Advanced Cardiac Life Support
|
|
|
- Julianna Willa Henderson
- 6 years ago
- Views:
Transcription

1 Advanced Cardiac Life Support

2 Algorithm
3
4
5
6
7
8
9

10
11
12
13 Drugs
14 Class I: definitely helpful, excellent Class II: Class II a -probably helpful; good to very good Class II b -possibly helpful; fair to good Class Indeterminate: insufficient evidence; no harm, but no benefit Class III: possibly harmful

15 Epinephrine - Why? How? What? Vasopressin - Why? How? What? Amiodarone Magnesium Procainamide Lidocaine
16 WHY? Natural catecholamine with and ß-adrenergic agonist activity Results in: flow to heart and brain SVR, SBP, DBP electrical activity in the myocardium & automaticity ( success with defibrillation) myocardial contraction (for refractory circulatory shock (CABG)) increases myocardial oxygen requirements Primary benefit: -vasoconstriction ß-adrenergic activity controversial b/c myocardial work WHEN? VF/VT, asystole, PEA, bradycardias
17 WHEN? Alternative to epinephrine for shock-refractory VT/VF WHY? Natural antidiuretic hormone Potent vasoconstrictor by stimulation of SM -V 1 receptors : BP & SVR; CO, HR, myocardial O2 consumption and contractility Does not myocardial oxygen consumption Not affected by severe acidosis Class IIb for shock-refractory VF Class Indeterminate for PEA, asystole Half life = minutes Dose? 40 Units IVP - one time only!!!
18 Class Drug Conduction Velocity Ia Ib Quinidine Procainamide Disopyramide Lidocaine Mexiletine Tocainide 0/ Refractory Period Automaticity Ion Block Sodium Sodium (fast on-off) Ic Flecainide Propafenone Moricizine 0 Sodium (slow on-off) II Beta-Blockers Calcium III IV Amiodarone Bretylium Sotalol 0 0 Verapamil Diltiazem Potassium Calcium
19 WHY? Class III antiarrhythmic (characteristics of all classes) Na, K and Ca channel blocker & & -adrenergic blocker Prolongs AP and RP Decreases AV conduction velocity & SN function New Recommendations (WHEN?): pulseless VT or VF (IIb) hemodynamically stable VT (IIb), polymorphic VT (IIb), widecomplex tachycardia uncertain origin (IIb) refractory PSVT (preserved function, IIa; impaired function IIb) atrial tachycardia (IIb) cardioversion of AF (IIa)
20 HOW? Cardiac arrest (PVT/VF) - 300mg IVP diluted in 20-30ml, may repeat with 150mg in 10 minutes, or start infusion (max=2..2 g/24h) Atrial & ventricular arrhythmias in impaired hearts WHAT? 150mg IVP over 10 min May repeat q10-15 min, or start gtt 1mg/min x 6 hours, then 0.5mg/min x 18 h Hypotension, bradycardia (slow rate, fluids)
21 WHY? WHEN? HOW? WHAT? Magnesium deficiency causes arrhythmias Facilitates ventricular repolarization by enhancing intracellular potassium flux, dilates coronary arteries Suspected hypomagnesemia, pulseless VT/VF, torsade de pointes Class IIa in suspected hypomagnesemia, TdP, and Class IIb in VF/VT: 1-2gm slow IVP in 100ml Hypotension at large doses
