Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure
|
|
|
- Myra George
- 6 years ago
- Views:
Transcription

1 June 28, 2016 Overview & Update on the Utilization of the Natriuretic Peptides in Heart Failure Linda C. Rogers, PhD, DABCC, FACB.
2 Agenda Overview of the Natriuretic Peptides and Efficacy studies Similarities and Differences Confounders Clinical Studies of Entresto and Implications for Measurement of the Natriuretic Peptides Page 2

3 Cardiac Natriuretic Peptides Physiological role: CNP Natriuresis, i.e., discharge of sodium by urinary excretion Regulates blood volume through osmotic hemodynamics ANP ANP Peptide ANP BNP CNP Stimulus for Release Atrial Distension Ventricular Overload Endothelial Stress BNP BNP Weber, et al. Heart 2006;92: xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 3



4 Physiology of BNP control Renin-angiotensin-aldosterone system (RAAS) Na+ Na+ Weber, et al. Heart 2006;92: Na+ Page 4
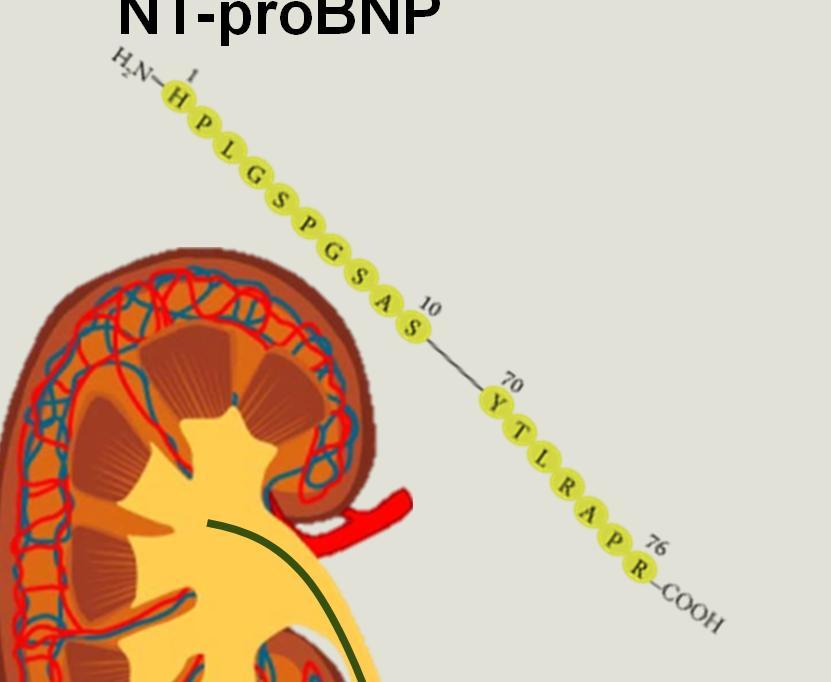
5 Natriuretic Peptides Hemodynamic NT-proBNP Stress 76 aaischemia ½ life Cardiotoxicity = 120 min Renal clearance Sepsis 1 Signal peptide HPhysiologically 2 N inactive (26 aa) H P L G S P G S A 10 S Cardiac myocyte BNP 32 aa 90 ½ life = 20 R K M D R I S ProBNP (108 aa) S min S S Pre-proBNP (134 aa) Enzymatic, C receptor, and renal clearance F G Physiologically C activec L Q G S G C Enzymatic K V L cleavage 70 Y T L R 76 A P R S P K M V R 108 R H COOH Blood stream COOH H2 N Martinez-Rumayor et al. Am J Cardiol 2008;101[suppl]:3A-8A Boerrigter, et al. Heart Fail Clin. Oct 2009; 5(4): Page 5 Unrestricted Siemens Healthcare Diagnostics Inc All rights reserved. Artifact #A91DX CAI UC1-4A00







6 Elimination Paths of BNP and NT-proBNP Impacts Half Life BNP NT-proBNP + + Half-Life = 20 minutes Half-Life = minutes Weber, et al. Heart 2006;92: Page 6 Siemens Healthcare Diagnostics

7 Decision Cut Points for Ruling Out Heart Failure NT-proBNP Age < 75 yrs: 125 pg/ml Age 75 yrs: 450 pg/ml BNP < 100 pg/ml These are the only accepted cut points, regardless of manufacturer. Source: Siemens IFU s Page 7


8 BNP and NT-proBNP Physiology Dilation of the left ventricle increases cardiac pre-probnp gene expression. The amount of pre-probnp released into the circulation is directly proportional to the extent of heart wall stretch. Pre-proBNP Thus, natriuretic peptide levels are an accurate reflection of the severity of heart failure. Page 8

9 Breathing Not Proper Study: BNP BNP is a useful test to distinguish patients with heart failure from those without heart failure. BNP is useful for both systolic and nonsystolic heart failure, even though nonsystolic heart failure diagnosis is more difficult to make and is oftern incorrectly excluded in the presence of normal left ventricular systolic function. BNP cannot reliably distinguish systolic dysfuncion from nonsystolic dysfunction: a measurement of left ventricular dysfunction is required to make this distinction and guide therapy accordingly. Maisel, et al. J Am Coll Cardiol. 2003;41: Page 9 Siemens Healthcare Diagnostics

10 PRIDE Study Supports the Clinical Utility of NT-proBNP NT-proBNP testing alone was superior to clinical judgment alone for diagnosing acute CHF. NT-proBNP plus clinical judgment was superior to NT-proBNP or clinical judgment alone. NT-proBNP measurement is a valuable addition to standard clinical assessment for the identification and exclusion of CHF in the emergency department setting. Januzzi, Am J Cardiol 2005;95: Page 10 Siemens Healthcare Diagnostics
11 ROC Curves Estimating Clinical Probability of Heart Failure Sensitivity a. McCullough PA, et al. Circulation. 2002;106: b. Januzzi JL, et al. Am J Cardiol. 2005;95: BNP Study a Specificity PRIDE Study b BNP + clinical assessment, AUC = NT-proBNP + clinical assessment, AUC = BNP alone, AUC = 0.90 NT-proBNP alone, AUC = Clinical assessment alone, AUC = 0.86 Clinical assessment alone, AUC = Page 11 Unrestricted Siemens Healthcare Diagnostics Inc All rights reserved. Artifact #A91DX CAI UC1-4A




12 Clinical Confounders to NP Interpretation CKD High BMI Age-associated increases 12 Page 12 Siemens Healthcare Diagnostics AFib

13 NP s in CKD BNP and NT-proBNP were elevated in kidney dysfunction even in the absence of systolic heart failure (SHF). NT-proBNP elevated more than BNP. Further research and association guidelines are necessary for clinical guidance. Jafri, et al. BMC Nephrol. 2013;14: Page 13 Siemens Healthcare Diagnostics
14 Impact of NPs in Patients with Renal Dysfunction and Dyspnea 2,250 BNP 16,000 NT-proBNP BNP (pg/ml) 2,000 1,750 1,500 1,250 1, NT-proBNP (pg/ml) 14,000 12,000 10,000 Manufacture decision cut-points are unchanged 8,000 6,000 4,000 2,000 0 > < 30 egfr (ml/min/1.73m2) Non-cardiac dyspnea 0 > < 30 egfr (ml/min/1.73m2) Chenevier-Gobeaux et al. Clin Chim Acta 2005;361: Cardiac dyspnea 14 Page 14 Siemens Healthcare Diagnostics
15 Natriuretic Peptides in Obese Patients with CHF BNP (pg/ml) BNP NT-proBNP p < NT-proBNP (pg/ml) Manufacture decision cut-points are unchanged p < ³ 30 Weight Categories (BMI) ³ 30 Weight Categories (BMI) Krauser, et al. Am Heart J. 2005;149: Page 15 Siemens Healthcare Diagnostics
16 Association Between Natriuretic Peptides and 1-Year Mortality Adjusted Risk Ration Quartile BNP pg/ml NT-proBNP pg/ml Q1 < 88 < 472 Q Q Q4 > 800 > Q1 Q2 Q3 Q4 N = 383 BNP NT-proBNP De Filippi, et al. Clin Chem 2007; 53: Page 16 Siemens Healthcare Diagnostics
17 Comparing BNP versus NT-proBNP Similarities Both show similar clinical diagnostic performance for HF. Both demonstrate prognostic performance (although NT-proBNP may outperform BNP). Studies for both suggest potential utility for therapeutic monitoring. Performance of both may be impacted by CKD (although NT-proBNP perhaps more so). Both may have clinical utility outside of HF (like ACS). Differences NT-proBNP appears more impacted by age (requiring age-specific cut-points). NT-proBNP has greater analytical stability (24 hours at room temp vs. 4 hours for BNP and NTproBNP may have greater stability when stored frozen). Absolute values are very different due to alternate mechanisms of clearance. BNP values are typically in the hundreds while NTproBNP can be in the thousands. Page 17
 and reduced ejection fraction.")
18 Intended Use LCZ696* A combination of sacubitril, a neprilysin inhibitor, and valsartan, an angiotensin II receptor blocker, indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II IV) and reduced ejection fraction. Usually administered in conjunction with other heart failure therapies, in place of an ACE inhibitor or other ARB. *trade name Entresto ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 18

19 Mechanism of Action of LCZ696 Valsartan Angiotensin Receptor Blocker LCZ696 Sacubitril Inhibition of Neprilysin Valsartan Blocks the angiotensin II type-1 (AT 1 ) receptor, inhibiting angiotensin II and the release of aldosterone. Neprilysin An endopeptidase that breaks down vasoactive peptides (BNP, bradykinin, and adrenomedullin); its inhibition may therefore reduce remodeling, vasoconstriction, and renal sodium retention and improve outcomes in HFrEF. Inhibition of neprilysin by LBQ657, the active metabolite of sacubitril, increases the levels of these peptides, decreasing vasoconstriction, sodium retention, and maladaptive remodeling. xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 19
20 The PARAMOUNT Trial The angiotensin receptor-neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomized controlled trial. Prospective comparison of ARNI (angiotensin receptor-neprilysin inhibitor) with ARB (angiotensin receptor blocker) on Management Of heart failure with preserved ejection fraction (PARAMOUNT). Solomon SD, Zile M, Pieske B, et al. Lancet. 2012;380(9851): Page 20
21 PARAMOUNT Trial: Inclusion and Exclusion Criteria Key Inclusion Criteria Age 40 years Documented stable chronic heart failure (NYHA II IV) with signs and symptoms of HF (dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, peripheral edema) LVEF 45% Plasma NT-proBNP >400 pg/ml at screening On diuretic therapy prior to visit 1, controlled systolic BP (<140 mmhg, or <160 mmhg if on three meds) egfr 30 ml/min/1.73 m 2 (MDRD) Patients with a K 5.2 mmol/l at visit 1 Key Exclusion Criteria Patients with a prior LVEF <45% at ANY time Patients who required treatment with both an ACE inhibitor and an ARB Isolated right HF due to pulmonary disease Dyspnea and/or edema from noncardiac causes, such as lung disease, anemia, or severe obesity Presence of valvular heart disease, hypertrophic cardiomyopathy, infiltrative cardiomyopathy, restrictive cardiomyopathy, or pericardial disease Coronary disease requiring revascularization during the study Page 21
22 PARAMOUNT Trial Primary Endpoint: Significant Reduction of NT-proBNP at 12 Weeks Patients with HFpEF taking ENTRESTO reduced NT-proBNP to a greater extent than valsartan after 12 weeks of therapy. This reduction became evident at 4 weeks and was sustained to 36 weeks, although the between-group difference was no longer significant. There was also a reduction in left atrial size, indicative of reverse left atrial remodeling and improvement in NYHA class in patients randomly assigned to ENTRESTO after 36 weeks compared with those randomly assigned to valsartan. ENTRESTO was well tolerated. HR = 0.77 ( ) P = These findings suggest that ENTRESTO may have beneficial effects in patients with HFpEF and that further testing of this drug may be warranted in patients with this condition. Page 22

23 PARADIGM-HF Trial N Engl J Med 2014; 371:e15September 11, 2014 xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 23
24 Aim of the PARADIGM-HF Trial Prospective Comparison of ARNI with ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure Trial (PARADIGM-HF) LCZ MG DAILY Enalapril 20 MG DAILY Specifically designed to replace current use of ACE inhibitors and angiotensin receptor blockers as the cornerstone of the treatment of heart failure. ARNI: Angiotensin receptor-neprilysin inhibition; ACEI: angiotensin-converting enzyme inhibition xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 24
25 PARADIGM-HF Trial Was Designed to Show Incremental Effect on Cardiovascular Death Primary Endpoint Primary endpoint was cardiovascular death or hospitalization for heart failure, but PARADIGM-HF was designed as a cardiovascular mortality trial. The sample size of the trial was determined by effect on cardiovascular mortality, not the primary endpoint. The Data Monitoring Committee was allowed to stop the trial only for a compelling effect on cardiovascular mortality (in addition to the primary endpoint). Difference in cardiovascular mortality of 15% between LCZ696 and enalapril was prospectively identified as being clinically important. Secondary Endpoints All-cause mortality. Change from baseline in the clinical summary score of the Kansas City Cardiomyopathy Questionnaire (KCCQ) at 8 months. Time to new onset of atrial fibrillation. Time to first occurrence of a protocoldefined decline in renal function. xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 25
26 PARADIGM-HF HR = 0.80 ( ) P = Number needed to treat = 21 HR = 0.80 ( ) P = Number needed to treat = (16.5%) 1117 (26.5%) 558 (13.3%) 914 (21.8%) N Engl J Med Sep 11;371:e15. Page 26
27 PARADIGM-HF 658 (15.6%) 835 (19.8%) 537 (12.8%) 711 (17.0%) N Engl J Med 2014; 371:e15September 11, 2014 Page 27


28 PARADIGM-HF: Cause of Death and Hospitalization Data PARADIGM-HF Cause of Death and Hospitalization Data vs. Current Standard of Care ACEi Enalapril McMurray et al. NEJM 2014;371: ; Packer et al. Circulation 2015;131:54-61 xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 28

29 Change in KCCQ Score at 8 Months LCZ696 Enalapril LCZ696 improved the symptoms and physical limitations of heart failure more than enalapril, p = Page 29

30 PARADIGM-HF: Conclusions In comparison with guideline-recommended doses of an ACE inhibitor, combined inhibition of both the angiotensin receptor and neprilysin was more effective not only in reducing all-cause and cardiovascular mortality, but also in reducing the risks and rates of multiple manifestations of clinical deterioration of surviving patients with heart failure. The effect of LCZ696 to stabilize the course of heart failure is likely to have important ramifications for both quality of life and resource utilization in this disorder. Page 30

31 PARADIGM-HF Trial Circulation. 2015;131: xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx Page 31
 and troponin (reflecting reduced cardiac injury) throughout the trial.")

32 The Effect of LCZ696 on NT-proBNP and BNP LCZ696 Enalapril In contrast, in comparison with enalapril, patients receiving LCZ696 had consistently lower levels of NT-proBNP (reflecting reduced cardiac wall stress) and troponin (reflecting reduced cardiac injury) throughout the trial. The contrasting effects of LCZ696 on the two types of natriuretic peptides represent an important finding, because the levels of the two peptides characteristically parallel each other during the course of heart failure. However, because BNP (but not NT-proBNP) is a substrate for neprilysin, levels of BNP will reflect the action of the drug, whereas levels of NT-proBNP will reflect the effects of the drug on the heart. Page 32
33 Summary PARAMOUNT Trial Patients with HFpEF taking ENTRESTO as compared to valsartan reduced NT-proBNP to a greater extent than valsartan after 12 weeks of therapy. This reduction became evident at 4 weeks and was sustained to 36 weeks, although the between-group difference was no longer significant. There was also a reduction in left atrial size, indicative of reverse left atrial remodeling and improvement in NYHA class in patients randomly assigned to ENTRESTO after 36 weeks compared with those randomly assigned to valsartan. ENTRESTO was well tolerated. These findings suggest that ENTRESTO may have beneficial effects in patients with HFpEF and that further testing of this drug may be warranted in patients with this condition. ENTRESTO is not currently approved for treatment of patients with HFpEF. Page 33 PARADIGM-HF Trial LCZ696 was more effective than enalapril for patients with HFrEF in reducing the risk of CV death and HF hospitalization, reducing the risk of CV death, reducing the risk of HF hospitalization, reducing all-cause mortality, and incrementally improving symptoms and physical limitations. LCZ696 was better tolerated than enalapril and less likely to cause cough, hyperkalemia, or renal impairment. Less likely to be discontinued due to an adverse event. More hypotension, but no increase in discontinuations. Not more likely to cause serious angioedema. However, because BNP (but not NT-proBNP) is a substrate for neprilysin, levels of BNP will reflect the action of the drug, whereas levels of NT-proBNP will reflect the effects of the drug on the heart. ENTRESTO was FDA-approved to treat chronic HF patients with reduced HFrEF.

421-9101 Email:")
34 Contact Linda C. Rogers, PhD, DABCC, FACB Senior Clinical Consultant Siemens Healthcare Scientific & Clinical Affairs Phone: (949) Page 34
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
ARxCH. Annual Review of Changes in Healthcare. Entresto: An Overview for Pharmacists
 Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Entresto: An Overview for Pharmacists David Comshaw, PharmD Candidate 2019 1 Gyen Musgrave, PharmD Candidate 2019 1 Suzanne Surowiec, PharmD, BCACP 1 Jason Guy, PharmD 1 1 University of Findlay College
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2/15/2017. Disclosures. Heart Failure = Big Problem. Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017
 Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Heart Failure Update Reducing Hospitalizations and Improving Patient Outcomes 02/18/2017 Julio A. Barcena, M.D. South Miami Heart Specialists Disclosures I have no relevant commercial relationships to
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Disclosure of Relationships
 Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
Disclosure of Relationships Over the past 12 months Dr Ruilope has served as Consultant and Speakers Bureau member of Astra-Zeneca, Bayer, Daiichi-Sankyo, Menarini, Novartis, Otsuka, Pfizer, Relypsa, Servier
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
ENTRESTO (sacubitril and valsartan) oral tablet
 oral tablet") ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
INIBITORI NEPRILISINA
 INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
INIBITORI NEPRILISINA Marco Canepa, MD, PhD Università degli Studi di Genova Cardiologia, Ospedale Policlinico San Martino IRCCS marco.canepa@unige.it ARNI: ANGIOTENSIN RECEPTOR NEPRILYSIN INHIBITORS
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD
 ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
ANGIOTENSIN RECEPTOR-NEPRILYSIN INHIBITORS IN HEART FAILURE FROM CHD Karen Stout, MD FACC Professor, Medicine/Pediatrics University of Washington Seattle, WA USA No disclosures Case 35 year old man with
REVIEW ARTICLE. Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2
 Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
Sacubitril/valsartan Use for the Hospitalist Mitchell Padkins 1, James Hart 1, Rachel Littrell 2 1 University of Missouri School of Medicine, Columbia, MO 2 Division of Cardiovascular Medicine, Department
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION
 CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
CADTH CANADIAN DRUG EXPERT COMMITTEE FINAL RECOMMENDATION SACUBITRIL/VALSARTAN (Entresto Novartis Pharmaceuticals) Indication: Heart Failure With Reduced Ejection Fraction Recommendation: The Canadian
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed
 Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
Biomarkers in the Age of Sacubitril/Valsa rten: Has the PARADIGM Changed Alan S. Maisel MD FACC Professor of Medicine, University of California, San Diego, Director, CCU and Heart Failure Program San Diego
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients
 Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Rationale and Practical Aspects of Sacubitril- Valsartan and Ivabradine Use in Heart Failure Patients Javed Butler, MD, MPH, MBA Patrick H. Lehan Professor of Medicine Professor of Physiology Chairman,
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO. Dario Leosco Università di Napoli Federico II
 LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD
LCZ696: LA NUOVA RIVOLUZIONE NELLA TERAPIA DELLO SCOMPENSO CARDIACO Dario Leosco Università di Napoli Federico II Projected changes in cardiovascular diseases CVD Deaths Increase 33% CVD DALYS 22% CAD
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
New Trials. Iain Squire. Professor of Cardiovascular Medicine University of Leicester. Chair, BSH
 New Trials Iain Squire Professor of Cardiovascular Medicine University of Leicester Chair, BSH BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: New Trials Speaker: Iain Squire
New Trials Iain Squire Professor of Cardiovascular Medicine University of Leicester Chair, BSH BSH Heart Failure Day for Revalidation and Training 2017 Presentation title: New Trials Speaker: Iain Squire
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
OTE HAR M A. Sacubitril/Valsartan (Entresto ): A New Dual Therapy Approved For Chronic Heart Failure. Vol. 31, Issue 3 December 2015.
: A New Dual Therapy Approved For Chronic Heart Failure. Vol. 31, Issue 3 December 2015.") P HAR M A Vol. 31, Issue 3 December 2015 N OTE Established 1985 Sacubitril/Valsartan (Entresto ): A New Dual Therapy Approved For Chronic Heart Failure Kellen Danley, PharmD Candidate H eart Failure (HF)
P HAR M A Vol. 31, Issue 3 December 2015 N OTE Established 1985 Sacubitril/Valsartan (Entresto ): A New Dual Therapy Approved For Chronic Heart Failure Kellen Danley, PharmD Candidate H eart Failure (HF)
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data,
 Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data, praktische Erfahrungen michael.boehm@uks.eu M. Böhm Innere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
Sacubitril/Valsartan unter der Lupe Subgruppenanalysen, real world data, praktische Erfahrungen michael.boehm@uks.eu M. Böhm Innere Medizin III (Kardiologie / Angiologie / Internistische Intensivmedizin)
New Winners in the World of Heart Failure. Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015
 New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
New Winners in the World of Heart Failure Laura Steffens PharmD Candidate 2016 CICU Presentation August 12, 2015 Jessup 2014 Shaking Things Up 2003: FDA approved eplerenone for the treatment of heart failure
Dr Dinna Soon. Consultant Cardiologist, Department of Cardiology. GP symposium 2 April 2016
 Dr Dinna Soon Consultant Cardiologist, Department of Cardiology GP symposium 2 April 2016 Case presentation 76 years old male, chronic smoker, hypertension, previous MI 3/7 SOB and chest tightness BP
Dr Dinna Soon Consultant Cardiologist, Department of Cardiology GP symposium 2 April 2016 Case presentation 76 years old male, chronic smoker, hypertension, previous MI 3/7 SOB and chest tightness BP
6/6/17. Heart Failure and Natriuretic Peptides. Learning objectives
 Heart Failure and Natriuretic Peptides Maria-Magdalena Patru, MD, PhD Director, Medical and Scientific Affairs This promotional educational activity is brought to you by Ortho-Clinical Diagnostics, Inc.
Heart Failure and Natriuretic Peptides Maria-Magdalena Patru, MD, PhD Director, Medical and Scientific Affairs This promotional educational activity is brought to you by Ortho-Clinical Diagnostics, Inc.
Practical considerations for the use of ARNI in CHF: clinical cases. J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece
 Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Practical considerations for the use of ARNI in CHF: clinical cases J. Parissis, Heart Failure Clinic, University of Athens, Athens, Greece Disclosures: Research grants and honoraria for lectures from
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Ejection Fraction in Patients With Chronic Heart Failure. Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction
 Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Diastolic Heart Failure or Heart Failure with Preserved Ejection Fraction Keith Miller MD Diastolic Heart Failure Risk Factors Common Risk Factors Aging Female gender Obesity Hypertension Diabetes mellitus
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
The clinical value of natriuretic peptide testing in heart failure
 The clinical value of natriuretic peptide testing in heart failure James L. Januzzi, Jr, MD, FACC, FESC Associate Professor of Medicine Harvard Medical School Roman W. DeSanctis Endowed Clinical Scholar
The clinical value of natriuretic peptide testing in heart failure James L. Januzzi, Jr, MD, FACC, FESC Associate Professor of Medicine Harvard Medical School Roman W. DeSanctis Endowed Clinical Scholar
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Heart Failure Update. Chim Lang
 Heart Failure Update Chim Lang Heart Failure Patient s Journey Acute Treat and stabilize Initiate monitoring Plan interventions Chronic Optimize drug and device therapy Manage Co-morbidities Subacute
Heart Failure Update Chim Lang Heart Failure Patient s Journey Acute Treat and stabilize Initiate monitoring Plan interventions Chronic Optimize drug and device therapy Manage Co-morbidities Subacute
HFpEF 2016 : Comorbidities and Outcomes
 HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
HFpEF 2016 : Comorbidities and Outcomes Christopher M. O Connor, MD, FACC CEO and Executive Director, Inova Heart and Vascular Institute Professor of Medicine, Duke University Editor in Chief, JACC: Heart
Heart Failure in Women: Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre
 Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
Heart Failure in Women: More than EF? Dr Goh Ping Ping Cardiologist Asian Heart & Vascular Centre Overview Review pathophysiology as it relates to diagnosis and management Rational approach to workup:
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association
 Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association We combed through both guidelines and summarized 3 recommendations
Role of Biomarkers for the Prevention, Assessment, and Management of Heart Failure: A Scientific Statement From the American Heart Association We combed through both guidelines and summarized 3 recommendations
2017 ACC/AHA/HFSA HF guidelines. Advances in the Use of Biomarkers in Heart Failure Patients. Outline
 Advances in the Use of Biomarkers in Heart Failure Patients Lori B. Daniels, MD, MAS, FACC, FAHA Professor of Medicine Director, Cardiovascular Intensive Care Unit Sulpizio Cardiovascular Center UC San
Advances in the Use of Biomarkers in Heart Failure Patients Lori B. Daniels, MD, MAS, FACC, FAHA Professor of Medicine Director, Cardiovascular Intensive Care Unit Sulpizio Cardiovascular Center UC San
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Update in Cardiology What s Hot in 2017?
 Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
Update in Cardiology What s Hot in 2017? Mark R. Milunski, MD, FACC, FACP Chief, Cardiology Section Orlando Veterans Affairs Medical Center Associate Professor of Medicine University of Central Florida
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs?
 How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
How Do You Mend a Broken Heart: The New Agents to Treat HF Paradigm Shift or Just the Same Old Drugs? Gregg C. Fonarow, MD FACC, FAHA, FHFSA Co-Chief UCLA Division of Cardiology Director, Ahmanson-UCLA
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
ECG in CRT patients & novel HF therapies. Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος
 ECG in CRT patients & novel HF therapies Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou has received grants from Medtronic Is identification
ECG in CRT patients & novel HF therapies Δημήτριος M. Κωνσταντίνου Ειδικός Καρδιολόγος, MD, MSc, PhD, CCDS Πανεπιστημιακός Υπότροφος Dr. Konstantinou has received grants from Medtronic Is identification
Summary 1. Comparative effectiveness
 Cost-effectiveness of Sacubitril/Valsartan (Entresto) for the treatment of symptomatic chronic heart failure in adult patients with reduced ejection fraction. The NCPE has issued a recommendation regarding
Cost-effectiveness of Sacubitril/Valsartan (Entresto) for the treatment of symptomatic chronic heart failure in adult patients with reduced ejection fraction. The NCPE has issued a recommendation regarding
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Use of Sacubitril/Valsartan in Heart Failure
 Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
Use of Sacubitril/Valsartan in Heart Failure & the PARADIGM-HF trial Sarah Mackenzie, PharmD student, University of Toronto Presentation Outline Overview of: Entresto PARADIGM-HF trial Critical Appraisal
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers
 Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION
 THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
THE PROPER APPROACH TO DIAGNOSING HEART FAILURE WITH PRESERVED EJECTION FRACTION James C. Fang, MD, FACC Professor and Chief Cardiovascular Division University of Utah School of Medicine Disclosures Data
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long. Case Study 2
 HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
HeFSSA Practitioners Program 2017 Theme The Patient Journey: Feel Good and Live Long Case Study 2 HEART FAILURE WITH MID-RANGE EJECTION FRACTION TREATMENT OPTIONS CLINICAL CASE MEDICAL HISTORY 59-year-old
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Sacubitril/valsartan: a cardiovascular drug with pluripotential actions
 Editorial Sacubitril/valsartan: a cardiovascular drug with pluripotential actions Steven G. Chrysant 1, George S. Chrysant 2 1 University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA; 2 INTEGRIS
Editorial Sacubitril/valsartan: a cardiovascular drug with pluripotential actions Steven G. Chrysant 1, George S. Chrysant 2 1 University of Oklahoma Health Sciences Center, Oklahoma City, OK, USA; 2 INTEGRIS
HF-Preserved Ejection Fraction
 HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
HF-Preserved Ejection Fraction Justin A. Ezekowitz, MBBCh MSc FRCPC FACC FESC FAHA Associate Professor, University of Alberta Co-Director, Canadian VIGOUR Centre Cardiologist, Mazankowski Alberta Heart
Biomarker-guided HF: What have we learned (so far)?
?") Biomarker-guided HF: What have we learned (so far)? James L. Januzzi, Jr, MD, FACC, FESC Associate Professor of Medicine Harvard Medical School Director, Cardiac ICU Massachusetts General Hospital DECLARATION
Biomarker-guided HF: What have we learned (so far)? James L. Januzzi, Jr, MD, FACC, FESC Associate Professor of Medicine Harvard Medical School Director, Cardiac ICU Massachusetts General Hospital DECLARATION
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Natriuretic Peptides The Cardiologists View. Christopher defilippi, MD University of Maryland Baltimore, MD, USA
 Natriuretic Peptides The Cardiologists View Christopher defilippi, MD University of Maryland Baltimore, MD, USA Disclosures Research support: Alere, BG Medicine, Critical Diagnostics, Roche Diagnostics,
Natriuretic Peptides The Cardiologists View Christopher defilippi, MD University of Maryland Baltimore, MD, USA Disclosures Research support: Alere, BG Medicine, Critical Diagnostics, Roche Diagnostics,
A new class of drugs for systolic heart failure: The PARADIGM-HF study
 INTERPRETING KEY TRIALS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will describe the mechanism and use of angiotensin receptor-neprilysin inhibitors in heart failure MARWA A. SABE, MD, MPH Department of
INTERPRETING KEY TRIALS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will describe the mechanism and use of angiotensin receptor-neprilysin inhibitors in heart failure MARWA A. SABE, MD, MPH Department of
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Heart Failure. GP Update Refresher 18 th January 2018
 GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
GP Update Refresher 18 th January 2018 Heart Failure Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President of British
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand
 Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Pravin Manga Division of Cardiology Department of Medicine University of Witwatersrand Overview Definition Epidemiology Biomarkers Treatment Clinical Heart Failure: Syndrome in which patients have typical
Clinical Trial Results Website
 Sponsor Novartis Pharmaceuticals Corporation Generic Drug Name (sacubitril/valsartan) Trial Indication(s) Chronic heart failure (CHF) with reduced ejection fraction (EF) Protocol Number CB2314 Protocol
Sponsor Novartis Pharmaceuticals Corporation Generic Drug Name (sacubitril/valsartan) Trial Indication(s) Chronic heart failure (CHF) with reduced ejection fraction (EF) Protocol Number CB2314 Protocol
Behandeling van Hartfalen: over 5 jaar
 Behandeling van Hartfalen: over 5 jaar Adriaan Voors, cardioloog UMCG Over 5 jaar Heart Failure Treatment in 5 Years HFrEF: best evidence, biggest pipeline Entresto Omcamtiv LVAD: destination therapy HFrEF:
Behandeling van Hartfalen: over 5 jaar Adriaan Voors, cardioloog UMCG Over 5 jaar Heart Failure Treatment in 5 Years HFrEF: best evidence, biggest pipeline Entresto Omcamtiv LVAD: destination therapy HFrEF:
New horizons in HF: potential of new drugs
 New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
New horizons in HF: potential of new drugs Marc A. Pfeffer, MD, PhD Dzau Professor of Medicine, Harvard Medical School Cardiovascular Division, Brigham & Women s Hospital Boston, Massachusetts FINANCIAL
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care. Md. Shahidul Islam, M.D., Ph.D
 ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care Md. Shahidul Islam, M.D., Ph.D shaisl@me.com 2 3 Circulating Biomarkers in Heart Failure. Berezin AE. Adv. Exp. Med.
ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care Md. Shahidul Islam, M.D., Ph.D shaisl@me.com 2 3 Circulating Biomarkers in Heart Failure. Berezin AE. Adv. Exp. Med.
6/29/2017. Role of Biomarkers in the Management of Heart Failure Patients. What s New in Biomarkers for HF Patients?
 What s New in Biomarkers for HF Patients? Role of Biomarkers in the Management of Heart Failure Patients Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Cardiovascular Intensive Care Unit
What s New in Biomarkers for HF Patients? Role of Biomarkers in the Management of Heart Failure Patients Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Cardiovascular Intensive Care Unit
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC
 Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an