PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
|
|
|
- Bethanie Stanley
- 6 years ago
- Views:
Transcription


1 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
2 Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD JUDGMENT
3 Airway and Breathing first Solid organ and Vascular injury => C Hollow viscous injury => Sepsis
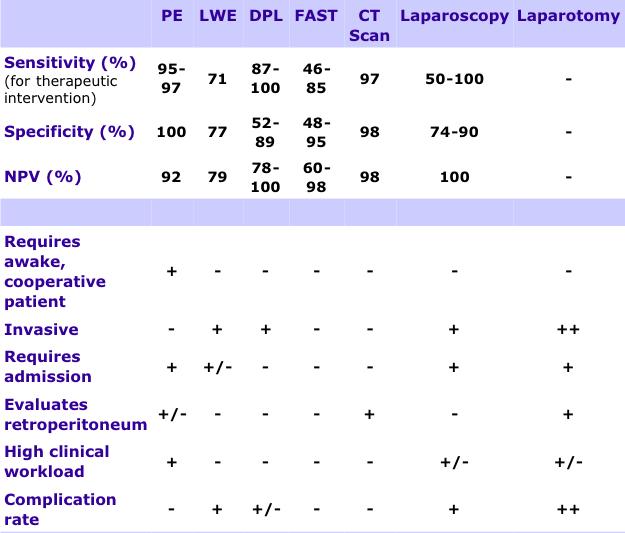
4 Investigate and assessment of abdomen base on three group 1)Normal abdomen 2)Equivocal require investigation 3)Obvious abdominal injury Diagnosis modalities 1) PE 2) DPL 3) FAST 4) CT scan 5) Diagnostic laparoscope

5
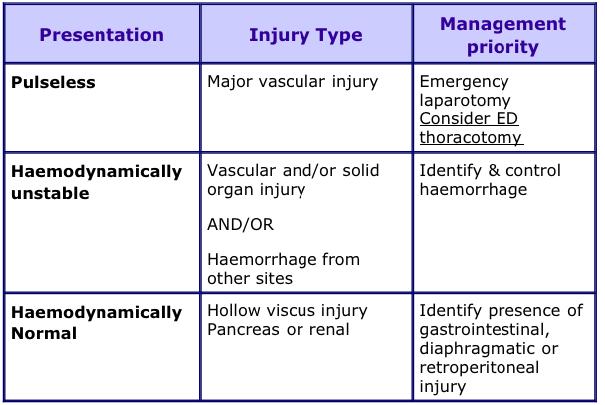
6 Hemodynamically normal patient Full evaluation and decision to surgery or non-operative management Hemodynamically stable patient Will benefit from investigation aimed to - Patient bled into abdomen? - Bleeding has stopped? - Hollow viscous injury?
7 Hemodynamically unstable patient Try to define bleeding is taking place e.g. pelvis or abdominal cavity FAST quicker than DPL but operator dependence Negative DPL => very clear that the intra abdominal bleeding is unlikely in unstable patient
8
9 Negative Exporation => Survive Positive Unexploration => Dead เจ บฟร, เส ยหน า, เส ยเวลา Operative complication (GA, wound, adhesion) Communication with patient and relative Except Negative Exploration in Pelvic Fx
10 Unstable vital sign with abdominal cause or Peritonitis (Diffuse Abdominal tender)
11 Bowel content Bile Urine Pancreatic juice Blood Difficult to exam in Head injury Cord injury Intoxication
12 Adequate analgesia Never mask abdominal symptom Make abdominal pathology easier to assess - Clear physical sign - Co-operative patient
13
14 FAST in unstable patient Positive => explore laparotomy Equivocal => DPL/DPA or explore laparotomy Negative => Find other bleeding, if not found DPL/DPA or explore laparotomy No ultrasound available =>DPL/DPA Not sent unstable patient to CT room Abdominal sign Pelvic fracture with lower abdominal sign
15

16 CT or FAST not available No other source in hemodynamic unstable Distinguish blood from other type of fluid DPA => gross blood in unstable patient Trauma Mattox Edition6
17 Not BP only Hypertensive patient?? Sign of poor tissue perfusion 4 classification of hypovolemic shock And Responsibility after fluid resuscitation

18 For 70 kg male Class I Class II Class III Class IV

19 2000 mlof isotonic solution in adult; 20 ml/kg in children
20 Solid organ injury => liver, spleen, kidney, pancreas Vascular injury with interventionist Need ICU Need OR available Need Surgeon available Necessary to CT scan??
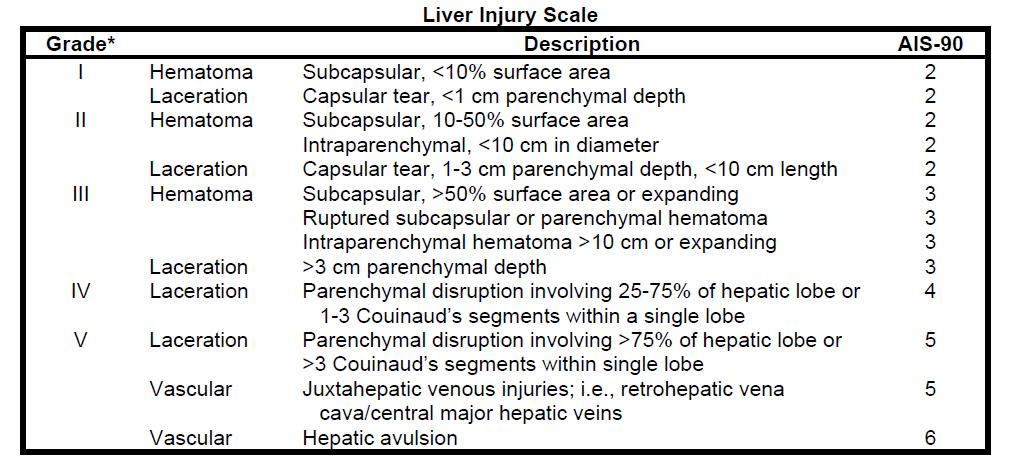
21 - Triple contrast - Solid parenchymal organ injury - Free air (Plain film abdomen) - Free fluid with Hounsfield Units - Contrast extravasations (lumen and vessel) - Injury grading Limitation - Hollow viscus - Mesenteric injury - Diaphragmatic injury - Bladder injury (need CT cystogram)
22
23 Trauma Mattox Edition6
24 Unstable Stable FAST Positive EL CT FAST Equivocal DPA +/- EL CT FAST Negative Find other bleeding, if not found DPA +/- EL Repeat FAST Observe CT?? CT not available???
25
26
27 Not routinely Stab wound Anterior abdomen No indication in Flank or back Under local anesthesia Positive => Penetration of posterior fascia Rarely practice in trauma center Trauma Mattox Edition6
28
29 Serial PE Observe 24 hr Ideal same surgeon Frequent check V/S Abdominal sigh every 4 hr Persist local symptom => other modality evaluated DPL Unstable with other cause bleeding Stable R/O hollow viscus or diaphragmatic injury FAST Not recomment
30 Routine laparotomy both stab and GSW Increase conservative in stab wound Laparotomy in GSW More conservative in GSW
31 Not routine in anterior stab wound Recommend in - Stab wound at flank and back (15% require surgical repair) - GSW Triple contrast Wound tract evaluated Free air, free fluid Contrast extravasate Intraluminal contrast leak Bowel wall defect
32 Trauma Mattox Edition6
33 Peritonitis Unstable vital sign Blood replacement??
34 Most common cause in trauma Presumed hemorrhagic shock until proven otherwise Fluid resuscitation in early signs and symptoms of blood loss Principle is Stop the bleeding and replace the volume loss
35 Whole blood is superior than component therapy PRBC:FFP ratio of 1:1 or 2:1 Platelet require in blood loss greater than 1.5 blood volume

36 อ ดร ร วและเต มน าให ท น ถ าต มแห ง => เล อดหมดต ว => ตาย Exsanguination = Extensive Hemorrhage
37 - Large syringe connect to pressure source (human hand) - IV pressure bag - Pneumatic external pressurized intravenous infusion system Increasing hematocrit and decreasing temperature => Increase blood viscosity
38 Manual of Definitive Surgical Trauma Care, Boffard Controlled resuscitation, balance resuscitation, permissive hypotension Keep SBP mmhg or 100 mmhg if head injury is suspected Penetrating trauma with hemorrhage No evidence in blunt trauma
39 Manual of Definitive Surgical Trauma Care, Boffard Delay aggressive fluid resuscitation until definitive control Prevent additional bleeding Balance of organ perfusion and Risk of rebleeding (accept a low normal blood pressure)
40
41 Manual of Definitive Surgical Trauma Care, Boffard Desire to reassess the intra-abdominal content (directed re-look) Evidence of decline of physiology reverse 1)Initial body temperature < 34 C 2)Initial acid-base status - Arterial ph <7.2 - Serum lactate > 5 mmol/l - Base deficit <-15 mmol/l in patient <55 years or <-6 mmol/l in patient >55 years
42 3)Onset coagulopathy PT >16 sec or PTT >60 sec >50% of normal 4)Other condition - >10 unit blood - SBP <90 mmhg more than 60 min - Operating time >60 min Control 1. Bleeding 2. Contamination
43
44 Thoracotomy if indication Laparotomy if indication In unstable patient, what is first? => depend on ICD content => prep both chest and abdomen

45
46 Diaphragmatic injury Difficult to diagnosis Both hemothorax and hemoperitonem in one penetrate wound Bowel content or NG tube at chest (Lt) from film chest in blunt Should be repair by non absorbable Laparoscopic diagnosis and repair is standard Can repair from thoracotomy or laparotomy
47 11 in 28 (39%) mortality in unstable pelvic Fx with laporotomy FAST positive => retroperitoneal hematoma passes into abdominal cavity J.K. Bryceland, Injury, Int. J. Care Injured in 80 unstable pelvic Fx patients with free fluid and undervent laparotomy 1 in 31 patient show retroperitoneal hemaotoma alone Mortality rate 35% in laparotomy group Steffen R, J Trauma.2004;57:
48 Unstable Trauma Mattox Edition6
49 Secondary brain injury - Hypovolemic shock - Polycompartment syndrome Severe HI associated DIC - Now, conservative in solid organ injury is accept - Threshold for laparotomy lower than non HI Laparotomy or CT head first?? Laparotomy in patient with GCS 2T?? Trauma Mattox Edition6
50 Trauma Mattox Edition6
51
52
53 Technique for temporary control of hemorrhage Perihepatic packing Electrocautery or argon beam coagulator Pringle s manoeuvre Hemostatis agent and glues Hepatic suture -> large curve needle Chromic
54 Technique for temporary control of hemorrhage Finger fracture hepatotomy and vessel ligation Tract temponade balloon (Sengstaken tube) Tractotomy and direct suture Mesh wrap Hepatic artery ligation
55 Technique for temporary control of hemorrhage Hepatic resection Hepatic vascular isolation Atriocaval shunt Veno-venous bypass
56 Hepatic vascular isolation Pringle s manoeuvre Clamp IVC above Rt kidney (Suprarenal) Clamp IVC above live (Suprahepatic)
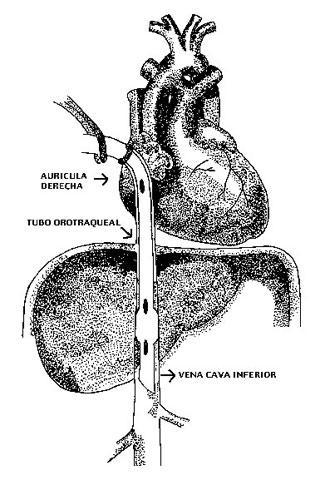
57 Atriocaval shunt
58
59
60
61 Good exposure Proximal and distal control Anatomical distortion from hematoma Active bleeding - Pressure first - Supraceliac control or Lt anterolateral thoracotomy in aorta injury - Supradiaphragmatic control in IVC Manual of Definitive Surgical Trauma Care, Boffard
62
 High mortality if delay diagnosis Should be Kocherization and open lesser sac in blunt abdominal")
63 Retroperitoneal organ In early of injury, abdominal exam is difficult FAST or DPL maybe negative Retorperitoneal free air in plain film or CT) High mortality if delay diagnosis Should be Kocherization and open lesser sac in blunt abdominal injury

64 Duodenal Inj Trauma Mattox Edition6

65 Trauma Mattox Edition6 Pancreatic Inj
66
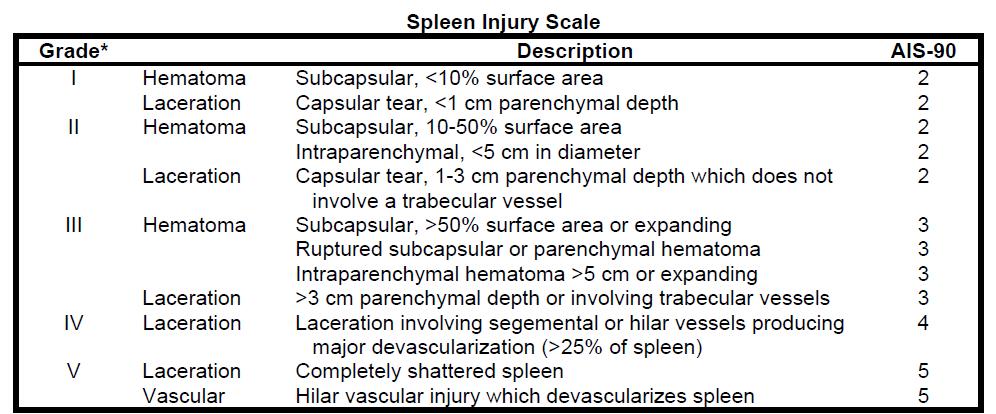
67 Non-operative Indication for surgery follow non-operative Hemodynamic instable Evidence of continued splenic hemorrhage Associate intra-abdominal injury requiring surgery Replacement of more than 50% of blood volume
68 Spleen not active bleeding -> left alone Splenic surface bleeding only -> packing, diathemy or fibril glue Minor lacerations -> absorbable suture use pledget, omental patch may be place
69 Splenic tears 1) Mesh wrap -> absorbable mesh e.g. Vicryl wrap from hilum and around parenchyma 2) Partial splenectomy -> ligating segmental vessel at hilum and seen demarcation ischemic pole 3) Splenectomy
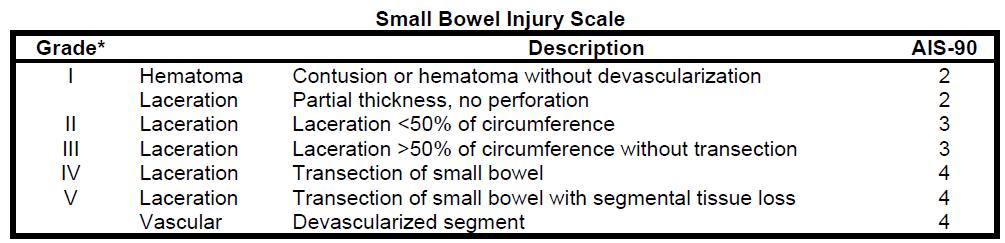
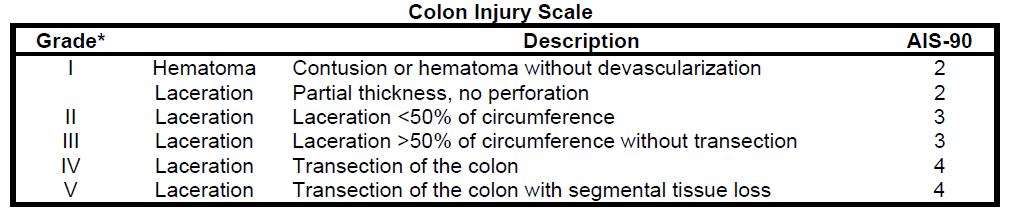
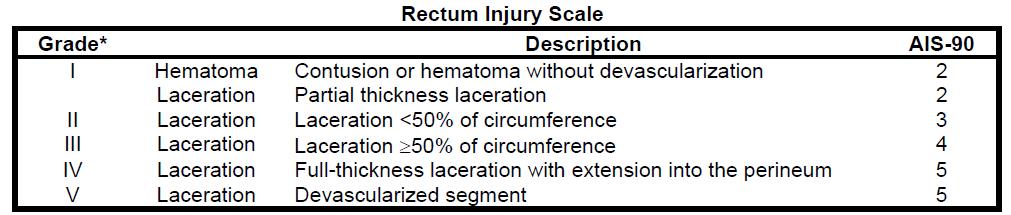
70 Option Primary repair Resection +/- anastomosis +/- proximal diversion Diversion only Depend on Position of injury => Stomach, Small bowel, Colon Severity of injury Contamination Patient status Can not conservative Need to Laparotomy
71

72 Aim of trauma is patient survive Different resource => different judgment Now, try conservative but patient safety is most important Don t forget call for help Damage control if indication
73
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
SAS Journal of Surgery ISSN SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p Available online at
; p Available online at") SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
SAS Journal of Surgery ISSN 2454-5104 SAS J. Surg., Volume-2; Issue-1 (Jan-Feb, 2016); p-53-59 Available online at http://sassociety.com/sasjs/ Original Research Article Clinical Study, Evaluation and
Penetrating Abdominal Trauma: Evaluation & Treatment
 Penetrating Abdominal Trauma: Evaluation & Treatment Charles Krin & Karim Brohi, London, UK, August 09, 2004; edited & updated by Christian Jones, Baltimore, MD, US, August 21, 2017 About this edition
Penetrating Abdominal Trauma: Evaluation & Treatment Charles Krin & Karim Brohi, London, UK, August 09, 2004; edited & updated by Christian Jones, Baltimore, MD, US, August 21, 2017 About this edition
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Emergency Laparotomy. Open vs Closed Abdomen
 Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Chapter 17. Abdominal Injuries
 Abdominal Injuries Chapter 17 Abdominal Injuries Introduction Changing patterns of warfare together with improvements in protective body armor combine synergistically to minimize truncal trauma incidence,
Abdominal Injuries Chapter 17 Abdominal Injuries Introduction Changing patterns of warfare together with improvements in protective body armor combine synergistically to minimize truncal trauma incidence,
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
ISPUB.COM. Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots. B Phillips CASE REPORT THE OPERATING ROOM
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma
 Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Deliberate Renal Ischemia
 Deliberate Renal Ischemia A Valuable and Safe Adjunct During Operations upon the Abdominal Aorta Robert K. Brawley, M.D., R. Darryl Fisher, M.D., Tom R. DeMeester, M.D., and Ronald C. Elkins, M.D. ABSTRACT
Deliberate Renal Ischemia A Valuable and Safe Adjunct During Operations upon the Abdominal Aorta Robert K. Brawley, M.D., R. Darryl Fisher, M.D., Tom R. DeMeester, M.D., and Ronald C. Elkins, M.D. ABSTRACT
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Review. 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach.
 Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Chapter 28 Review Review 1. Peritonitis would MOST likely result following injury to the: A. liver. B. spleen. C. kidney. D. stomach. Review Answer: D Rationale: In general, solid organs bleed when injured
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
Emergency Department Thoracotomy
 Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
UROLOGIC TRAUMA. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Point of Care Ultrasound (PoCUS)
") Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Study of management of blunt injuries to solid abdominal organs
 Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
Original article: Study of management of blunt injuries to solid abdominal organs 1Dr. Jayant Jain, 2 Dr. S.P. Singh, 3 Dr. Arun Bhargava 1III year resident, Dept of General Surgery NIMS hospital and medical
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
FAST Focused Assessment with Sonography in Trauma
 FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
FAST Focused Assessment with Sonography in Trauma Wilma Rodriguez Mojica,MD,FACR Professor of Radiology UPR School of Medicine Ultrasound Section - Radiological Sciences Department OBJECTIVES Understand
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
Changing Trends in the Management of Penetrating Abdominal Trauma - from Mandatory Laparotomy towards Conservative Management.
 DOI: 10.21276/aimdr.2016.2.6.SG6 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 Changing Trends in the Management of Penetrating Abdominal Trauma - from Mandatory Laparotomy towards Conservative
DOI: 10.21276/aimdr.2016.2.6.SG6 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 Changing Trends in the Management of Penetrating Abdominal Trauma - from Mandatory Laparotomy towards Conservative
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had