Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
|
|
|
- Phebe Lambert
- 6 years ago
- Views:
Transcription
1 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
2

3 ACHD Resources in Ohio ACHAHEART.ORG
4 Situations When We Might Help When you don t know a lot about a CHD diagnosis. When a CHD diagnosis includes a person s name. Fontan. Mustard. Senning. Rastelli. Jatene.
5 Situations When We Might Help CHD patients who are cyanotic. CHD patients with pulmonary hypertension. CHD patients with only one ventricle. CHD patients needing noncardiac surgery. CHD patients needing special cardiac surgery. David operation. Ross procedure. Aortic valve repair.
6 Situations When We Might Help CHD patient candidates for a heart catheterization. Sexually active CHD patients. CHD patients contemplating pregnancy. Pregnant CHD patients. CHD patients with arrhythmias. CHD patients with syndromes.
7 Consider ACHD clinics to contain resource people who have developed networks of specialists with special interests and abilities.

8 The Toronto Congenital Cardiac Centre for Adults founded 1959
9
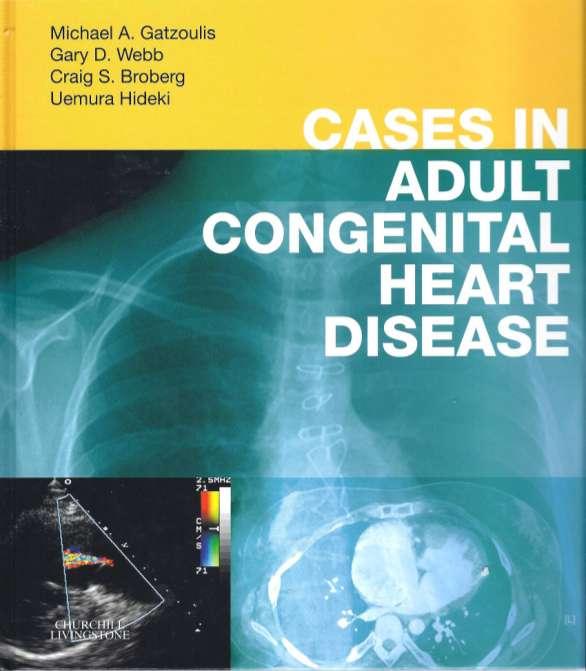
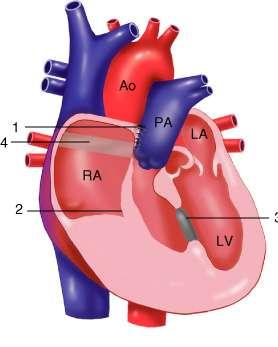
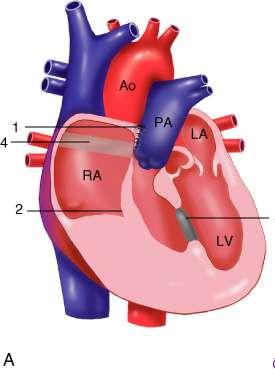
10 Patient 63 - History 31-year-old female supermarket clerk 16 weeks pregnant. Cyanotic at birth. Left BT shunt at age 11. Lateral tunnel Fontan procedure at age 20. Lost to follow-up until age 31.
11
12 Patient 63 - History NYHA class I. No functional decline recently. No medications.
13 Patient 63 Risk Factors Don t know much about that. Fontan. Blalock Taussig. Man s name. Pregnancy.
14 What is a Fontan procedure? I don t know. A type of transposition repair. A type of tetralogy repair. A type of single ventricle repair.
15 What are the pregnancy issues associated with a Fontan procedure? Choose as many as are applicable Atrial flutter. Thromboembolism. Fetal loss. Cyanosis. Maternal death. All of the above.

16 Patient 63

17 Patient 63
18 Fontan Pregnancy Management Close monitoring. High-risk pregnancy team. Consider anticoagulation. Planned vaginal delivery. Planned epidural.
19 Patient 63 Patient Course and Outcome Induced at 39 weeks. Epidural anesthetic. Normal vaginal delivery. Healthy baby boy.
20
21 Patient 61 - History 24-year-old man, works as an engineer. Born with tricuspid atresia. Palliated with bilateral Blalock-Taussig shunts. Atriopulmonary Fontan procedure at age 6. Started on warfarin at age 16 for possible pulmonary embolism.
22
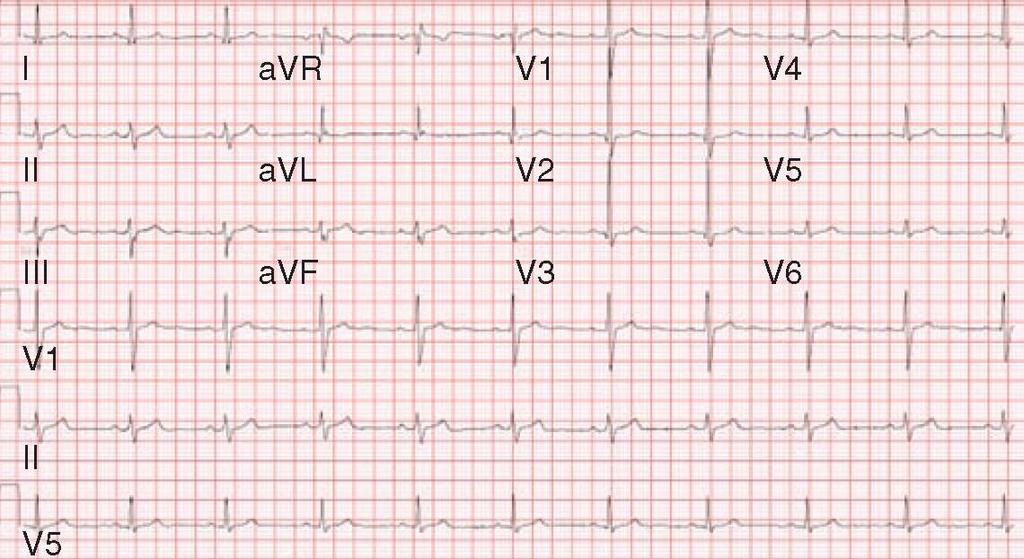
23 Patient 61 - History At age 17, developed recurrent atrial flutter. Treated with various antiarrhythmics, including amiodarone. By age 21, was in chronic atrial fibrillation. Was otherwise doing well (NYHA I).
24 Patient 61 - Physical Examination BP 118/72 Pulse 70 (irregular) Height 68 inches Weight 137 pounds Pulse oximetry 96%
25 Patient 61 - Physical Examination Bilateral thoracotomy and midline sternotomy scars. JVP hard to assess. Chest clear. Normal precordial examination. Normal heart sounds with no murmurs. No hepatomegaly, ascites, or edema.
26 Patient 61 Risk Factors Don t know much about that. Fontan. Blalock Taussig. Man s name. Arrhythmia. One ventricle.

27 Patient 61
28 Patient 61 - What next steps? Optimize anticoagulation. Refer for immediate surgery. Consider thrombolysis. No specific treatment needed.
29 Patient 61 Decision and Management A Fontan revision was elected. Right atrial thrombus removed along with excess right atrial tissue. Extracardiac Fontan constructed. Arrhythmia surgery not possible because of operative difficulties.
30
31 Patient 61 Decision and Management Immediately postoperatively Hemodynamically unstable Persistent bleeding Sternal closure impossible, so skin only closure. Maximum pressors.
32 Patient 61 Decision and Management Postoperative complications Compartment syndrome left leg. Recurrent tension pneumothorax. Acute tubular necrosis Tracheotomy.. Discharged home after four months, in atrial fibrillation, and on warfarin.

33 Patient 61
34
35 Patient 53 - History 38-year-old woman Original CHD diagnoses TGA VSD PS Age 7, Rastelli procedure with a 20 mm Dacron conduit including a Hancock valve

36 Rastelli Procedure
37 Patient 53 - History Age 25, Strep sanguis endocarditis She was found to have severe conduit obstruction, moderate subaortic stenosis, a small residual VSD, and preserved biventricular function. Her conduit was replaced using a homograft, her VSD was enlarged to reduce the LVOT gradient, and a baffle was placed between LV and the aorta.
38 Patient 53 - History Age 35, heart catheterization showed a 40 mmhg gradient across the RV-PA conduit with mild LVOTO and mild AR. Sotalol was started for suspected paroxysmal atrial tachycardia. Age 38, NYHA class III with exertional dyspnea and fatigue. She is limited to 100 yards on the flat. She avoids steps. Current medications: warfarin; sotalol 80 mg BID; furosemide 20 mg daily; sertraline 100 mg daily
39 Patient 53 - Physical Examination BP 110/70 Pulse 46 Height 70 inches Weight 209 pounds Pulse oximetry 97%
40 Patient 53 - Physical Examination JVP 8 cm ASA. Chest clear. Possible right ventricular lift. Second sound loud and single. Grade 4 long ejection systolic murmur upper left sternal border. No hepatomegaly or edema.
41 How much conduit obstruction does she have? Mild. Moderate. Severe. Don t know.

42 Patient 53

43 Patient 53
44 Patient 53 - Echo Report Normal LV size and function. Peak LVOT gradient 20 mmhg. RVH with mild-moderate hypokinesis. Mild TR. Valved conduit not seen.
45 Patient 53 Risk Factors Don t know much about that. TGA. VSD/PS. Man s name. Exercise intolerance. Sexually active.

46 Patient 53

47 Patient 53

48 Patient 53

49 Patient 53
50 Patient 53 Why is she NYHA class III? Choose as many as are applicable The stenosed conduit? The sotalol? Chronotropic incompetence? Anemia? Lung disease?
51 Patient 53 Management and Outcome Conduit from RV to PA removed and replaced. Smooth postop course. Patient NYHA I after convalescence.
52
53 Patient 41 - History 31-year-old woman Original CHD diagnoses Tetralogy of Fallot Age 3, transannular patch repair. Progressive pulmonary regurgitation, severe. Asymptomatic and full time work, but has slowed down a bit.
54 Patient 41 - Physical Examination BP 110/70 Pulse 70 Height 62 inches Weight 189 pounds Pulse oximetry 100%
55 Patient 41 - Physical Examination Midline sternotomy scar. Normal JVP. RV heave. Grade 2 ejection systolic murmur. Grade 2 low pitched diastolic murmur.

56 Patient 41

57 Patient 41
58 Patient 41 - Echo Report Normal LV size and function. Right ventricle severely dilated. Laminar (severe) pulmonary regurgitation.
59 Patient 41 Risk Factors Don t know much about that. Tetralogy. Pulmonary regurgitation. Man s name. Candidate for a heart catheterization.
60 Patient 41

61 Patient 41

62 Patient 41
63 Patient 41 Pulmonary Regurgitant Fraction 48%
64 Patient 41 Treatment Options? Choose as many as are applicable Bioprosthetic pulmonary valve replacement. Mechanical pulmonary valve replacement. Percutaneous pulmonary valve replacement. Continued observation.
65 Patient 41 Plan and Outcome Pulmonary valve replacement elected. 23 mm homograft used (bioprosthesis). Previous patch excised. Exercise intolerance for improved after convalescence. RV volumes reduced by 30% on follow-up MRI.
66
67 Patient 25 - History 45-year-old man Original CHD diagnoses Aortic coarctation (isolated) Age 3, coarctation repair (details unknown). Recently found to have high blood pressure. Treated with an ACE inhibitor and a beta blocker. No cardiovascular symptoms.
68 Patient 25 - Physical Examination BP 156/70 right arm 115/60 left arm 118/? right thigh Pulse 44 Height 70 inches Weight 202 pounds Pulse oximetry 98%
69 Patient 25 - Physical Examination Left thoracotomy scar. Pulse delay right radial to right femoral. Very weak pedal pulses. Grade 2 ejection systolic murmur. Grade 2-3 murmur of aortic regurgitation. Faint continuous murmur heard over the back.

70 Patient 25

71 Patient 25

72 Patient 25 Patient 25 - Echo Report Bicuspid aortic valve. Mild aortic regurgitation. Normal left ventricular size and function. Coarctation gradient 47 mmhg with diastolic tail
73 Patient 25 - MRI Report Mild dilation of the ascending aorta. Hypoplastic distal aortic arch with severe coarctation. Collateralization present.

74 Patient 25 - MRI
75 Patient 25 Risk Factors Possible candidate for cardiovascular surgery. Possible candidate for a heart catheterization.
76 Patient 25 Treatment Options? Choose as many as are applicable Surgical repair of aortic coarctation. Balloon dilation of aortic coarctation. Stent placement for aortic coarctation. More aggressive antihypertensive therapy.

77 Patient 25 Plan and Outcome Stent therapy of aortic recoarctation elected.
78 Patient 25 Plan and Outcome BP right arm BP left arm BP right leg Prior to procedure 156/70 115/60 118/? 3 weeks after procedure 108/65 113/70 132/80

79 Patient 25 Plan and Outcome
80 Case 19
81 Patient 19 - History 26-year-old woman Original CHD diagnoses Normal heart Infective endocarditis Age 9 and 10, aortic valve repair for aortic regurgitation. Age 18, Ross procedure. Age 26, declining exercise capacity, limited to two floors vertically.
82 Patient 19 - Physical Examination BP 100/42 Pulse 100 Height 70 inches Weight 147 pounds Pulse oximetry 100%
83 Patient 19 - Physical Examination Bounding peripheral pulses. Positive Duroziez sign. Cardiac apex displaced and active. Grade 2 medium length ejection systolic murmur. Grade 2 high-pitched diastolic murmur LSB.

84 Patient 19

85 Patient 19

86 Patient 19
87 Patient 19 - Echo Report Left ventricle dilated to 62 mm diastolic. Normal LV systolic function. Ascending aortic dilation to 55 mm. Severe neoaortic valve regurgitation. Homograft function normal on the right side of the heart.

88 Patient 19 - Echo

89 Patient 19 - Echo
90 Patient 19 Risk Factors CHD patients needing special cardiac surgery. David operation. Ross procedure. Aortic valve repair?
91 Patient 19 - Which management would you consider? Choose as many as are applicable Bentall procedure with mechanical aortic valve. Bentall procedure with bioprosthetic aortic valve. Valve sparing root replacement.
92 Patient 19 Management and Outcome Valve sparing aortic root replacement elected. At surgery, the neoaortic valve leaflets appeared normal. The aortic annulus was less dilated than were the sinuses. The aorta was replaced using a David technique, sewing a 26 mm Dacron graft with preformed sinuses down to the annulus with resuspension of the neoaortic leaflets. The coronary arteries were reimplanted.
93 Patient 19 Management and Outcome The patient did well with no residual aortic valve regurgitation.

94 Patient 19 Management and Outcome
95 Case 6
96 Patient 6 - History 34-year-old woman Generally healthy childhood. Told that her heart was on the right side. Occasional episodes of hemoptysis as a teenager. Hemoptysis recurred after a recent successful pregnancy. Lifelong non-smoker. Very good exercise capacity.
97 Patient 6 - Physical Examination BP 100/68 Pulse 62 Height 56 inches Weight 141 pounds Pulse oximetry 98%
98 Patient 6 - Physical Examination Normal JVP. Clear chest. Right-sided apical impulse. Heart sounds normal, no murmurs. Right-sided liver.
99 Patient 6

100 Patient 6
101 Patient 6 - Echo Report Dextroposition of the heart with normal cardiac chamber anatomy. Mild right heart dilation. Normal RVSP.

102 Patient 6 - MRI

103 Patient 6 - MRI

104 Patient 6 Patient 6 - MRI

105 Patient 6 - CT

106 Patient 6 Patient 6 - CT
107 Patient 6 Risk Factors Don t know much about that. Anomalous pulmonary venous connection. Scimitar syndrome.
108 Patient 6 - What management would you consider? Choose as many as are applicable Observation. Surgical repair of scimitar circulation. Embolization of anomalous arterial supply. Surgical resection of abnormal lung segment.
109 Patient 6 Management and Outcome Observation was elected. Many patients with scimitar syndrome have a shunt less than 2/1 and do not need redirection of their venous return. She did not have lung sequestration on CT scanning. Her lung parenchyma was normal. Over an 8-year follow-up, the patient has done well.
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Congenital Heart Disease II: The Repaired Adult
 Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
PREGNANCY AND CONGENITAL HEART DISEASE
 PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
PREGNANCY AND CONGENITAL HEART DISEASE SIDDHARTH JADHAV M.D. Assistant Professor of Radiology E.B. Singleton Department of Pediatric Radiology Texas Children's Hospital COMMERCIAL DISCLOSURE - None Objectives
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease. Pregnancy and Cardiovascular Disease MCQ
 Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
Miscellaneous Cardiology Topics pregnancy - congenital - myocarditis - pericardial disease Maan Jokhadar, MD, FACC Emory Center for Advanced Heart Failure Therapy Emory Adult Congenital Heart Center Pregnancy
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Cardiovascular MRI of Adult Congenital Heart Disease
 Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
CongHeartDis.doc. Андрій Миколайович Лобода
 CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
CongHeartDis.doc Андрій Миколайович Лобода 2015 Зміст 3 Зміст Зміст 4 A child with tetralogy of Fallot is most likely to exhibit: -Increased pulmonary blood flow -Increased pressure in the right ventricle
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Anesthetic Considerations in Adults with Congenital Heart Disease
 CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Pulmonary Valve Replacement
 Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS
 ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS V.S. Mahadevan, MD, F.R.C.P. Director, Structural and Adult congenital Interventional Cardiology Program William W
ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS V.S. Mahadevan, MD, F.R.C.P. Director, Structural and Adult congenital Interventional Cardiology Program William W
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Adults With Congenital Heart. Disease. An Expanding Population. In this article:
 Adults With Congenital Heart Disease An Expanding Population Continued progress in diagnosing and managing infants and children with congenital heart disease will likely result in a better prognosis and
Adults With Congenital Heart Disease An Expanding Population Continued progress in diagnosing and managing infants and children with congenital heart disease will likely result in a better prognosis and
Adult with Cyanotic Congenital Heat Disease
 Adult with Cyanotic Congenital Heat Disease Savitri Srivastava Director, Pediatric & Congenital Heart Disease Fortis Escorts Heart Institute Okhla Road, New Delhi Cyanotic Adult WCC & IVUS 2015 Adult Cyanotic
Adult with Cyanotic Congenital Heat Disease Savitri Srivastava Director, Pediatric & Congenital Heart Disease Fortis Escorts Heart Institute Okhla Road, New Delhi Cyanotic Adult WCC & IVUS 2015 Adult Cyanotic
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pregnancy and Heart Disease. Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA
 Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
Pregnancy and Heart Disease Shilpa Kshatriya, MD, FACC Heartland Cardiology, PA Pregnancy and the Heart 2 % of pregnancies involve maternal CV disease CV disease does not preclude pregnancy but poses risk
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων
 Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
Έγκυος και συγγενής καρδιοπάθεια: Τι πρέπει να γνωρίζει ο Καρδιολόγος Ενηλίκων Αντώνιος Π. Βλάχος Αναπληρωτής Καθηγητής Παιδοκαρδιολογίας Πανεπιστήμιο Ιωαννίνων No conflict of interest Pregnancy and CHD
The Rastelli procedure has been traditionally used for repair
 En-bloc Rotation of the Truncus Arteriosus A Technique for Complete Anatomic Repair of Transposition of the Great Arteries/Ventricular Septal Defect/Left Ventricular Outflow Tract Obstruction or Double
En-bloc Rotation of the Truncus Arteriosus A Technique for Complete Anatomic Repair of Transposition of the Great Arteries/Ventricular Septal Defect/Left Ventricular Outflow Tract Obstruction or Double
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη
 Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Καρδιοπάθειες και κύηση. Υπάρχουν ενδείξεις διακοπής; Λαζαρίδου Φωτεινή, ΕΒ Καρδιολόγος Νοσοκομείο «Αγ Παύλος», Θεσσαλονίκη ~ 3% of women 18 44 years of age have cardiac disease ~ 1% of pregnancies are
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Adult Congenital Heart Disease: What Every Practitioner Should Know
 Adult Congenital Heart Disease: What Every Practitioner Should Know Sabrina Phillips, MD FACC FASE Associate Professor of Medicine Director of Adult Congenital Heart Disease Services The University of
Adult Congenital Heart Disease: What Every Practitioner Should Know Sabrina Phillips, MD FACC FASE Associate Professor of Medicine Director of Adult Congenital Heart Disease Services The University of
Difficult echocardiography in an adult patient with repaired congenital heart disease
 Difficult echocardiography in an adult patient with repaired congenital heart disease Markus Schwerzmann, MD Center for Congenital Heart Disease University of Bern Clinical history 19 year old male, 168
Difficult echocardiography in an adult patient with repaired congenital heart disease Markus Schwerzmann, MD Center for Congenital Heart Disease University of Bern Clinical history 19 year old male, 168
Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service
 Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service Objective 1 Hyperlipidemia does NOT cause congenital heart
Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service Objective 1 Hyperlipidemia does NOT cause congenital heart
Surgical Procedures. Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder
 PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
2018 Guideline for the Management of Adults with Congenital Heart Disease
 2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
Pregnancy and Heart Disease. Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital
 Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Pregnancy and Heart Disease Alexandra A Frogoudaki Adult Congenital Heart Clinic ATTIKON University Hospital Pregnancy is not a state Hemodynamic changes During pregnancy Estrogens 1. Renin 2.
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery
 Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Adult Congenital Heart Disease Certification Examination Blueprint
 Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the