Meet the experts: Cardiogenic Shock
|
|
|
- Jonathan Lloyd
- 6 years ago
- Views:
Transcription


1 Meet the experts: Cardiogenic Shock Inotropes: effects on the heart, the microcirculation and other organs ACCA Masterclass 2017 Alessandro Sionis Director Acute & Intensive Cardiac Care Unit Hospital de la Santa Creu I Sant Pau Universitat de Barcelona Spain
2 Disclosures (last 5 years) Speaker: Abiomed, Maquet, Novartis, Orion-Pharma Clinical trials: Cardiorentis, Novartis, Orion-Pharma Research grants: Novartis, Orion-Pharma Royalties: No
 Wet Dry NO (5% of AHF patients) POOR PERFUSION?")
3 PATIENT WITH AHF Bedside assessment to identify haemodynamic profile CONGESTION? YES (95% of AHF patients) Wet Dry NO (5% of AHF patients) POOR PERFUSION? NO YES NO YES Wet & Warm Wet & Cold Dry & Warm Dry & Cold Adapted from 2016 ESC HF Guildeines
4 PATIENT WITH AHF Bedside assessment to identify haemodynamic profile CONGESTION? YES (95% of AHF patients) Wet Dry NO (5% of AHF patients) POOR PERFUSION? NO YES NO YES Wet & Warm Wet & Cold Dry & Warm Dry & Cold Adapted from 2016 ESC HF Guildeines
5 Definitions of Terms Used in Cardiogenic Shock Diagnosis Term Definition Symptoms/signs of congestion (left-sided) Symptoms/signs of congestion (right-sided) Symptoms/signs of hypoperfusion Hypotension Hypoxaemia Orthopnoea, paroxysmal nocturnal dyspnoea, pulmonary rales (bilateral), peripheral oedema (bilateral). Jugular venous dilatation, peripheral oedema, congested hepatpmegaly, hepatojugular reflux, ascites, symptoms of gut congestionsymptoms of gut congestion. Clinical: cold sweated extremities, oliguria, mental confusion, dizziness, narrow pulse pressure. Laboratory measures: metabolic acidosis, elevated serum lactate, elevated serum creatinine. Hypoperfusion is not synonymous with hypotension, but often hypoperfusion is accompanied by hypotension. Systolic BP <90 mmhg Arterial PaO2 <80 mmhg (<10,67 kpa) Acidosis ph <7.35 Elevated blood lactate Oliguria Urine output >2 mmol/l <0.5 ml/kg/h

 Consider mechanical circulatory support")

6 Wet & Cold Systolic blood pressure <90 mmhg? YES NO Inotropic agent Consider vasopressor in refractory cases Diuretic (when perfusion corrected) Consider mechanical circulatory support if no response to drugs Vasodilators Diuretics Consider inotropic agent in refractory cases Adapted from 2016 ESC HF Guildeines
7 Targeted Medical Treatment in CS Congestion (high or normal LVEDP) Poor perfusion (low cardiac output)
 imaging allows direct visualization of sublingual microcirculation Ince C.")
8 Microcirculation The ultimate therapeutic goal in CS is to restore microcirculatory function (adequate oxygen supply to sustain cellular function) Active recruitment of microcirculation is essential Sublingual perfused capillary density (PCD) imaging allows direct visualization of sublingual microcirculation Ince C. Crit Care Med 1999; 27:
 Spronk PE.")
9 Microcirculatory Shutdown Increased oxygen consumption and impaired oxygen delivery and extraction due to microcirculatory shutdown and shunting During sepsis (and CS) microvasculature is the first to go and the last to recover Before and after nitroglycerin Orthogonal polarisation spectral imaging (OPS) Spronk PE. Lancet 2001; 360:
10 Microcirculation in Cardiogenic Shock Survival stratified according to quartile of baseline sublingual PCD den Uil CA. Eur Heart Jour 2010;31:
, metabolized independent of liver and renal function Pharmacodynamic properties: increases contractility, increases mean arterial pressure, maintenance of diastolic blood pressure,")
11 Portrait of The Ideal Cathecolamine Pharmaceutically: non-toxic, stable preparation, compatible with other drugs, peripherally deliverable, easy titration (on-off effect), steady effect (no tachyphylaxis), metabolized independent of liver and renal function Pharmacodynamic properties: increases contractility, increases mean arterial pressure, maintenance of diastolic blood pressure, increases cardiac output, improves regional perfusion, no increase in myocardial oxygen consumption, no tachycardia, non-arrhythmogenic, suitable in pregnancy and paediatric populations Beneficial effect on hard clinical end-points (save lives) Cost effective

12
13 What We Have Increase myocardial oxygen consumption Increase myocardial ischaemia Can trigger arrhythmias (ventricular and supraventricular) Can cause infarct expansion Can worsen peripheral tissue perfusion and microcirculation No clear clinical benefit
14 Currently Available Inotropes and Vasopressors Drug Mechanism Effect Dobutamine β1 (and β2) receptor Inotropic, chronotropic, mild vasodilatation Dopamine D 1-2 (0.5 to 3 μg/kg/min), β1 (3-10 μg/kg/min) and α1 (>10 μg/kg/min) receptors Dose dependent (inotropic, chronotropic, vasoconstriction) Milrinone Phosphodisterase 3 inhibitor Inotropic, vasodilatation Levosimendan Ca 2+ sensitizer, ATP-dependent K + channels Inotropic, vasodilatation Noradrenaline α1 (mild β1) Vasocontriction Adrenaline α1, β1 and β2 Inotropic (low dose), vasoconstriction (higher doses)

15 Levosimendan: SURVIVE Trial Randomized, double-blind trial comparing levosimendan versus dobutamine 1327 AHF patients with LVEF <30%, insufficient response to iv diuretics and: dyspnoea at rest or mechanical ventilation, oliguria, PCWP > 18 mmhg and/or CI <2.2 L/min/m 2 Vey sick cardiogenic shock patients excluded Mebazaa A. JAMA 2007;297:
16 Levosimendan: SURVIVE Trial Mebazaa A. JAMA 2007;297:
 Primary end-point changes in clinical status during first 5 days Packer M.")
17 Levosimendan: REVIVE Trial Randomized, double-blind trial comparing levosimendan vs placebo (inclusion , published 2013) 600 AHF patients with LVEF <35% (CS excluded) Primary end-point changes in clinical status during first 5 days Packer M. J Am Coll Cardiol HF 2013;1:103 11

18 Levosimendan: REVIVE Trial Significant benefit in favour of levosimendan for primary end-point but increased risk of adverse cardiovascular events Significant drop in BNP but no effect on mortality Packer M. J Am Coll Cardiol HF 2013;1:103 11

