TRANSFUSIONS FIRST, DO NO HARM
|
|
|
- Marian Stafford
- 6 years ago
- Views:
Transcription
1 TRANSFUSIONS FIRST, DO NO HARM


2 BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women
3 BECAUSE In OB you are transfusing 2 instead of 1
4 BECAUSE BLOOD IS A LIQUID TRANSPLANT

5 RISKS versus BENEFITS versus ALTERNATIVES
6 RISKS
7 TRANSFUSION RELATED IMMUNE MODULATION (TRIM) Immune Activation TA-GVHD TRALI Alloimmunization Red cell antibodies Platelet antibodies Leukocyte antibodies Immune Suppression Nosocomial Infections Postoperative Infections Cancer Recurrence Enhanced Allograft Survival Microchimerism Lymphoma (SLL) Leukemia (CLL) Chest 2005;127:
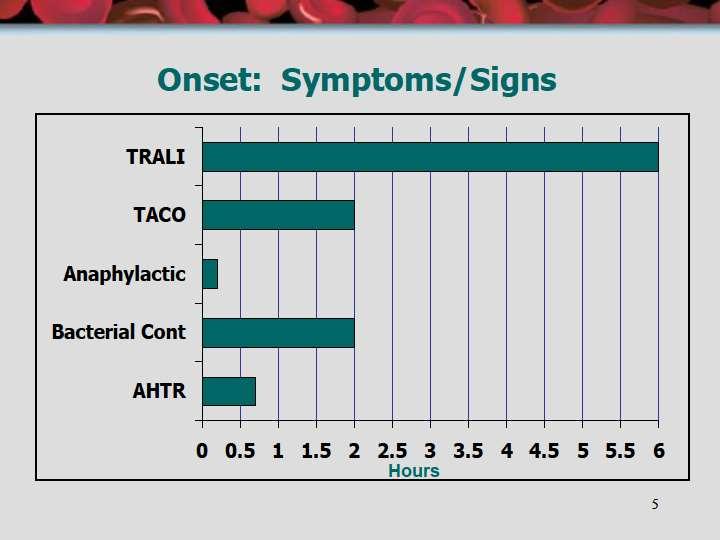
8 TRALI Any blood product can cause it Noncardiogenic pulmonary edema within 6 hours of transfusion with hypoxia Dyspnea, hypoxia, hypotension, fever, crackles Anti-neutrophil or anti-hla antibodies/ cytokines Mortality 5% to 25% Supportive care Do NOT use diuretics
9
10 TRANSFUSION INFECTIONS 68 Emerging Pathogens ZIKA VIRUS Babesiosis Malaria Lyme disease Chikungunya virus Parvoviruses vcjd Borrelia Parvoviruses Brucella Leishmania Rickettsia EBV TTV LCV Herpes viruses 6,7,8 Dengue 68 other emerging diseases from CDC

11 CLINICAL CONSEQUENCES OF RED CELL STORAGE Transfusion 2006;46:
12 RBCs ARE DAMAGED GOODS Decreased 2,3 DPG Decreased ATP Decreased nitric oxide Decreased deformability Increased adhesiveness and aggregation Increased free hemoglobin Formation of microparticles
13 BENEFITS and ALTERNATIVES
14 RBC TRANSFUSIONS Acute Hemorrhage Chronic Anemia only with significant symptoms (chest pain, CHF, marked orthostatic changes not responsive to saline) DO NOT TRANSFUSE A NUMBER!!!!
15 RBC TRANSFUSIONS HBG LESS THAN 7 Resuscitated critically ill patients Critically ill with hemodynamically stable anemia Critically ill with mechanical ventilation Critically ill with stable cardiac disease
16 RBC TRANSFUSIONS Should be given as SINGLE units NEW RULE instead of 2 REMEMBER ---- less is more
17 CHRONIC ANEMIA FIRST --- Identify cause of the anemia Transfuse only with significant symptoms (chest pain, CHF, marked orthostatic changes not responsive to saline) Do NOT transfuse a number!!!! ONLY ONE UNIT AT A TIME (NOT TWO) CONSIDER ALTERNATIVES
18 IRON THERAPY ALWAYS consider oral or IV iron therapy as an ALTERNATIVE to RBC transfusions Usually have maximal reticulocytosis in 7 to 10 days Usually see 2 gram rise in hemoglobin 1 week Usually see normal hemoglobin values in one month Order set #233 Iron Gluconate 250mg x4

19 36 year old heavy menses hemoglobin 5.6 After 4 doses IV iron her hemoglobin was 10.4 in 3 and a half weeks
20 RED BLOOD CELL NO NOs Do NOT transfuse red blood cells for Anemia that can be treated medically Volume replacement Oncotic pressure Improve wound healing (only need 4 g/dl) Sense of well being
21 PRE-OP ANEMIA Diagnose it Treat it medically Do NOT transfuse it!!!
22 CELL SAVER New and improved Better washing of red cells and use of microaggregate filter Very helpful with patient with multiple antibodies 800 procedures done safely in OB Amnionic fluid embolism risk negligible Can order as STAND-BY
23 YELLOW BLOOD PLATELETS FRESH FROZEN PLASMA (FFP) CRYOPRECIPITATE (CRYO)
24 HEMOSTATIC RANGE MUST DIFFERENTIATE HEMOSTATIC RANGE FROM REFERENCE RANGE Platelets: 50,000 (hemostatic) INR: less than 2 (hemostatic) Fibrinogen: 100 (hemostatic) 200 (pregnant) Reference platelets: 150, ,000 Reference INR: Reference fibrinogen:
25 PLATELETS Prophylaxis < 10,000 Bleeding < 50,000 Bleeding confined spaces (like brain) < 100,000 Platelet dysfunction (drugs) --- ANY count Massive blood transfusion

26 PLATELETS Therapeutic dose One plateletpheresis pack From only one donor Equivalent to 6 to 10 random platelets ABO/Rh compatibility preferred NEVER use microaggregate filter
27 PLATELETS Timing of transfusion If actively bleeding, then transfuse ASAP If pre-procedure, then give within 4 hours of procedure or surgery Should raise platelets 30 to 60K
28 PLATELET NO-NOs Do NOT transfuse platelets for Thrombotic thrombocytopenic purpura (TTP) Immune thrombocytopenia (ITP) Post-transfusion purpura (PTP) Heparin induced thrombocytopenia (HIT) Drug-induced thrombocytopenia (DIT) UNLESS life threatening bleeding
29 EPIDURAL / SPINAL 170 obstetrical patients with platelet counts between 50,000 to 100,000 No complications Recommendation of platelet count at least 75,000 for epidural anesthesia????? BEWARE of RAPIDLY FALLING platelet counts!!!!!!!!!!!
30 FRESH FROZEN PLASMA Bleeding with INR of 2 or greater Massive blood transfusion URGENT warfarin reversal (if no 4-PCC) Vitamin K (10mg IV) 4 Prothrombin Complex Concentrate (4-PCC) Factor deficiencies without concentrates Heparin resistance
31 COAGULATION FACTOR HEMOSTATIC LEVELS Fibrinogen Prothrombin Factor V Factor VII Factor VIII Factor X Factor XIII 50mg/dl 20-30% 15-20% 15-20% 15-20% 15-20% 2-5% Mannuci, Blood, 2004;104:1243
32 FFP MUST BE GIVEN AT RIGHT TIME Only give within 4 hours of a procedure or when actually bleeding Coagulation effect only lasts about 6 hours NEVER give the night before a procedure NEVER give to normalize INR

33 FFP MUST BE ADEQUATE DOSE USUAL DOSE to 20 ml/kg Average volume of one FFP is 300 ml So minimum dose is usually at least 3 FFP in 70 kg patient (up to 5 FFP)
34 FFP NO NOs Do NOT transfuse FFP to Normalize abnormal INR results Patients on heparin (unless heparin resistant) Increase blood volume Increase albumin level Elevated INR that can be corrected with Vitamin K or PCC
35 CRYOPRECIPITATE Bleeding with fibrinogen less than 100 UNLESS pregnant than less than 200 Massive blood transfusion Congenital fibrinogen deficiencies Factor XIII deficiency
36 Fibrinogen Levels and PPH Hypofibrinogenemia in the setting of PPH has emerged in the literature as a predictor for progression to severe PPH Several studies have associated low fibrinogen levels with the severity of PPH: Low fibrinogen levels early in the bleeding were a predictor for severe PPH Fibrinogen levels < 2 g/l were independently associated with an increased risk of severe PPH Hematology. 2015: International Journal of Obstetric Anesthesia. 2013;22:
37 Fibrinogen Levels and PPH (cont.) Fibrinogen levels are predictive for severe PPH only after the onset of hemorrhage A recent study has found no correlation between prelabor fibrinogen levels and PPH Hematology. 2015: International Journal of Obstetric Anesthesia. 2013;22:
38 PPH Etiology Etiologies for PPH include medical, obstetric, and surgical The Four Ts of PPH Tone (uterine atony) Tissue (retained placenta or placental abnormalities) Trauma (injury to the uterus, birth canal, and supporting structures) Thrombin (coagulopathies)
39 Coagulation in Pregnancy Pregnancy normally results in a hypercoagulable state Progressive elevations in procoagulant factors occurs (vwf, FVII, FVIII, FIX), and peaks 2-3 hours post-partum
40 Coagulation in Pregnancy (cont.) Anticoagulant factor (e.g. Protein S) and fibrinolytic activity also decrease Fibrinogen levels at term pregnancy are nearly double normal levels of nonpregnant female ( mg/dl vs mg/dl) These physiological changes help reduce blood loss at the time of delivery
41 Mechanisms of PPH Recent data suggests that PPH may share some of the same mechanisms seen in traumatic bleeding Early tissue hypoperfusion caused by obstetrical hemorrhage results in activation of Protein C which leads to decreased fibrin formation and increased fibrinolysis American Journal of Perinatology.2013;30:1-4
42 Hyperfibrinolysis in PPH Up-regulation of thrombomodulin occurs on the endothelial cells in response to tissue hypoperfusion Increased binding of thrombin to thrombomodulin occurs, which in turn, activates Protein C Protein C inactivates factors Va & VIIIa which prevents conversion of prothrombin to thrombin and subsequent fibrin formation Protein C also inhibits plasminogen activator 1 (PAI-1), which leaves tpa activity unchecked to cause increased fibrinolysis
43 TXA AT WESLEY Since 2013, 128 women given TXA prophylactically and only 1 (0.8%) was transfused (but was three days later)! Since 2013, 78 women given TXA for bleeding and only 26 (33%) were transfused and 52 (65%) were not transfused
44 When to call MBT in PPH The precise threshold to activate the protocol in obstetric patients is difficult to establish Decision usually subjective & may include: Amount of blood already lost Rate and magnitude of ongoing blood loss Likelihood that medical and surgical intervention will control the bleeding any time soon 44
45 Massive Hemorrhage NOTIFY BLOOD BANK x22850 Order Set Massive Blood Trans Adult gets the Blood Transfusion Protocol (MBT)
46 Massive Blood Transfusion Protocol (MBT) Must have baseline labs (Hbg,INR,Plt,Fib) which is the acute bleed profile === === ===repeat 5 RBCs 4 FFP 1 Plateletpheresis 5 Cryo TUBE STATION #36 stat lab/blood bank
47 POSSIBLE CHANGES TO MBT FIBRINOGEN CONCENTRATE INSTEAD OF CRYOPRECIPITATE THAWED OR LIQUID PLASMA READY TO GO ---- MIGHT BE Group AB or Group A 5 RBC 4FFP 1 Plateletpheresis
48 ALTERNATIVES Pharmacy is the NEW blood bank!!! IV Iron (iron gluconate, order #233) IV Vitamin K Antifibrinolytics (TXA, order set #193) Coagulation Factor Concentrates Kcentra (4 factor PCC) Humate P (for VWD) Fibrinogen concentrate new, not yet at WMC
TRANSFUSIONS WHY DO WE EVEN CARE?????
 TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
TRANSFUSIONS WHY DO WE EVEN CARE????? BECAUSE BLOOD CAN KILL 7 TRALI DEATHS SINCE 2002 WMC 5 women Because in OB you are transfusing 2 instead of 1 BECAUSE BLOOD IS A LIQUID TRANSPLANT JOINT COMMISSION
Massive Transfusion. MPQC Spring Summit April 29, Roger Belizaire MD PhD
 Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
Massive Transfusion MPQC Spring Summit April 29, 2015 Roger Belizaire MD PhD Take home points 1. Blood is always available. Requests for massive transfusion or emergency release typically only require
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Blood Transfusion Guidelines in Clinical Practice
 Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Transfusion Guidelines in Clinical Practice Salwa Hindawi Director of Blood Transfusion Services Associate Professor in Haematology and Transfusion Medicine King Abdalaziz University, Jeddah Saudi
Blood Components & Indications for Transfusion. Neda Kalhor
 Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
Blood Components & Indications for Transfusion Neda Kalhor Blood products Cellular Components: Red blood cells - Leukocyte-reduced RBCs - Washed RBCs - Irradiated RBCs Platelets - Random-donor platelets
CrackCast Episode 7 Blood and Blood Components
 CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
CrackCast Episode 7 Blood and Blood Components Episode Overview: 1) Describe the 3 categories of blood antigens 2) Who is the universal donor and why? 3) Define massive transfusion 4) List 5 physiologic
Blood Component Therapy
 Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Component Therapy Dr Anupam Chhabra Incharge-Transfusion Medicine Pushpanjali Crosslay Hopital NCR-Delhi Introduction Blood a blood components are considered drugs because of their use in treating
Blood Components Transfusion Criteria
 Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Adults 1. Packed Cells: Dosage one unit of red blood cells will raise the Hbg by 1 gram; Hct by 3% in a 70Kg adult. Red Blood Cells should be transfused based on clinical need. In the absence of acute
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient
 Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Bleeding, Coagulopathy, and Thrombosis in the Injured Patient June 7, 2008 Kristan Staudenmayer, MD Trauma Fellow UCSF/SFGH Trauma deaths Sauaia A, et al. J Trauma. Feb 1995;38(2):185 Coagulopathy is Multi-factorial
Approach to bleeding disorders &treatment. by RAJESH.N General medicine post graduate
 Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
Approach to bleeding disorders &treatment by RAJESH.N General medicine post graduate 2 Approach to a patient of bleeding diathesis 1. Clinical evaluation: History, Clinical features 2. Laboratory approach:
New Advances in Transfusion EM I LY CO BERLY, M D
 New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
New Advances in Transfusion EM I LY CO BERLY, M D TRANSFUSI ON M EDI CI NE FELLO W VANDERBI LT UNI VERSITY Objectives To discuss the terminology, components, transfusion risks, and dosing guidelines for
GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS
 CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
CHILDREN S HOSPITALS AND CLINICS OF MINNESOTA Introduction: GUIDELINES FOR THE TRANSFUSION OF BLOOD COMPONENTS These guidelines have been developed in conjunction with the hospital Transfusion Committee.
Transfusion 2004: Current Practice Standards. Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service
 SBB SWMC Transfusion Service") Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Transfusion 2004: Current Practice Standards Kay Elliott, MT (ASCP) SBB SWMC Transfusion Service Massive Transfusion Protocol (MTP) When should it be activated? Massive bleeding i.e. loss of one blood
Massive transfusion: Recent advances, guidelines & strategies. Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad
 Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
Massive transfusion: Recent advances, guidelines & strategies Dr.A.Surekha Devi Head, Dept. of Transfusion Medicine Global Hospital Hyderabad Massive Hemorrhage Introduction Hemorrhage is a major cause
My Bloody Talk. Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne
 My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
My Bloody Talk Dr Ben Turner MBBS, FANZCA, FCICM The Royal Children s Hospital, Melbourne Disclosures No conflicts of interest Interest in conflict Blood transfusion Massive transfusion definitions Transfusion
Transfusion Medicine Best Practices: Indications for Blood Components
 Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
Transfusion Medicine Best Practices: 1.0 Policy Statements 1.1 Regional Health Authorities (RHAs) shall develop policies, processes and procedures for ordering, distribution, storage, transfusion and administration
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA Transfusion Criteria Version#2 POLICY NO.
 LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
LifeBridge Health Transfusion Service Sinai Hospital of Baltimore Northwest Hospital Center BQA 1011.02 Transfusion Criteria Version#2 Department POLICY NO. PAGE NO. Blood Bank Quality Assurance Manual
Effective Date: Approved by: Laboratory Director, Jerry Barker (electronic signature)
") 1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
1 of 5 Policy #: 702 (PHL-702-05) Effective Date: 9/30/2004 Reviewed Date: 8/1/2016 Subject: TRANSFUSION GUIDELINES Approved by: Laboratory Director, Jerry Barker (electronic signature) Approved by: Laboratory
ADULT TRANSFUSION GUIDELINES ORDERED COMPONENT
 ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
ADULT TRANSFUSIN GUIDELINES RDERED Packed red cells (RBCs) RBCs, WBCs, platelets & plasma (minimal) Increase red cell mass and oxygen carrying capacity; generally indicated when Hgb is 7 gm or Hct 21 unless
Transfusion Medicine III
 Transfusion Medicine III Blood Products from Collection to Use D. Joe Chaffin, MD Loma Linda University 3/5/2019 FFP WB RBC Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep
Transfusion Medicine III Blood Products from Collection to Use D. Joe Chaffin, MD Loma Linda University 3/5/2019 FFP WB RBC Anticoagulant/Preservatives Why we need 21 Day Shelf Life Prevent clotting Keep
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference
 Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Use of Prothrombin Complex Concentrate to Reverse Coagulopathy Rio Grande Trauma Conference John A. Aucar, MD, MSHI, FACS, CPE EmCare Acute Care Surgery Del Sol Medical Center Associate Professor, University
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created
 Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
Bassett Medical Center The Mary Imogene Bassett Hospital Clinical Laboratory Blood Bank Title: Blood Transfusion Guidelines 2016 Revision: 1 Created By: Bray, Karen Last Approved Time: 7/22/2016 12:41:34
Blood transfusion. Dr. J. Potgieter Dept. of Haematology NHLS - TAD
 Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Blood transfusion Dr. J. Potgieter Dept. of Haematology NHLS - TAD General Blood is collected from volunteer donors >90% is separated into individual components and plasma Donors should be: healthy, have
Risk of ID transmission. Patient Blood Management - Blood Safety and Component Utilization. Transfusion and Cancer 4/9/2014
 Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Patient Blood Management - Blood Safety and Component Utilization Lowell Tilzer M.D. Pathology and Lab Medicine Kansas University Med Center Risk of ID transmission Pre NAT Post NAT HIV 1:607,000 ~1:2.5
Disseminated Intravascular Coagulation. M.Bahmanpour MD Assistant professor IUMS
 به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
به نام خدا Disseminated Intravascular Coagulation M.Bahmanpour MD Assistant professor IUMS Algorithm for Diagnosis of DIC DIC Score factor score Presence of known underlying disorder No= 0 yes=2 Coagolation
Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes ~ 100 units Heparin neutralization in ~ 5 min
 Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
Nanik (Nayri) Hatsakorzian Pharm.D/MPH candidate 2014 Touro University College of Pharmacy CA Bleeding Reversal Agents Agent Dose MoA/PK/Admin Adverse events Disadvantages Protamine Heparin: 1mg neutralizes
The ABC s of Blood Components. Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service
SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service") The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
The ABC s of Blood Components Terry Downs, MT(ASCP)SBB Administrative Manager University of Michigan Hospitals Blood Bank and Transfusion Service Objectives Describe three additives used in blood components.
Hemostasis and thrombosis in patients with liver disease. Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands
 Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
Hemostasis and thrombosis in patients with liver disease Ton Lisman, Dept Surgery, UMC Groningen, The Netherlands Importance of the liver in hemostasis Synthesis of Coagulation factors Fibrinolytic proteins
2/2/2011. Blood Components and Transfusions. Why Blood Transfusion?
 Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
Blood Components and Transfusions Describe blood components Identify nursing responsibilities r/t blood transfusion Discuss factors r/t blood transfusion including blood typing, Rh factor, and cross matching
UKGS TRANSFUSION SERVICE PRODUCTS AND AVAILABILITY
 Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Lexington, KY Page 1 of 13 Affected Sites: Enterprise Chandler X Good Samaritan I. PRINCIPLE: The UK Good Samaritan Hospital is dedicated to serve the patients with safe, high quality blood products and
Coagulation, Haemostasis and interpretation of Coagulation tests
 Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
Coagulation, Haemostasis and interpretation of Coagulation tests Learning Outcomes Indicate the normal ranges for routine clotting screen and explain what each measurement means Recognise how to detect
BLOOD TRANSFUSION. Dr Lumka Ntabeni
 BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
BLOOD TRANSFUSION Dr Lumka Ntabeni Blood transfusion definition SAFE transfer of BLOOD COMPONENTS from a DONOR to a RECEPIENT CONTENT Brief history of blood transfusion How is safety guaranteed? How do
Crossmatching and Issuing Blood Components; Indications and Effects.
 Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Crossmatching and Issuing Blood Components; Indications and Effects. Alison Muir Blood Transfusion, Blood Sciences, Newcastle Trust Topics Covered Taking the blood sample ABO Group Antibody Screening Compatibility
Chest diseases Hospital Laboratory Hematology Practice guidelines
 Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Chest diseases Hospital Laboratory Hematology Practice guidelines Title RBCs transfusion in Adults SOP Code Policy Owner Hematology Unit Section Hematology Prepared By Dr. Taher Ahmed Abdelhameed Issuing
Prothrombin Complex Concentrate- Octaplex. Octaplex
 Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Prothrombin Complex Concentrate- Concentrated Factors Prothrombin Complex Concentrate (PCC) 3- factor (factor II, IX, X) 4-factor (factors II, VII, IX, X) Activated 4-factor (factors II, VIIa, IX, X) Coagulation
Consent Laboratory Transfuse RBC
 Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Peds Blood Product Infusion Order Set (386) [386] Blood product review will be performed unless exclusion criteria met. MD: Please note if transfusion giv en outside of parameter, please justify use in
Hematology Review. CCRN exam. The Coagulation Cascade. The Coagulation Cascade. Components include: Intrinsic pathway Extrinsic pathway Common pathway
 CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
CCRN exam Hematology Review CCRN Review October 2013 Department of Critical Care Nursing Hematology is 2% of the exam Focus on coagulation cascade, DIC, and HIT Anatomy of the hematologic system Bone marrow
Intraoperative haemorrhage and haemostasis. Dr. med. Christian Quadri Capoclinica Anestesia, ORL
 Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
Intraoperative haemorrhage and haemostasis Dr. med. Christian Quadri Capoclinica Anestesia, ORL Haemostasis is like love. Everybody talks about it, nobody understands it. JH Levy 2000 Intraoperative Haemorrhage
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
Managing Coagulopathy in Intensive Care Setting
 Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
Managing Coagulopathy in Intensive Care Setting Dr Rock LEUNG Associate Consultant Division of Haematology, Department of Pathology & Clinical Biochemistry Queen Mary Hospital Normal Haemostasis Primary
23/10/2011. Case One: Mrs. B. Mrs. B., 36 year old, 30 weeks pregnant, 2 nd baby Blood type A negative Belted driver of minivan, struck a parked car
 GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
GETTING IT BLOODY RIGHT: CHOOSING THE BEST PRODUCT Kathleen Eckert, ART, Transfusion Safety Officer, LHSC Brenda Morgan, RN BScN MSc, CNS, Critical Care, Victoria Hospital, LHSC http://www.transfusionontario.org/public-en/public.php
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Heme (Bleeding and Coagulopathies) in the ICU
 in the ICU") Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Heme (Bleeding and Coagulopathies) in the ICU General Topics To Discuss Transfusions DIC Thrombocytopenia Liver and renal disease related bleeding Lack of evidence in managing critical illness related
Blood Product Utilization A Mythbusters! Style Review. Amanda Haynes, DO 4/28/18
 Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Blood Product Utilization A Mythbusters! Style Review Amanda Haynes, DO 4/28/18 Objectives Describe concepts in Patient Blood Management Review common misconceptions surrounding blood transfusion Summarize
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Blood Products & Transfusion. Karim Rafaat, M.D.
 Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
Blood Products & Transfusion Karim Rafaat, M.D. Compatibility Testing Compatibility testing involves three separate procedures involving both donor and recipient blood. 1. ABO & Rh blood type identification
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hematologic Emergency. Le Wang, MD, PhD Hematology & Oncology
 Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
Hematologic Emergency Le Wang, MD, PhD Hematology & Oncology Severe Thrombocytopenia (ITP) Clinical: bleeding risk 0 no bleeding; 1 minimal bleeding after trauma; 2 spontaneous but selflimited bleeding;
MASSIVE TRANSFUSION PROTOCOL
 MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
MASSIVE TRANSFUSION PROTOCOL IF YOU ANTICIPATE EMERGENT NEED FOR LARGE AMOUNTS OF BLOOD IN A SHORT PERIOD OF TIME Call Blood Bank: 6622121 Tell them you have a patient who needs a Massive Transfusion and
EMSS17: Bleeding patients course material
 EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
EMSS17: Bleeding patients course material Introduction During the bleeding patients workshop at the Emergency Medicine Summer School 2017 (EMSS17) you will learn how to assess and treat bleeding patients
POLICY NO. Printed copies are for reference only. Please refer to the electronic copy for the latest version.
 Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
Department Blood Bank POLICY NO. 4633 Department Of Pathology LBH Transfusion Criteria Version# 2 PAGE NO. 1 OF 9 Printed copies are for reference only. Please refer to the electronic copy for the latest
What s in the Massive Transfusion Protocol (MTP) Package?
 Package?") What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
What s in the Massive Transfusion Protocol (MTP) Package? The Massive Transfusion Protocol Package is a set of documents intended to improve the coordination of a Massive Transfusion Protocol. The kit
Pediatric massive transfusion protocols
 University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
University of New Mexico UNM Digital Repository Emergency Medicine Research and Scholarship Emergency Medicine 2014 Pediatric massive transfusion protocols Ramsey Tate Follow this and additional works
2012, Görlinger Klaus
 Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Gerinnungsmanagement der Gegenwart - wie gehen wir heute vor? 25. Allander Gerinnungsrunde am 15. März 2012 Klaus Görlinger Universitätsklinikum Essen klaus@goerlinger.net CSL Behring GmbH Octapharma AG
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol
 Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
Adult Reversal of Anticoagulation and Anti-platelet Agents for Life- Threatening Bleeding or Emergency Surgery Protocol Page Platelet Inhibitors 2 Aspirin, Clopidogrel (Plavix), Prasugrel (Effient) & Ticagrelor
WELCOME. Evaluation Summary
 WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
WELCOME Evaluation Summary 489 delegates from 40 countries Delegate s specialty 239 respondents Delegate s professional activity 208 respondents Overall Evaluation This symposium was helpful for your clinical
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hematologic Disorders. Assistant professor of anesthesia
 Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
Preoperative Evaluation Hematologic Disorders Dr M.Razavi Assistant professor of anesthesia Anemia Evaluation needs to consider the extent and type of surgery, the anticipated blood loss, and the patient's
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY
 MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
MANAGEMENT OF COAGULOPATHY AFTER TRAUMA OR MAJOR SURGERY 19th ANNUAL CONTROVERSIES AND PROBLEMS IN SURGERY Thabo Mothabeng General Surgery: 1 Military Hospital HH Stone et al. Ann Surg. May 1983; 197(5):
Guideline for Treatment of Head Injury in the Anticoagulated Patient
 Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
Guideline for Treatment of Head Injury in the Anticoagulated Patient GUIDELINE: GUIDELINE FOR TREATMENT OF HEAD INJURY IN THE ANTICOAGULATED PATIENT BACKGROUND: Chronic anticoagulation therapy is used
Use of Prothrombin Complex Concentrates (PCC) CONTENTS
 CONTENTS") CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
CONTENTS Page 1: Exclusion Criteria and Approved Indications for Use Page 2: Dosing / Administration / Storage Page 4: Prescribing / Monitoring / Dispensing Page 5: Cautions / Warnings / Cost Analysis
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
Note: Page numbers of article titles are in boldface type. A Abdominal tumors, in children, 530 531 Alkalinization, in tumor lysis syndrome, 516 Allopurinol, in tumor lysis syndrome, 515 Anaphylaxis, drug
1 Transfusion Medicine and Blood Bank Department, H. São João, Centro
 Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Original Article Interventional Algorithms for the Control of Coagulopathic Bleeding in Surgical, Trauma, and Postpartum Settings: Recommendations From the Share Network Group Clinical and Applied Thrombosis/Hemostasis
Bleeding and Thrombotic Disorders. Kristine Krafts, M.D.
 Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Bleeding and Thrombotic Disorders Kristine Krafts, M.D. Bleeding and Thrombotic Disorders Bleeding disorders von Willebrand disease Hemophilia A and B DIC TTP/HUS ITP Thrombotic disorders Factor V Leiden
Transfusion in major bleeding: new insights. Gert Poortmans
 Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
Transfusion in major bleeding: new insights Gert Poortmans Trauma Cardiac Surgery Major Surgery with ongoing blood loss Burn Surgery Lethal Triad Polytransfusion: definitions Coagulation Coagulopathy of
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
Groupe d Intérêt en Hémostase Périopératoire
 How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
How do I treat massive bleeding? Red blood cell / plasma / platelet ratio and massive transfusion protocols Anne GODIER Service d Anesthésie-Réanimation Hopital Cochin Paris Groupe d Intérêt en Hémostase
Haematology and Transfusion
 Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
Haematology and Transfusion dr.w.engelhardt@gmail.com Wolfram Engelhardt Offenburg, Germany James Blundell 1828 Diameter 6-8 µm Erythrocytes Women: Men: 4-5 x 10 6 /µl 5-6 x 10 6 /µl live 100-120 days
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal
 PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
PREDLOG SMERNIC ZA KLINIČNO UPORABE SVEŽE ZMRZNJENE PLAZME Guidelines for clinical use of FFP proposal Dragoslav Domanovič, MD. PhD. Blood transfusion centre of Slovenia, Ljubljana FFP - definition Fresh
Chapter 1 The Reversing Agents
 Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
Available Strategies to Reverse Anticoagulant Medications Michael L. Smith, Pharm. D., BCPS, CACP East Region Pharmacy Clinical Manager Hartford HealthCare Objectives: Describe the pharmacological agents
Coagulopathy: Measuring and Management. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
Coagulopathy: Measuring and Management Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine No Financial Disclosures Objectives Define coagulopathy of trauma Define
MANAGEMENT OF COMMON BLEEDING DISORDERS. Auro Viswabandya Department of Haematology, CMC, Vellore
 MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
MANAGEMENT OF COMMON BLEEDING DISORDERS Auro Viswabandya Department of Haematology, CMC, Vellore BLOOD CLOT : PRIMARY HAEMOSTASIS (Platelets) + SECONDARY HAEMOSTASIS (Coagulation Factors) HAEMOSTATIC DISORDERS
Components of Blood. N26 Blood Administration 4/24/2012. Cabrillo College ADN/C. Madsen RN, MSN 1. Formed elements Cells. Plasma. What can we give?
 Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Components of Blood Formed elements Cells Erythrocytes (RBCs) Leukocytes (WBCs) Thrombocytes (platelets) Plasma 90% water 10% solutes Proteins, clotting factors 1 What can we give? Whole blood Packed RBC
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital
 Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Transfusion Reactions/Complications Mary Berg, M.D. Medical Director, Transfusion Services Associate Professor of Pathology University of Colorado Hospital Acute Transfusion Reactions Can be seen with
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89
 Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
Chapter 3 Diseases of the Blood and Bloodforming Organs and Certain Disorders Involving the Immune Mechanism D50-D89 Presented by Jennifer Kurkulonis 1 FOUR MAJOR TYPES OF BLOOD CELLS White blood cells
HEME 10 Bleeding Disorders
 HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
HEME 10 Bleeding Disorders When injury occurs, three mechanisms occur Blood vessels Primary hemostasis Secondary hemostasis Diseases of the blood vessels Platelet disorders Thrombocytopenia Functional
ADMINISTRATIVE CLINICAL Page 1 of 6
 ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
ADMINISTRATIVE CLINICAL Page 1 of 6 Anticoagulant Guidelines #2: REVERSAL OF OR MANAGEMENT OF BLEEDING WITH ANTICOAGULANTS Origination Date: Revision Date: Reviewed Date: 09/12 09/12, 01/13, 11/13, 11/15
Review. Blood Components for Hemostasis. RBC Transfusion. Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT
 Blood Components for Hemostasis Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT We present an overview of revised indications and doses for routinely transfused blood components. Targeted blood
Blood Components for Hemostasis Karen W. Eldin, MD 1, and Jun Teruya, MD, DSc 1,2 ABSTRACT We present an overview of revised indications and doses for routinely transfused blood components. Targeted blood
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES
 TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
TRANSFUSION SUPPORT IN HEPATOBILIARY AND PANCREATIC SURGERIES Dr.K.C.Usha Professor & Head Dept: Of Transfusion Medicine & Director, Model Blood Bank Government Medical College Trivandrum,Kerala INTRODUCTION
Treatment of the Medically Compromised Patient
 Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Treatment of the Medically Compromised Patient Nashville Area Continuing Dental Education Series November 3, 2010 Harry J. Brown, MD Chief Medical Officer, Nashville Area Outline General Principles Specific
Thursday, February 26, :00 am. Regulation of Coagulation/Disseminated Intravascular Coagulation HEMOSTASIS/THROMBOSIS III
 REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
REGULATION OF COAGULATION Introduction HEMOSTASIS/THROMBOSIS III Regulation of Coagulation/Disseminated Coagulation necessary for maintenance of vascular integrity Enough fibrinogen to clot all vessels
Bleeding Disorders. Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph
 Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
Bleeding Disorders Dr. Mazen Fawzi Done by Saja M. Al-Neaumy Noor A Mohammad Noor A Joseph Joseph Normal hemostasis The normal hemostatic response involves interactions among: The blood vessel wall (endothelium)
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
Coagulation Disorders. Dr. Muhammad Shamim Assistant Professor, BMU
 Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Coagulation Disorders Dr. Muhammad Shamim Assistant Professor, BMU 1 Introduction Local Vs. General Hematoma & Joint bleed Coagulation Skin/Mucosal Petechiae & Purpura PLT wound / surgical bleeding Immediate
Transfusion Medicine Kris0ne Kra1s, M.D.
 Transfusion Medicine Kris0ne Kra1s, M.D. Transfusion Medicine Outline Blood groups Introduc0on ABO system Rh system Other systems Blood transfusion Blood products Indica0ons Tes0ng Dangers Transfusion
Transfusion Medicine Kris0ne Kra1s, M.D. Transfusion Medicine Outline Blood groups Introduc0on ABO system Rh system Other systems Blood transfusion Blood products Indica0ons Tes0ng Dangers Transfusion
Guidelines for Use of Canine Blood Components
 Guidelines for Use of Canine Blood Components Cryoprecipitate This product is prepared by a controlled thaw of fresh frozen plasma, resulting in a concentration of Factor VIII, Factor XIII, vwf and some
Guidelines for Use of Canine Blood Components Cryoprecipitate This product is prepared by a controlled thaw of fresh frozen plasma, resulting in a concentration of Factor VIII, Factor XIII, vwf and some
Transfusion: indications (RBC, platelets, granulocytes, plasma)
") Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Transfusion: indications (RBC, platelets, granulocytes, plasma) BHS Educational Course: course n 5 22/3/2014 Timothy Devos (KU Leuven) Indications for the transfusion of erythrocytes General rules only
Transfusion Medicine Potpourri. BUMC - Phoenix Internal Medicine Residents September 29, 2015
 Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
Transfusion Medicine Potpourri BUMC - Phoenix Internal Medicine Residents September 29, 2015 Clinical case A 24 year old female with sickle cell anemia has just moved to the area and presents as a new
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche
 L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
L iter diagnostico di laboratorio nelle coagulopatie congenite emorragiche Armando Tripodi Angelo Bianchi Bonomi Hemophilia and Thrombosis Center Dept. of Clinical Sciences and Community Health University
Red cell antigens and blood group antibodies
 Hematology Blood transfusion د.ميسم مؤيد علوش Objectives: O Identify the most important blood group systems? O List types of antibodies and the main features of each type? O Define the ABO system and its
Hematology Blood transfusion د.ميسم مؤيد علوش Objectives: O Identify the most important blood group systems? O List types of antibodies and the main features of each type? O Define the ABO system and its
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital
 Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital") DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) Pichika Chantrathammachart MD Division of Hematology, Department of Medicine Ramathibodi Hospital Disseminated intravascular coagulation (DIC) Disseminated
Learning Objectives: At the end of this exercise, the student will be able to:
 Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Applications in Transfusion Medicine- A CBL Exercise- Student Guide 1 Title: Applications in Transfusion Medicine A CBL Exercise Purpose: At the conclusion of this exercise, students will be able to apply
Blood/Blood Component Utilization and Administration Annual Compliance Education
 Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
Blood/Blood Component Utilization and Administration Annual Compliance Education This course contains annual compliance education necessary to meet compliance and regulatory requirements. Instructions:
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR
 MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
MANAGEMENT OF OVERANTICOAGULATION AND PREOPERATIVE MANAGEMENT OF WARFARIN DOSE 1. GUIDELINES FOR THE MANAGEMENT OF AN ELEVATED INR 1.1 Time to lower INR Prothrombinex-VF - 15 minutes Fresh Frozen Plasma
Effect of under filling tube
 Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
Effect of under filling tube 2 What constitutes underfilling? A 4.5ml vacutainer collection tube should contain at least 4ml of blood Less than that could give falsely prolonged clotting times ALSO be
2.5 Other Hematology Consult:
 The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
The Warfarin Order Sheet has been approved by the P & T committee to be implemented by pharmacists. These orders are not used to treat patients with serious hemorrhagic complications. WARFARIN TARGET INR
How can ROTEM testing help you in trauma?
 How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
How can ROTEM testing help you in trauma? Complicated bleeding situations can appear intra and post operatively. They can be life-threatening and always require immediate action. A fast differential diagnosis
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE
 TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two
TREATMENT & MANAGEMENT OF VON WILLEBRAND DISEASE Dr Susan Russell Director HTC Sydney Children s Hospital, Randwick HFA Meeting 2015 What is von Willebrand Factor? VWF is a large multimeric protein Two