Neonatal Single Ventricle Heart Disease Recognition, Management, Counseling
|
|
|
- Beryl Lynch
- 6 years ago
- Views:
Transcription


1 Neonatal Single Ventricle Heart Disease Recognition, Management, Counseling Christopher J. Petit MD Assistant Professor, Pediatric Cardiology Director, Single Ventricle Program Baylor College of Medicine, Texas Children s Hospital Houston, TX
2 Disclosure No financial relationships to disclose FDA nothing to disclose
3 Objectives Recognize presentation of critical heart disease Determine PGE 1 -dependency Understand ideal pre-operative management in neonates with single ventricle Understand goals of palliative surgery Long-term outlook for patients with single ventricle
4 Disclaimer Single ventricle heart disease talk Critical Heart Disease in the Neonate Much more likely to face critical heart disease All single ventricle infants can be treated like Critical Heart Disease
5 Congenital Heart Disease: an Overview CHD (1:125) ~35,000 annually (USA) Complex CHD (1:350) ~11,000 annually (USA) Critical CHD (1:600) ~6,000 annually (USA)


6 What is Critical Heart Disease PGE 1 dependent Requires neonatal intervention Surgery TGA? Septostomy and arterial switch HLHS Norwood procedure Pulmonary Atresia shunt Catheterization Critical Aortic Stenosis balloon valve dilation
7 What is Critical Heart Disease? PGE 1 dependent because heart disease is stable during in utero circulation due to wide-open Ductus venosus Ductus arteriosus Foramen ovale
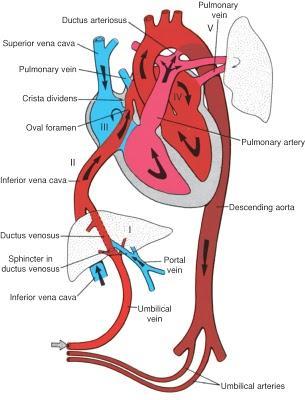

8 Fetal Circulation

9 Fetal Circulation in Single Ventricle Ductus arteriosus as versatile role player PDA provides flow to LUNGS in right heart obstruction PDA as a conduit to BODY in left heart obstruction

10 Pink is good Too much pulmonary blood flow Pink At risk of poor systemic flow Pulmonary edema Metabolic acidosis NEC Shock
11 Purple is better And blue may be perfectly fine! Check for metabolic acidosis If normal lactate, then O 2 delivery is sufficient Normal fetal O 2 sat = 60-75% Blue is better than grey! Poor perfusion/lactic acidosis

12 Infant Cardiac Care Team Dedicated team of Neonatologists Cardiologists Obstetricians CV Surgeons Focus on early management and monitoring of infants with SV heart disease Texas Children s Hospital: 30 pts/year 1-year survival: ~ 85%
13 What is Single Ventricle? Single Ventricle Physiology: Aortic Sat = Pulmonary Artery Sat Normal Physiology: Aortic Sat > Pulmonary Artery Sat Transposition Physiology Aortic Sat < Pulmonary Artery Sat

14 Normal Transposition Single Ventricle PA sat < Ao sat PA sat > Ao sat PA sat = Ao sat


15 Single Ventricle Physiology Doesn t mean SV Anatomy Seen in large VSDs, large PDAs, common atrium, etc Management is the same as in Single Ventricle Heart Disease: Optimize systemic output!
16 Single Ventricle Anatomy Variety of congenital heart defects fall under heading SV Underdevelopment/atresia of right or left Inlet Common Ventricular Inlet Underdevelopment/atresia of Outlet True common ventricle (less common)




17 Single Ventricle Anatomic Types Normal Outlet Obstruction Inlet Obstruction
18 Single Ventricle Anatomy Types Right Heart Obstruction Tricuspid Atresia Pulm Atresia/IVS Severe Ebstein s Anomaly DORV variants Left Heart Obstruction HLHS Aortic Atresia Tricuspid atresia/tga DILV* Unbalanced CAVC*
19 Presentation of Right Heart Obstruction Type SV Ductal constriction brings on cyanosis Often a gradual process Perfusion, blood pressure, HR often normal prior to complete constriction of ductus


20 Management of Right Heart Inlet Obstruction Ductal-dependent until proven otherwise Cardiac management involves PGE 1 until definitive palliation can take place o Ductal stenting o Blalock-Taussig Shunt o RVOT stenting Tricuspid valve atresia, with normal great arteries


21 Right Heart Outflow Obstruction Hypoplastic right heart syndrome Ductus provides all pulmonary blood flow ASD allows complete mixing of systemic and pulmonary venous blood
22 SV Right Heart Obstruction Ductal dependency for pulmonary blood flow ASD almost always large and right-to-left Await definitive therapy Valve perforation BT shunt Ductal stent Hypoplastic Right Heart Syndrome
23 Presentation of Left Heart Obstruction Type SV For left heart obstruction (HLHS), ductal constriction causes Metabolic acidosis Hypotension Shock Not cyanosis! (screening pulse-ox) May present in first hours of life or first days/week of life
24 Role of PGE 1 in Single Ventricle Neonates Most forms of SV are duct-dependent lesions PGE 1 not needed if patent systemic and pulmonary outlets present And there is no aortic coarctation And there is no pulmonary artery coarctation *if cyanosis or acidosis develop: PGE 1 Echo to solidify anatomy

25 History of Prostagandin Prostaglandins approved in US late 1970s Can be given in any vessel Artery, vein, intraosseous Systemic & pulmonary vasodilator Side Effects: Apnea Fever Hypotension Seizures Rash Circulation 1976


26 Prostaglandin E 1 Rash 0.05 PGE 0.05 mcg/k/minmpge 005mcg/kg/mincg/kg/min Courtesy of Gil Wernorvsky PGE 0.01 mcg/k/min 10 minutes later
 no acidosis, infants may feed while")
27 Prostaglandin Use in SV Neonates Start low-dose: 0.01 mcg/k/min In newborns in shock, may initiate PGE 1 at 0.05mcg/k/min. Infants require adequate intravascular volume to maintain blood pressure while on PGE 1 If adequate cardiac (less output, is more) no acidosis, infants may feed while awaiting surgery! Avoid apnea, avoid intubation!
28 First Steps in Management Initial newborn assessment UVC/UAC if possible (not critical) PGE 1 infusion Monitor for acidosis or cyanosis In stable patient, with fetal diagnosis, limited echocardiogram can be performed within 12 hours to confirm anatomy Assess CNS, other organs
29 Initial Management of SV Neonate Genetic evaluation Turner s (45 X,0) Preoperative brain imaging Careful counseling of parents Short term challenges Long term outlook
30 Balanced Circulation? Goal of neonatal management of SV in 2012 Maximize systemic output Balance is misnomer Usually unattainable Usually undesirable
31 Balance Qp:Qs Nelson et al, Cardiol Young 2004

32 Oxygen Delivery 1. Output trumps Qp:Qs ratio 1. High or low Qp:Qs ratio can lead to acidosis Barnea et al, JACC 1994
33 How best to manage SV Neonate Pre-op? Review fetal circulation Fetal circulation High PVR state Low SVR state Mimic this physiology postnatally! PVR and SVR

 Circulation")
34 Fetal Circulation - Normal Three guiding principles High PVR Low SVR (placental) Circulation favors the brain











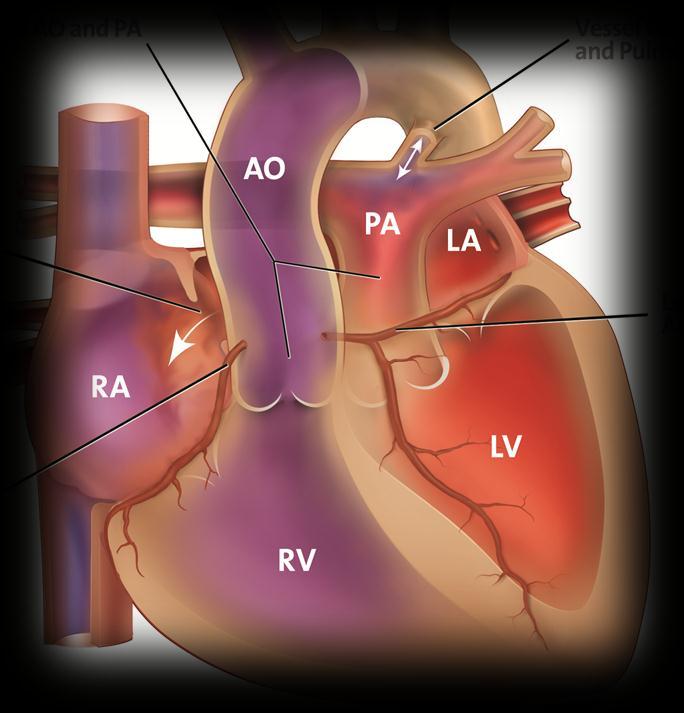
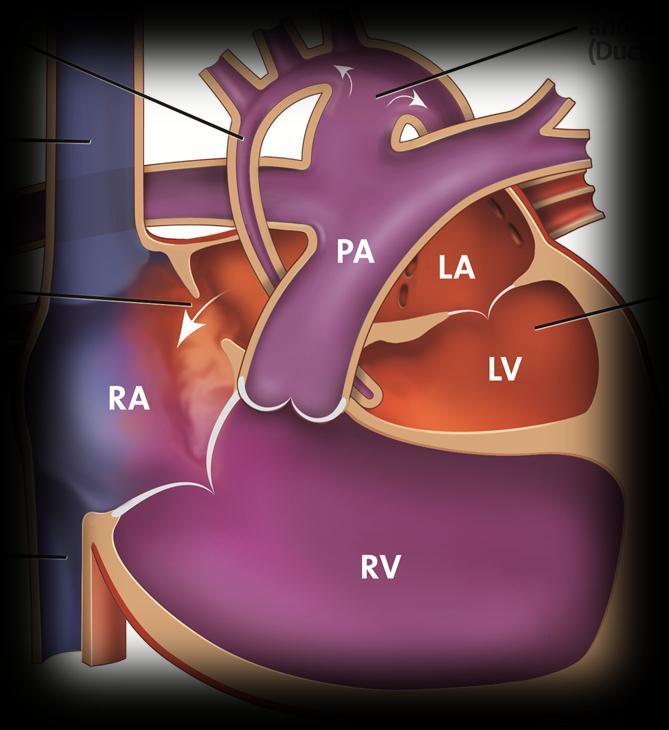
35 Fetal Circulation in HLHS Fetal circulation: Nearly normal when PDA is large and ASD is open Arch flow is retrograde Systemic flow intact Pulmonary flow is restricted

36 Fetal Ultrasound - Normal

37 HLHS: Left-to-right atrial shunting

38 HLHS: Retrograde flow in aortic arch


39 Fetal Circulation in HLHS Shillingford, Cardiol Young 2007
40 Fetal Circulation, cont Head circumference Fetal cerebral blood flow Does this have functional correlation? Lower pulsatility in middle cerebral artery in left heart obstruction type SV
41 How to maintain fetal environment? PGE 1 Low inspired O 2 Room air Only use O 2 when hypoxia Natural airway Maintains higher CO 2 Elevates PVR

42 Avoid Intubation Use low-dose PGE 1 as a rule May use caffeine to help avoid/treat apnea Transport intubation for the ride! Preop mechanical ventilation associated with poor outcomes
43 Mechanical Ventilation Hornick, ATS 2011
44 Ventilator Management in SV Neonates Avoid elective intubation Use lowest rate/tidal volume possible Avoid low CO 2 Lowest mean airway pressure possible Maximizes ventricular filling FiO 2 21% -- goal saturations 75-80% Don t drop guard after ETT in place!
45 In Unstable Neonate with SV Cyanotic PaO 2 < 30 ; SaO 2 < 75% 100% FiO 2 CXR to assess lungs PTX, Congestion STAT echo to assess the atrial septum / pulm veins Rule-out anemia Acidotic Room Air Intravascular volume Increase PGE 1 to mcg/kg/min CXR ± AXR STAT echo to assess ductus, ventricular function
46 Restrictive Atrial Septum in HLHS Causes pulmonary congestion Low cardiac output Metabolic/respiratory acidosis poor gas exchange Cyanosis Emergency!

47 Cyanosis Despite PGE1
48 Intact/Restrictive Atrial Septum
 in group 1 ost severe form of anatomic obstruction and 22 group 2 with a lesser degree of anatomic n.")
49 Surg GLATZ ET AL 9 OUTCOM E OF HLHS WITH ATRIAL RESTRICTION Restrictive Atrial Septum 1635 bability value of less than 0.05 was considered. Outcomes are poor 40% survival by 1yr aracteristics ht patients were identifi ed: 16 (42%) in group 1 ost severe form of anatomic obstruction and 22 group 2 with a lesser degree of anatomic n. The anatomic findings are listed in Table 1. birth weight for all patients was 3, g; (47%) were female and 20 patients (53%) were average gestational High age PVR at birth was 38 2 e patients (13%) were born prematurely at a 2 to 36 weeks. Five Chronic patients (13%) effusions had genetic phic syndromes including Turner s syndrome letion of chromosome 11q, and one undefi ned consisting of marked facial dysmorphia and nomalies. There was no difference in percent- Pulmonary veins are arteriolized ients with low birth weight ( 2,500 g), premaenetic syndromes between group 1 and group 0, 0.3, 0.37, respectively). Additional cardiac ntified included small ventricular septal defects errant right subclavian artery (n 1), aberrant Fig 2. Kaplan M eier survival curve demonstrating estimated 3-year cumulative survival as a function of time for all patients. Number of patients remaining at various times isannotated. Glatz et al, ATS 2007
50 Other Considerations Poor ventricular function May try inotropes/afterload reduction Dopamine Milrinone Severe atrioventricular valve regurgitation Surgical problem
51 Surgical Palliation of Single Ventricle Achieves stable circulation Unobstructed systemic flow Restricted but stable pulmonary flow Wide open ASD (surgically-created fetal circulation)
")


 Fontan")

52 History Management of Single Ventricle (SV) heart disease has evolved tremendously since the 1950s Blalock-Taussig Shunt : 1944 Glenn Shunt : 1958 (dogs) Fontan Operation : 1971 Norwood Operation for HLHS : 1983
53 History, cont Surgical advances were not thought of as stages of palliation Operations as definitive treatment for congenital heart disease Certainly, much of what is now practiced will appear out of date in coming years Much of what is known owes to experiences, errors, limited successes of past 6 decades
54 Probability of Mortality or Morbidity Operative Risk: Stage I Norwood Timing of Surgical Palliation Once you hit here There is no advantage in waiting Hours Days > ~ 1-2 Weeks Age/Weight at Surgery



55 Timing of Surgery: Norwood Norwood palliation: for HLHS, other SV variants Physiologic Repair of Hypoplastic Left Heart Syndrome Achieves anatomically the desired fetal physiology Restricted pulmonary blood flow Unrestricted systemic blood flow Norwood, NEJM 1983 Petit, CHD 2011







56 Modified Norwood Approaches Modified Norwood with RV-PA conduit ( Sano ) Hybrid Norwood
57 Timing of Surgery, cont. Our practice: Once stable, perform thorough echocardiogram Surgery within 1 st week of life Managed early post-op in cardiac ICU Transitioned to step-down service Discharge planned for 1 st month of life
58 Late Presentation Single Ventricle Infants with some forms of SV may present several days-weeks postnatally Cyanosis: Almost always prompts a cardiac workup Tetralogy of fallot Transposition Pulmonary atresia Tricuspid atresia
59 Late Presentation SV Disease Neonate presenting with acidosis: Work-up to evaluate number of systems Infectious: rule-out sepsis Viral/Bacterial Metabolic: rule-out inborn errors of metabolism Endocrine: rule-out CAH, other pathway errors GI: rule-out volvulus, enterocolitis Cardiac: rule out coarctation, left heart obstruction, myocarditis
 1:600 (ductal")
60 Playing the Odds Endocrine: 1:15,000 Metabolic: 1:8,000 Infectious: 1:3,000 GI: 1:2,500 Cardiac: 1:125 (all forms of CHD) 1:600 (ductal dependent CHD)
61 Late Presentation - Acidosis Unless another system is obviously affected, PGE 1 infusion should be ordered at same time as the echocardiogram
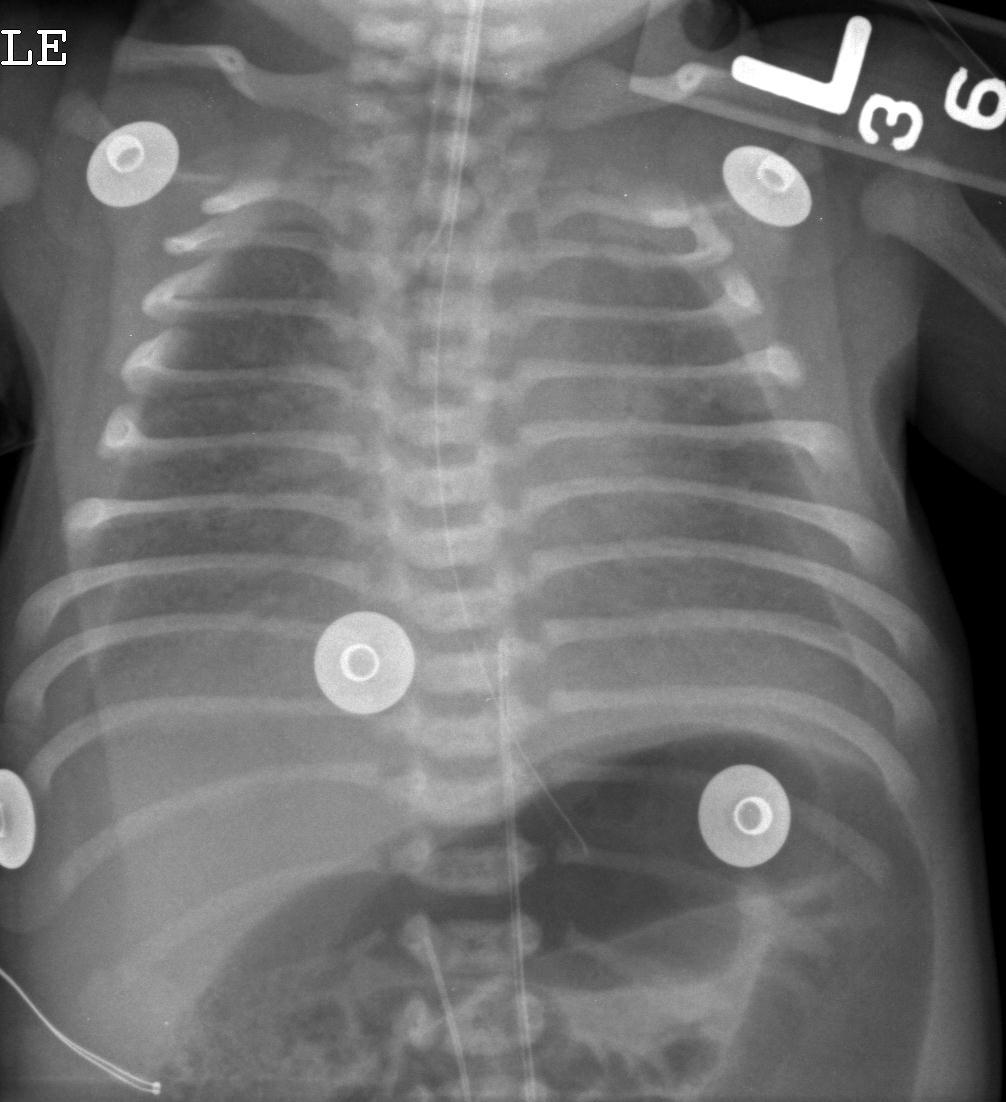
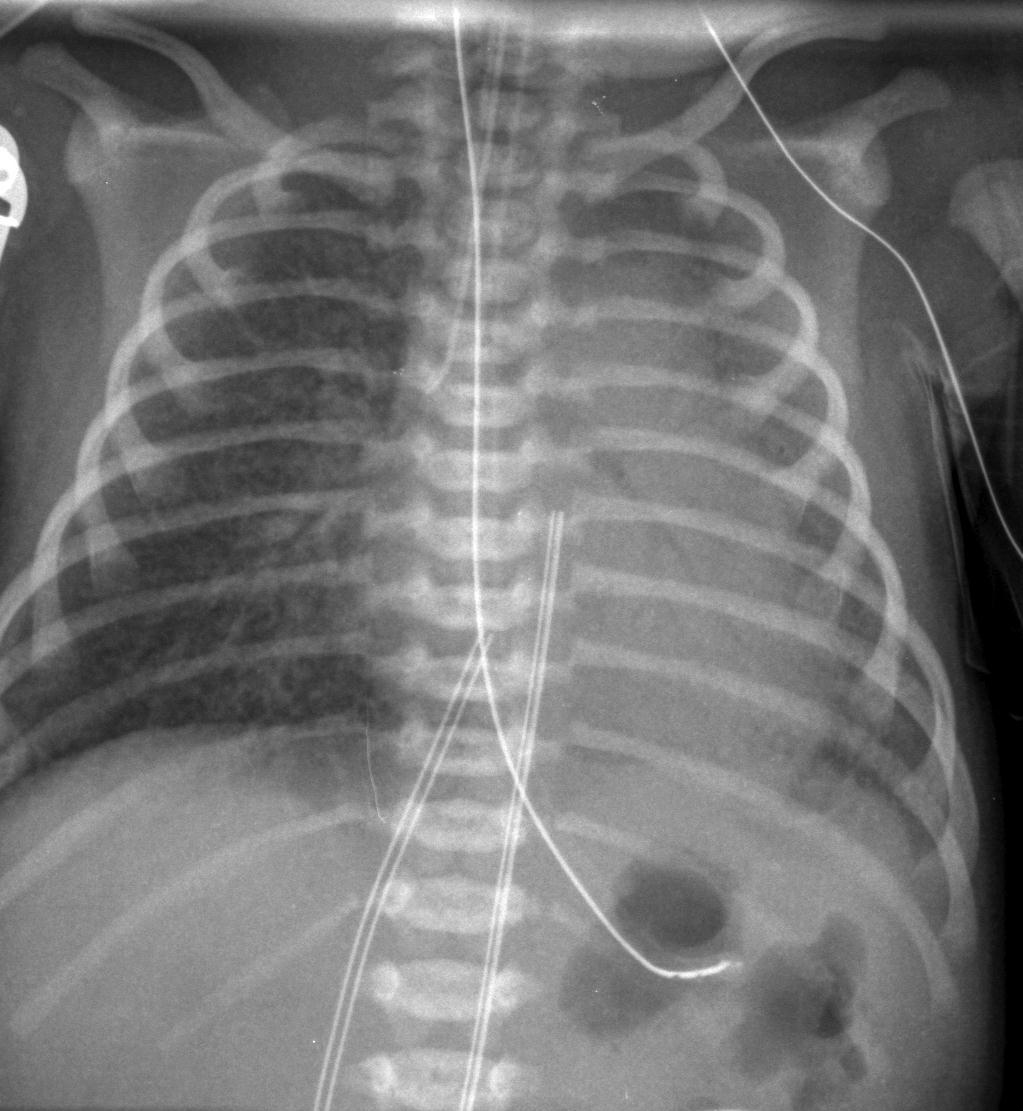
62 Case 1: 4 week old term infant Grunting respirations, pulse ox 95% Poor po feeding and vomiting x 3 weeks Poor urine output x 1 week Cool, mottled, but pink extremities Cap refill 3-4 seconds
63 Diagnosis? A) Septic shock B) Endocrine/metabolic disorder C) Right heart obstructive CHD D) Left heart obstructive CHD E) Who cares if it s C or D, start the PGE 1!!!

64 CXR Echo: HLHS, depressed RV function, ductus arteriosus almost completely closed
65 Case 2: 1 day old term female Apgars 7/9 Crying, vigorous Saturations 92%
66 Case 2: Plan of Action? PGE 1? Stat Echo? Recheck in am?
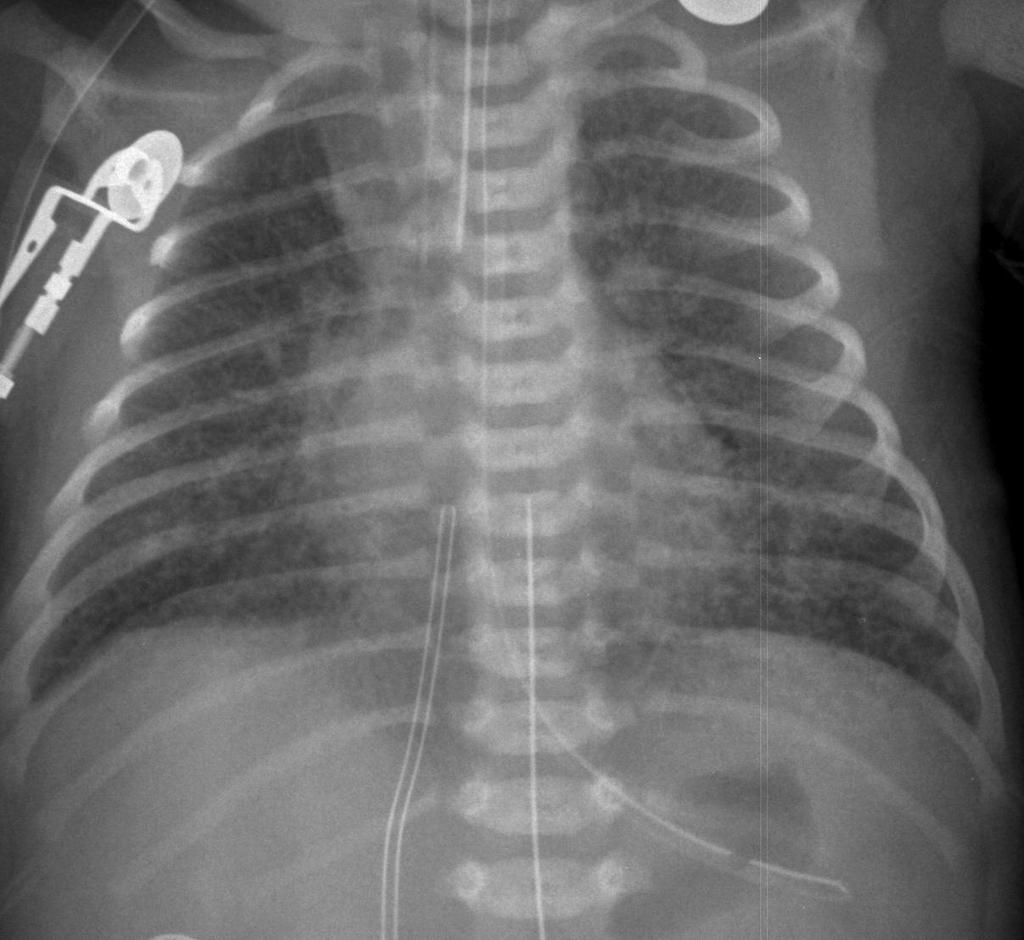
67 Case 2: cont Saturations drop to low-80s by 18 hours of life Lung disease? CXR clear PGE 1 started sats rise Echo pulmonary atresia

68 Pulmonary Atresia
69 Case 2: plan? Now what? Transfer to regional cardiac center Timing? Intubate for safe transport Use low dose PGE 1 (o.o1 mcg/k/min)
 5-year survival: 65-75% Heart transplantation is the destination for all survivors Many complications,")
70 Big Picture: Single Ventricle Outcomes Usually 3 surgical steps to palliation Norwood (neonate) Glenn (3-5 months) Fontan (2-4 years) 5-year survival: 65-75% Heart transplantation is the destination for all survivors Many complications, morbidities
71 Long Term Survival Careful family counseling is essential Common understanding among all team member is essential
72 Take Home Points For best neonatal outcomes: Neonatology + Cardiology + CV Surgery must work as an integrated team Common goal Common understanding of challenges Consistent approach within each team * not necessarily single approach across institutions!
73 Summary Critical heart disease is common More important to be attuned to Critical heart disease than Single Ventricle PGE 1 at low dose is safe, and may avoid intubation Avoid mechanical ventilation whenever possible Maintain fetal environment (high PVR, open PDA, open ASD) in critical heart disease

74 Thank You!
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Critical Heart Disease in the Newborn. What you need to know
 Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Critical Heart Disease in the Newborn What you need to know DISCLOSURES Nothing to report OBJECTIVES DESCRIBE NEONATAL CARDIOVASCULAR PHYSIOLOGY RECOGNIZE NEONATAL CARDIAC EMERGENCIES FORMULATE TREATMENT
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Leitlinien. Hypoplastisches Linksherzsyndrom. Hypoplastic left heart syndrome (HLHS)
") 1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION
 Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Deok Young Choi, Gil Hospital, Gachon University NEONATES WITH EBSTEIN S ANOMALY: PROBLEMS AND SOLUTION Carpentier classification Chauvaud S, Carpentier A. Multimedia Manual of Cardiothoracic Surgery 2007
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
The Fetal Cardiology Program
 The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
The Fetal Cardiology Program at Texas Children s Fetal Center About the program Since the 1980s, Texas Children s Fetal Cardiology Program has provided comprehensive fetal cardiac care to expecting families
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
The blue baby. Case 4
 Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Case 4 The blue baby Mrs Smith has brought her baby to A&E because she says he has started turning blue. What are your immediate differential diagnoses? 1 Respiratory causes: Congenital respiratory disorder.
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Management of a Patient after the Bidirectional Glenn
 Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
CCHD Screening with Pulse Oximetry: A Success Story!
 CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
CCHD Screening with Pulse Oximetry: A Success Story! Nicole Spillane, MD Associate Director of Neonatology, HackensackUMC Hackensack Meridian Health Objective Recognize the contribution of pulse oximetry
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database. Carlos M.
 Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database Carlos M. Mery, MD, MPH Assistant Professor, and Pediatrics Congenital Heart Texas
Incidence and treatment of chylothorax after cardiac surgery in children: analysis of a large multi-institutional database Carlos M. Mery, MD, MPH Assistant Professor, and Pediatrics Congenital Heart Texas
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
The Physiology of the Fetal Cardiovascular System
 The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
The Physiology of the Fetal Cardiovascular System Jeff Vergales, MD, MS Department of Pediatrics Division of Pediatric Cardiology jvergales@virginia.edu Disclosures I serve as the medical director for
Objectives. Prenatal Diagnosis of Critical Congenital Heart Disease. The Law. Disclosure. Dylan s Story
 Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Keeping the Beat: Pediatric Cardiac Screening and Management of Congenital Heart Disease Prenatal Diagnosis of Critical Congenital Heart Disease Robert Koppel, MD Neonatal/Perinatal Medicine, Pediatrics
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Introduction to Fetal Medicine. Lloyd R. Feit M.D. Associate Professor of Pediatrics Warren Alpert Medical School Brown University
 Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
Associate Professor of Pediatrics Warren Alpert Medical School Brown University Fetal Cardiology Important in evaluation of high risk pregnancies. Information obtainable in > 95% of patients attempted.
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The fetal circulation
 Peter John Murphy MB ChB DA FRCA The fetal circulation (Fig. 1) is markedly different from the adult circulation. In the fetus, gas exchange does not occur in the lungs but in the placenta. The placenta
Peter John Murphy MB ChB DA FRCA The fetal circulation (Fig. 1) is markedly different from the adult circulation. In the fetus, gas exchange does not occur in the lungs but in the placenta. The placenta
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Approach to a baby with cyanosis
 Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Approach to a baby with cyanosis Objectives Cyanosis : types Differentials: cardiac vs. non cardiac Approach Case scenarios Cyanosis Greek word kuaneos meaning dark blue Bluish discolouration of skin,
Before we are Born: Fetal Diagnosis of Congenital Heart Disease
 Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Before we are Born: Fetal Diagnosis of Congenital Heart Disease Mohamed Sulaiman, MD Pediatric cardiologist Kidsheart: American Fetal & Children's Heart Center Dubai Healthcare City, Dubai-UAE First Pediatric
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome
 Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
Atrial Septostomy in HLHS and ECMO: Indications, Technique and Outcome Dr Damien Kenny, MB, MD Assistant Professor of Pediatrics Director of the Cardiac Catheterization Hybrid Suite Co-Director of the
NCC Review Cardiac 8/22/12. Intrauterine Blood Flow. Topics
 NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
NCC Review Cardiac Tracey Buckley MSN,RNC, NNP-BC Cape Fear Valley Health System Topics Transition to Extrauterine Life Cyanosis Congenital Heart Disease (CHD) Clinical Manifestations of CHD Therapeutic
11/27/2012. Objectives. What is Critical Congenital Heart Disease?
 Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
Screening for Critical Congenital Heart Disease in the Apparently Healthy Newborn A presentation of Texas Pulse Oximetry Project: A Joint Educational Initiative of The University of Texas Health Science
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center
 Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
Regional Prenatal Congenital Heart Disease Detection and Practices Lori Erickson MSN, RN, CPNP-PC Ward Family Heart Center The Children's Mercy Hospital, 2014. 05/14 Objectives Evaluate our regional prenatal
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist
 Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
Adult Congenital Heart Disease for the Internist Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Upon completion of this presentation, the participant will be able to:
 B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
B12 Neonatal Cardiology Review Nicole Bowie, NNP-/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL The speaker has signed a disclosure form and indicated she has no significant
DIAGNOSIS, MANAGEMENT AND OUTCOME OF HEART DISEASE IN SUDANESE PATIENTS
 434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
Neonatal Cardiac Anomalies
 Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Objectives Neonatal Cardiac Anomalies Karen Knuth, RNC, MN, NNP-BC, ARNP Seattle Childrens Hospital What is CHD? Normal anatomy and circulation Clinical presentation: signs and symptoms Diagnostics Common
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
FANNP 28TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW OCTOBER 17-21, 2017
 Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Neonatal Cardiology Review Nicole Bowie, NNP/BC, PNP Neonatal Nurse Practitioner Jackson Memorial Hospital, Miami, FL B12 The speaker has signed a disclosure statement indicating that she has no significant
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease II: The Repaired Adult
 Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery
 Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Accuracy of the Fetal Echocardiogram in Double-outlet Right Ventricle
 Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
Blackwell Publishing IncMalden, USACHDCongenital Heart Disease 2006 The Authors; Journal compilation 2006 Blackwell Publishing, Inc.? 200723237Original ArticleFetal Echocardiogram in Double-outlet Right
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Preoperative Echocardiographic Assessment of Uni-ventricular Repair
 Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
Preoperative Echocardiographic Assessment of Uni-ventricular Repair Salem Deraz, MD Pediatric Cardiologist, Aswan Heart Centre Magdi Yacoub Heart Foundation Uni-ventricular repair A single or series of
Summary. HVRA s Cardio Vascular Genetic Detailed L2 Obstetrical Ultrasound. CPT 76811, 76825, _ 90% CHD detection. _ 90% DS detection.
 What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
What is the role of fetal echocardiography (2D 76825, cardiovascular color flow mapping 93325) as performed in conjunction with detailed fetal anatomy scan (CPT 76811) now that AIUM requires limited outflow
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
DORV: The Great Chameleon. Heart Conference October 15, 2016 Tina Kwan, MD
 DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
DORV: The Great Chameleon Heart Conference October 15, 2016 Tina Kwan, MD Kenneth Maehara, Ph.D. May 7, 1942 - August 26, 2013 A.R. A classic case of broken heart 38 week AGA F born at an OSH to
Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita
 Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita The Children's Mercy Hospital, 2014. 05/14 Objectives Review current local and regional
Regional Prenatal Congenital Heart Disease Detection and Practices Jenny Ecord, APRN Ward Family Heart Center Wichita The Children's Mercy Hospital, 2014. 05/14 Objectives Review current local and regional
Stent implantation into the patent ductus arteriosus in cyanotic congenital heart disease with duct-dependent or diminished pulmonary circulation
 The Turkish Journal of Pediatrics 2007; 49: 413-417 Original Stent implantation into the patent ductus arteriosus in cyanotic congenital heart disease with duct-dependent or diminished pulmonary circulation
The Turkish Journal of Pediatrics 2007; 49: 413-417 Original Stent implantation into the patent ductus arteriosus in cyanotic congenital heart disease with duct-dependent or diminished pulmonary circulation
MEDICAL SCIENCES Vol.I -Adult Congenital Heart Disease: A Challenging Population - Khalid Aly Sorour
 ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
ADULT CONGENITAL HEART DISEASE: A CHALLENGING POPULATION Khalid Aly Sorour Cairo University, Kasr elaini Hospital, Egypt Keywords: Congenital heart disease, adult survival, specialized care centers. Contents
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery s present: Early Repair Era
 Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Deborah Kozik, DO Assistant Professor Division of Cardiothoracic Surgery 1954 1960: Experimental Era 1960 s 1980 s: Palliation Era 1980 s present: Early Repair Era 2010 2030 s: Fetal Interventions Hybrid
Transient malformations like PDA and PDA of prematurity were not considered. We have divided cardiac malformations in 2 groups:
 CARDIAC MALFORMATIONS DETECTED AT BIRTH Anwar Dudin-MD, Annie Rambaud-Cousson-MD, Mahmoud Nashashibi-MD Pediatric Department Makassed Hospital Jerusalem Diagnosis of congenital heart disease in the neonatal
CARDIAC MALFORMATIONS DETECTED AT BIRTH Anwar Dudin-MD, Annie Rambaud-Cousson-MD, Mahmoud Nashashibi-MD Pediatric Department Makassed Hospital Jerusalem Diagnosis of congenital heart disease in the neonatal