19 Levosimendan in Cardiogenic Shock Small (32 patients), single center, open label, randomized trial Fuhrmann JT. Crit Care Med 2008; 36:
20 Noradrenaline Comparison of norepinephrine and dopamine in the treatment of shock De Backer D. N Engl J Med 2010; 372:779
21 Effect of AHF Treatment on Mortality: Propensity Score Analysis ALARM-HF Registry Whole Cohort Mebazaa A. Intensive Care Med Feb;37(2):290-30
22 Inodilators in Cardiogenic Shock: Propensity Score Analysis ALARM-HF, EFFICA, AHEAD Registries (988 CS patients) HR: 0.66 [ ] Perracchio R. PLoS One. 2013;8(8):e71659
23 Vasoactive All (n=220) ACS (n=178) non-acs (n=42) p Vasopressors Noradrenaline 75% 76% 69% NS Adrenaline 21% 23% 14% NS Dopamine 26% 29% 12% 0.03 Vasopressin/Terlipressin 4% 5% - NS Simultaneous vasopressors 30% 33% 14% 0.02 Inotropes Use of Inotropes and Vasopressors in the CardShock Study Dobutamine 49% 51% 43% NS Levosimendan 24% 22% 31% NS PDE3i 4% 4% 5% NS Simultaneous vasopressor and inotrope 55% 56% 50% NS Tarvasmaki T et al. Crit Care Med 2016;20:208
24 Use of Inotropes and Vasopressors in the CardShock Study 94% of patients received vasoactive medication Initiated within the first 24 hours Vasopressors in 98% of cases Inotropes in 94% of cases Overall, associations with clinical presentation were modest NO marked associations with medical history, initial BP or HR, LVEF Tarvasmaki T et al. Crit Care Med 2016;20:208
25 Adrenaline Independent Predictor of Mortality Predictors of 90-day Mortality: Multivariable Logistic Regression Model Variable OR 95% CI p Adrenaline use Age History of MI History of CABG ACS etiology Initial confusion Systolic BP (per mmhg decrease) LVEF (per % decrease) <0.001 Blood lactate (mmol/l increase) <0.001 Tarvasmaki T et al. Crit Care Med 2016;20:208
26 Adrenaline Independent Predictor of Mortality Survival curves for use of adrenaline Propensity score: age, gender, medical history (myocardial infarction, coronary artery bypass graft surgery, hypertension, renal insufficiency), acute coronary syndrome as the etiology of cardiogenic shock, resuscitation prior to inclusion and initial presentation (confusion, blood lactate, creatinine, systolic blood pressure, sinus rhythm, and left ventricular ejection fraction). Tarvasmaki T et al. Crit Care Med 2016;20:208
27 Adrenaline Use Related to Deterioration in Cardiac and Renal Biomarkers in CS Tarvasmaki T et al. Crit Care Med 2016;20:208
28 Adrenaline Use Related to Deterioration in Cardiac and Renal Biomarkers in CS Overall 90-day mortality was 46% and significantly higher in adrenaline group vs other vasopressors: 90% vs 35%, p<0.001 The strong association of adrenaline with increased mortality remained even after propensity score adjustment Adrenaline use was associated with markedly worse evolution of cardiac and renal biomarker levels over the initial 96 hours likely due to an increase in myocardial oxygen consumption, excessive vasoconstriction and/or direct organ toxic damage due to intense adrenergic stimulation This may, in part, explain significantly higher mortality among patients receiving adrenaline
 Den Uil CA.")
29 Inotropes: Why Have We Failed? 30 CS patients (baseline parameters) Den Uil CA. PLoS One Aug 1;9(8):e103978
30 Inotropes: Why Have We Failed? Changes in perfused capillary density for individual patients Den Uil CA. PLoS One Aug 1;9(8):e103978
31 Inotropes: Why Have We Failed? Effects on Parameters of Macro- and Microcirculation Den Uil CA. PLoS One Aug 1;9(8):e103978
32 What Do The ESC Guidelines Say? Recommendations for inotropic and agents and vasopressors in patients with cardiogenic shock Short-term, i.v. infusion of inotropic agents may be considered in patients with hypotension (SBP <90 mmhg) and/or signs/symptoms of hypoperfusion despite adequate filling status, to increase cardiac output, increase blood pressure, improve peripheral perfusion and maintain end-organ function. IIb C An intravenous infusion of levosimendan or a PDE III inhibitor may be considered to reverse the effect of beta-blockade if beta-blockade is thought to be contributing to hypotension with subsequent hypoperfusion. IIb C Inotropic agents are not recommended unless the patient is symptomatically hypotensive or hypoperfused because of safety concern. III A 556, 557
33 What Do The ESC Guidelines Say? Recommendations for inotropic and agents and vasopressors in patients with cardiogenic shock A vasopressor (norepinephrine preferably) may be considered in patients who have cardiogenic shock, despite treatment with another inotrope, to increase blood pressure and vital organ perfusion. IIb B 558 It is recommended to monitor ECG and blood pressure when using inotropic agents and vasopressors, as they can cause arrhythmia, myocardial ischaemia, and in the case of levosimendan and PDE III inhibitors also hypotension. I C 540, In such cases intra-arterial blood pressure measurement may be considered. IIb? C
34 Take Home Messages Lack of evidence for clinical benefit for currently available inotropes and vasopressors In spite of this, virtually all cardiogenic shock patients receive treatment with cathecolamines usually a combination of inotrope and vasopressor Adrenaline use seems to be associated with increased mortality Trials to determine an evidence-based approach to vaso-active agent use are urgently needed Treatment tailored by assessment and optimization of microcirculation targets

