Shock. Zeng xuan Hu OCT17
|
|
|
- Reynold Harrison
- 6 years ago
- Views:
Transcription
1 Shock Zeng xuan Hu OCT17 1
2 Objective Concept Categories Principles of management 2
3 Definition Inadequate tissue perfusion to maintain normal cellular function Not all hypotensive patients are in shock Not all patients in shock are hypotensive young patient, compensated 3
4 Definition Inadequate delivery of O2 (DO2) Inability to utilize deliered O2 4

5 Definition 5
6 Inadequate tissue perfusion-assessment Mental status change Vital sign changes(hypotensive) Oliguria Lactate Base deficit Cr transaminase abnormaity Underlying disease-nf Compensatory machenism -Vasoconstriction, tachy 6

7 Lactate Insufficient O 2 pyruvate lactate dehydrogenase lactate dehydrogenase lactate liver(50%), kidney(30%) The admission level, highest level, time interval to normalize lactate are important prognostic indicators for survival. 7
8 Base deficit The amount of base in mmoles needed to titrate 1 L of whole blood to a ph of 7.40 Mild (3 to 5 mmol/l), moderate (6 to 14 mmol/l), severe (15 mmol/l) Worsen base deficit associated higher mortality Caveat: administration of bicarbonate, hypothermia, hypocapnia

9 Hypovolemic Shock

10 Distributive Shock Anaphylactic Septic Neurogenic Adrenal Insufficiency

11 Cardiogenic Shock Myopathic,arrhyth mic,mechanical
12 Obstructive Shock Cardiac Tamponade Tension Pneumothorax Massive PE
13 Classification of shock Hypovolemic Distributive Obstructive Cardiogenic 13
14 Principle of management ABC Restore tissue perfusion Underlying disease Monitor Supportive care 14

15 Management
16 Vasopressor/inotrop 16
17 Case Study Mr. MS 70 male with PHx of CAD 12 hour post MIS splenectomy in PAR Called for low BP What s your approach?
18 Mr. MS A intubated SaO2 97% on Fi02 of 50% B C BP 80/60, HR 110, Temp 37.2, JVP flat Right IJ in place Combative and confused Cool, mottled extremities Distended abdomen U/O borderline received 3 L NS bolus
19 Mr. MS Findings suggest inadequate tissue perfusion? What type of shock do this pt likely have? differentials? -hypovolemic,obstructive, cardiogenic, distributive Next? 19

20 Mr. MS Resucitation WBC 24, Hb 65 Pl 243 coag N trop 0.5 Lactate 4.2 ABG mild met acidosis CXR bibasilar atelectasis ECG sinus tachycardia, Next? 20
21 Mr. MS Bood transfusion started. Taken immediately OR where bleeding identified from a short gastric artery. Ligated. 1 L blood evacuated. Given 6U prbc, 4U FFP and 5U Plts intraop Brought to PAR and remains intubated Hypovolemic shock
22 Mr. MS( cont.. On POD 2, complains of substernal chest pain and SOB. BP falls to 90/60mmHg with HR 120. Neck veins are distended. Most likely cause?
23 Acute Respiratory Failure Zengxuan Hu OCT17 23
24 Definition Defect in one or both gas exchange functions: oxygenation and carbon dioxide elimination PaO2<60mmHg or PaCO2>45mmHg Derangements in ABGs
25 Types I, Hypoxemic II, hypercapnic III, Perioperative I V, Shock Mechanism V/ Q mismatch Alveolar ventilation Atelectasis Hypoperfusion Etiology Airspace flooding 1. CNS drive 2. N-M coupling FRC 1. Cardiogenic 2. hypovolemic 3. Septic Clinical Description 1. ARDS 2. Alveolar hemorrhage 1. Overdose/CNS injury 2. Myasthenia gravis, upper abdominal incision, anesthesia 1. Myocardial infarct 2. endotoxemia, bacteremia
26 Mechanism Hypoventilation V/Q mismatch Shunt Diffusion abnormality

27 Hypoventilation Won t breathe resp drive Brainstem stroke Sedatives Can t breathe NM system Lung/airway Chest wall/pleura PaCO2 and PaO2 Alveolar arterial PO2 gradient is normal
28 V/Q mismatch Capillary flow excessive relative to vent V/Q ratio < 1 Small airway occlusion-asthma Alveoli-collapse,fluid, excessive capillary blood flow Admin. of 100% O2 eliminate hypoxemia
29 Shunt The deoxygenated blood bypasses the alveoli and mixes with oxygenated blood hypoxemia Persistent of hypoxemia despite 100% O2 inhalation Hypercapnia occur when shunt is excessive > 50%
30 Intracardiac Causes of Shunt Right to left shunt Pulmonary Fallot s tetralogy Eisenmenger s syndrome A/V malformation Pneumonia Atelectasis/collapse Pulmonary hemorrhage Pulmonary contusion

31 Diffusion Abnormality Abnormality of the alveolar membrane the number of the alveoli ARDS Fibrotic lung disease
32 Presentations of hypoxia Respiratory tachypnea, dyspnea CNS effects Impaired judgment and cognitive function Depressed brainstem function-consciousness Cardiovascular effects Arrhythmia Myocardial depression Hypotension, Shock
33 Presentations of hypercapnia CNS-mental status change Anxiety, irritability Confusion Lethargy, Stupor, coma Respiratory shallow breathing Cardiovascular effects Hypotension Ventricular irritability
34 ABG CBC, Hb Anemia Polycythemia Urea, Creatinine Electrolytes (K, Mg, Ph) Troponin TSH Diagnosis of RF -Investigations tissue hypoxemia chronic RF Aggravate RF MI Hypothyroidism
35 Chest x ray Echocardiography Diagnosis of RF Investigations PFT- (FEV1/ FVC ratio) Decrease Increase Pulmonary edema ARDS Cardiogenic ARDS Rt ventricular hypertrophy in CRF Airflow obstruction Restrictive lung disease
36 Investigations ECG cardiac cause of RF Arrhythmia due to hypoxemia & severe acidosis Right heart catheterization Pulmonary capillary wedge pressure (PCWP) Normal ARDS (<18 mmhg) Increased Cardiogenic pulmonary edema
37 Hypoxemic Respiratory Failure Yes Hypoventilation Is PaCO2 increased? No (PAO2 - PaO2)? (PAO2 - PaO2) Yes No Hypoventilation alone Respiratory drive Neuromuscular dz Hypovent plus another mechanism Shunt Is low PO2 correctable with O2? No Yes V/Q mismatch Inspired PO2 High altitude FIO2
38 Hypercapnic Respiratory Failure PaCO2 >45mmHg Not compensation for metabolic alkalosis (PAO2 - PaO2) normal Alveolar Hypoventilation increased V/Q abnormality PI max Nl VCO2 VCO2 Central Hypoventilation Neuromuscular Disorder V/Q Abnormality Hypermetabolism Overfeeding

39 Management A B C, identify reversible causes Endotracheal intubation: Indications Severe Hypoxemia Altered mental status Severe acidosis
40 Mechanical ventilation Increase PaO2 Lower PaCO2 Rest respiratory ms (respiratory ms fatigue)


41 Noninvasive Ventilatory support (IPPV) Mild to moderate RF Intact airway, Alert, normal airway protective reflexes Nasal or full face mask, BPAP,CPAP Improve oxygenation, Reduce work of breathing Increase cardiac output
42 Treating Underlying Disease Antibiotics Pneumonia Infection Bronchodilators (COPD) Salbutamol reduce bronchospasm airway resistance Anticholinergics (COPD) Ibratropium bromide inhibit vagal tone relax smooth ms
43 Hemodynamic Support Fluids and electrolytes Maintain fluid balance and avoid fluid overload Reduction of O2 requirements Vasopressor, inotropes The maintenance of cardiac output is crucial for O2 delivery Diuretics (pulmonary edema) Frusemide, Metalozone

44 Ventilation strategy Recruitment maneuvers Prone Inhaled nitric oxide High frequency oscillation 44
45 Case study A 58 M with no known medical histoy admitted for gallstone pancreatitis. Receives supportive care. POA 2 getting worse.sob. Tachypneic 35/min. Shallow breathing. Using accessory muscles. On 70 % O2 with mask. Anxious. BP 110/60, HR 90, Temp 37.5, GCS 15 ABG PH 7.34, Po2 40, Pco2 40, Diminished breath sounds bilaterally with scattered rhonchi CXR: bilateral nonsegmental infiltrates. no effusion or PTX. What findings suggest RF? What form of RF? Does he require intubation?

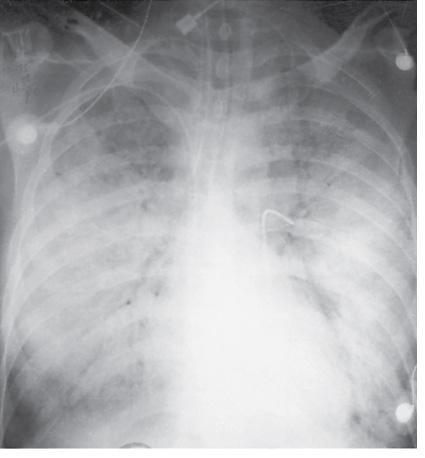
46 CXR-bilateral infiltration 46
 Intubation:severe hypoxemia, tachypneicimpending respiratory arrest, underlying disease process not")
47 Case study Diagnosis ARF type 1 ARDS/Acute lung injury DD: Aspiration, pnuemonia, PE, cardiogenic pulmonary edema, lung contusion(trauma) Intubation:severe hypoxemia, tachypneicimpending respiratory arrest, underlying disease process not clear.
48 Case study 57 F with Myasthenia Gravis x 1 yr on MESTINO(pyridostigmine) 40mg daily Depression with borderline personality feature. Presents to ER with 2 week s general weakness, mild SOB x 2 days. In no cute distress. Vitals N. SaO2 95% with 4 L NP VC x 3 showed 800ml. ABG 7.35/48/31. Po2 73. CXR possible right side pneumonia. What form of RF? Management?
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Interpretation of Arterial Blood Gases. Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB)
") Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Weeks 1-3:Cardiovascular
 Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Weeks 1-3:Cardiovascular Cardiac Output The total volume of blood ejected from the ventricles in one minute is known as the cardiac output. Heart Rate (HR) X Stroke Volume (SV) = Cardiac Output Normal
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Interpretation of Arterial Blood Gases (ABG)
") Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Arterial Blood Gases. Dr Mark Young Mater Health Services
 Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Dr. Sinan Butrus F.I.C.M.S. Clinical Standards & Guidelines. Kurdistan Board For Medical Specialties
 Guidelines For the Management of Respiratory Acidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Respiratory acidosis is an acid-base balance
Guidelines For the Management of Respiratory Acidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Respiratory acidosis is an acid-base balance
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SHOCK. May 12, 2011 Body and Disease
 SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
SHOCK May 12, 2011 Body and Disease Shock Definition of shock Pathophysiology Types of shock Management of shock Shock Definition? Shock What the Duke Community would have experienced if Gordon Hayward
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Shock Management. Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate. PDF created with pdffactory Pro trial version
 Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Shock Management Seyed Tayeb Moradian MSc, Critical Care Nursing Ph.D Candidate Definition of Shock The definition of shock does not involve low blood pressure, rapid pulse or cool clammy skin - these
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Outline. ABG Interpretation: A Respirologist s approach. Acid-Base Disturbances. What use is an ABG? Acid-Base Disturbances. Alveolar Ventilation
 Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
to optimize By Jin Xiong Lian, BSN, RN, CNS
 Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Successful Strategies to Improve Surgical ICU Documentation
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Successful Strategies to Improve Surgical ICU Documentation Brent Hadder, MD Assistant Professor, Department of Anesthesia
7th Annual Association for Clinical Documentation Improvement Specialists Conference Successful Strategies to Improve Surgical ICU Documentation Brent Hadder, MD Assistant Professor, Department of Anesthesia
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Normal Cardiac Anatomy
 Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Mosby,, an affiliate of Elsevier Normal Cardiac Anatomy Impaired cardiac pumping Results in vasoconstriction & fluid retention Characterized by ventricular dysfunction, reduced exercise tolerance, diminished
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Respiratory Failure how the respiratory physicians deal with airway emergencies
 Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Arterial Blood Gas Analysis
 Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the
 Objectives At the end of the session the") Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Clinical Application of Point of Care Testing. Tom Ahrens, PhD, RN, CCNS, FAAN Research Scientist Barnes-Jewish Hospital St.
 Clinical Application of Point of Care Testing Tom Ahrens, PhD, RN, CCNS, FAAN Research Scientist Barnes-Jewish Hospital St. Louis, MO Are We Monitoring Patients the Right Way? No. Our current practices
Clinical Application of Point of Care Testing Tom Ahrens, PhD, RN, CCNS, FAAN Research Scientist Barnes-Jewish Hospital St. Louis, MO Are We Monitoring Patients the Right Way? No. Our current practices
Respiratory failure Dr. Kamaran
 Respiratory failure Dr. Kamaran Respiratory failure refers to a condition in which pulmonary gas exchange fails to maintain normal arterial oxygen and carbon dioxide. Respiratory failure is a condition
Respiratory failure Dr. Kamaran Respiratory failure refers to a condition in which pulmonary gas exchange fails to maintain normal arterial oxygen and carbon dioxide. Respiratory failure is a condition
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than