22 WHY? Type IB antiarrhythmic Affects fast Na+ channels, shortens refractory period Suppresses spontaneous depolarization Local anesthetic, increases fibrillation threshold Suppresses ventricular ectopy post-mi Without effecting myocardial contractility, BP or AV nodalconduction WHEN? SECOND-CHOICE agent VT/VF refractory to electrical countershock and epinephrine (Indeterminate) Control of PVC s (Indeterminate) Hemodynamically stable VT (IIb) Not for routine prophylaxis post-mi, however, accepted in high-risk patients (hypokalemia, myocardial ishchemia, LV dysfunction)
23 HOW? WHAT? Class IIa: mg/kg IVP q5-10 min (max=3mg/kg) Infusion (with pulse): 1-4 mg/min (if pulse is regained) Therapeutic Levels: µg/ml ET Dose: times IV dose Preparation: 1-2 gm/250 ml D5W or NS Hepatic metabolism, renal elimination Bradycardia, cardiac arrest, seizures Lidocaine toxicity/neurotoxicity - twitching, LOC, seizures, coma Lidocaine levels persist in low CO states
24 Calcium channel blockers Beta-blockers Digoxin Amiodarone Procainamide Flecainide (IV form in ACLS -not available in US) Propafenone (IV form in ACLS -not available in US) Sotalol (IV form in ACLS -not available in US)
25 WHY? Verapamil: Diltiazem: WHEN? Blocks inward flow of Ca and Na, slows conduction, RP in AVN Terminate reentrant arrhythmias requiring AVN conduction Control ventricular response rate in AF/AFl Coronary vasodilation May exacerbate CHF Negative inotrope & chronotrope (good anti-ischemic) Class I for acute and preventative SVT Direct negative chronotropic effect, mild negative inotrope Highly effective in controlling ventricular response in A Fib Control ventricular response rate in patients with AF/Fl, or MAT Verapamil: PSVT not requiring cardioversion
26 HOW? Verapamil: mg IVP, over 2 min (max=30mg) 5-10 mg/hr Diltiazem: 0.25 mg/kg IVP, may repeat with 0.35mg/kg in 15 min 5-15 mg/hr WHAT? Contraindicated in wide QRS complex tachycardias and ventricular tachycardias, exacerbation of CHF in patients with LV dysfunction Transient decrease in BP Avoid in sick sinus syndrome of AV block (w/out pacer) May potentiate digoxin toxicity. Incompatible with bicarbonate, epinephrine, furosemide
27 WHY? WHEN? B-adrenergic blockade, slows conduction and increases refractory period in AV node AMI (reduces rate of reinfarction), reduces recurrent ischemia and incidence of VF in post- MI patients, USA HOW? Atenolol: mg IV over 5 min Metoprolol: 5-10 mg IVP q 5 min Propranolol: 0.1 mg/kg IV divided into min intervals Esmolol: 500 mcg/kg over 1 min 50 mcg/kg/min WHAT? Hypotension, bradycardia, AV block, overt heart failure or severe bronchospasm/copd
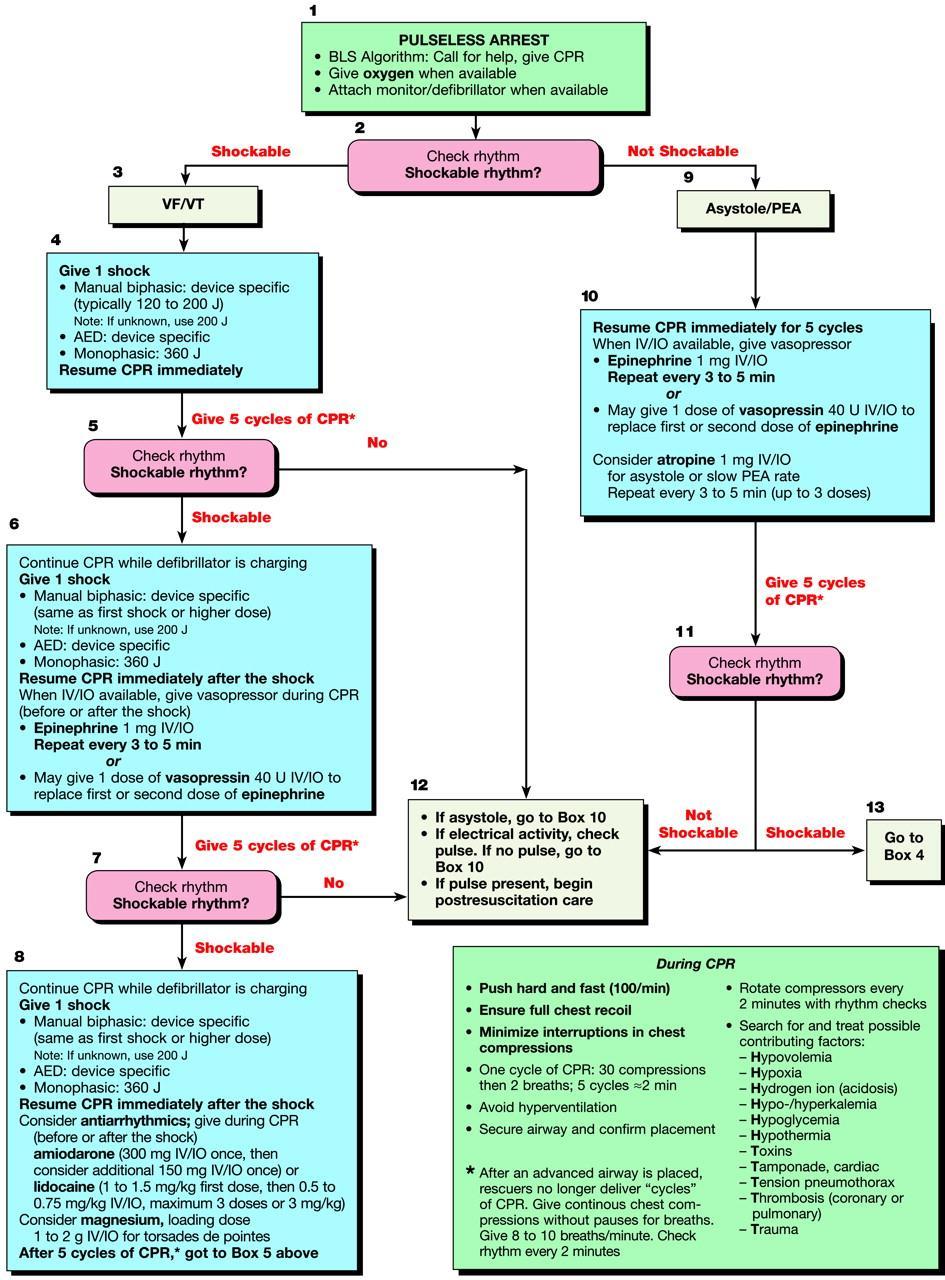
28 PEA no pulse with + electrical activity (not VF/VT) Reversible if underlying cause is reversed (5 H s, 5 T s) Hypovolemia, hypoxia, hydrogen ion (acidosis), hyper/hypokalemia, hyper/hypothermia Tablets, tamponade, tension pneumothorax, thrombosis (ACS), thrombosis (PE) Problem Epinephrine Atropine Search for the probable cause and intervene (HCO3) 1 mg IV q3-5 min. With slow heart rate, 1 mg IV q3-5 min. (max. dose 0.04 mg/kg)
29 WHY? Anticholinergic/direct vagolytic Enhances sinus node automaticity and AVN conduction WHEN? PEA, symptomatic sinus bradycardia, asystole, HOW? Bradycardia: mg IV q3-5 min Asystole: 1 mg IV q 3-5 min Max = 0.04 mg/kg or 3 mg ET Dose=1-2mg diluted in 10ml Paradoxical bradycardia with insufficient dose (<0.5mg) WHAT? Tachycardia; 2nd or 3rd degree AV block (paradoxical slowing may occur), MI (may worsen ischemia/hr) Incompatible with bicarbonate, epinephrine & norepinephrine
30 Vagal stimulation Adenosine
31 WHY? WHEN? HOW? WHAT? Endogenous nucleoside, slows conduction through the AV node and can interrupt AV nodal reentry pathways PSVT (half-life=10 sec) If PSVT persists may want longer acting agent (verapamil or diltiazem) 6 mg rapid IV over 1-3 sec, followed by 20 ml NS flush. May repeat in 1-2min with 12 mg dose. Max.=30 mg Flushing, dyspnea, chest pain, post-conversion bradycardia Drug interaction with theophylline, dipyridamole
32 Atropine Dopamine Epinephrine
33 WHY? WHEN? NE precursor Stimulates DA, & -adrenergic receptors (doserelated) Want -stimulation, for bradycardia-induced hypotension Hypotension/shock HOW? renal: 2-5 mcg/kg/min cardiac: 5-10 mcg/kg/min (B 1 & alpha) vascular: mcg/kg/min (alpha) Preparation: WHAT? 400 mg/250 ml D5W or NS Tachycardia, tachyphylaxis, proarrhythmic If requiring > 20mcg/kg/min consider adding NE
34 Oxygen Nitroglycerin Morphine Sulfate Aspirin Clopidogrel Thrombolytics Heparin Beta-blockers Glycoprotein IIb/IIIa receptor antagonists ACE inhibitor HMG CoA reductase
35 Why? increases hemoglobin saturation, improves tissue oxygenation supply to ischemic tissues 16-17% oxygen from mouth-to-mouth When? How? Must give supplemental oxygen in ACLS Always for MI NC 4 L/min, intubation, etc Goal - Osat=97-98% Confirm tube placement

36 WHY? binds to receptors on vascular smooth muscle - vasodilation (venous > arterial) venous BF to heart (preload) & O2 consumption dilates coronary arteries - myocardial blood supply antagonizes vasospasm increases collateral flow to ischemic myocardium inhibits infarct expansion decreases pain
37 WHEN? Ischemic chest pain; pulmonary edema (when SBP>100); AMI SL NTG -drug of choice for angina IV NTG - drug of choice for unstable angina or AMI Congestive heart failure with ischemia HOW? IV: mcg/min, increase by 5-10 mcg/min q5-10 min until desired effect or hemodynamic compromise SL: 1 tablet (0.4mg) SL q5min times 3 Spray: 1 spray onto oral mucosa
38 Preparation: 50 mg/250 ml D5W or NS Cautions: hypotension - treat with fluids, and rate reduction/elimination bradycardia - vasovagal reflex to hypotension treat with fluids, rate reduction, atropine reflex tachycardia also a concern headache, dizziness - may be diminished by laying down patients develop tachyphylaxis to effects - promote nitrate-free periods, intermittent dosing and lowest-possible doses
39 WHY? (Pain can catecholamines - BP, HR, O2 demands) Opiate analgesic pain, preload and afterload, SVR, anxiety Relieves pulmonary congestion, myocardial oxygen demand WHEN? Pain, pulmonary edema, BP > 90 mm Hg HOW? 1-3mg IVP (2-15 mg IVP q15-30 min prn) CAUTION? Respiratory & CNS depression, bradycardia, hypotension, N/V
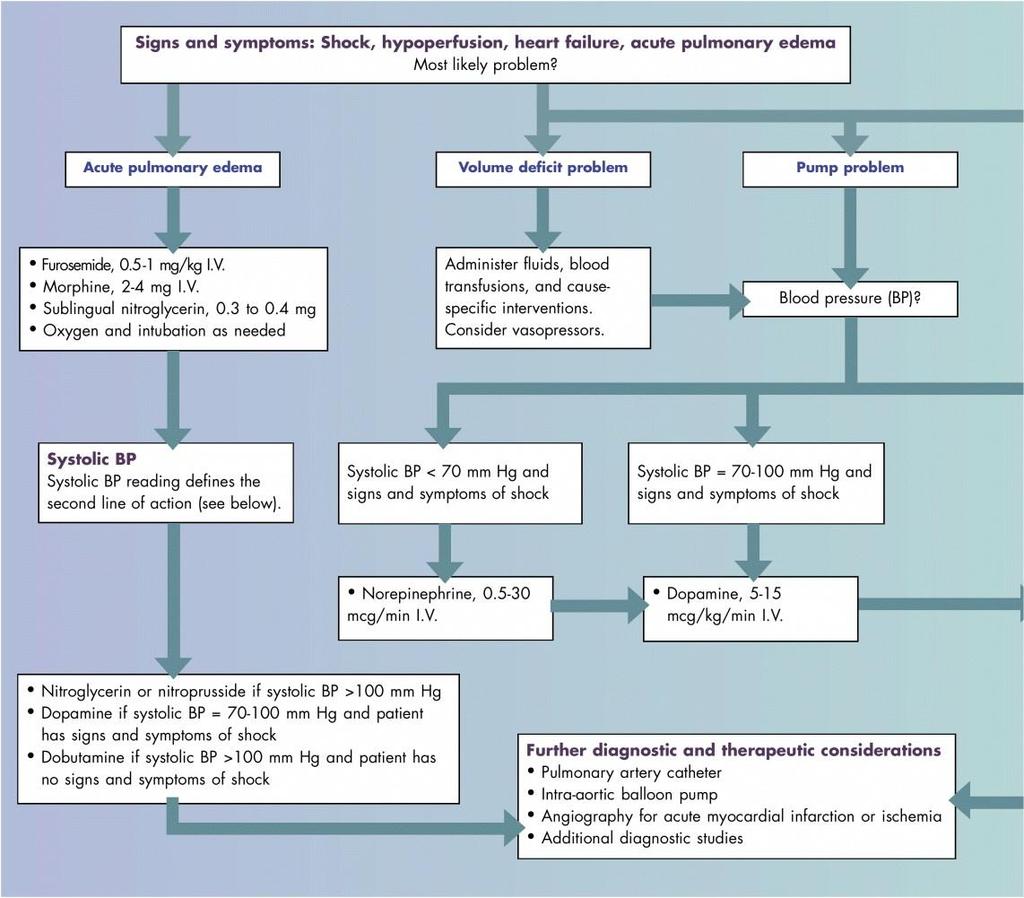
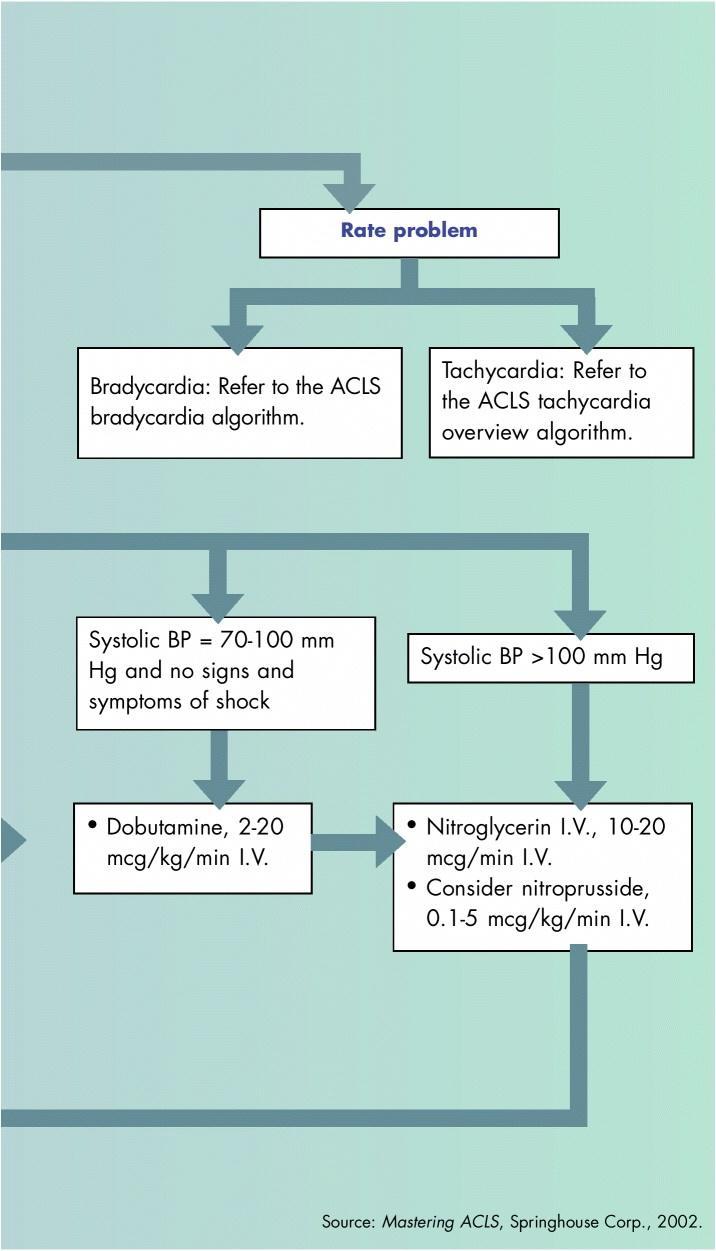
40 Volume: fluids, blood, vasopressors Pump: s/s of shock - vasopressors; no s/s shock - dobutamine BP (>100 mm Hg) - NTG, Nitroprusside pulmonary edema -furosemide 0.5-1mg/kg, morphine 1-3mg, NTG SL, oxygen/intubate Rate: see algorithms
41 Action: Indication: Dose: Preparation: Caution: Alpha & ß-adrenergic stimulation, increases contractility and HR, vasoconstriction, improves coronary blood flow Shock refractory to fluid replacement, severe hypotension mcg/min refractory shock = 8-30 mcg/min 4-8mg/250 ml D5W or NS Hypertension, myocardial ischemia, cardiac arrest, palpitations
42 Action: Indication: Dose: Preparation: Caution: B1- adrenergic activity Inotrope in heart failure/hypotension 2-20 mcg/kg/min 250 mg/250 ml D5W or NS tachyarrhythmias,worsens myocardial ischemia
43 Action: Indication: Dose: Preparation: Caution: Antihypertensive, peripheral vasodilator, reduces afterload, increases CO and relieves pulmonary congestion Hypertension, AMI, CHF mcg/kg/min, and titrate up to 10mcg/kg/min 50 mg/250 ml D5W Cyanide and thiocyanate toxicity, hypotension
44 WHY? WHEN? HOW? WHAT? Enhances sodium shift intracellularly, buffers acidosis, decreases toxicity of TCA s, increases clearance of acidic drugs Class I - hyperkalemia Class IIa - bicarbonate-responsive acidosis metabolic acidosis secondary to loss of bicarb (renal/gi); overdoses (TCAs, phenobarbital, aspirin) Class IIb - protracted arrest in intubated patients Class III - hypoxic lactic acidosis 1 meq/kg IVP, 0.5mEq/kg q10 min prn May worsen outcome if not intubated/ventilated. Metabolic alkalosis, decreased O2 delivery to tissues, hypokalemia, CNS acidosis, hypernatremia, hyperosmolarity Incompatible with calcium, epinephrine, atropine, norepinephrine, isoproterenol
45
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Mr. Eknath Kole M.S. Pharm (NIPER Mohali)
") M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
M.S. Pharm (NIPER Mohali) Drug Class Actions Therapeutic Uses Pharmacokinetics Adverse Effects Other Quinidine IA -Binds to open and inactivated Na+ -Decreases the slope of Phase 4 spontaneous depolarization
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
 Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
ACLS Emergency Cardiac Drug Therapy (bolded = changes based on 2005 AHA ACLS Guidelines) revised 01/18/07
 revised 01/18/07") Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
ANTI - ARRHYTHMIC DRUGS
 ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ANTI - ARRHYTHMIC DRUGS CARDIAC ACTION POTENTIAL K Out Balance Ca in/k out Na in K Out GENERATION OF ARRHYTHMIAS Four mechanisms of arrhythmia generation; Increased normal automaticity Abnormal automaticity
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care EMERGENCY PHARMACOLOGY I & II. ADENOSINE (Adenocard)
") EMERGENCY PHARMACOLOGY I & II Advanced Cardiac Life Support Seminole Community College Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care International Consensus
EMERGENCY PHARMACOLOGY I & II Advanced Cardiac Life Support Seminole Community College Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care International Consensus
7/21/2017. Learning Objectives. Current Cardiovascular Pharmacology. Epinephrine. Cardiotonic Agents. Epinephrine. Epinephrine. Arthur Jones, EdD, RRT
 Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Antiarrhythmic Drugs 1/31/2018 1
 Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Antiarrhythmic Drugs 1/31/2018 1 Normal conduction pathway: 1- SA node generates action potential and delivers it to the atria and the AV node 2- The AV node delivers the impulse to purkinje fibers Other
Chapter (9) Calcium Antagonists
 Calcium Antagonists") Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Chapter (9) Calcium Antagonists (CALCIUM CHANNEL BLOCKERS) Classification Mechanism of Anti-ischemic Actions Indications Drug Interaction with Verapamil Contraindications Adverse Effects Treatment of Drug
Management Of Medical Emergencies. Zakaria S. Messieha, DDS
 Management Of Medical Emergencies Zakaria S. Messieha, DDS Z.S. Messieha Associate Professor, Anesthesiology University Of Illinois At Chicago Necessity Of Emergency Protocol Aging patient population.
Management Of Medical Emergencies Zakaria S. Messieha, DDS Z.S. Messieha Associate Professor, Anesthesiology University Of Illinois At Chicago Necessity Of Emergency Protocol Aging patient population.
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Blanchard Valley Hospital Pharmacy Code Blue Overview
 Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Antiarrhythmic Pharmacology. The Electronics
 Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Arrhythmias. Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium.
 Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Arrhythmias Simple-dysfunction cause abnormalities in impulse formation and conduction in the myocardium. However, in clinic it present as a complex family of disorders that show variety of symptoms, for
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias. 1. beat too slowly (sinus bradycardia). Like in heart block
. Like in heart block") Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Arrhythmias It is a simple-dysfunction caused by abnormalities in impulse formation and conduction in the myocardium. The heart is designed in such a way that allows it to generate from the SA node electrical
Intravenous Infusions
 Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
Intravenous Infusions 1) An IV insulin infusion can be used for patients: a) with out of control diabetes b) with DKA (Diabetic Ketoacidosis) c) after a heart attack 2) Hyperglycemia is an adaptive response
PHARMACOLOGY OF ARRHYTHMIAS
 PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
PHARMACOLOGY OF ARRHYTHMIAS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: November 27, 2012 Materials on: Exam #5 Required reading: Katzung, Chapter 14 1 CARDIAC ARRHYTHMIAS Abnormalities
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Cardiac Drugs: Chapter 9 Worksheet Cardiac Agents. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate.
 Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Complete the following. 1. drugs affect the rate of the heart and can either increase its rate or decrease its rate. 2. drugs affect the force of contraction and can be either positive or negative. 3.
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
Chapter 26. Media Directory. Dysrhythmias. Diagnosis/Treatment of Dysrhythmias. Frequency in Population Difficult to Predict
 Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Chapter 26 Drugs for Dysrythmias Slide 33 Slide 35 Media Directory Propranolol Animation Amiodarone Animation Upper Saddle River, New Jersey 07458 All rights reserved. Dysrhythmias Abnormalities of electrical
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2018 2 Ion Permeability Changes Potential Changes Genes and Proteins 3 Cardiac Na+ channels 5 6
B. 14 Antidysrhythmic drugs. a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification
 B. 14 Antidysrhythmic drugs a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification I II III IV membrane stabilizers all ERP, ERP/APD, all except c APD classified
B. 14 Antidysrhythmic drugs a. Classify antidysrhythmics by their electrophysiological actions. Vaughan-Williams classification I II III IV membrane stabilizers all ERP, ERP/APD, all except c APD classified
Chapter 14. Agents used in Cardiac Arrhythmias
 Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Chapter 14 Agents used in Cardiac Arrhythmias Cardiac arrhythmia Approximately 50% of post-myocardial infarction fatalities result from ventricular tachycarida (VT) or ventricular fibrillation (VF). These
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
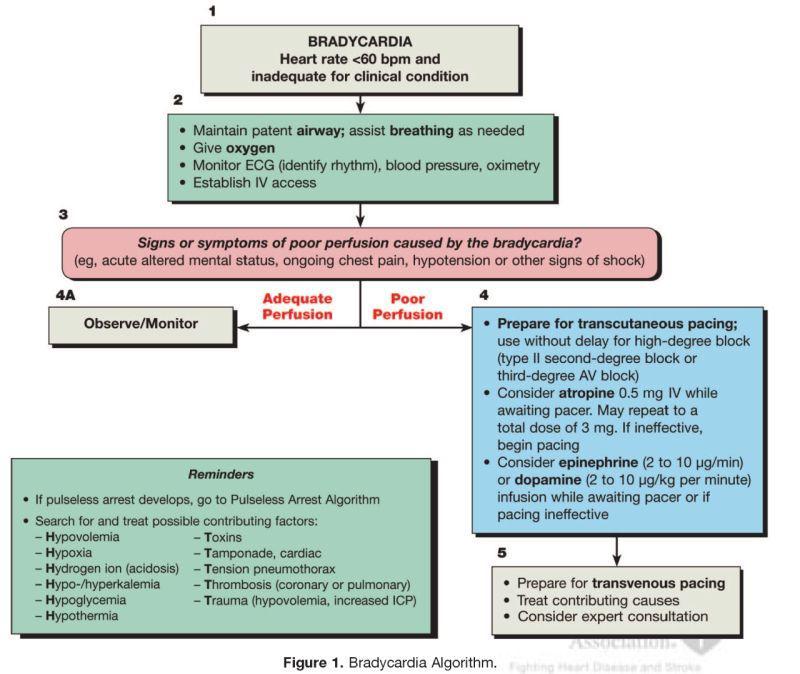
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Advanced Cardiac Life Support ACLS
 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
ACLS Study Guide Key guidelines recommendations for healthcare professionals:
 1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Antiarrhythmic Drugs. Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017
 Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Antiarrhythmic Drugs Munir Gharaibeh MD, PhD, MHPE School of Medicine, The University of Jordan November 2017 Types of Cardiac Arrhythmias Abnormalities of Impulse Formation: Rate disturbances. Triggered
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
WRITER TRISTAN WALKER TABLE OF CONTENTS. The Basics of cardiac pharmacology 2007
 WRITER TRISTAN WALKER TABLE OF CONTENTS 1. WHAT ARE THE MAJOR CLASSES OF CARDIAC DRUGS?...2 2. HOW DO THEY WORK?...3 3. CONSIDERATIONS FOR THE PEDIATRIC PATIENT...7 4. SUMMARY TABLE...10 REFERENCES...14
WRITER TRISTAN WALKER TABLE OF CONTENTS 1. WHAT ARE THE MAJOR CLASSES OF CARDIAC DRUGS?...2 2. HOW DO THEY WORK?...3 3. CONSIDERATIONS FOR THE PEDIATRIC PATIENT...7 4. SUMMARY TABLE...10 REFERENCES...14
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
ANGINA PECTORIS. angina pectoris is a symptom of myocardial ischemia in the absence of infarction
 Pharmacology Ezra Levy, Pharm.D. ANGINA PECTORIS A. Definition angina pectoris is a symptom of myocardial ischemia in the absence of infarction angina usually implies severe chest pain or discomfort during
Pharmacology Ezra Levy, Pharm.D. ANGINA PECTORIS A. Definition angina pectoris is a symptom of myocardial ischemia in the absence of infarction angina usually implies severe chest pain or discomfort during
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
6 th Floor and 7 East Nurses Guide Intravenous Drip List Approved for RN Administration University of Kentucky Chandler Medical Center
 RATE Abciximab (Reopro) Alteplase (tpa, Activase) All units 6S and 6W ONLY Platelet aggregation inhibitor Thrombolytic agent Bolus: 0.25 mg/kg IV over 5 min Infusion: 0.125 0.9 mg/kg (max 90 mg); 10% of
RATE Abciximab (Reopro) Alteplase (tpa, Activase) All units 6S and 6W ONLY Platelet aggregation inhibitor Thrombolytic agent Bolus: 0.25 mg/kg IV over 5 min Infusion: 0.125 0.9 mg/kg (max 90 mg); 10% of
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
! YOU NEED TO MONITOR QT INTERVALS IN THESE PATIENTS.
 Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Antiarrhythmic Drugs Öner Süzer
 Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 09.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Antiarrhythmic Drugs Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 09.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Figure 14 1 Schematic representation
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Nitroglycerin and Heparin Drip Interfacility Protocols
 Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Nitroglycerin and Heparin Drip Interfacility Protocols EMS Protocol This protocol applies to nitroglycerin and Heparin drips that are initiated at the transferring facility prior to transport and are not
Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT
 Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT Introduction Evidence supporting the use of lidocaine and amiodarone for advanced cardiac life support was considered by international
Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT Introduction Evidence supporting the use of lidocaine and amiodarone for advanced cardiac life support was considered by international
Michigan Adult Cardiac Protocols TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Critical Care Medication Administration
 Critical Care Medication Administration 1. HEPARIN (units/hour): Given in LII, LI, HG, ER, HCHA, PACU, Cath Lab, MSONT Purpose: Anticoagulation. Used to treat Acute MI, CVA, DVT, etc. Identify concentration
Critical Care Medication Administration 1. HEPARIN (units/hour): Given in LII, LI, HG, ER, HCHA, PACU, Cath Lab, MSONT Purpose: Anticoagulation. Used to treat Acute MI, CVA, DVT, etc. Identify concentration
Pediatric Code Blue FOCUS on Medications. Objectives
 Pediatric Code Blue FOCUS on Medications Objectives The learner will be able to: 1. List commonly used pediatric code drugs based on PALS 2015 guidelines 2. Discuss mechanism of action, clinical indications,
Pediatric Code Blue FOCUS on Medications Objectives The learner will be able to: 1. List commonly used pediatric code drugs based on PALS 2015 guidelines 2. Discuss mechanism of action, clinical indications,
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
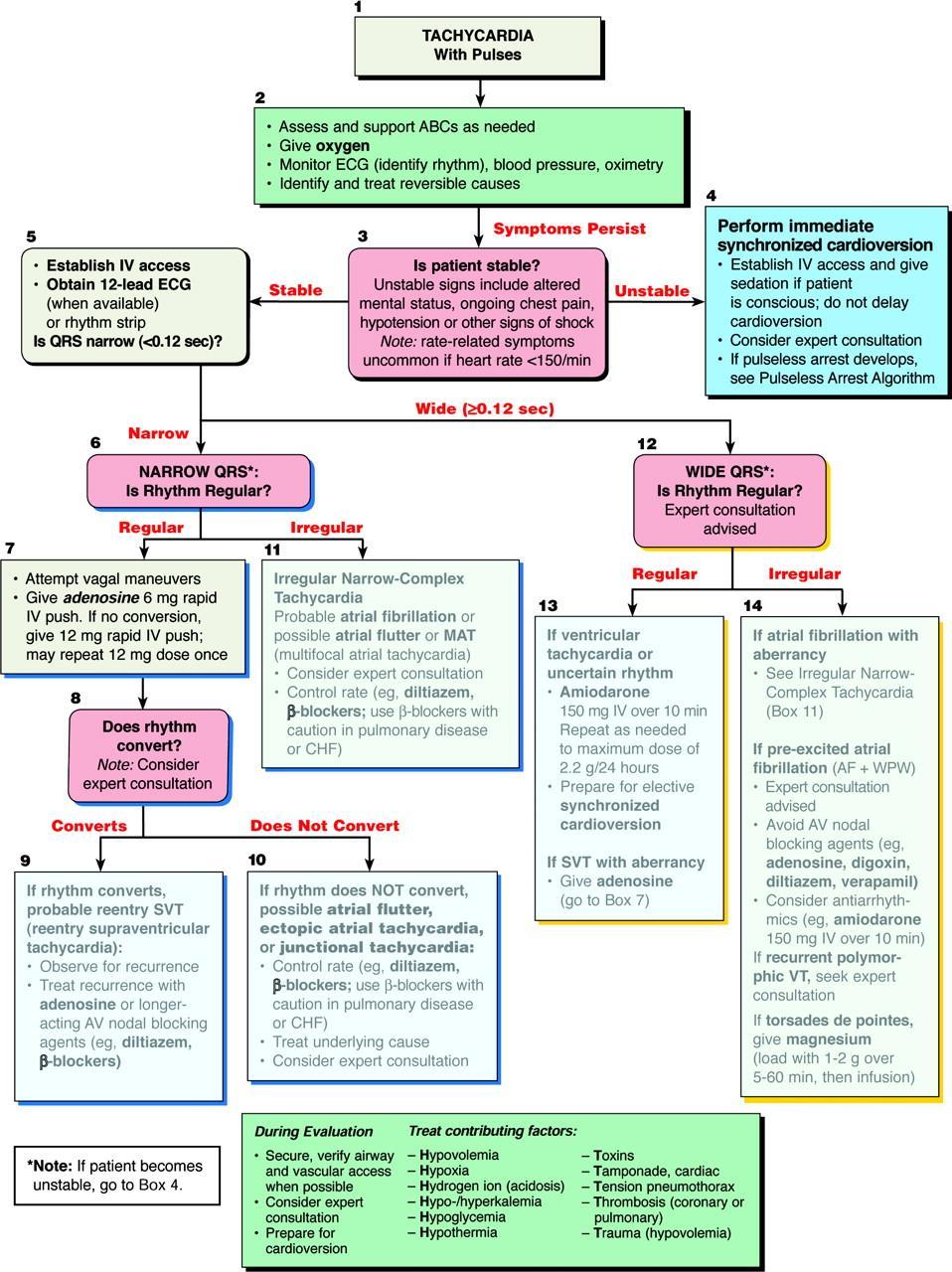
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient
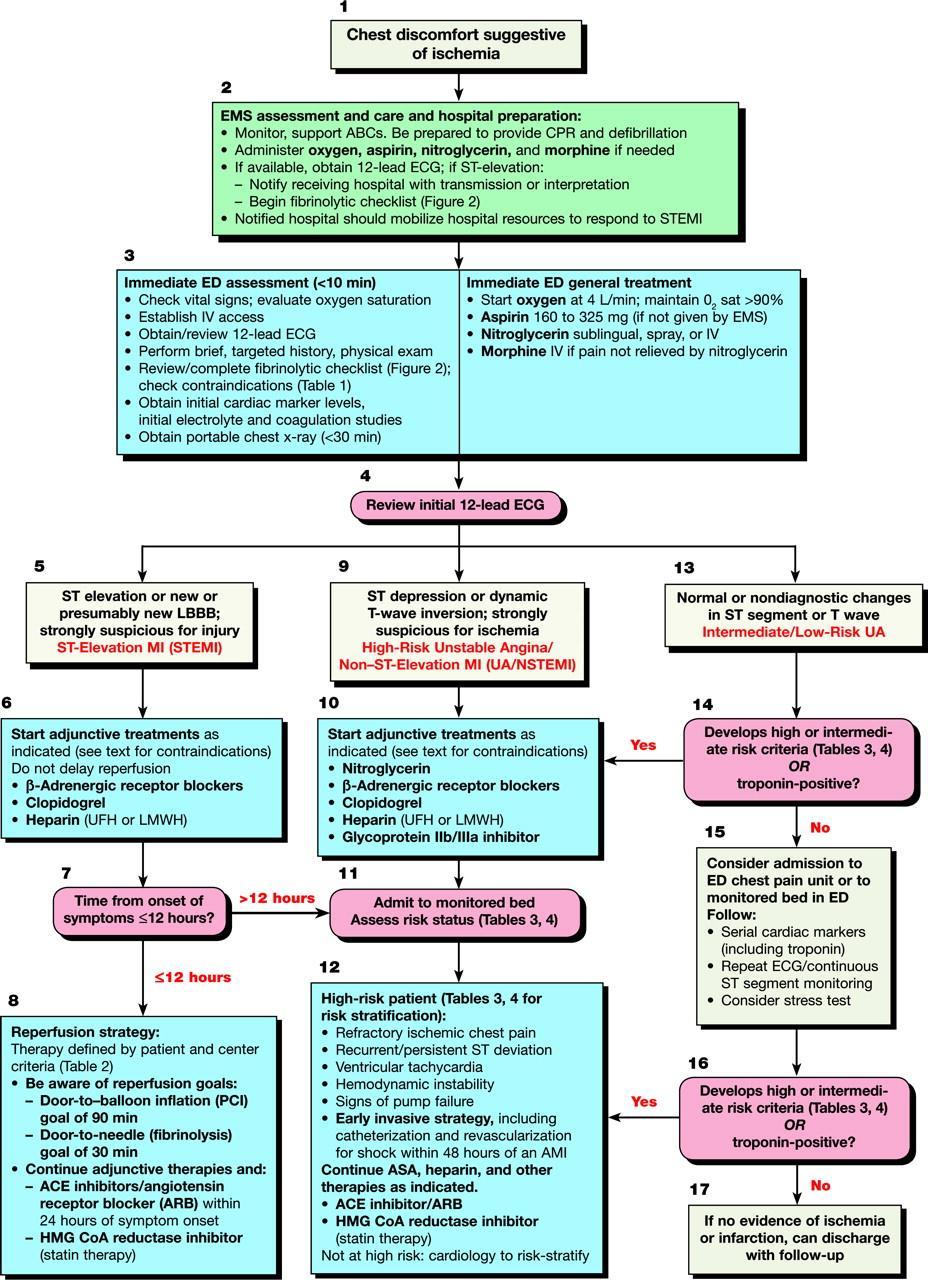
 MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
MEDICATIONS CARDIOVASCULAR URGENCIES & EMERGENCIES 12/29/14. Cardiovascular Emergency Medications. Cardiovascular Emergency Medications
 CARDIOVASCULAR URGENCIES & EMERGENCIES Steven Ganzberg, DMD, MS Director of Anesthesiology, Century City Outpatient Surgery Center Clinical Professor of Anesthesiology, UCLA School of Dentistry sganzberg@ucla.edu
CARDIOVASCULAR URGENCIES & EMERGENCIES Steven Ganzberg, DMD, MS Director of Anesthesiology, Century City Outpatient Surgery Center Clinical Professor of Anesthesiology, UCLA School of Dentistry sganzberg@ucla.edu
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
Management of acute Cardiac Arrhythmias
 Management of acute Cardiac Arrhythmias Dr. Zulkeflee Muhammad MBChB (New Zealand), MRCP (United Kingdom) Cardiologist Electrophysiology Unit Istitut Jantung Negara Objectives Review the etiology and recognition
Management of acute Cardiac Arrhythmias Dr. Zulkeflee Muhammad MBChB (New Zealand), MRCP (United Kingdom) Cardiologist Electrophysiology Unit Istitut Jantung Negara Objectives Review the etiology and recognition
Advanced Cardiac Life Support G 2010
 Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
ARRHYTHMIA SINUS RHYTHM
 ARRHYTHMIA Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU 1 SINUS RHYTHM SA node is cardiac pacemaker Normal sinus rhythm 60-100 beats/min Depolarisation
ARRHYTHMIA Dr. Ahmed A. Elberry, MBBCH, MSc, MD Assistant Professor of Clinical Pharmacy Faculty of pharmacy, KAU 1 SINUS RHYTHM SA node is cardiac pacemaker Normal sinus rhythm 60-100 beats/min Depolarisation
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets
 METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Antidysrhythmics HST-151 1
 HST-151 1 Antidysrhythmics I. Ventricular muscle cell action potential a. Phase 0: Upstroke b. Phase 1: Early-fast repolarization c. Phase 2: Plateau d. Phase 3: Repolarization e. Phase 4: Diastole HST-151
HST-151 1 Antidysrhythmics I. Ventricular muscle cell action potential a. Phase 0: Upstroke b. Phase 1: Early-fast repolarization c. Phase 2: Plateau d. Phase 3: Repolarization e. Phase 4: Diastole HST-151
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College