Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
|
|
|
- Alison Garrett
- 6 years ago
- Views:
Transcription
1 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College of Medicine, Mayo Clinic
2 DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None
3 Topics Systolic Blood Pressure Intervention Trial (SPRINT): a clinical practice changing study? Heart Outcomes Prevention Evaluate 3 (HOPE 3): Can statins and/or antihypertensive drugs lower CV risk in a population without dyslipidemia or hypertension and without baseline CVD? What is the best add-on drug in patients with resistant hypertension? Allopurinol: new uses for an old drug?
4 In an otherwise healthy 80 year old patient with hypertension, the Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that reducing the SBP to 120/80 resulted in all but one of the following: A. A significant reduction in cardiovascular and all cause mortality B. This benefit occurred regardless of baseline frailty status and/or gate speed C. A higher incidence of acute kidney injury but not in eventual renal outcomes (50% decrease in egfr, dialysis, or transplant) D. More syncope and orthostatic hypotension E. More injurious falls
5 In an otherwise healthy 80 year old patient with hypertension, the Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that reducing the SBP to 120/80 resulted in all but one of the following: A. A significant reduction in cardiovascular and all cause mortality B. This benefit occurred regardless of baseline frailty status and/or gate speed C. A higher incidence of acute kidney injury but not in eventual renal outcomes (50% decrease in egfr, dialysis, or transplant) D. More syncope and orthostatic hypotension E. More injurious falls
6
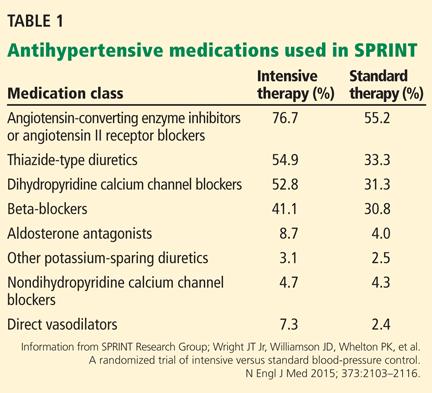
7 Systolic Blood Pressure Intervention Trial (SPRINT) Randomized 9361 persons 50 y/o with SBP 130 mm Hg (most on medications) and increased CV risk* but no DM, to SBP target <120 mm Hg (intensive) or <140 mm Hg (standard treatment) Primary composite outcome MI, other ACS, stroke, heart failure, death from CV cause
8 Systolic Blood Pressure Intervention Trial (SPRINT)
9 Systolic Blood Pressure Intervention Trial (SPRINT) Stopped early due to significantly lower rate of primary composite outcome of 1.65% per year in the intensive-treatment and 2.19% per year in standardtreatment group (HR with intensive treatment, 0.75; 95% confidence interval [CI], 0.64 to 0.89; P<0.001) All-cause mortality significantly lower in the intensivetreatment group (HR 0.73; 95% CI, 0.60 to 0.90; P = 0.003)
10


11 SPRINT results and adverse events
12 Is it really a good idea to lower BP to 120/80 mm Hg in patients 75 years or older?

13 Original Investigation April 2014 Antihypertensive Medications and Serious Fall Injuries in a Nationally Representative Sample of Older Adults Mary E. Tinetti, MD1,2; Ling Han, MD, PhD1; David S. H. Lee, PharmD, PhD3; Gail J. McAvay, PhD1; Peter Peduzzi, PhD2; Cary P. Gross, MD1; Bingqing Zhou, PhD2; Haiqun Lin, PhD2 [+] Author Affiliations JAMA Intern Med. 2014;174(4): doi: /jamainternmed

14 Williamson et al. JAMA 2016;315:
15 Background In the US: 75% of persons over 75 years have hypertension Benefits of antihypertensive treatment are conflicting Systolic hypertension in the elderly program (SHEP): benefits were limited to participants without a self-reported physical ability limitation Hypertension in the very elderly trial (HYVET): consistent benefit regardless of frailty status Williamson et al. JAMA 2016;315:
16 Baseline characteristics of patients 75 years or older Intensive treatment (SBP< 120), n=1317 Standard treatment (SBP<140), n=1319 IT ST Williamson et al. JAMA 2016;315:
17 Outcomes BPs: intensive: 123/62 standard: 135/67 Intensive: 1 additional drug, 121 vs. 124 mm Hg in fit vs. frail, no difference in standard group The absolute rate of serious adverse events was higher, but not statistically different in the intensive vs. the standard treatment group for Hypotension (2.4 vs. 1.4%) Syncope (3.0 vs. 2.4%) Electrolyte abnormalities (4.0 vs. 2.7%) Acute kidney injury (5.5 vs. 4.0% The were no differences in the incidences of injurious falls or orthostatic hypotension Williamson et al. JAMA 2016;315:
18 Outcomes (continued) Williamson et al. JAMA 2016;315:
19 Conclusions Lowering SBP to the 120s in the elderly reduces CV events and all cause mortality regardless of frailty status (despite a mean DBP of 62) Generally well tolerated How to approach management of hypertension in a community dwelling patient 75 years or older and without baseline orthostatic hypotension (SBP< 110 after 1 minute standing): Begin with an initial SBP goal of <140 and if tolerated well, try for <130
20 In a 65 year old man without known cardiovascular disease, BP 138/82 and LDL-C 127, what may be an effective strategy to reduce cardiovascular risk? A. rosuvastatin 10 mg/d B. candesartan 16 mg and hctz 12.5 mg/d C. both D. neither
21 In a 65 year old man without known cardiovascular disease, BP 138/82 and LDL-C 127, what may be an effective strategy to reduce cardiovascular risk? A. rosuvastatin 10 mg/d B. candesartan 16 mg and hctz 12.5 mg/d C. both D. neither
22 The polypill : a strategy to reduce cardiovascular disease by more than 80% Wald NJ, Law MR, BMJ 2003;326:1419 Heart attack, stroke, other preventable cardiovascular diseases kill or seriously affect half the population in Western societies Drug treatment to prevent IHD and stroke have been limited to single risk factors, targeting the minority of patients in the tail end of risk factor distribution and reducing them to the level of the average population 96% of deaths from IHD and stroke occur in people 55 yrs with average or high normal risk factor values (average age is yrs), therefore, to meaningfully reduce CV disease morbidity and mortality, everyone 55 or older needs to be treated with drugs
23 The polypill Contents Statin: 10 mg atorvastatin or other equivalent 3 BP drugs (1/2 usual starting dose) Hctz, atenolol, and an ACEI Folic acid (remember this is 2003) Aspirin (low dose) Risk reduction and adverse events (age 55 yrs) were based on results of individual clinical trials of each drug separately-and then multiplying the relative risks of each agent for a combined effect Years of life gained calculated from population studies/registry data of longevity in people 55 or older who did not have a vascular disease event Wald NJ, Law MR, BMJ 2003;326:1419

24 The polypill: risk reduction Wald NJ, Law MR, BMJ 2003;326:1419

25 The polypill: proportion of people who would benefit and years of event-free life gained Adverse events: 8% if 3 best tolerated bp drugs used: hctz, ARB, CCB 15% if 3 previously described, least expensive bp drugs used Wald NJ, Law MR, BMJ 2003;326:1419
26 The polypill: Conclusions (provocative to say the least) In people 55 or older: may prevent 88% or heart attacks, 80% of strokes and 1 in 3 would gain an average of years without having a heart attack or stroke All people 55 or older should be treated No need for baseline risk factor measurements (LDL-C, BP, homocysteine, platelet function) since intervention should be effective regardless of baseline values No need for monitoring in most patients in absence of symptoms or particular concern for events e.g., asthma-bb, renal disease-acei or ARB, etc Should be low-cost since all drugs now generic If a drug formulation prevented all cancers and was safe, would it be widely used? Wald NJ, Law MR, BMJ 2003;326:1419
27 N Engl J Med 2016;374:
28 HOPE-3 N=12,705 pts (men 55 or older, women 65 or older with at least one CV risk factor though women could be 60 or older with 2 risk factors): Elevated waist-to-hip ratio Low HDL-C Impaired glucose tolerance Current or recent tobacco use FH premature CAD Early renal dysfunction No indication or contraindication to study drugs Could have hypertension but not on an ACEI, ARB, or thiazide diuretic There were no specific lipid or BP levels mandated for entry N Engl J Med 2016;374:
29 HOPE centers, 21 countries Patients randomized to: Candesartan 16 mg plus HCTZ 12.5 mg or placebo Rosuvastatin 10 mg or placebo No specific LDL-C or BP targets Outcomes: First coprimary: composite of death from CVD, nonfatal MI, nonfatal stroke Second coprimary: composite of above plus resuscitated cardiac arrest, heart failure, or revascularization Secondary outcome: second coprimary plus angina with evidence of ischemia Planned mean f/u of 5 years N Engl J Med 2016;374:
 Mean SBP 138 mm Hg Mean LDL-C 128 mg/dl Mean f/u 5.")

30 HOPE-3 Baseline characteristics: Mean age 65.7 yrs (46.2% women) Mean SBP 138 mm Hg Mean LDL-C 128 mg/dl Mean f/u 5.6 yrs Adherence: at end of trial, 75% in dual Rx group remained on Rx vs 72% for the dual placebo group Adverse effects: muscle weakness and dizziness higher in the combined-therapy group N Engl J Med 2016;374:
31 Systolic blood pressure Mean decrease: 6.2 Hg mm, combined Rx vs dual placebo N Engl J Med 2016;374:
32 LDL-cholesterol Mean decrease: 33.7 mg/dl, combined Rx vs dual placebo N Engl J Med 2016;374:
33 Coprimary and secondary outcomes N Engl J Med 2016;374:

34 Coprimary and secondary outcomes Differences for candesartan/hctz vs dual placebo=ns
35 Conclusions In intermediated risk patients treated for 5.6 yrs, rosuvastatin plus candesartan/hctz reduced cv events vs dual placebo Relative RR=29%, absolute RR=1.4% NNT to prevent one coprimary outcome event =72, 63 for a secondary outcome event Benefit attributed to rosuvastatin although trend towards benefit with BP drugs in the top third of pts with the highest baseline SBP? Diuretic dose too low (should have been chlorthalidone?) Polypill may not yet be ready for prime-time New Engl J Med 2016;374: , , and
36 A 62 year old woman with hypertension presents with an office BP of 157/90 and home BPs averaging 152/84. Drugs are HCTZ 50 mg/d, amlodipine 10 mg/d, and losartan 100 mg/d. A previous screen for secondary causes of hypertension was negative. The most effective next add-on drug is: A. Bisoprolol 5 mg/d B. Spironolactone 25 mg/d C. Doxazosin 4 mg/d D. Minoxidil 2.5 mg/d
37 A 62 year old woman with hypertension presents with an office BP of 157/90 and home BPs averaging 1/84. Drugs are HCTZ 50 mg/d, amlodipine 10 mg/d, and losartan 100 mg/d. A previous screen for secondary causes of hypertension was negative. The most effective next add-on drug is: A. Bisoprolol 5 mg/d B. Spironolactone 25 mg/d C. Doxazosin 4 mg/d D. Minoxidil 2.5 mg/d
38 2011 MFMER slide- 38 Resistant Hypertension Definition Failure to reach the BP goal (<140/90 mm Hg) based on office BP: Appropriate three-drug regimen that includes a diuretic Full doses of all drugs Adherence to therapy Controlled BP requiring 4 drugs AHA Professional Education Committee of the Council for High Blood Pressure Research
39 2011 MFMER slide- 39 Resistant Hypertension Prevalence Unknown 15-20% referral clinics and clinical trials ALLHAT 42,418 participants 30% on 3 or more BP medications Control rate 66% Furberg CD et al. JAMA 2002;288:2981 Loetta G et al. J Hum Hypertens 2008;22:119
40 2011 MFMER slide- 40 Ambulatory blood pressure measurement in resistant hypertension 68,045 patients in Spanish registry 8295 (12.2%) with resistant HTN Office BP 140/90 mm Hg on 3 drugs with one being a diuretic After ABPM: 5182 (62.5%) True RH 3113 (37.5%) White-Coat RH Cut-point ABPM: 24-hr average BP <130/80 mm Hg Hypertension 2011;57:
41 2011 MFMER slide- 41 Resistant Hypertension Management Steps Exclude white-coat effect, noncompliance, interfering substances and secondary causes Control ECV - dietary sodium, diuretic appropriate for level of renal function Titrate drugs to maximum tolerable doses Combine drugs with complimentary mechanisms of action: Diuretic + RAAS blocker + CCB Spironolactone as a fourth agent Resulted in significant reduction by office BP or ABPM in metaanalysis of 15 studies (Dahal et al. Am J Hypertens 2015;28: )
42 Spironolactone not only lowers blood pressure.
43 OSA may be the most common secondary cause of hypertension Konecny, Kara, Somers. Hypertension 2014;63:

44 Complex interactions between OSA and BP Konecny, Kara, Somers. Hypertension 2014;63:
45
46 Gaddam et al. J Hum Hypertens 2010;24:

47 Changes in OSA parameters after treatment with spironolactone Gaddam et al. J Hum Hypertens 2010;24:
48 How could spironolactone improve OSA indices? OSA is associated with significant extracellular volume expansion-typically not controlled on a thiazide diuretic At night when supine, fluid mobilization leads to peripharyngeal fluid accumulation resulting in increased pharyngeal obstruction-aldosterone must play a role Other evidence of a role for volume overload:-volume reduction improves OSA in: CHF ESRD pts switched to nocturnal hemodialysis or peritoneal dialysis

49 Hypothesis: resistant hypertension is predominantly caused by sodium retention, therefore, spironolactone will be the most effective add-on agent and its effectiveness will be inversely proportional to the baseline plasma renin level Lancet 2015;386:
50 Study Design Inclusion criteria Clinic SBP 140 ( 135 for diabetics) and home SBP 130 (mean of 18 readings over 4 days) Maximally tolerated doses of ACEI/ARB + CCB + diuretic Ages yrs 4 week placebo run in, then randomized to spironolactone (25-50 mg), doxazosin (4-8 mg), bisoprolol (5-10 mg) or placebo All subjects receive all drug in randomized fashion for 12 weeks (first 6 at low dose, second 6 at higher dose) Primary outcome measurement: average home SBP measured in triplicate AM and PM for 4 consecutive days prior to a study visit (Micolife automated device) Lancet 2015;386:

51 Baseline Characteristics Lancet 2015;386:

52 Results: blood pressure Lancet 2015;386:


53 Results: blood pressure Lancet 2015;386:

54 The lower the baseline renin, the better the response to spironolactone Lancet 2015;386:
 of the 285 patients exposed to spironolactone developed a serum potassium on a single occasion of > 6 meq/l (maximum 6.")
55 Results: Adverse Events Discontinuations due to renal impairment, hyperkalemia, and gynecomastia were not increased with spironolactone vs all others Mean change in serum K was 0.45 meq/l 6 (2%) of the 285 patients exposed to spironolactone developed a serum potassium on a single occasion of > 6 meq/l (maximum 6.5) Lancet 2015;386:
56 Conclusions Spironolactone was more effective than doxazosin or bisoprolol in reducing home blood pressure in patients with resistant hypertension Spironolactone was most effective in patients with the lowest baseline plasma renin (supporting the hypothesis of volume expansion in patients with resistant hypertension) Despite adding spironolactone to a regimen of an ACEI or ARB, the risk of hyperkalemia was low (though should be followed closely, at least initially) It is my go-to drug, particularly in the setting of OSA and obesity Lancet 2015;386:
57 Allopurinol has been demonstrated to do all of the following except: A. Lower blood pressure B. Reduce the development of new kidney disease and delay the progression of chronic kidney disease C. Reduce the risk of coronary events and stroke D. Increase the risk of Type 2 Diabetes Mellitus
58 Allopurinol has been demonstrated to do all of the following except: A. Lower blood pressure B. Reduce the development of new kidney disease and delay the progression of chronic kidney disease C. Reduce the risk of coronary events and stroke D. Increase the risk of Type 2 Diabetes Mellitus
59 Uric acid is a player in cardiovascular and kidney disease Hypertension 2016;67:
60 Clinical studies of allopurinol Lowers blood pressure in adolescents (JAMA 2008;300:924) and older adults (J Clin Hypertens 2013;15:435) Delays progression of renal disease and reduces cardiovascular risk and hospitalizations in patients with CKD (Clin J Am Soc Nephrol 2010;5:1388) Decreases the new onset of renal failure in people 65 years or older (the higher the dose and the longer the treatment the better)(ann Rheum Dis 2016;0:1)

61 Hypertension 2016;67:
62 Methods United Kingdom Clinical Research Practice Datalink (UK CRPD): Demographics, diagnoses, medical histories, prescriptions from 500 primary care practices (n > 3.4 million patients) Identified 2400 pts 65 yrs or older and on allopurinol (presumably for gout) and 42,000 matched controls not on allopurinol. All subjects had a dx of hypertension Exclusions: CKD Primary outcomes (new event over 10 yrs follow-up): Stroke Cardiac event (MI or acute coronary syndrome Hypertension 2016;67:
63 Baseline characteristics Any Allopurinol Exposure No Yes Age (y) BP 156/86 157/86 Sex (% female) Gout?? Yes group: higher BMI, higher creatinine, less CCB use, more DM and ACEI use, same amount of diuretic use Hypertension 2016;67:

64 Results Allopurinol dosing: Low: <300 mg/d High: mg/d Serum uric acid levels: Pre-Rx only available in onethird of allopurinol group with f/u levels available in one-third of that group Mean mg/dl Hypertension 2016;67:
65 Conclusions Allopurinol was associated with a reduced risk of both stroke (by 50%) and cardiac events (by 39%) in hypertensive patients 65 yrs or older This benefit appears limited to patients on allopurinol doses of 300 mg/d or higher Limitations retrospective Indications for allopurinol not specified Gout is an independently-associated risk factor for CVD Limited serum uric acid data Need for prospective clinical trials
66 Take-home Points In hypertensive patients age 75 and older, decreasing systolic blood pressure towards 120 mm Hg may be well tolerated and beneficial (CVD, all-cause mortality) In patients with intermediate cv risk factors and without clinical cvd, treatment with rosuvastatin (regardless of LDL-C) may be beneficial Spironolactone is the best add-on drug in patients with resistant hypertension Consider the use of allopurinol in older hypertensive patients with hyperuricemia, especially in the setting of chronic kidney disease
67 Thank you
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
JNC-8. (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines
 An Update on Hypertension Guidelines") JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
The State of Hypertension in NZ in 2010 personal view
 The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4)
 and The International Polycap Study 3 & 4 (TIPS 3 & 4)") The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Hypertension and Cholesterol in the Elderly
 Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden