Polytrauma and Critical Care
|
|
|
- Meghan Sharon Bates
- 6 years ago
- Views:
Transcription
1 Polytrauma and Critical Care Dr Mike Brunner M.B.B.S., F.R.C.A. Consultant in Anaesthesia and Intensive Care Medicine Northwick Park and St Mark s s Hospital Harrow England


2 My Hospital

3 My Football Team

4 My Favourite Place




5 Trauma - Introduction
6 Introduction Trauma is the leading cause of death in the first 4 decades of life in most European countries. Third cause of death in all age groups (in 2020 may be second cause of death) 3.8 million deaths / year worldwide 312 million injured / year worldwide 3 patients permanently disabled / death
7 Lost life years Trauma Cancer Cardio vascular Claire Merrick et. al. Prehospital Trauma Life Support, Mosby, 2003
8 Introduction 1 in 3 deaths occurred in hospital as a result of an injury which could have been prevented (Royal College of Surgeons of England, 1988)
9 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Vehicle Environment
10 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Vehicle Environment
11 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts Vehicle Environment
12 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Environment
13 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Antilock brakes Environment
14 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Antilock brakes Air bags deploys Environment
15 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Antilock brakes Air bags deploys Environment Speed limits
16 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Antilock brakes Air bags deploys Environment Speed limits Impact-absorbing absorbing barriers
17 Motor vehicle accidents prevention PREEVENT EVENT POSTEVENT Host Avoid alcohol consumption Use of safety belts First aid by bystanders Vehicle Antilock brakes Air bags deploys Environment Speed limits Impact-absorbing absorbing barriers Emergency medical service (access to trauma system)

18 Prevention Page last updated at 10:43 GMT, Thursday, 25 September :43 3 UK Road deaths fall to record lows Road deaths have fallen to their lowest level since records began in 1928, according to figures published by the Department for Transport. Last year a total of 2,946 people died - a 7% reduction on the previous year when 3,172 died.
19 Introduction 1 in 3 deaths occurred in hospital as a result of an injury which could have been prevented Deaths occur due to failure of simple management in the early stages ( GOLDEN( HOUR ), rather than a failure of complex definitive treatment (Royal College of surgeons of England, 1988)
20 Trimodal Death Distribution Number of Deaths Immediate Deaths Early Deaths Hours Time After Injury Late Deaths Weeks
21 Trimodal Death Distribution Number of Deaths Early Deaths Hours Time After Injury Weeks

22
23 Plane crash in Nebraska,, killed, 4 injured
24 When I can provide better care in the field with limited resources than what my children and I received at the primary care facility there is something wrong with the system and the system has to be changed. ~ James Styner, MD, FACS ~ 1977
25 ATLS

26 These guidelines seek to set achievable standards for trauma treatment services which could realistically be made available to almost every injured person in the world. World Health Organization 2004
27 ATLS Concept ABCDE-approach to evaluation / treatment
28 ATLS Concept A B C D E Airway Breathing Circulation Disability Expose
29 ATLS Concept ABCDE-approach to evaluation / treatment Treat greatest threat to life first Definitive diagnosis not immediately important Time is of the essence Do no further harm
30 ATLS - Initial Assessment / Management Primary Survey Definitive Care Resuscitation Re-evaluation evaluation Detailed Secondary Survey Re-evaluation evaluation
31 Assessing the patient in 10 seconds Identify yourself Ask the patient his / her name Ask the patient what happened
32 Appropriate response confirms A B Patent airway Breathing C D Clear thinking
33 Beware Continue to observe and have a high index of suspicion Especially if patient has - Maxillofacial injury - Soft-tissue injury of neck - Facial or neck burns - Hoarse voice (Laryngeal injury / tracheal burn)
34 If no response, proceed with rapid primary survey
35 Primary Survey A B C D E Airway: C-spine protection Breathing: Oxygenation Circulation: Stop the Bleeding! Disability: Neuro Status Expose: Environment & Body Temp
36 A Airway Simple management manoeuvres Suction Chin lift Jaw thrust Use simple equipment to help
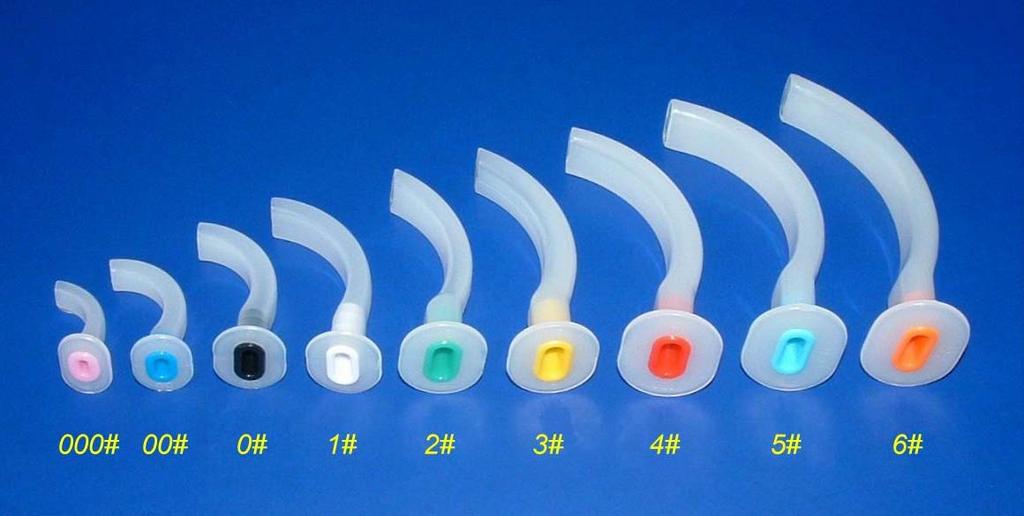
37 A Airway

38 A Airway LMA i-gel LMA


39 A Airway
40 A Airway Simple management manoeuvres Suction Chin lift Jaw thrust Definitive airway: Cuffed tube in trachea
41 A Airway (important message)

42 A Airway The reported incidence of cervical spine injury in the setting of major trauma is 1.5% 4%. Emerg Med J 2004;21: Anesth Analg 1991;73: Can J Anaesth 1990;37: Arch Surg 1994;129: Ann Emerg Med 1998;32:461 9.

43 Protecting the spine Immobilize entire patient on long spine board


44 Protecting the spine Apply semirigid cervical collar/head block
45
46
47 Manual in-line stabilisation (MILS)
48
49
50
51
52

53 Intubating Laryngeal Mask Airway (IMLA)
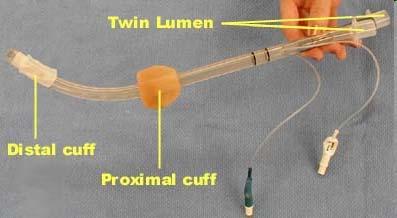
54 Combitube

55 Combitube 98% 2%
56 Combitube Inflation of the large pharyngeal cuff of the Combitube exerts pressure against the vertebral bodies of C2, C3 and/or C4, depending on placement.
57 Gold Standard airway management for patient with potential C-spine C injury requiring immediate and/or urgent airway control rapid sequence induction of anaesthesia orotracheal intubation with cricoid pressure manual in-line immobilization of the head and neck Precise cervical spine in-line immobilization should be maintained throughout the intubation manoeuvres. Criswell JC, Parr MJA, Nolan JP. Emergency airway management in patients with cervical spine injuries. Anaesthesia 1994; 49: 900-3
58 B Breathing Confirm ETT in the right place Look at chest movements Paradoxical Asymmetric Listen in the axillae

59 B Breathing Right main bronchus intubation
60 B Breathing Confirm ETT in the right place Look at chest movements Paradoxical Asymmetric Listen in the axillae End tidal CO 2 Assess oxygenation Pulse oximeter


61 End Tidal CO 2 Monitors/Pulse Oximeters The StatCO2 The Capnocheck II Hand-Held Held O2/SpO2 Monitor
62 B Breathing Think about Pneumothorax (tension) Haemothorax ETT in the wrong place (if in doubt.take it out!!)
63 B Breathing GIVE 100% O 2
64 B Breathing 100 % SaO PaO 2 (mm Hg/kPa)
65 Oxygen delivery (VO 2 ) VO 2
66 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34
67 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2
68 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2 x CO
69 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2 x CO = 150 (g/dl) x 1.34 x 100% x 5 (l/min)
70 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2 x CO = 150 (g/dl) x 1.34 x 100% x 5 (l/min) = 1000 ml/min
71 C Circulation & Heamorrhage Control Shock is a generalized state of hypoperfusion causing: Anaerobic metabolism Lactic acid production Cellular dysfunction Cell death MOF
72 Causes of shock Haemorrhagic vs Nonhaemorrhagic Blood loss Tension pneumothorax Cardiac tamponade Cardiogenic Neurogenic Septic

73 Treatment of shock Direct pressure STOP the bleeding! Operation Splint fractures
74 Treatment of shock Restore volume! CO = Stroke volume (SV) x Heart rate (HR)
75 Treatment of shock Starlings Law of the Heart Stroke volume (BP, CO, UO) Initial fibre length (CVP, PCWP, LVEDP)
76 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2 x CO = 150 (g/dl) x 1.34 x 100% x 5 (l/min) = 1000 ml/min
77 The Rule of 2 s 2 s and 5 s5 Give 2 mls/kg fluid stat If CVP goes up by 5 stop giving fluid If CVP goes up by less than 5, give 2 mls/kg fluid again Keep giving 2 mls/kg fluid until CVP goes up by 5 and stays up
78 Monitoring the Response Identify Improved Organ Function CNS: Improved level of consciousness Renal: urinary output Skin: Warm, capillary refill Respirations: Improved rate and depth Vital signs: Return to normal



79 Treatment of shock Restore volume! Vascular access


80 Treatment of shock Restore volume! Warmed fluid

81 Which fluid?????? Crystalloid V Colloid

82
83 Oxygen delivery (VO 2 ) VO 2 = [Hb] x 1.34 x SaO 2 x CO = 150 (g/dl) x 1.34 x 100% x 5 (l/min) = 1000 ml/min
84 Treatment of shock Prevent hypothermia!
85 D Disability Baseline neurological examination GCS score Pupillary response OBSERVE FOR DETERIORATION!!!!
86 E Exposure / Environment Completely undress the patient PREVENT HYPOTHERMIA!!
87 The Golden Hour Multiple organ failure after trauma affects even long-term survival and functional status Critical Care 2007, 11:R95doi: /cc6111
88 The Golden Hour Multiple organ failure after trauma affects even long-term survival and functional status Critical Care 2007, 11:R95doi: /cc6111 MOF increased the overall risk of death 6.0 times.
89 The Golden Hour Multiple organ failure after trauma affects even long-term survival and functional status Critical Care 2007, 11:R95doi: /cc6111 MOF increased the overall risk of death 6.0 times. Patients with MOF were 3.9 times more likely to require personal assistance in activities of daily living.
90 The Golden Hour Multiple organ failure after trauma affects even long-term survival and functional status Critical Care 2007, 11:R95doi: /cc6111 MOF increased the overall risk of death 6.0 times. Patients with MOF were 3.9 times more likely to require personal assistance in activities of daily living. Conclusion - the presence of MOF greatly increased mortality and the risk of impaired functional status.

91
92 Secondary Survey Start only when ABCDE has been done and reassessed Vital functions are returning to normal
93 Secondary Survey - Components History
94 Secondary Survey - Components History AMPLE A M P L E Allergies Medications Past illnesses Last meal Events / Environment
95 Secondary Survey - HEAD GCS Score (again) Full neurological exam Motor and sensory and reflexes Full eye and ear exam
96 Intracranial Pressure (ICP) 10 mm Hg = Normal > 20 mm Hg = Abnormal > 40 mm Hg = Severe Sustained ICP leads to brain function and outcome
 60-55-")


97 Monro-Kellie Doctrine ICP (mm Hg) Point of Decompensation Compensation Volume of Mass Herniation
98 Cerebral Perfusion Pressure MBP ICP = CPP
99 Cerebral Perfusion Pressure MBP ICP = CPP Normal
100 Cerebral Perfusion Pressure MBP ICP = CPP Normal Cushing s Response
101 Cerebral Perfusion Pressure MBP ICP = CPP Normal Cushing s Response
102 Cerebral Perfusion Pressure MBP ICP = CPP Normal Cushing s Response Hypotension
103 Cerebral Perfusion Pressure MBP ICP = CPP Normal Cushing s Response Hypotension
104 Treatment Minimize secondary brain injury - ABCDE - Maintain CPP - Maintain blood pressure (systolic > 90 mm Hg) - Reduce ICP
105 Treatment Maintain MAP Euvolaemic fluid resuscitation Isotonic fluids Inotropes
106 Treatment Reduce ICP Controlled ventilation Goal: PaCO 2 at 35 mm Hg Head up tilt Paralysis Mannitol Surgery
107 Treatment Mannitol Use with signs of tentorial herniation Dose: 1.0 g / kg IV bolus Consult with neurosurgeon first
108 Secondary Survey Cervical Spine Tenderness Complete motor and sensory exam Reflexes X-ray

109 Normal C-Spine C Xray



110 Secondary Survey Cervical Spine Only 6 vertebrae seen



111 Secondary Survey Cervical Spine Atlas fracture

112 Secondary Survey Cervical Spine C5/6 step fracture


113 Secondary Survey Cervical Spine Er!!!!!!!!

114 Secondary Survey Cervical Spine MRI of cervical fracture-dislocation with cord injury
115 Neurogenic shock Associated with cervical / high thoracic spine injury Neurological (not a heamodynamic) phenomenon Occurs shortly after cord injury Variable duration Flaccidity and loss of reflexes Hypotension and slow heart rate
116 Treat / prevent secondary injury Ensure adequate ventilation and oxygenation Properly immobilize entire patient Maintain blood pressure with fluid and inotropes Atropine as needed for bradycardia Avoid transfer delay! Methylprednisolone
117 IV Methylprednisolone Blunt injury only Start within 8 hours of injury 30 mg/kg over 15 minutes 5.4 mg/kg over next. 23 hours if started within 3 hours of injury 48 hours if started within 3 to 8 hours after injury
118 Secondary Survey - Neck Type of injury Blunt v Penetrating

119 Secondary Survey - Neck
120 Secondary Survey - Neck Type of injury Blunt v Penetrating Look for increasing airway obstruction, stridor or hoarseness KEEP KEEP LOOKING AND LISTENING!!
121 Secondary Survey - Chest Inspect Palpate Percuss Auscultate X-rays






122 Secondary Survey - Chest Haemothorax and flail






123 Secondary Survey - Chest Pneumothorax

124 Secondary Survey - Chest Pneumothorax deep sulcus sign

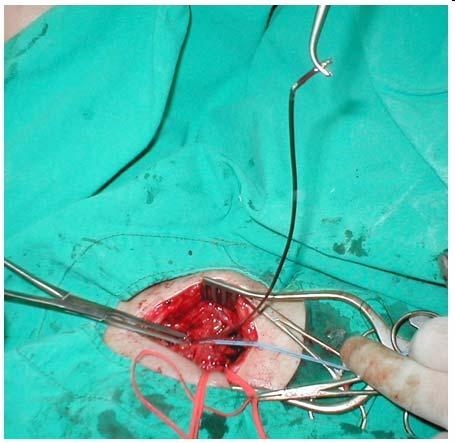
125 Chest Drain Insertion

126 Chest Drain Insertion

127 Chest Drain Insertion

128 Chest Drain Insertion

129 Chest Drain Insertion

130 Secondary Survey- Chest Tension pneumothorax This is a post mortem X-ray!!
131 Tension Pneumothorax Respiratory distress Distended neck veins Non-central trachea Hypotension and tachycardia Hyperresonance Absent breath sounds

132 Tension Pneumothorax - Treatment Immediate decompression
133 Secondary Survey - Chest Haemothorax
134 Haemothorax At least 1500 ml blood Flat (not distended) neck veins Hypotension and tachycardia Absent breath sounds Dullness to percussion (not hyperresonance) h
135 Haemothorax - Treatment Rapid volume resuscitation Operation


136 Haemothorax Multiple stab wounds Don t t forget the back
137 Secondary Survey Perineum Urethral blood Rectal tone, integrity, blood Vaginal blood, lacerations
138 Secondary Survey - Pelvis -Pain on palpation - Unequal leg length - Instability - SIGNIFICANT BLOOD LOSS!!
139 Secondary Survey Musculoskeletal:Extremities Contusion, deformity Pain Perfusion Peripheral nerve status Potential blood loss Compartment syndrome Fat embolus
140 Fat Embolism Syndrome (FES) Fat emboli were first noted by F.A. Zenker in 1861 in a railroad worker with a thoraco-lumbar crush injury Fat embolism develops in nearly all patients with fractured bones and is asymptomatic 1-3% chance of developing FES with single long bone fracture (increases with number of fractures) Mortality rate 10-20% Chest 2003;123:4
141 FES - pathophysiology 2 theories: Mechanical theory: Large fat droplets deposited in pulmonary capillary beds, and via a-v a v shunts to the brain. Causes local ischaemia and inflammation. Biochemical theory: Degradation of fat to free fatty acids cause vasculitis/ards in animals. Probably phospholipase A2 and CRP mediated.

142 Pathogenesis of ARDS in FES Fat emboli obstructs lung vessel (20microns) platelets and fibrin adhere Lipase creates FFA Inflammatory changes->endothelial damage->ards
143 FES clinical signs Cardiopulmonary (12-72 hrs after insult) Early persistent tachycardia Tachypnoea, dyspnoea, and hypoxia due to V-Q V mismatch ½ of pts with FES require mechanical ventilation (Bulger, Archives of Surgery 1997; 132: 435-9) High temperature spikes

144 FES clinical signs Dermatological (24-36 hrs after insult) Reddish-brown nonpalpable petechiae over upper body, especially axillae Occur in 20-50% of patients and resolve quickly

145 FES clinical signs Subconjunctival & oral hemorrhages/petechiae

146 FES clinical signs Neurologic (80% of patients with FES) Agitated delirium Stupor, seizures, or coma Retinal haemorrhages with intra-arterial arterial fat globules visible on fundoscopy
147 FES - investigations Blood (non-specific) Thrombocytopenia Anaemia Hypofibrinogenaemia hypocalcaemia Fat globules seen in urine, blood & sputum stained with Sudan or oil red N.B. fat in urine common in all trauma patients Imaging CXR-diffuse bilateral pulmonary infiltrates
148
149 FES - investigations Imaging Head CT-nil or diffuse white matter petechial haemorrhages BAL-staining of alveolar macrophages for fat (controversial benefit)
150 FES - treatment Medical care Supportive in nature Maintain oxygenation and ventilation Stabilize haemodynamics Blood products as needed Surgical care Early stabilization of fractures to minimize bone marrow embolization Arch Surg 1997; 132:
151 FES - steroids Steroid prophylaxis is controversial to prevent FES Theorized blunting of inflammatory response and complement activation Prospective studies suggests prophylactic steroids benefit high risk patients Few studies and small study size, so remains controversial Once FES established, steroids have not shown improved outcomes
152 FES alcohol!!!!!!! ABSTRACT: In an analysis of the cases of 100 consecutive patients with diaphyseal fractures in the major bones of the lower limb, the incidence of fat embolism syndrome was 17%. The blood alcohol level was determined at the time of admission. A raised level of alcohol in the blood was associated with a lower incidence of fat embolism. Bone Joint Surg Am. 1977;59: R Myers and JJ Taljaard

153 Marmara earthquake Turkey 1999

154 Crush Injury Crush syndrome first recorded in bombing of London during WWII: 5 people who were crushed presented in shock with swollen extremities, dark urine. Later died from renal failure.
155 Rhabdomyolysis - incidence Occurs in up to 85% of patients with traumatic injuries. Those with severe injury who develop rhabdomyolysis-induced induced renal failure have a 20% mortality rate Crush injury to any part of the body (e.g. hand) Laying on limb for long period of time
156 Rhabdomyolysis - pathophysiology Not usually directly due to ischaemia Muscle sarcolemma stretch and permeability increases Influx of sodium, water, & extracellular calcium into the sarcoplasm Cells swell reduced function myocytic death Leak of intracellular metabolites into circulation Free radicals then cause further membrane injury
157 Rhabdomyolysis symptoms and signs Clinical: Muscle pain & weakness dark urine (myoglobin) Hypovolaemic shock (fluid moves into damaged tissue) Electrolyte abnormalities: K + (leakage) Ca 2+ (sequestered in injured tissues) Metabolic acidosis phosphate Myoglobinaemia/uria
 and obstructs renal")
158 Rhabdomyolisis - ARF Myoglobin precipitates (particularly in hypovolemia) and obstructs renal tubules
159 Rhabdomyolisis - ARF Myoglobin directly toxic to the renal tubular cells especially in acid urine At ph < 5.6, myoglobin dissociates into its 2 components Globin (nontoxic) Ferrihaemate (probably toxic)
 2-32 3 h Excreted in bile Urine sample Myoglobinuria dipstick will be (+) for haemoglobin, RBC s s and myoglobin Microscopy: no RBC s,, brown casts, uric acid")
160 Lab tests Serum Creatinine Kinase Correlates with severity of rhabdomyolisis Levels peak within 24h Normally U/L >5000 U/L - high correlation with renal failure Serum myoglobin t(1/2) h Excreted in bile Urine sample Myoglobinuria dipstick will be (+) for haemoglobin, RBC s s and myoglobin Microscopy: no RBC s,, brown casts, uric acid crystals

161 Early Treatment Begin early (on the field) Ideally ½ NS with 100mmol/L bicarb corrects acidosis prevents tubular precipitation of myglobin reduces risk of hyperkalaemia 10ml/h 15% mannitol renal vasodilator free radical scavenger Forced diuresis w/in 6 hrs of admission


162 Late Treatment
163 In Summary
164 Successful management of the trauma patient requires. Teamwork Speed Efficiency Keeping it simple Using your skills Effective JUST LIKE

165
166
Lutheran Medical Center Department of Surgery
 Lutheran Medical Center Department of Surgery Morbidity & Mortality Conference Case & Topic Presentation Baiju C. Gohil, M.D. April 9, 2004 FAT EMBOLISM SYNDROME INTRODUCTION Fat emboli were first noted
Lutheran Medical Center Department of Surgery Morbidity & Mortality Conference Case & Topic Presentation Baiju C. Gohil, M.D. April 9, 2004 FAT EMBOLISM SYNDROME INTRODUCTION Fat emboli were first noted
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D.
 1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
1. In a rear-impact motor vehicle crash, which area of the spine is most susceptible to injury? A. Cervical B. Thoracic C. Lumbar D. Sacral-coccygeal 2. A 36-year-old male sustains blunt force thoracic
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
INTERNATIONAL TRAUMA LIFE SUPPORT
 INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
INTERNATIONAL TRAUMA LIFE SUPPORT NC ITLS Rev. 2/18 STUDENT GUIDE TO INTERNATIONAL TRAUMA LIFE SUPPORT What to wear ITLS is a practical course that stresses hands-on teaching. You should wear comfortable
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
ITLS Advanced Pre-Test Annotated Key 8 th Edition
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D.
 1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
1. Which of the following organs is contained in the retroperitoneal region of the abdomen? A. Stomach B. Liver C. Kidney D. Uterus 2. What is Sellick's maneuver? A. A method allowing the rescuer to hold
Crush Injury. Professeur D. MATHIEU. Medicine
 Crush Injury Professeur D. MATHIEU Department of Critical Care and Hyperbaric Medicine University Hospital of Lille - France Definitions Crush Injury An injury sustained when a body part is subjected to
Crush Injury Professeur D. MATHIEU Department of Critical Care and Hyperbaric Medicine University Hospital of Lille - France Definitions Crush Injury An injury sustained when a body part is subjected to
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Basic Assessment and Treatment of Trauma
 Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
Basic Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls 1.2
11. Spinal cord injury
 11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
11. Spinal cord injury Introduction Always think spinal (vertebral) and/or spinal cord injury (SCI) in children with trauma. Remember SCIWORA cord injury may be present without abnormalities on routine
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
Introduction to Advanced Trauma Life Support ATLS
 Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Introduction to Advanced Trauma Life Support ATLS Objectives Concepts of primary & secondary survey Priorities & Life threatening conditions Clinical & Surgical skills Basic knowledge Rapid assessment
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Pre-hospital Trauma Life Support. Rattiya Banjungam Emergency Physician, Khon Kaen Hospital
 Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Pre-hospital Trauma Life Support Rattiya Banjungam Emergency Physician, Khon Kaen Hospital Golden principles of Prehospital Trauma Care Golden Hour There is a golden hour if you are critically injured,
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH
 Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Care of the Deteriorating Patient in Recovery NADIA TICEHURST : CLINICAL NURSE EDUCATOR PERI ANAESTHETICS BENDIGO HEALTH Intended learning outcomes Describe the components of a comprehensive clinician
Trauma is a Disease Lets Get it Right A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome
 A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome druffol@lumc.edu 708.216.4541 Lets Get it Right Trauma is a Disease Importance of Trauma Care and the trauma provider role
A Good Trauma Examination Gives Your Patient Increased Odds for a Good Outcome druffol@lumc.edu 708.216.4541 Lets Get it Right Trauma is a Disease Importance of Trauma Care and the trauma provider role
Pediatric Code Blue. Goals of Resuscitation. Focus Conference November Ensure organ perfusion
 Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Code Blue Focus Conference November 2015 Duane C. Williams, MD Pediatric Critical Care Department of Pediatrics Children s Hospital of Richmond at VCU Goals of Resuscitation Ensure organ perfusion
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chapter Goal. Learning Objectives. Chapter 17. Hemorrhage & Shock
 Chapter 17 Hemorrhage & Shock Chapter Goal Use assessment findings to formulate field impression and implement treatment plan for patient with hemorrhage or shock Learning Objectives Describe epidemiology,
Chapter 17 Hemorrhage & Shock Chapter Goal Use assessment findings to formulate field impression and implement treatment plan for patient with hemorrhage or shock Learning Objectives Describe epidemiology,
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Introduction (1 of 3)
") Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Chapter 10 Shock Introduction (1 of 3) Shock (hypoperfusion) means a state of collapse and failure of the cardiovascular system. In the early stages, the body attempts to maintain homeostasis. As shock
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
Advanced Assessment and Treatment of Trauma
 Advanced Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls
Advanced Assessment and Treatment of Trauma Final Exam Version 1 1. In which of the following scenarios would the potential for serious injury or death be the GREATEST? A. 77-kg (170-lb) man who falls
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
SHOCK AETIOLOGY OF SHOCK (1) Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function
 Inadequate circulating blood volume ) Loss of Autonomic control of the vasculature (3) Impaired cardiac function") SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
SHOCK Shock is a condition in which the metabolic needs of the body are not met because of an inadequate cardiac output. If tissue perfusion can be restored in an expeditious fashion, cellular injury may
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: Shock Revised: 11/2013 (12 questions on trauma exam from this outline) DEFINITIONS Aerobic metabolism
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
Emergency Medical Training Services Emergency Medical Technician Basic Program Outlines Outline Topic: Shock Revised: 11/2013 DEFINITIONS Aerobic metabolism is energy using oxygen into cells. Anaerobic
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
APPROACH TO TRAUMA CARE
 APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
APPROACH TO TRAUMA CARE Timothy Murray, RN, CFRN Jan 2017 OBJECTIVES Demonstrate Concepts of Primary and Secondary Patient Assessment Establish Management Priorities in Trauma Situations Initiating Interventions
Acute spinal cord injury
 Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
Acute spinal cord injury Thakul Oearsakul Songklanagarind hospital Hat Yai Songkhla Introduction New SCI 10000-12000 cases Approximately 4.0-5.3 per 100000 population Common causes of traumatic SCI :Motor
CRITICAL CARE FOUNDATION POLYTRAUMA
 CRITICAL CARE FOUNDATION Rungta Hospital, Malviya Nagar, Jaipur (Supported by Indian Society of Critical Care Medicine, Jaipur Chapter) MODULE 2 POLYTRAUMA Note : All rights reserved. No part of this module
CRITICAL CARE FOUNDATION Rungta Hospital, Malviya Nagar, Jaipur (Supported by Indian Society of Critical Care Medicine, Jaipur Chapter) MODULE 2 POLYTRAUMA Note : All rights reserved. No part of this module
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours
 Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Time Equals Neurons - Spinal Cord Injury Management in the first 4 Hours William D. Whetstone M.D. Clinical Professor UCSF Department of Emergency Medicine SFGH ED Center for Neuro-Critical Emergencies
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Hypotension / Shock. Adult Medical Section Protocols. Protocol 30
 Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Hypotension / Shock History Blood loss - vaginal or gastrointestinal bleeding, AAA, ectopic Fluid loss - vomiting, diarrhea, fever nfection Cardiac ischemia (M, CHF) Medications Allergic reaction regnancy
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency First Response (EFR) Skills Assessment Sheets V4 June 2017
 Skills Assessment Sheets V4 June 2017") Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Emergency First Response () Skills Assessment Sheets V4 June 2017 Airway management & ventilation Airway management & ventilation Trauma jaw thrust 1 Hand positions 2 Perform jaw thrust / mouth open 3
Anesthesia for multiple trauma: from the scene to the OR
 Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
Anesthesia for multiple trauma: from the scene to the OR Gary Hartstein,, M.D. Service d'anesthésie-réanimationsie-réanimation Service des Urgences CHU Liège B.35 4000 Liège Course outline philosophy of
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
CHILD IN NON - TRAUMATIC COMA
 May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2
 CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
CARDIAC ARREST IN SPECIAL CIRCUMSTANCES 2 M1 Objectives To understand how resuscitation techniques should be modified in the special circumstances of: Hypothermia Immersion and submersion Poisoning Pregnancy
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
MANAGEMENT OF THORACIC TRAUMA. Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA
 MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury
 Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
SAFE approach. Unresponsive? Shout or call for help. Open Airway. Not Breathing normally? 30 chest compressions. 2 rescue breaths
 Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Basic Life Support Dial 2222 Chin lift, head tilt jaw thrust Look, listen, feel For 10 seconds Rate 100/min *Lateral tilt* SAFE approach Unresponsive? Shout or call for help Open Airway Not Breathing normally?
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium
 Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
Written 01/09/17 Rewritten 3/29/17 for Interior Regional EMS Symposium MARIA E. MANDICH MD Fairbanks Memorial Hospital Emergency Department Attending Physician Interior Region EMS Council Medical Director
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT
 PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
PRE-HOSPITAL PATIENT CARE PROTOCOLS BASIC LIFE SUPPORT/ADVANCED LIFE SUPPORT Board Approved June 2007 Revised December 2009 Revised July 2011 Revised June 2015 435 Hunter Street Fredericksburg, VA 22401
Chapter 39 Trauma in the Elderly
 Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Paediatric Shock. Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK
 Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
Paediatric Shock Dr Andrew Pittaway Department of Anaesthesia Bristol Royal Hospital for Children Bristol, UK Self-assessment: 1. What is the definition of shock? 2. List the different pathophysiological
It s as easy as ABC. Dr Andrew Smith
 It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
It s as easy as ABC Dr Andrew Smith ABCDE A simple method to apply to your assessment of patients. It is a good failsafe in all situations i.e. At an end of an OSCE when you re put under pressure! Correct
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Sign up to receive ATOTW weekly
 PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Paediatric Neurosurgical Emergencies. Kate Parkins Consultant Paediatric Intensivist Alder Hey
 Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
Paediatric Neurosurgical Emergencies Kate Parkins Consultant Paediatric Intensivist Alder Hey Level of consciousness AVPU GCS D Neurological Assessment Pupillary reaction to light Limb movements History
 TRAUMA LIFE SUPPORT PRE-HOSPITAL EXAMINATION (TLS P) 1. A high-risk bodily fluid for spreading infection is. a. sweat b. saliva c. blood d. urine 2. Items that can be used to reduce the spread of infection
TRAUMA LIFE SUPPORT PRE-HOSPITAL EXAMINATION (TLS P) 1. A high-risk bodily fluid for spreading infection is. a. sweat b. saliva c. blood d. urine 2. Items that can be used to reduce the spread of infection
Oral and Maxillofacial Surgeons and the seriously injured patient. Barts and The London NHS Trust
 Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation