Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough?
|
|
|
- Rodney Holt
- 6 years ago
- Views:
Transcription
1 Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital Detroit, Michigan Supplemental oxygen ± endotracheal intubation and mechanical ventilation Central venous and arterial catheterization Sedation and/or paralysis (if intubated) 8-12 mm Hg CVP <8 mm Hg Crystalloid Colloid Intubation and Mechanical Ventilation =65 and =9 mm Hg MAP ScvO 2 <65 mm Hg >9 mm Hg <7% Vasopressor or Nitroglycerin Transfusion of red cells to hematocrit =3% =7% <7% =7% Dobutamine & Digoxin Goals achieved Yes No Hospital admission 1


2 Communication Avoids Misunderstanding and Prevents Problems Inflammatory Mediators Produce Cardiovascular Insufficiency Increased Metabolic Demands: Fever, Tachypnea Hypovolemia,Vasodilation & Myocardial Depression Microvascular Alterations: Impaired Tissue Oxygen Utilization Cytopathic Tissue Hypoxia Fink, Crit Care Clin, 22 2
3 The Purpose of Resuscitation Perhaps Forgotten VO2 Delivery Dependent Endpoints and Tools Global tissue hypoxia Critical DO 2 Delivery Independent Optimum region DO 2 The Problem Uniformity of terminology Uniformity of goals Under-resuscitation Over-resuscitation Multiple outcome measures in clinical trials How do we solve the problem? Substrates Goal Directed Optimization of Cardiac Function O 2 ATP Glucose Endpoints of Resuscitation SvO 2 Lactate - Stress - Pain - Hyperthermia - Shivering - Work of breathing Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output (a-v)co 2 Microcirculation Happy Cell Base Deficit phi Mediators DO 2 3
4 Macro Endpoints Delivery Dependent Delivery Independent VO2 Physical Exam Heart Rate Blood Pressure Shock Index Urine Output CVP/PCWP Global tissue hypoxia Optimum region Critical DO 2 DO 2 Substrates Goal Directed O 2 ATP Glucose Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure 4
5 Effects of perfusion pressure on tissue perfusion in septic shock OBJECTIVE: To measure the effects of increasing MAP on systemic O2 metabolism and regional tissue perfusion in septic shock. DESIGN: Prospective study. SETTING: MICU and SICU patients in a tertiary care teaching hospital. PATIENTS: 1 patients with septic shock requiring pressor agents to maintain a MAP > 6 mm Hg after fluid resuscitation to a PAOP > 12 mm Hg. LeDoux, Crit Care Med, 2 Effects of perfusion pressure on tissue perfusion in septic shock INTERVENTIONS: Norepinephrine was titrated to MAPs of 65, 75, and 85 mm Hg in 1 patients with septic shock. Cardiac Index Lactate A-Gastric pco2 Urine Output 65 mmhg 4.7+/-.5 L/min/m2 3.1+/-.9 meq/l 13+/-3 mm Hg (1.7+/-.4 kpa) 49+/-18 ml/hr 85 mmhg 5.5+/-.6 L/min/m2 (p <.3) 3.+/-.9 meq/l (NS) 16+/-3 at 85 mm Hg (2.1+/-.4 kpa) (NS) 43+/-13 ml/h (NS) LeDoux, Crit Care Med, 2 5

6 Effects of perfusion pressure on tissue perfusion in septic shock CONCLUSIONS: Increasing the MAP from 65 mm Hg to 85 mm Hg with norepinephrine does not significantly affect systemic oxygen metabolism skin microcirculatory blood flow urine output splanchnic perfusion. LeDoux, Crit Care Med, 2 Radial artery pressure monitoring underestimates central arterial pressure during vasopressor therapy in critically ill surgical patients Critical Care Medicine 1998;26: Todd Dorman, MD, FCCM; Michael J. Breslow, MD, FCCM; Pamela A. Lipsett, MD; Jeffrey M. Rosenberg, MD, PhD; Jeffrey R. Balser, MD, PhD; Yaniv Almog, MD; Brian A. Rosenfeld, MD, FCCM Radial artery pressure underestimates central pressure in hypotensive septic patients receiving high-dose vasopressor therapy. The higher mean femoral arterial pressures: immediate reduction in norepinephrine infusions in 11 of the 14 patients. Clinical management, based on radial pressures, may lead to excessive vasopressor administration. 6
7 7
8 6 58% 54% Mortality (%) 4 2 2% 37% No Vasopressor No Vasopressor to Low Dose Vasopressor No Vasopressor to High Dose Vasopressor Low Dose to High Dose Vasopressor 15% % Receiving Vasopressors hours 6-72 hours -72 hours No Corticosteroids 8
 - Coronary Perfusion Pressure An ICU Therapy Forever Changed A restrictive strategy of red-cell transfusion is at least as effective as and possibly superior to a liberal transfusion")
9 Substrates Goal Directed O 2 ATP Glucose DO 2 - PaO 2 - Hemoglobin - Cardiac Output Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure An ICU Therapy Forever Changed A restrictive strategy of red-cell transfusion is at least as effective as and possibly superior to a liberal transfusion strategy 9
10 Stop An International Crisis Transfusions do make a difference in shock or global tissue hypoxia states. Abuse to the clinician after giving blood Conservative management during the convalescent phase. Hemodilution After Volume Control Treatment * * * Control Treatment hours 6-72 hours -72 hours 2 15 Baseline 3 hours 6 hours 7-72 hours 3.6 Liters More Fluid 6 ml No difference in blood transfused over 72 hours between groups ml -72 hours 1

11 Hemodynamic Phases of Sepsis Transfusion Decisions Depend on the Clinical Sate Delivery Dependent Delivery Independent S OER Lactate S OER Lactate S OER Lactate DO 2crit DO 2 Even SvO 2 is a combination of various tissue beds. The coronary circulation is at the highest risks. 11
12 Hemodynamic Phases of Sepsis Transfusion Decisions Depend on the Clinical Sate Delivery Dependent Delivery Independent S OER Lactate S OER Lactate S OER Lactate DO 2crit DO 2 Transfusion Decisions Depend on the Clinical Sate Delivery Dependent Delivery Independent Dietrich, Critical Care, Med, 2 S OER Lactate Marik, S JAMA, 2 Herbert, NEJM, 21 OER Vincent, JAMA, 22 Lactate DO 2crit DO 2 12
13 Transfusion Studies EGDT, NEJM, 22 Hebert, NEJM, 1999 Vincent, JAMA, 22 Marik, JAMA, 1993 Setting ED ICU ICU ICU Time (hours) <1 24 hours Over 2 weeks Up to 48 hours Age Hemoglobin * 9.9 Lactate (mm/l) ± ± SvO 2 (%) CVP (mmhg) Resuscitated Cardiac Index Transfusion Studies EGDT, NEJM, 22 Hebert, NEJM, 1999 Vincent, JAMA, 22 Marik, JAMA, 1993 APACHE 2.4± ± ± ± Mortality And Endpoints % 22.2 vs. 28.1% (.5) % ICU 22-17% 28 day Decreased phi In shock or global tissue hypoxia? 1% 16-13% 2-23% Excluding dialysis patients, patients likely to die in 24 hours and patients in established septic shock (systolic blood pressure <9 mmhg). 13
 - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output 14")
14 Substrates Goal Directed O 2 ATP Glucose - Stress - Pain - Hyperthermia - Shivering - Work of breathing Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output 14


15 ScvO 2 SvO2 7-75% - + Stress Pain Hyperthermia Shivering Work of breathing DO 2 PaO2 Hgb Cardiac Output Using Metabolic Endpoints SvO 2 15
 Survivors Nonsurvivors %Survival 27 1 21 6 77.8 3 19 13.")
16 Lactate and Outcome (Mizock, Dis Mon, 1989) (Weil, Circulation, 197) Survivors Non-survivors Lactate (mm/l) Clearance <24 hrs hrs >48 hrs N = Time (hrs) Survivors Nonsurvivors %Survival (Abramson and Scalea, J Trauma, 1993) 16
 ED Length of Stay (hrs) No clearance < mm/l/hr Intermediate clearance -1 mm/l/hr High clearance >1 mm/l/hr Lactate (mm/l) 14 12 1 8 6 4 2 14 N = 114 No")
17 Crit Care Med 24 Vol. 32, No. 8 Lactate (ED Admission - ED Discharge) ED Length of Stay (hrs) No clearance < mm/l/hr Intermediate clearance -1 mm/l/hr High clearance >1 mm/l/hr Lactate (mm/l) N = 114 No Clearance High Clearance ED Admission ED Discharge Crit Care Med 24 Vol. 32, No. 8 Lactate (ED Admission - ED Discharge) ED Length of Stay (hrs) Lactate Clearance % Quartiles of Lactate Clearance N =
18 Early Lactate Clearance 11 No Clearance 1 Intermediate Clearance High Clearance 9 MODS Time (hr) p<.5 Mortality (%) No Clearance Intermediate Clearance 12 High Clearance % Lactate Clearance Quartiles and mean Biomarker Levels over 72 Hours Caspase-3 (ng/ml) Lactate Clearance Quartiles 18
19 % Lactate Clearance Quartiles and mean Biomarker Levels over 72 Hours IL-8 (pg/ml) Lactate Clearance Gropus 1 Tumor necrosis factor a (pg/ml) Caspase-3 (ng/ml) Substrates Goal Directed O 2 ATP Glucose - Stress - Pain - Hyperthermia - Shivering - Work of breathing Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output Microcirculation Crit Care Med 24 Vol. 32, No. 9 19
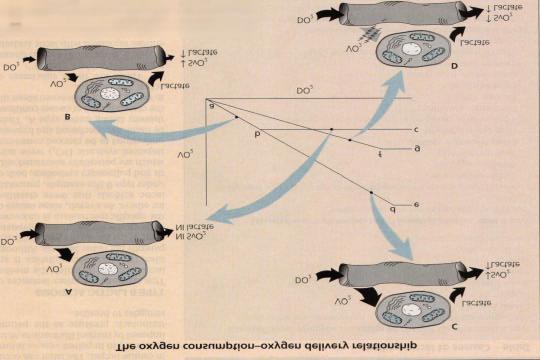
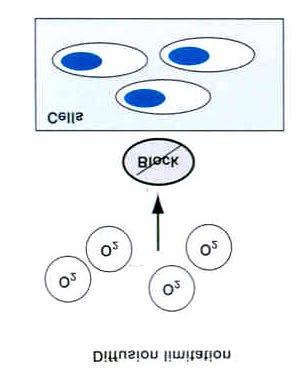
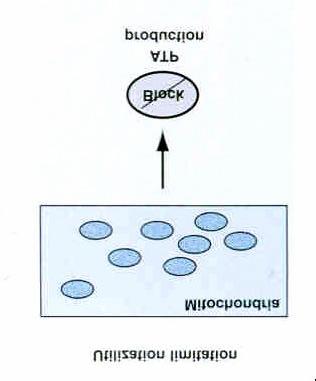
20 The oxygen consumption-delivery relationship Microcirculatory Dysfunction 2




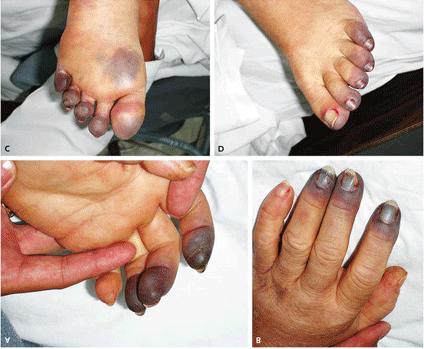
21 Lancet 22 Orthogonal polarization spectral (OPS) imaging allows visualisationof the microcirculation. Assessing microcirculatory flow in septic-shock patients who had a MAP > 6 mm Hg and CVP > 12 mm Hg. The infusion of.5 mg of nitroglycerin resulted in a marked increase in microvascular flow on OPS imaging. Improved recruitment of the microcirculation could be a new resuscitation endpoint in septic shock. Micro-Circulatory Defects Vascular occlusion and vasopressor use Ischemia and Cellular Hypoxia 21
22 Increasing O2 Consumption Bihari, NEJM, minute infusion of a vasodilator, prostacyclin (5 ng/kg/min in 27 critically ill patients with acute respiratory failure and measured: O2 delivery and uptake to tissues Extraction ratio (uptake/delivery) In the survivors: O2 extraction ratio fell increased. In the patients who died: O2 extraction ratio rose did not change. Increasing O2 Consumption Bihari, NEJM, 1987 Conclusion: (an underappreciated endpoint) Substantial O2 debt or cryptic shock in patients who subsequently die. Inadequate tissue oxygenation may be difficult to recognize Important mechanism in the development of irreversible multiple organ failure. 22
 Acute myocardial infarction (Rady, Chest, 1993) Heart transplantation (Mancini, J Clin Monit, 1991) Liver transplantation (Chest, 1992) ARDS (Appel, Chest, 1992) 23")
23 Oxygen Debt: To Pay or Not to Pay Direct Association of Decreased Increased Mortality Cardiac arrest (Rivers, Chest, 1994) Trauma (Moore, J of Trauma, 1992) Sepsis (Tuchschmidt, Chest, 1991) Acute myocardial infarction (Rady, Chest, 1993) Heart transplantation (Mancini, J Clin Monit, 1991) Liver transplantation (Chest, 1992) ARDS (Appel, Chest, 1992) 23
24 Substrates Goal Directed O 2 ATP Glucose Endpoints of Resuscitation SvO 2 Lactate - Stress - Pain - Hyperthermia - Shivering - Work of breathing Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output (a-v)co 2 Microcirculation Happy Cell Base Deficit phi Mediators DO 2 Metabolic Endpoints of Resuscitation Delivery Dependent Delivery Independent VO2 ScvO 2 (a-v)pco 2 Gastric Tonometry Sublingual Cap. Base Deficit Lactate Global tissue hypoxia O 2 extraction Optimum region Pulmonary Artery Catheter in the ICU Critical DO 2 DO 2 24
25 (a-v) pco 2 Gradient < 5 mmhg PaCO 2 but PvCO 2 in circulatory failure and low flow states (Mecher, Crit Care Med, 199) PcvCO 2 PmvCO2 Inverse relationship between CI and (a-v) pco 2 (Ducey, Crit Care Med, 1992), (Durkin, J Crit Care, 1993) (Rackow, Crit Care Med, 1994), (Teboul, Crit Care Med, 1998) PaCO 2 (a-v) pco 2 increases mortality (Bakker, Chest, 1992) (a-v) pco 2 and Cardiac Index CI pac (L/min/m 2 ) Mixed venous N = 83 CI pac (L/min/m 2 ) Central venous (a-mv)pco 2 (mmhg) (a-cv)pco 2 (mmhg) ln(ci) = (a-mv)pCO 2 r 2 =.87 ln(ci) = (a-cv)pCO 2 r 2 =.9 (Cuschieri, Rivers and Donnino, Int Care Med, 25) 25


26 Sublingual Capnometry Weil, Crit Care Med 1999; 27: healthy volunteers without clinical signs of shock physical signs of circulatory shock PSL CO 2 mm Hg / / /- 24 Lactate (mm/l) < 2.5 >2.5 N Died from shock Survivors Initial PSL CO 2 mm Hg Correlation with lactate (r 2 =.84; p <.1) N When P SL CO ( 2 ) > 7 mm Hg, its positive predictive value for the presence of physical signs of circulatory shock was 1.. When it was <7 mm Hg, it predicted survival with a predictive value of
27 Base Deficit Amount of base required to titrate 1L blood to normal ph. Indicator of volume deficit. Guide to resuscitation in trauma patient.(davis, J Trauma, 1988) Affected by administration of bicarbonate, temp, ETOH, heparin. Can I use Base Deficit or Anion Gap? Lactate Range mmol/l 4. to to 9.9 >1 Serum HCO3>22 and A.G. < % 8.3% % Wira and Rivers, Crit Care Med, 25 27


28 Crit Care Med, 27 Moderate Global Tissue Hypoxia: Lactate < 4 and >2 mmole/liter and ScvO2 < 7% Resuscitated: Lactate < 2 mmole /liter and ScvO2 > 7% Severe Global Tissue Hypoxia: Lactate > 4 mmole/liter and ScvO2 < 7%) 28
 8 6 4 2 3 6 12 24 36 48 6 72 Hours after the start of treatment Lactate > 4 mm/l and ScvO2 <7% Lactate")
 5 TNF-α (pg/ml) 125 1 75 25 5 25 3 6 12 24 36 48 6 72 Hours after the start of treatment 3 6 12 24 36 48 6")
 7 6 5 4 3 2 1 3 6 12 24 36 48 6 72 Hours after the start of treatment 29")
29 IL-8 murine (pg/ml) EGDT Standard Therapy Hours after the start of treatment Il-8 (pg/dl) Hours after the start of treatment Lactate > 4 mm/l and ScvO2 <7% Lactate > 2 and < 4 mm/l and ScvO2 <7% Lactate < 2 mm/l and ScvO2 > 7% Chest, 25 1 Tumor Necrosis Factor TNF- α (pg/ml) 5 TNF-α (pg/ml) Hours after the start of treatment Hours after the start of treatment 5 4 Caspase Caspase-3 (ng/ml) Hours after the start of treatment Caspase-3 (ng/ml) Hours after the start of treatment 29
 3 2 ICAM-1 (ng/ml) 4 3 2 1 1 3 6 12 24 36 48 6 72")
30 IL-1 receptor Antagonist 15 EGDT Control Lactate>4 and ScvO2<7% Lactate>2 and ScvO 2<7% Lactate<2 and ScvO 2 >7% IL-1ra (pg/ml) IL-1ra (ng/ml) Hours after the start of treatment Hours after the start of treatment 5 Intracellular Adhesion Molecule ICAM-1 (ng/ml) 3 2 ICAM-1 (ng/ml) Hours after the start of treatment Hours after the start of treatment 3
31 31
32 Optimization Trials A Closer Look Late Early Mortality (Boyd, New Horiz, 1996) (Kern, Crit Care Med, 22) 32
33 Substrates Goal Directed O 2 ATP Glucose Endpoints of Resuscitation SvO 2 Lactate - Stress - Pain - Hyperthermia - Shivering - Work of breathing Hemodynamic - Preload (CVP, PCWP) - Afterload (MAP, SVR) - Contractility (SV) - Heart Rate (BPM) - Shock Index (HR/SBP) - Coronary Perfusion Pressure DO 2 - PaO 2 - Hemoglobin - Cardiac Output (a-v)co 2 Microcirculation Happy Cell Base Deficit phi Mediators DO 2 33
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
DO 2 > VO 2. The amount of oxygen delivered is a product of cardiac output (L/min) and the amount of oxygen in the arterial blood (ml/dl).
 and the amount of oxygen in the arterial blood (ml/dl).") Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
An early warning indicator of tissue hypoxia.
 An early warning indicator of tissue hypoxia. Continuous ScvO2 monitoring with the PreSep oximetry catheter Are your vital signs telling you everything? Valuable time may be lost before traditional vital
An early warning indicator of tissue hypoxia. Continuous ScvO2 monitoring with the PreSep oximetry catheter Are your vital signs telling you everything? Valuable time may be lost before traditional vital
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
PiCCO based algorithms
 European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Pediatric Septic Shock. Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee
 Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
Pediatric Septic Shock Geoffrey M. Fleming M.D. Division of Pediatric Critical Care Vanderbilt University School of Medicine Nashville, Tennessee Case 4 year old male with a history of gastroschesis repaired
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! seminaires iris. Daniel De Backer
 Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update
 Special Articles Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update Steven M. Hollenberg, MD; Tom S. Ahrens, DNS, RN, CCRN, CS; Djillali Annane, MD, PhD; Mark E. Astiz,
Special Articles Practice parameters for hemodynamic support of sepsis in adult patients: 2004 update Steven M. Hollenberg, MD; Tom S. Ahrens, DNS, RN, CCRN, CS; Djillali Annane, MD, PhD; Mark E. Astiz,
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Hemodynamic Support of Sepsis
 Practice Parameters for Hemodynamic Support of Sepsis in Adult Patients Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the March 1999 issue of Critical Care Medicine
Practice Parameters for Hemodynamic Support of Sepsis in Adult Patients Copyright by the SOCIETY OF CRITICAL CARE MEDICINE These guidelines can also be found in the March 1999 issue of Critical Care Medicine
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Cardiopulmonary System
 Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Sepsis and septic shock
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
The Concept of Early Goal-Directed Therapy in Sepsis Syndrome
 Med. J. Cairo Univ., Vol. 79, No. 2, March 223-232, 2011 www.medicaljournalofcairouniversity.com The Concept of Early Goal-Directed Therapy in Sepsis Syndrome HAZEM EL-AKABAWY, M.D.; MERVAT KHALAF, M.D.;
Med. J. Cairo Univ., Vol. 79, No. 2, March 223-232, 2011 www.medicaljournalofcairouniversity.com The Concept of Early Goal-Directed Therapy in Sepsis Syndrome HAZEM EL-AKABAWY, M.D.; MERVAT KHALAF, M.D.;
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients
 Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients Presenters Dr. Nathan Shapiro Dr. Laurence Dubensky Evidence Based Approaches
Sepsis Learning Collaborative: Evidence-based Approaches to Sepsis Resuscitation Sepsis Resuscitation in Medically Complex Patients Presenters Dr. Nathan Shapiro Dr. Laurence Dubensky Evidence Based Approaches
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
I n 2001, Rivers et published a landmark
 828 REVIEW Early goal-directed therapy: a UK perspective A D Reuben, A V Appelboam, l Higginson, J G Lloyd, N I Shapiro... The surviving sepsis campaign developed guidelines in 2003 that were designed
828 REVIEW Early goal-directed therapy: a UK perspective A D Reuben, A V Appelboam, l Higginson, J G Lloyd, N I Shapiro... The surviving sepsis campaign developed guidelines in 2003 that were designed
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Clinical relevance of perioperative ScvO 2 monitoring
 Risk adapted peri operative haemodynamic management Clinical relevance of perioperative ScvO 2 monitoring Euroanaesthesia 2007 Meeting Munich, Germany, 9.-12. June 2007 Claus-Georg KRENN Dept. of Anaesthesia
Risk adapted peri operative haemodynamic management Clinical relevance of perioperative ScvO 2 monitoring Euroanaesthesia 2007 Meeting Munich, Germany, 9.-12. June 2007 Claus-Georg KRENN Dept. of Anaesthesia
Making vasopressors safer
 Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
Making vasopressors safer Requirements for safe vaspressor use In an ideal world 1. Knowledge of what constitutes optimal vasopressor dosing 2. A culture of cautiousness regarding vasopressors What do
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Useful diagnostic measures: chest x ray to check pulmonary edema, ECG and ECHO to detect cardiac abnormalities (1).
.") Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents
Cardiogenic shock Etiology The most common cause of cardiogenic shock is LV dysfunction and necrosis as a result of acute myocardial infarction (AMI) (1). Acute valvular insufficiency or stenosis prevents