New Horizons in Cardiogenic Shock. Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute
|
|
|
- Melanie Ball
- 6 years ago
- Views:
Transcription

1 New Horizons in Cardiogenic Shock Timothy D. Henry, MD Director of Cardiology Cedars-Sinai Heart Institute

2 AMI Shock Mortality Unchanged in > 20 years US AMI/CGS cases per year 1, High In-Hospital Mortality During AMI Cardiogenic Shock 3 N = 23, Sandhu A, McCoy l, Negi S, et al. Use of Mechanical Circulatory Support in Patients Undergoing Percutaneous Coronary Intervention; Insights from the National Cardiovascular Data Registry. Circulation, 2015;132: Acute Cardiac Assist Report, Health Research International August Jeger, et al. Ann Intern Med. 2008
3 Randomized Trials Cardiogenic Shock Trial Follow-up n/n n/n Relative Risk Mortality 95% CI Relative Risk 95% CI Revascularization SHOCK 1 year 81/ / (0.54;0.95) SMASH 30 days 22/32 18/ (0.66;1.29) Total 103/ / (0.69;0.97) Early revascularization better Medical treatment better Vasopressors SOAP-2 (CS subgroup) 28 days 64/145 50/ (0.55;0.93) Norepinephrine better Dopamine better Inotropes Unverzagt et al. 30 days 5/16 10/ (0.11;0.97) Levosimendan better Control better Glycoprotein IIb/IIIa inhibitors PRAGUE-18 In-hospital 15/40 13/ (0.59;2.27) Abciximab better Standard treatment better NO synthase inhibitors TRIUMPH 30 days 97/201 76/ (0.91;1.45) SHOCK II 30 days 24/59 7/ (0.59;2.69) Cotter et al. 30 days 4/15 10/ (0.13;1.05) Total 125/275 93/ (0.85;1.29) NO synthase inhibition better Placebo better IABP IABP-SHOCK I 30 days 7/19 6/ (0.45;3.72) IABP-SHOCK II 30 days 119/ / (0.79;1.17) Total 126/ / (0.81;1.18) IABP better Standard treatment better LVAD Thiele et al. 30 days 9/21 9/ (0.48;1.90) Burkhoff et al. 30 days 9/19 5/ (0.57;3.10) ISAR-SHOCK 30 days 6/13 6/ (0.44;2.29) IMPRESS in Severe Shock 30 days 11/24 12/ (0.51;1.66) Total 35/77 32/ (0.70;1.44) LVAD better IABP better Thiele et al. Eur Heart J 2015;36:



4 Inotrope Harm in Cardiogenic Shock 1. Marked increase in MVO2 at a time of oxygen starvation. 2. Tachycardia increases MVO2 and decreases diastolic interval. 3. Marked increase in LVEDP causes further decrease in diastolic perfusion pressure and increased wall tension. 4. Tachycardia mediated apoptosis may decrease myocardial recovery.
 Mortality 54% 65% 65% 74% 32% 0 1 2 3 4+ Number of Inotropes/Pressors Samuels LE et al, J Card Surg. 1999 1. Basir M, Schreiber T, Grines C, et al.")
5 Increased Inotrope Exposure is associated with Mortality in AMI/CGS Mortality and Number of Inotropes from cvad Registry 1 P<0.001 (N=287) Mortality 54% 65% 65% 74% 32% Number of Inotropes/Pressors Samuels LE et al, J Card Surg Basir M, Schreiber T, Grines C, et al. Effect of Early Initiation of Mechanical Circulatory Support on Survival in Cardiogenic Shock. Am. J. of Cardiology, 2016
 89 56% Swan 53% 57 43% 36 45% 45% 46% 49 48% 33 55 47% 37% 12 21 38% 13 14 Survival 0% to 10% 10%")

6 6 SG USE ASSOCIATED WITH IMPROVED OUTCOMES Distribution of Survival to Explant at Impella Sites (379 sites supported >4 AMICS patients) 89 56% Swan 53% 57 43% 36 45% 45% 46% 49 48% % 37% % Survival 0% to 10% 10% to 20% 20% to 30% 30% to 40% 40% to 50% 50% to 60% 60% to 70% 70% to 80% 80% to 90% 90% to 100% Total # of Patients N=68 N=147 N=277 N=488 N=777 N=465 N=425 N=331 N=99 N=62 ABIOMED INTERNAL CLINICAL QUALITY DATA AMI/CGS APRIL 2015 MARCH 2016
 Database, US AMI/CGS Apr 2009 Jan 2017.")
7 Hemodynamic Monitoring associated with Improved Survival in AMI/CGS IQ Database 1 63% cvad Registry 2 76% 68% P= % P< N=8767 N=5217 N=634 N=516 No Hemodynamic Monitoring Hemodynamic Monitoring No Hemodynamic Monitoring Hemodynamic Monitoring 1. Abiomed Impella Quality (IQ) Database, US AMI/CGS Apr 2009 Jan Survival to Explant. Danvers, MA: Abiomed. 2. cvad survival to explant
8 Key Issues Culprit-Shock Cardiac Arrest-Cardiogenic shock interaction New AHA Scientific Statement-Shock centers and Shock teams Refractory Shock
9
 Multivessel-PCI (n=1,194) 80.3% de Waha et al.")
10 Multivessel PCI in Cardiogenic Shock Metaanalysis Mortality Registry-Data: 19.7% Culprit only-pci (n=4,857) Multivessel-PCI (n=1,194) 80.3% de Waha et al. Eur Heart J Acute Cardiovasc Care. 2017; epub
11 Multivessel PCI in Cardiogenic Shock? Metaanalysis Mortality Registry-Data MV-PCI C-PCI Events Total Events Total Short-term follow-up RR 95%CI IABP-SHOCK II [ ] ALKK [ ] KAMIR [ ] Yang et al [ ] Cavender et al [ ] EHS-PCI [ ] NCDR [ ] Overall [ ] Heterogeneity: τ 2 =0.007, I 2 =31.0%, p=0.19 Test for overall effect: p= Multivessel PCI better Culprit only PCI better MV-PCI C-PCI Long-term follow-up RR 95%CI Events Total Events Total IABP-SHOCK II [ ] KAMIR [ ] Yang et al [ ] Cavender et al [ ] Mylotte et al [ ] van der Schaaf et al [ ] SHOCK [ ] Overall [ ] Heterogeneity: τ 2 =0.043, I 2 =67.8%, p=0.005 Test for overall effect: p= Multivessel PCI better Culprit only PCI better de Waha et al. Eur Heart J Acute Cardiovasc Care. 2017; epub
12 Hypothesis Culprit lesion only PCI (with possible staged revascularization) is superior to immediate multivessel PCI in multivessel coronary artery disease ( 2 mm in diameter, >70% stenosis incl. CTO) patients with cardiogenic shock complicating acute myocardial infarction. Thiele et al. Am Heart J. 2016;172:
13 Statistical Methodology Primary Study Endpoint: 30-day all-cause mortality or renal replacement therapy Secondary Study Endpoints: 30-day all-cause mortality Renal failure with requirement of renal replacement therapy Time to hemodynamic stabilization Duration of catecholamine therapy Serial creatinine-clearance Length of ICU-stay SAPS-II score Requirement and length of mechanical ventilation All-cause death within 6 and 12 months follow-up Recurrent infarction within 30-days, 6 and 12 months follow-up Death or recurrent infarction at 6 and 12 months follow-up Rehospitalization for congestive heart failure within 30 days, 6-, and 12-months follow-up Death/recurrent infarction/rehospitalization for congestive heart failure within 30 days, 6-, and 12-months follow-up Need for repeat revascularization (PCI and/or CABG) within 30 days, 6-, and 12-months follow-up Peak creatine kinase, creatine kinase-mb and troponin level during hospital stay Sample Size: Estimated 50% event rate in multivessel PCI versus 38% in culprit lesion only group for primary endpoint 1 interim analysis (50% of patients) 2-sided Chi 2 -test; power: 80%, alpha=0.048 for final analysis 684 patients To compensate losses in follow-up 706 patients Thiele et al. Am Heart J. 2016;172:
14 Study Flow Chart 1075 patients with acute myocardial infarction (STEMI and NSTEMI) and cardiogenic shock screened 369 excluded 706 randomized 351 randomized to culprit lesion only PCI 344 full informed consent 301 culprit lesion only PCI 43 immediate multivessel PCI 60 staged PCI 1 staged CABG 13 urgent PCI Allocation Informed consent Revascularization 355 randomized to immediate multivessel PCI 342 full informed consent 310 immediate multivessel PCI 32 culprit lesion only PCI 8 staged PCI 0 staged CABG 5 urgent PCI Follow-up 344 with 30-day follow-up 341 with 30-day follow-up 1 lost to follow-up Primary endpoint analysis 344 primary endpoint analysis 341 primary endpoint analysis
15 Baseline Characteristics Characteristic Culprit only PCI (n=344) Multivessel PCI (n=342) Age (years); median (IQR) 70 (60-78) 70 (60-77) Male sex; n/total (%) 257/343 (74.9) 267/342 (78.1) Prior myocardial infarction; n/total (%) 60/339 (17.7) 53/335 (15.8) Prior PCI; n/total (%) 64/339 (18.9) 63/335 (18.8) Prior coronary arterial bypass surgery; n/total (%) 20/341 (5.9) 13/337 (3.9) Signs of impaired organ perfusion; n/total (%) Altered mental status Cold, clammy skin and extremities Oliguria Arterial lactate >2.0 mmol/l 237/341 (69.5) 233/338 (68.9) 80/334 (24.0) 216/334 (64.7) 224/341 (65.7) 236/335 (70.4) 93/326 (28.5) 224/330 (67.9) Fibrinolysis <24 h before randomization; n/total (%) 19/341 (5.6) 15/341 (4.4) Resuscitation before randomization; n/total (%) 177/341 (51.9) 189/342 (55.3) ST-elevation myocardial infarction; n/total (%) 206/335 (61.5) 209/330 (63.3) No. of diseased vessels; n/total (%) /343 (0.9) 122/343 (35.6) 218/343 (63.6) 2/342 (0.6) 124/342 (36.3) 216/342 (63.2) Patients with at least one CTO; n/total (%) 77/344 (22.4) 82/342 (24.0) Left ventricular ejection fraction (%); median (IQR) 33 (25-40) 30 (21-40)
16 Treatment Characteristic Culprit only PCI (n=344) Multivessel PCI (n=342) Femoral access; n/total (%) 287/343 (83.7) 277/342 (81.0) 0.36 Radial access; n/total (%) 61/343 (17.8) 66/342 (19.3) 0.61 Stent implanted in culprit lesion; n/total (%) 326/343 (95.0) 324/342 (94.7) 0.86 Drug-eluting stent in culprit lesion; n/total (%) 305/326 (93.6) 308/324 (95.1) 0.41 TIMI-flow III post PCI of culprit lesion; n/total (%) 289/342 (84.5) 293/338 (86.7) 0.46 Immediate PCI of non-culprit lesions; n/total (%) 43/344 (12.5) 310/342 (90.6) <0.001 Immediate complete revascularization; n/total (%) 26/344 (7.6) 277/342 (81.2) <0.001 Total amount of contrast agent (ml); median (IQR) 190 ( ) 250 ( ) <0.001 Staged PCI of non-culprit lesions; n/total (%) 60/344 (17.4) 8/341 (2.3) <0.001 Staged coronary artery bypass surgery; n/total (%) 1/344 (0.3) 0/341 >0.99 Mechanical circulatory support; n/total (%) 99/344 (28.8) 95/342 (27.8) 0.77 Intraaortic balloon pump; n/total (%) 25/99 (25.3) 26/95 (27.4) 0.74 Impella 2.5; n/total (%) 16/99 (16.2) 18/95 (18.9) 0.61 Impella CP; n/total (%) 30/99 (30.3) 18/95 (18.9) 0.07 TandemHeart; n/total (%) 2/99 (2.0) 0/ ECMO; n/total (%) 18/99 (18.2) 27/95 (28.4) 0.09 Mild hypothermia; n/total (%) 111/344 (32.3) 118/340 (34.7) 0.50 Mechanical ventilation; n/total (%) 273/344 (79.4) 282/339 (83.2) 0.20 Duration of mechanical ventilation (days); median (IQR) 3 (1-7) 3 (1-7) 0.97 Duration of intensive care treatment (days); median (IQR) 5 (2-12) 5 (2-11) 0.61
17 All-cause mortality or renal replacement therapy (%) Primary Study Endpoint All-Cause Mortality or Renal Replacement Therapy Immediate multivessel PCI Culprit lesion only PCI 55.4% 45.9% Number at risk: Culprit lesion only PCI Relative risk 0.83; 95% confidence interval ; P= Days after randomization Immediate multivessel PCI
18 All-cause mortality (%) All-Cause Mortality Immediate multivessel PCI 51.5% 40 Culprit lesion only PCI 43.3% Relative risk 0.84; 95% confidence interval ; P= Days after randomization Number at risk: Culprit lesion only PCI Immediate multivessel PCI
19 Renal replacement therapy (%) Renal Replacement Therapy Immediate multivessel PCI Culprit lesion only PCI 16.4% 11.6% Number at risk: Culprit lesion only PCI 0 Relative risk 0.71; 95% confidence interval ; P= Days after randomization Immediate multivessel PCI
20 Arterial lactate (mmol/l) Arterial Lactate 9 8 P=0.78* P=0.13* P=0.89* P=0.39* P=0.78* P=0.07* P=0.16* P=0.26* 7 6 Culprit lesion only PCI Immediate multivessel PCI *No adjustment for multiple testing Pre PCI Post PCI 8h 16h 24h 32h 40h 48h
21 Estimated glomerular filtration rate (ml/min) Glomerular Filtration Rate 120 P=0.87* P=0.56* P=0.12* P=0.04* P=0.04* *No adjustment for multiple testing Culprit lesion only PCI Immediate multivessel PCI Baseline Day 1 Day 2 Day 3 Day 4
22 Conclusions In patients with multivessel coronary artery disease and cardiogenic shock complicating acute myocardial infarction culprit lesion only PCI with possible staged revascularization reduced the composite of mortality or requirement for renal replacement therapy at 30 days. This effect in the primary outcome was mainly driven by a 30-day mortality reduction. This largest randomized European multicenter trial in cardiogenic shock complicating myocardial infarction challenges current guideline recommendations.
23 Key Issues Culprit-Shock Cardiac Arrest-Cardiogenic shock interaction New AHA Scientific Statement-Shock centers and Shock teams Refractory Shock
24 Cardiac Arrest Out-of-hospital cardiac arrest (OOHCA) 295,000 people annually in the US 7.9% median survival rate Anoxic encephalopathy and neurologic deficits Therapeutic hypothermia (TH) clinical trials ILCOR recommendation for TH after resuscitation Lloyd-Jones D, Adams R, Carnethon M et al. Heart disease and stroke statistics-2009 update. Circulation 2009;119:e21-e181.
25 Cardiac Arrest ( ) Cardiac Arrest (+) Interaction of Cardiac Arrest and Cardiogenic Shock Cardiogenic Shock (+) 184 Patients In-hospital Mortality: 47.3% 1 Year Mortality: 51.6% 259 Patients In-hospital Mortality: 25.1% 1 Year Mortality: 33.6% Cardiogenic Shock ( ) 317 Patients In-hospital Mortality: 20.2% 1 Year Mortality: 22.7% 4157 Patients In-hospital Mortality: 1.7% 1 Year Mortality: 5.5%
26 OHCA survival to hospital discharge by 5-year time periods Comilla Sasson et al. Circ Cardiovasc Qual Outcomes. 2010;3:63-81

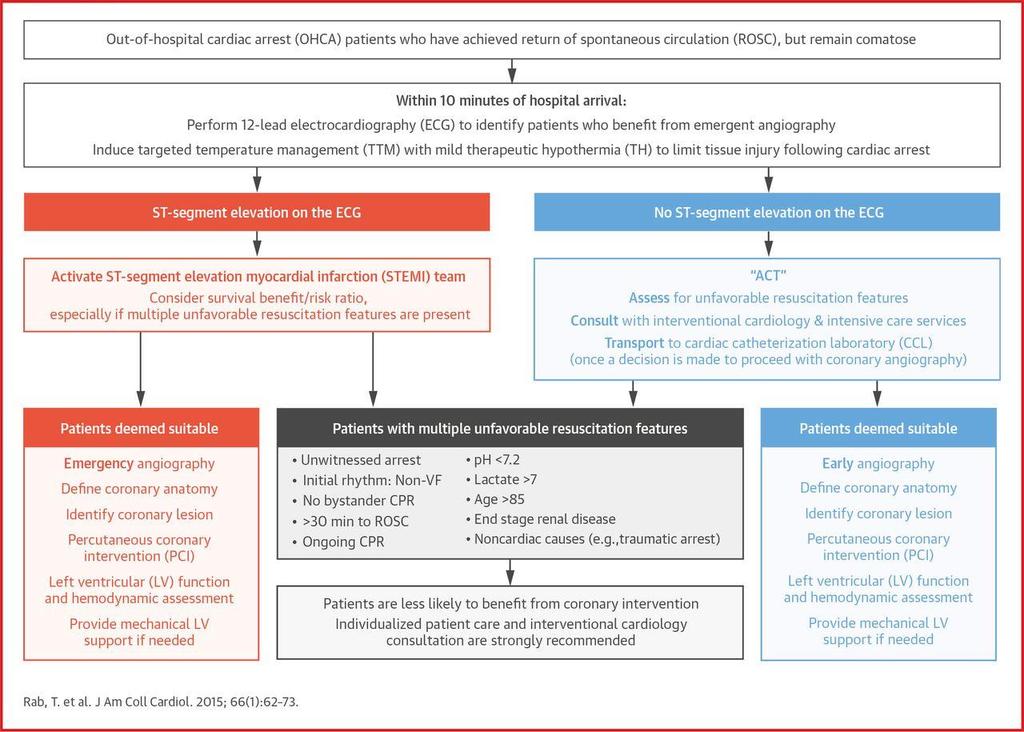
27 With hypothermia and PCI! Survival improves to 50-60% with Favorable neurological outcomes in 86% of survivors Rab et al. JACC 2015;66:62-73
28 Early predictors of survival in OHCA Florence Dumas et al. Circ Cardiovasc Interv. 2010;3:
29

30
31 Key Issues Culprit-Shock Cardiac Arrest-Cardiogenic shock interaction New AHA Scientific Statement-Shock centers and Shock teams Refractory Shock
32
33 Circulation 2017

34




35 Detroit Cardiogenic Shock Initiative DETROIT CSI


36 DETROIT CSI PROTOCOL

37 DETROIT CSI PROTOCOL

38 DETROIT CSI PROTOCOL


39 National Shock Initiative Physicians from over 40 hospitals have contacted us about joining Detroit CSI First site outside of Detroit launched in August: Mercy Fitzgerald Hospital in Philadelphia Similar to Detroit, regional groups are forming to work together on CGS Detroit Cardiogenic Shock Initiative
 2 0% 20% 40% 60% 80% 100% Survival to Explant 1. Data on file. Abiomed Impella Quality(IQ)Data, AMI/CGS Apr 2016 Sept 2017. Danvers, MA: Abiomed. 2. 525 sites supporting >6 AMICS patients, 7,483 patients total since March 2016")
40 National Outcomes Improving Distribution of Impella Site Outcomes 1 # of Sites 51% 62% 22% relative improvement in overall outcomes since March, 2016 (p<0.0001) 2 0% 20% 40% 60% 80% 100% Survival to Explant 1. Data on file. Abiomed Impella Quality(IQ)Data, AMI/CGS Apr 2016 Sept Danvers, MA: Abiomed sites supporting >6 AMICS patients, 7,483 patients total since March 2016


41
42 Key Issues Culprit-Shock Cardiac Arrest-Cardiogenic shock interaction New AHA Scientific Statement-Shock centers and Shock teams Refractory Shock

43 Early Transport to Cath Lab for ECMO and Revasc in Refractory VF (?OHCA)
44 Early Transport to Cath Lab for ECMO and Revascularization in Refractory Ventricular Fibrillation Out of Hospital VF/VT Initial rhythm DCCV x3 and 300mg Amiodarone without ROSC Time to CCL <30 min Initial CCL ABG and lactate Stop if: ETCO2<10mmHg, PaO2<50mmHg or Lactate >18 mmol/l If ROSC, immediate Cor Angio +/- IABP. If no ROSC, ECLS, then Cor Angio +/- IABP. Continue ACLS/ECLS for 90 minutes/pci; if no ROSC by 90 minutes, declared dead

45

46 Comparison Between the Refractory VF/VT Protocol and the Historical Comparison Group


47

48

49
50 Complication Rate 13% on ECMO had Vascular Complications 4 with significant retroperitoneal bleeding requiring transfusion 3 developed an ischemic leg after thrombosis of the distal perfusion cath

51
52
The Case for Multivessel Revascularization in Shock
 The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
CULPRIT-SHOCK: A Randomized Trial of Multivessel PCI in Cardiogenic Shock. Holger Thiele, MD on behalf of the CULPRIT-SHOCK Investigators
 CULPRIT-SHOCK: A Randomized Trial of Multivessel PCI in Cardiogenic Shock Holger Thiele, MD on behalf of the CULPRIT-SHOCK Investigators Disclosure Statement of Financial Interest Within the past 12 months,
CULPRIT-SHOCK: A Randomized Trial of Multivessel PCI in Cardiogenic Shock Holger Thiele, MD on behalf of the CULPRIT-SHOCK Investigators Disclosure Statement of Financial Interest Within the past 12 months,
Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella
 Supported With Impella") Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella William O Neill, MD, FACC Medical Director Structural Heart Disease at Henry Ford Hospital, MI AMI Shock Mortality
Outcomes for 15,259 US Patients With Acute MI Cardiogenic Shock (AMICS) Supported With Impella William O Neill, MD, FACC Medical Director Structural Heart Disease at Henry Ford Hospital, MI AMI Shock Mortality
Controversies in Cardiogenic Shock. Timothy D. Henry, MD Cedars-Sinai Heart Institute
 Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
A National Cardiogenic Shock Initiative (CSI):
:") A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
A National Cardiogenic Shock Initiative (CSI): Insights from the Impella Quality (IQ) Program, cvad Registry and the Detroit CSI Experience William O Neill, MD, FACC Medical Director Structural Heart Disease
Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017
 Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017 Holger Thiele Cardiogenic Shock STEMI Guidelines Steg et al. Eur Heart J.2012;33:2569-2619 Cardiogenic Shock CHF Guidelines
Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017 Holger Thiele Cardiogenic Shock STEMI Guidelines Steg et al. Eur Heart J.2012;33:2569-2619 Cardiogenic Shock CHF Guidelines
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Cardiogenic Shock and Initiatives to Reduce Mortality
 Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
Cardiogenic Shock and Initiatives to Reduce Mortality Tanveer Rab, MD, FACC William O Neill, MD, FACC Perwaiz Meraj, MD, FACC Alex Truesdell, MD, FACC The Golden Hours? 50% dead within 10 hours Overall
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
IABP SHOCK II trial:
 IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
IABP SHOCK II trial: Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic
Management of Cardiogenic shock. Prof. Christian JM Vrints
 Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Accepted Manuscript. Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD S (18)
") Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
Accepted Manuscript Improving Survival in Cardiogenic shock: Is Impella the Answer?,, James J Glazier MD, Amir Kaki MD PII: S0002-9343(18)30496-0 DOI: 10.1016/j.amjmed.2018.04.045 Reference: AJM 14684
Introduction to Acute Mechanical Circulatory Support
 Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
Introduction to Acute Mechanical Circulatory Support Navin K. Kapur, MD, FACC, FSCAI, FAHA Associate Professor, Department of Medicine Interventional Cardiology & Advanced Heart Failure Programs Executive
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
ST-Elevation Myocardial Infarction & Cardiogenic Shock. - What Should We Do?
 ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
ST-Elevation Myocardial Infarction & Cardiogenic Shock - What Should We Do? Advanced Angioplasty 2008 Dan Blackman Leeds General Infirmary Conflicts of interest Advisory Boards Cordis Boston Scientific
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial
 Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial Georg Fuernau, Johannes Beck, Steffen Desch, Ingo Eitel, Christian Jung, Sandra Erbs, Norman Mangner,
Mild Hypothermia in Cardiogenic Shock Complicating Myocardial Infarction the Randomized SHOCK-COOL Trial Georg Fuernau, Johannes Beck, Steffen Desch, Ingo Eitel, Christian Jung, Sandra Erbs, Norman Mangner,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
DECLARATION OF CONFLICT OF INTEREST. Research grants: Sanofi-Aventis
 DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
Andrew Civitello MD, FACC
 Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Timing the Transition from Short Term to Long Term Mechanical Circulatory Support Andrew Civitello MD, FACC Medical Director, Heart Transplant Program Director, Fellowship Co-Director, Baylor St. Luke's
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO)
") Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart, ECMO) Michael A. Gibson, MD Assistant Professor of Medicine University of California, Irvine Division of Cardiology
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012
 Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
Acute heart failure: ECMO Cardiology & Vascular Medicine 2012 Lucia Jewbali cardiologist-intensivist 14 beds/8 ICU beds Acute coronary syndromes Heart failure/ Cardiogenic shock Post cardiotomy Heart
4/22/2016 Updated. AllinaHealthSystem. Cardiogenic Shock: Definition. No Disclosures. Cardiogenic Shock: Declining (But Still High) Case Fatality Rate
 Case Fatality Rate") 4/22/216 Updated Definition End-organ hypoperfusion secondary to cardiac failure Advanced Cardiopulmonary Support for the Critically Ill Adult April 22, 216 Cardiogenic Shock Michael A. Samara, MD FACC
4/22/216 Updated Definition End-organ hypoperfusion secondary to cardiac failure Advanced Cardiopulmonary Support for the Critically Ill Adult April 22, 216 Cardiogenic Shock Michael A. Samara, MD FACC
Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the COACT trial
 Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the On behalf of the COACT investigators Jorrit Lemkes, MD, Interventional cardiologist Amsterdam UMC, Vrije Universiteit Amsterdam,
Coronary Angiography after Cardiac Arrest without ST-Segment Elevation: the On behalf of the COACT investigators Jorrit Lemkes, MD, Interventional cardiologist Amsterdam UMC, Vrije Universiteit Amsterdam,
Post resuscitation care and role of urgent angiography after cardiac arrest. Georg Fuernau Luebeck
 Post resuscitation care and role of urgent angiography after cardiac arrest Georg Fuernau Luebeck The journey CPR and guidelines European Resuscitation Council American Heart Association International
Post resuscitation care and role of urgent angiography after cardiac arrest Georg Fuernau Luebeck The journey CPR and guidelines European Resuscitation Council American Heart Association International
Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California
 High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
High Risk PCI Making Possible the Impossible Ray Matthews MD Professor of Clinical Medicine Chief of Cardiology University of Southern California Disclosures Abiomed Research Support Consulting Agreement
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Recovering Hearts. Saving Lives.
 Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Recovering Hearts. Saving Lives ṬM The Door to Unload (DTU) STEMI Safety & Feasibility Pilot Trial November 218 Recovering Hearts. Saving Lives. LEGAL DISCLAIMERS This presentation includes select slides
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Circulatory Support: From IABP to LVAD
 Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Circulatory Support: From IABP to LVAD Howard A Cohen, MD, FACC, FSCAI Director Division of Cardiovascular Intervention Co Director Cardiovascular Interventional ti Laboratories Lenox Hill Heart & Vascular
Impella CP Versus Intra-Aortic Balloon Pump in Acute Myocardial Infarction Complicated by Cardiogenic Shock: The IMPRESS trial
 Accepted Manuscript Impella CP Versus Intra-Aortic Balloon Pump in Acute Myocardial Infarction Complicated by Cardiogenic Shock: The IMPRESS trial Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Krischan
Accepted Manuscript Impella CP Versus Intra-Aortic Balloon Pump in Acute Myocardial Infarction Complicated by Cardiogenic Shock: The IMPRESS trial Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Krischan
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
Controversies In STEMI Management
 Controversies In STEMI Management Professor Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology Department, Alexandria University - Egypt Past President of the Egyptian Society of Cardiology President
Controversies In STEMI Management Professor Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology Department, Alexandria University - Egypt Past President of the Egyptian Society of Cardiology President
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome'
 'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
'Coronary artery bypass grafting in patients with acute coronary syndromes: perioperative strategies to improve outcome' Miguel Sousa Uva Chair ESC Cardiovascular Surgery WG Hospital da Cruz Vermelha Portuguesa
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
 STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Cardiogenic Shock Protocol
 Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
Cardiogenic Shock Protocol Impella Devices Best Practices in AMI Cardiogenic Shock Identify 1-3 SBP < 90 mmhg or on inotropes /pressors Cold, clammy, tachycardia Lactate elevated > 2 mmoi /L Stabilize
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
PROMUS Element Experience In AMC
 Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Percutaneous Mechanical Circulatory Support Devices
 Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
Percutaneous Mechanical Circulatory Support Devices Daniel Vazquez RN, RCIS Miami Cardiac & Vascular Institute FINANCIAL DISCLOSURES none CASE STUDY CASE STUDY 52 year old gentlemen Complaining of dyspnea
EACTS Adult Cardiac Database
 EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
EACTS Adult Cardiac Database Quality Improvement Programme List of changes to Version 2.0, 13 th Dec 2018, compared to version 1.0, 1 st May 2014. INTRODUCTORY NOTES This document s purpose is to list
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Alex versus Xience Registry Preliminary report
 Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
Interventional Cardiology Network Alex versus Xience Preliminary report Mariusz Gąsior 1,2, Marek Gierlotka 1, Lech Poloński 1,2 1 3rd Department of Cardiology, Medical University of Silesia Centre tor
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI. ISAR-REACT 4 Trial
 Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
Abciximab plus Heparin versus Bivalirudin in Patients with NSTEMI Undergoing PCI ISAR-REACT 4 Trial Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität, Munich, Germany On behalf of F.-J.
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI
 Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Supplementary Online Content
 Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
Cover Page The handle http://hdl.handle.net/1887/21543 holds various files of this Leiden University dissertation Author: Dharma, Surya Title: Perspectives in the treatment of cardiovascular disease :
University of Leipzig Heart Center
 Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic shock Holger
Randomized comparison of intraaortic balloon counterpulsation versus optimal medical therapy in addition to early revascularization in acute myocardial infarction complicated by cardiogenic shock Holger
Final published version:
 Clinical Characteristics and Outcomes of Patients With Myocardial Infarction and Cardiogenic Shock Undergoing Coronary Artery Bypass Surgery: Data From The Society of Thoracic Surgeons National Database
Clinical Characteristics and Outcomes of Patients With Myocardial Infarction and Cardiogenic Shock Undergoing Coronary Artery Bypass Surgery: Data From The Society of Thoracic Surgeons National Database
MANAGEMENT OF CARDIOGENIC SHOCK
 MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
MANAGEMENT OF CARDIOGENIC SHOCK CASE PRESENTATION 37 year old Dutch female No known coronary artery disease risk factors 1 week post partum at time of presentation (G3P3) after an uncomplicated normal
Disclosures. Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 ECG. Case. Case. Case Summary 4/22/2016
 Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Ted Feldman, M.D., MSCAI FACC FESC
 Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
Support Technologies and High Risk Intervention Patient Selection: When Not to Use Them Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas December 7-10 th, 2014 Ted
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
MCS for Acute Heart Failure Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant
 MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
MCS for Acute Heart Failure 2016 Eric Adler MD Associate Professor of Medicine Medical Director Cardiac Transplant Why do we decompensate? Which Heart Failure Patients Should Get Palliative Care and Who
27th Annual ELSO Conference San Diego, CA
 27th Annual ELSO Conference San Diego, CA VA ECMO in the cath lab best timing? Impella or ECMO? Michael R. Mooney, MD, FACC, FSCAI, FAHA Director, Coronary Therapeutics Minneapolis Heart Institute at Abbott
27th Annual ELSO Conference San Diego, CA VA ECMO in the cath lab best timing? Impella or ECMO? Michael R. Mooney, MD, FACC, FSCAI, FAHA Director, Coronary Therapeutics Minneapolis Heart Institute at Abbott
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials
 Accepted Manuscript Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Melchior Seyfarth,
Accepted Manuscript Impella Versus Intra-Aortic Balloon Pump For Treatment Of Cardiogenic Shock: A Meta-Analysis of Randomized Controlled Trials Dagmar M. Ouweneel, MSc, Erlend Eriksen, MD, Melchior Seyfarth,
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Counterpulsation. John N. Nanas, MD, PhD. Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece
 John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
John N. Nanas, MD, PhD Professor and Head, 3 rd Cardiology Dept, University of Athens, Athens, Greece History of counterpulsation 1952 Augmentation of CBF Adrian and Arthur Kantrowitz, Surgery 1952;14:678-87
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA. IMP v4
 1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
1 TREATMENT OF HIGHER RISK PATIENTS INTRODUCTION TO PROTECTED PCI WITH IMPELLA FDA APPROVES IMPELLA FOR HIGH-RISK PCI 2 Impella is the only hemodynamic support device proven safe and effective in elective
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
1/5/2017. The Next Frontier: Advanced Cardiogenic Shock U MICHIGAN EPERIENCE
 % SURVIVAL 1/5/2017 The Next Frontier: Advanced Cardiogenic Shock William W. O Neill, MD Henry Ford Health System Medical Director Center for Structural Heart Disease Detroit, MI U MICHIGAN EPERIENCE 1983-1985
% SURVIVAL 1/5/2017 The Next Frontier: Advanced Cardiogenic Shock William W. O Neill, MD Henry Ford Health System Medical Director Center for Structural Heart Disease Detroit, MI U MICHIGAN EPERIENCE 1983-1985
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction
 Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
Who is the high risk patient?
 Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Who is the high risk patient? High risk of periprocedural death or other major complications (hemodynamic compromise, MI, stroke, dialysis) Contributors of Risk Lesion/Procedure Governed by 1. Patient
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in Patients with Non-ST Elevation ACS
 Angioplasty to Blunt the rise Of troponin in Acute coronary syndromes Randomized for an immediate or Delayed intervention A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in
Angioplasty to Blunt the rise Of troponin in Acute coronary syndromes Randomized for an immediate or Delayed intervention A Multicenter Randomized Trial of Immediate Versus Delayed Invasive Strategy in
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion
 Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 OSPEDALE Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
High Risk PCI for Heart Failure
 High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
High Risk PCI for Heart Failure Ray Matthews MD Professor of Clinical Medicine Chief, Division of Cardiovascular Medicine University of Southern California Los Angeles, California Disclosures Abiomed Research
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR
 PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
PUMP FAILURE COMPLICATING AMI: ISCHAEMIC VSR Dr Susanna Price MD PhD MRCP ESICM FFICM FESC Consultant Cardiologist & Intensivist Royal Brompton & Harefield NHS Foundation Trust DECLARATIONS Educational
State of the art lecture: 21st Century Post resuscitation management
 State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
TREATMENT OPTIONS IN CARDIOGENIC SHOCK WITH INTRA-AORTIC BALLOON COUNTERPULSATION
 TREATMENT OPTIONS IN CARDIOGENIC SHOCK WITH INTRA-AORTIC BALLOON COUNTERPULSATION *Markus W. Ferrari Clinic of Internal Medicine I, HELIOS Dr-Horst-Schmidt-Clinic, Wiesbaden, Germany *Correspondence to
TREATMENT OPTIONS IN CARDIOGENIC SHOCK WITH INTRA-AORTIC BALLOON COUNTERPULSATION *Markus W. Ferrari Clinic of Internal Medicine I, HELIOS Dr-Horst-Schmidt-Clinic, Wiesbaden, Germany *Correspondence to
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants