cascade
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Reversal of Novel Oral Anticoagulants. Angelina The, MD March 22, 2016
 Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Reversal of Novel Oral Anticoagulants Angelina The, MD March 22, 2016 Argatroban Bivalirudin Enoxaparin Lepirudin Heparin Dabigatran Apixaban 1939 1954 1998 2000 1999 2001 10/2010 7/2011 12/2012 1/2015
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
VENOUS THROMBOEMBOLISM PHARMACOLOGY. University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D
 VENOUS THROMBOEMBOLISM PHARMACOLOGY University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D LEARNING OBJECTIVES Know what factors anticoagulant medications
VENOUS THROMBOEMBOLISM PHARMACOLOGY University of Hawai i Hilo DNP Program NURS 603 Advanced Clinical Pharmacology Danita Narciso Pharm D LEARNING OBJECTIVES Know what factors anticoagulant medications
Post-procedure dose ok after hours. 12 hours (q 24h dosing only) assuming surgical hemostasis; second dose 24 hours after first dose.
 assuming surgical hemostasis; second dose 24 hours after first dose.") Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Medication Time to wait after last dose Post-procedure dose ok after hours Can pull catheter hours after last dose Can give next dose hours after pulling catheter Enoxaparin (Lovenox) Prophylactic dose
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Anticoagulation Task Force
 Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Anticoagulation Task Force Newest Recommendations Donald Zabriskie, BPharm, MBA, RPh Pharmacy Patient Care Services Cleveland Clinic- Fairview Hospital THE DRUGS THE PERFECT ANTICOAGULANT Oral administration
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
ADVOCATE HEALTHCARE GUIDELINE FOR ANTITHROMBOTIC REVERSAL
 Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
Minimal clinical evidence exists to support the efficacy of nonspecific procoagulant therapies that promote thrombin formation and antifibrinolytics in the setting of antithrombotic-related bleeding. Hemostatic
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Platelet-fibrin clot. 50Kd STEMI. Abciximab. Video of a IIb/IIIa inhibitor in action. Unstable Angina and non-stsegment
 Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
Objectives IIb/IIIa, Vitamin K, and Direct Thrombin Inhibition in Cardiology Michael Gulseth, Pharm. D., BCPS Assistant Professor, Duluth Pharmacy 6122 February 14, 2005 Describe the pharmacology, kinetics,
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Anticoagulation Update David J. Moliterno, MD
 David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
David J., MD Anticoagulant Agents n Cardiovascular Medicine: An Update David J., MD Professor and Chairman Division of Cardiovascular Medicine The University of Kentucky Linda and Jack Gill Heart nstitute
Blood Thinner Agent. Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy
 Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
Blood Thinner Agent Done by: Meznah Al-mutairi Pharm.D Candidate PNU Collage of Pharmacy Outline: Blood thinner agent definition. anticoagulants drugs. Thrombolytics. Blood thinner agent Therapeutic interference
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Endoscopy and the Anticoagulated Patient
 Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults
 Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Guidelines for the Management of Anticoagulant and Anti-Platelet Agent Associated Bleeding Complications in Adults Purpose: To be used as a common tool for all practitioners involved in the care of patients
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
True/False: Idarucizumab can be utilized for the management of bleeding associated with dabigatran.
 Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Anticoagulants: Agents, Pharmacology and Reversal
 Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
Anticoagulants: Agents, Pharmacology and Reversal Lori B Heller, M.D. Cardiac Anesthesiology Swedish Heart and Vascular Institute Medical Director, Swedish Blood Management Clinical Instructor, University
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran
 Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Discuss the role of idarucizumab for the management of bleeding associated with dabigatran Understand dosing, preparation and administration of idarucizumab I have no financial interest/arrangement or
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥
 Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
Management of antithrombotic agents before endoscopy 삼성서울병원소화기내과임상강사이세옥 Risk vs Benefit Hemorrhage Thrombosis Hemorrhage rarely fatal, controlled by endoscoic therapeutic measures, TAE, operation Thrombotic
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy
 David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy stewardw@etsu.edu At the conclusion of this program, the audience should
David Stewart, PharmD, BCPS Assistant Professor of Pharmacy Practice East Tennessee State University Bill Gatton College of Pharmacy stewardw@etsu.edu At the conclusion of this program, the audience should
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulant Drugs. by: Dr. M. Kamandi Fellowship of hematology and Oncology
 Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
Novel Anticoagulant Drugs by: Dr. M. Kamandi Fellowship of hematology and Oncology A-Novel Oral Anticoagulants A drug that is: safe and effective has predictable pharmacology has few drug drug and drug
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
New Anticoagulants Therapies
 New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
New Anticoagulants Therapies Rachel P. Rosovsky, MD, MPH October 22, 2015 Conflicts of Interest No disclosures 2 Agenda 3 Historical perspective Novel oral anticoagulants Stats Trials Approval Concerns/Limitations
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Update on Anticoagulants & Antiplatelet Drugs
 Update on Anticoagulants & Antiplatelet Drugs President, PRN Associates Continuing Medical Education, Tucson, AZ Objectives Recall the basic principles of hemostatis Describe the basic and clinical pharmacology
Update on Anticoagulants & Antiplatelet Drugs President, PRN Associates Continuing Medical Education, Tucson, AZ Objectives Recall the basic principles of hemostatis Describe the basic and clinical pharmacology
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Chapter 1 Introduction
 Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Chapter 1 Introduction There are several disorders which carry an increased risk of thrombosis, clots that interfere with normal circulation, including: venous thromboembolism (VTE), comprising both deep
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS
 NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
NOACS/DOACS*: COMPARISON AND FREQUENTLY-ASKED QUESTIONS OBJECTIVES: To provide a comparison of the newer direct oral anticoagulants (DOACs) currently available in Canada. To address frequently-asked questions
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation. MPharm Programme & OSPAP Programme. Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics
 MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
MPharm Programme & OSPAP Programme Anticoagulation Tania Jones Senior Lecturer in Pharmacy Practice & Therapeutics tania.jones@sunderland.ac.uk Lecture MPHM13 / MPHM14 2017-2018 MPHM13 & MPHM14 Objectives
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS
: COMPARISON AND FREQUENTLY ASKED QUESTIONS") NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
NEW/NOVEL ORAL ANTICOAGULANTS (NOACS): COMPARISON AND FREQUENTLY ASKED QUESTIONS OBJECTIVES: To provide a comparison of the new/novel oral anticoagulants (NOACs) currently available in Canada. To address
New Age Anticoagulants: Bleeding Considerations
 Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Ontario Regional Blood Coordinating Network March 23, 2012 New Age Anticoagulants: Bleeding Considerations Bill Geerts, MD, FRCPC Thromboembolism Specialist, Sunnybrook HSC Professor of Medicine, University
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Endoscopy in the Era of Anti- Platelet and Anti-Coagulation
 Endoscopy in the Era of Anti- Platelet and Anti-Coagulation Larissa Fujii-Lau, MD Assistant Professor of Medicine University of Hawaii Clinical Updates in Gastroenterology, Hepatology, and Nutrition 1/20/2017
Endoscopy in the Era of Anti- Platelet and Anti-Coagulation Larissa Fujii-Lau, MD Assistant Professor of Medicine University of Hawaii Clinical Updates in Gastroenterology, Hepatology, and Nutrition 1/20/2017
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Disclosure. Objectives. New Anticoagulants 6/5/2014 GHASSAN HADDAD M.D FHM. South Miami hospital Director of the Anticoagulation clinic.
 /5/1 New Anticoagulants: Opportunities, Challenges and Practical Considerations GHASSAN HADDAD M.D FHM. Chief of Hospital Medicine i South Miami hospital Director of the Anticoagulation clinic. Financial
/5/1 New Anticoagulants: Opportunities, Challenges and Practical Considerations GHASSAN HADDAD M.D FHM. Chief of Hospital Medicine i South Miami hospital Director of the Anticoagulation clinic. Financial
ADVANCES IN ANTICOAGULATION
 ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
ADVANCES IN ANTICOAGULATION The Clinicians Perspective Claudine M. Lewis Cardiologist OUTLINE Indications for anticoagulants Review - Physiology of Hemostasis Types of anticoagulants New anticoagulants
Anticoagulants. Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT
 Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
Haemostasis Thrombosis Phases Endogenous anticoagulants Stopping blood loss Pathological formation of a haemostatic plug Arterial associated with atherosclerosis Venous blood stasis e.g. DVT Vascular Platelet
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Hemostasis and Blood Forming Organs
 Hemostasis and Blood Forming Organs Subcommittee: Williams, Patricia B. (Chair) pbwillia@umich.edu McMillan, David dcmcmillan@unmc.edu Dobrydneva, Yuliya dobrydy@evms.edu DEFEROXAMINE FERROUS SULFATE ferrous
Hemostasis and Blood Forming Organs Subcommittee: Williams, Patricia B. (Chair) pbwillia@umich.edu McMillan, David dcmcmillan@unmc.edu Dobrydneva, Yuliya dobrydy@evms.edu DEFEROXAMINE FERROUS SULFATE ferrous
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY
 EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
EAU GUIDELINES ON THROMBOPROPHYLAXIS IN UROLOGICAL SURGERY K.A.O. Tikkinen (Chair), R. Cartwright, M.K. Gould, R. Naspro, G. Novara, P.M. Sandset, P.D. Violette, G.H. Guyatt Introduction Utilising recent
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
CHAPTER 17 Antithrombotic Agents Heparins
 CHAPTER 17 Antithrombotic Agents Heparins Structure Mechanism of Action Pharmacokinetics Limitations of Unfractionated Heparin Heparin Induced Thrombocytopenia Heparin Rebound Low Molecular Weight Heparins
CHAPTER 17 Antithrombotic Agents Heparins Structure Mechanism of Action Pharmacokinetics Limitations of Unfractionated Heparin Heparin Induced Thrombocytopenia Heparin Rebound Low Molecular Weight Heparins
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
European Heart Journal 2015 doi: /eurheartj/ehv320
 European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type
European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 1 2 Clinical implications of high-sensivity troponin assays European Heart Journal 2015 doi: 10.1093/eurheartj/ehv320 Conditions other than Type