35
36 Slide title here with space for two lines of text Bullet point one, lorem ipsum dolor sit amet Bullet point two, lorem ipsum dolor sit amet Sub-bullet point one, lorem ipsum dolor sit amet Sub-bullet point two, lorem ipsum dolor sit amet Bullet point one, lorem ipsum dolor sit amet Bullet point two, lorem ipsum dolor sit amet Sub-bullet point one, lorem ipsum dolor sit amet Sub-bullet point two, lorem ipsum dolor sit amet ACCA Masterclass 2017
37 Targeted Medical Treatment in CS Congestion (high or normal LVEDP) Poor perfusion (low cardiac output) Increase CO and reduce LVEDP without worsening hypotension Improve tissue perfusion Improve survival

38 Microcirculation Sublingual perfused capillary density measured with sidestream dark-field imaging den Uil CA. Eur Heart Jour 2010;31:

39 Microcirculation in Cardiogenic Shock den Uil CA. Eur Heart Jour 2010;31:


40 Low-dose Dopamine: Rose-AHF Trial Chen HH. JAMA 2013;310(23):

41 Low-dose Dopamine: Rose-AHF Trial No significant effect of dopamine on secondary endpoints: Decongestion Renal function Symptom relief Chen HH. JAMA 2013;310(23):
42 Cuffe MS. JAMA 2002;287:1541-7

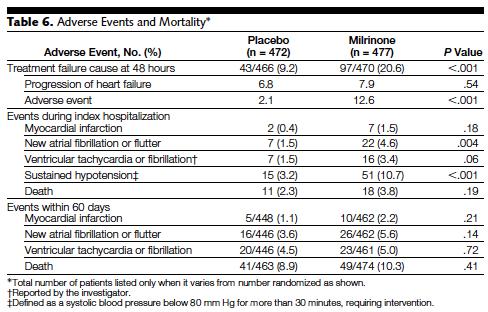
43 Cuffe MS. JAMA 2002;287:1541-7
44 Dobutamine: Meta-analysis of 21 trials (632 AHF patients) Mortality Thackray S. Eur J Heart Fail. 2002;4(4):515-29
45 Milrinone vs Dobutamine or Dopamine Mortality Pooled fixed effect on mortality OR 1.37 (95% CI 0.23 to 8.46) Thackray S. Eur J Heart Fail. 2002;4(4):515-29
46 CardShock Study 220 patients with CS ACS 81% non-acs 19% STEMI 68% NSTEMI 13% Mechanical complications 9% Severe low-output failure 10% Other 9% Ischemic CMP Dilated CMP... Valvular cause 5% Takotsubo 2% Myocarditis 2% Harjola V-P. Eur J Heart Fail. 2015;17:501
Intravenous Inotropic Support an Overview
 Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Intravenous Inotropic Support an Overview Shaul Atar, MD Western Galilee Medical Center, Nahariya Affiliated with the Faculty of Medicine of the Galilee, Safed, Israel INOTROPES in Acute HF (not vasopressors)
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment
 ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
ESC 2012 27Aug - 3Sep, 2012, Munich, Germany Treating the patient with acute heart failure. What do we really know? Principles of acute heart failure treatment Marco Metra, MD, FESC Cardiology University
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Management of acute decompensated heart failure and cardiogenic shock. Arintaya Phrommintikul Department of Medicine CMU
 Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Management of acute decompensated heart failure and cardiogenic shock Arintaya Phrommintikul Department of Medicine CMU Acute heart failure: spectrum Case 64 y/o M with Hx of non-ischemic DCM (LVEF=25-30%)
Acute heart failure, beyond conventional treatment: persisting low output
 Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Acute heart failure, beyond conventional treatment: persisting low output Alexandre Mebazaa, FESC Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Inotropes for the treatment of advanced heart failure: The role of intermittent administration
 Inotropes for the treatment of advanced heart failure: The role of intermittent administration Dr John T Parissis, Heart Failure Unit, Attikon University Hospital Athens, Greece Disclosures - ALARM investigator
Inotropes for the treatment of advanced heart failure: The role of intermittent administration Dr John T Parissis, Heart Failure Unit, Attikon University Hospital Athens, Greece Disclosures - ALARM investigator
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft
 Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Hemodynamic improvement upon levosimendan treatment in low cardiac output patients following coronary artery bypass graft M. Buerke, K. Krohe, M. Russ, C. Schneider, H. Lemm, R. Prondzinsky, I. Friedrich,
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
13/12/15. Diagnóstico, identificación y selección de pacientes con shock cardiogénico susceptibles de tratamiento avanzado. De Que Estamos Hablando?
 Diagnóstico, identificación y selección de pacientes con shock cardiogénico susceptibles de tratamiento avanzado Barcelona, 11 de diciembre 2015 Alessandro Sionis Unidad de Cuidados Intensivos Cardiolgicos
Diagnóstico, identificación y selección de pacientes con shock cardiogénico susceptibles de tratamiento avanzado Barcelona, 11 de diciembre 2015 Alessandro Sionis Unidad de Cuidados Intensivos Cardiolgicos
Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια. Ι.Κανονίδης
 Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια Ι.Κανονίδης Cardiac Glycosides Chronic Congestive Heart Failure DIGOXIN Na-K ATPase Na + K + Na-Ca Exchange Na + Ca ++ Ca ++ K + Na + Myofilaments
Δακτυλίτιδα και Ινότροπα Φάρμακα στην Καρδιακή Ανεπάρκεια Ι.Κανονίδης Cardiac Glycosides Chronic Congestive Heart Failure DIGOXIN Na-K ATPase Na + K + Na-Ca Exchange Na + Ca ++ Ca ++ K + Na + Myofilaments
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK
 PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
PHARMACOLOGICAL MANAGEMENT OF CARDIOGENIC SHOCK Doron Zahger, MD Department of Cardiology, Soroka University Medical Center, Faculty of Health Sciences, Ben Gurion University of the Negev, Beer Sheva,
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS
 Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Department of Intensive Care Medicine UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS UNDERSTANDING CIRCULATORY FAILURE IN SEPSIS a mismatch between tissue perfusion and metabolic demands the heart, the vasculature
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Means failure of heart to pump enough blood to satisfy the need of the body.
 Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Means failure of heart to pump enough blood to satisfy the need of the body. Due to an impaired ability of the heart to adequately to fill or eject blood. HEART FAILURE Heart failure (HF) means decreased
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
ACUTE HEART FAILURE. Julie Gorchynski MD, MSc, FACEP, FAAEM. Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014
 ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
ACUTE HEART FAILURE Julie Gorchynski MD, MSc, FACEP, FAAEM Department of Emergency Medicine Emergency Residency Program UTHSC, San Antonio TCEP 2014 No disclosures Objectives Overview Cases Current Therapy
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
When Fluids are Not Enough: Inopressor Therapy
 When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
When Fluids are Not Enough: Inopressor Therapy Problems in Neonatology Neonatal problem: hypoperfusion Severe sepsis Hallmark of septic shock Secondary to neonatal encephalopathy Vasoplegia Syndrome??
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
DECLARATION OF CONFLICT OF INTEREST Cardiogenic Shock Mechanical Support Eulàlia Roig FESC Heart Failure and HT Unit Hospital Sant Pau - UAB Barcelona. Spain No conflics of interest Mechanical Circulatory
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland
 2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
2016 ESC Heart Failure Guidelines: what is new? Piotr Ponikowski Wroclaw, Poland Disclosures Consultancy fees and speaker s honoraria from: Amgen, Servier, Novartis, Johnson & Johnson, Merck, Berlin Chemie,
Disclosures. Objectives 10/11/17. Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock. I have no disclosures to report
 Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Short Term Mechanical Circulatory Support for Advanced Cardiogenic Shock Christopher K. Gordon MSN, ACNP-BC Disclosures I have no disclosures to report 1. Pathophysiology 2. Epidemiology 3. Assessment
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure
 Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Integrating Current Knowledge into Consensus Guidelines for Acute Decompensated Heart Failure J. Herbert Patterson, Pharm.D., FCCP One of Four Continuing Education Programs in the Series, Acute Decompensated
Management of Acute Heart Failure
 Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Management of Acute Heart Failure Uri Elkayam, MD Professor of Medicine University of Southern California School of Medicine Los Angeles, California elkayam@usc.edu ADHF Treatments Goals.2 Improve symptoms.
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Pharmacology of inotropes and vasopressors
 Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Pharmacology of inotropes and vasopressors Curriculum 3.3 Recognises and manages the patient with circulatory failure 4.4 Uses fluids and vasoactive / inotropic drugs to support the circulation PR_BK_41
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Vasoactive drugs. Dr. Zohair Alaseri, MD
 Vasoactive drugs Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department of Emergency Medicine King Saud University
Vasoactive drugs Dr. Zohair Alaseri, MD FRCPc, Emergency Medicine FRCPc, Critical Care Medicine Intensivest and Emergency Medicine Consultant Chairman, Department of Emergency Medicine King Saud University
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Heart failure hospitalizations with preserved or reduced ejection fraction
 Clinical profile and in-hospital outcomes in patients admitted for heart failure with preserved or reduced ejection fraction. EPI-CARDIO prospective registry Tajer, C; Mariani, J; de Abreu, M; Charask,
Clinical profile and in-hospital outcomes in patients admitted for heart failure with preserved or reduced ejection fraction. EPI-CARDIO prospective registry Tajer, C; Mariani, J; de Abreu, M; Charask,
Medical Management of Acutely Decompensated Heart Failure. William T. Abraham, MD Director, Division of Cardiovascular Medicine
 Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Medical Management of Acutely Decompensated Heart Failure William T. Abraham, MD Director, Division of Cardiovascular Medicine Orlando, Florida October 7-9, 2011 Goals of Acute Heart Failure Therapy Alleviate
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017
 VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
VASOPRESSORS AND INOTROPES CLINICAL PROFESSOR ANDREW BEZZINA FACEM MAY 2017 CONFLICTS OF INTEREST OVERVIEW Why? When? What? How? WHY? Circulation WHY? - SHOCK!!! Pump (Heart) HYPOVOLAEMIC the pipes have
State of the Art: acute heart failure Is it just congestion?
 ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
ESC CONGRESS 2017 Barcelona, 26. 30. August 2017 State of the Art: acute heart failure Is it just congestion? S.B. Felix, FESC Klinik für Innere Medizin B Ernst-Moritz-Arndt-Universität Greifswald 1456
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient
 Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Prevention of Atrial Fibrillation and Heart Failure in the Hypertensive Patient The Issue of Primary Prevention of A.Fib. (and Heart Failure) and not the Prevention of Recurrent A.Fib. after Electroconversion
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Dobutamine Kills Good Hearts! Levosimendan May Not
 ISPUB.COM The Internet Journal of Cardiology Volume 2 Number 1 Dobutamine Kills Good Hearts! Levosimendan May Not S Kumar Citation S Kumar. Dobutamine Kills Good Hearts! Levosimendan May Not. The Internet
ISPUB.COM The Internet Journal of Cardiology Volume 2 Number 1 Dobutamine Kills Good Hearts! Levosimendan May Not S Kumar Citation S Kumar. Dobutamine Kills Good Hearts! Levosimendan May Not. The Internet
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
CARDIOGENIC SHOCK. Antonio Pesenti. Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI)
") CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
CARDIOGENIC SHOCK Antonio Pesenti Università degli Studi di Milano Bicocca Azienda Ospedaliera San Gerardo Monza (MI) Primary myocardial dysfunction resulting in the inability of the heart to mantain an
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR
 ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
Dobutamine-induced increase in heart rate is blunted by ivabradine treatment in patients with acutely decompensated heart failure
 Dobutamine-induced increase in heart rate is blunted by ivabradine treatment in patients with acutely decompensated heart failure Yuksel Cavusoglu, KU Mert, A Nadir, F Mutlu, E Gencer, T Ulus, A Birdane
Dobutamine-induced increase in heart rate is blunted by ivabradine treatment in patients with acutely decompensated heart failure Yuksel Cavusoglu, KU Mert, A Nadir, F Mutlu, E Gencer, T Ulus, A Birdane
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Acute peri-operative. Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm
 Acute peri-operative left heart failure Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts for this lecture Acute peri-operative
Acute peri-operative left heart failure Alexandre Mebazaa, Hôpital Lariboisière, Université Paris 7 U942 Inserm Conflict of Interest Lecture fee: Orion No other conflicts for this lecture Acute peri-operative
Slide 1. Slide 2. Slide 3. Managing Acute Heart Failure Trials and Tribulations. Declaration of
 Slide 1 Managing Acute Heart Failure Trials and Tribulations Martin R Cowie MD MSc FRCP FRCP (Ed) FESC Professor of Cardiology, Imperial College London m.cowie@imperial.ac.uk @ProfMartinCowie Slide 2 Declaration
Slide 1 Managing Acute Heart Failure Trials and Tribulations Martin R Cowie MD MSc FRCP FRCP (Ed) FESC Professor of Cardiology, Imperial College London m.cowie@imperial.ac.uk @ProfMartinCowie Slide 2 Declaration
Acute HF is a complex and often life-threatening clinical condition. 1 Existing
 ACUTE HEART FAILURE: WHAT IS NEW? John Parissis, MD, PhD; Vasiliki Bistola, MD Author affiliations: Heart Failure Unit, University of Athens, Athens, Greece Address for correspondence: John Parissis, Navarinou
ACUTE HEART FAILURE: WHAT IS NEW? John Parissis, MD, PhD; Vasiliki Bistola, MD Author affiliations: Heart Failure Unit, University of Athens, Athens, Greece Address for correspondence: John Parissis, Navarinou
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT
 Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Charles Spencer MD, FRCP Consultant Cardiologist Mid Staffs NHSFT Key Messages Heart Failure is Common Heart failure is complex Heart Failure is a major issue for the NHS Heart Failure has a worse prognosis
Controversies in Cardiogenic Shock. Timothy D. Henry, MD Cedars-Sinai Heart Institute
 Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
Controversies in Cardiogenic Shock Timothy D. Henry, MD Cedars-Sinai Heart Institute Key Issues Cardiac Arrest-Cardiogenic shock interaction New SCAI Classification Refractory Shock Shock with Multivessel
Acute heart failure syndromes: clinical challenges. Pathophysiology. ESC Congress August. Paris, France. Marco Metra
 ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
ESC Congress 2011 27-31 August. Paris, France. Acute heart failure syndromes: clinical challenges. Pathophysiology Marco Metra Cardiology, Dept. Of experimental and applied medicine. University of Brescia.
ACUTE HEART FAILURE in the ED. Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia
 ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
ACUTE HEART FAILURE in the ED Pr. Samir Nouira Emergency Department Fattouma Bourguiba University Hospital Monastir Tunisia ACUTE HEART FAILURE 80% Acute Heart Failure Syndrome Sensitivity Specificity
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
CLASIFICATION OF ACUTE HEART FAILURE
 CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
CLASIFICATION OF ACUTE HEART FAILURE CLINICAL STATUS HR SBP mmhg CI L/min/m 2 PCWP mmhg Congestion Killip/Forrester Diuresis Hupoperfusion End-organ hypoperfusion I. Acute decompensated CHF +/ Low normal
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Sepsis and septic shock
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
WHY ADMINISTER CARDIOTONIC AGENTS?
 Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Cardiac Pharmacology: Ideas For Advancing Your Clinical Practice The image cannot be displayed. Your computer may not have enough memory to open the image, or Roberta L. Hines, M.D. Nicholas M. Greene
Stopping the Revolving Door of ADHF
 Stopping the Revolving Door of ADHF Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center
Stopping the Revolving Door of ADHF Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017
 Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Mechanical circulatory support in cardiogenic shock The Cardiologist s view ACCA Masterclass 2017 Pascal Vranckx MD, PhD. Medical director Cardiac Critical Care Services Hartcentrum Hasselt Belgium Disclosure
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial
: A Randomized Clinical Trial") Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Acute Myocardial Infarction Complicated by Cardiogenic Shock
 Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Acute Myocardial Infarction Complicated by Cardiogenic Shock Navin K. Kapur, MD, FACC, FSCAI Assistant Professor, Division of Cardiology Director, Acute Circulatory Support Program Director, Interventional
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors:
 Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Utilizing Vasopressors: Critical Care Advances in the Emergency Department José A. Rubero, MD, FACEP, FAAEM Associate Program Director University of Central Florida/HCA GME Consortium Emergency Medicine
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella