SUNY Downstate Department of Surgery
|
|
|
- Muriel Lamb
- 6 years ago
- Views:
Transcription


1 Christopher Lau Kings County Hospital Center SUNY Downstate Department of Surgery October 13, 2011

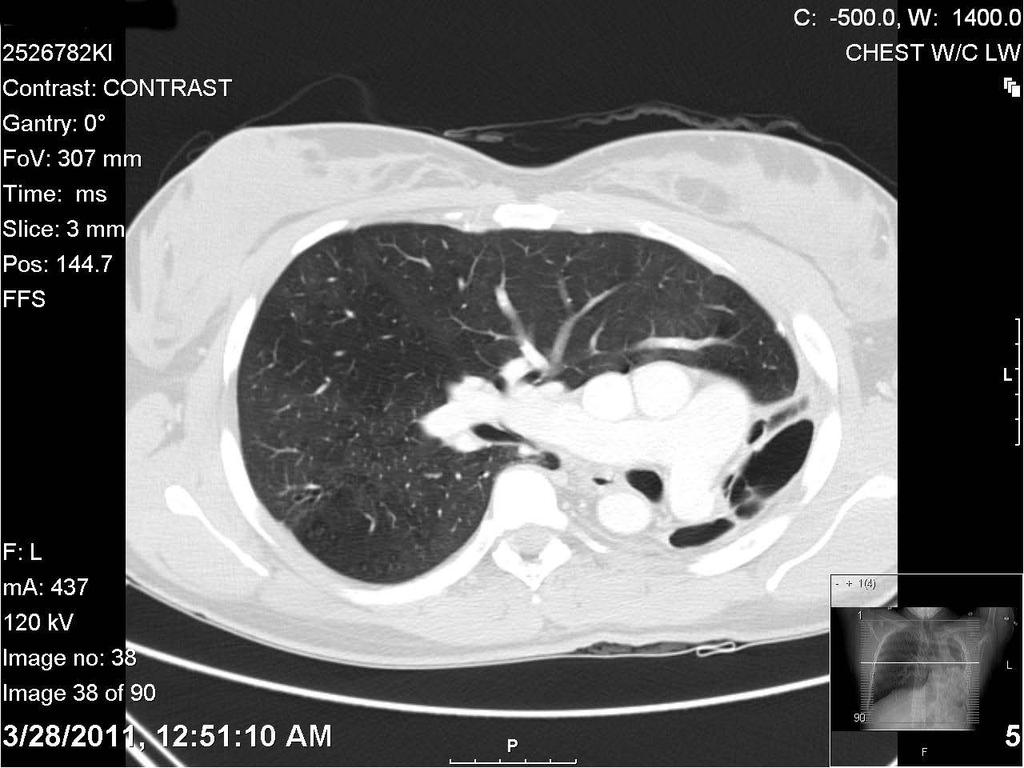
2 xx year old female first presented in April 2011 with cough, SOB, left sided pleuritic chest pain Symptoms progressively worsening for 5-10 years Recurrent respiratory infection with productive sputum, improves with antibiotics Known left lung collapse since adolescence as per patient No history of TB, PE, tachypnea PPD negative in Feb, HIV negative per patient
3 Asthma Left lung collapse PSH: None Social Hx: No tobacco, etoh, drugs Family Hx: no hx of cancer or respiratory problems NKDA Meds: Albuterol PRN
4 T 97.8, BP 120/68, HR 69, RR 14 Gen: AAOx3, NAD Neck: trachea midline CVS: S1S2 normal, no murmurs Chest: CTA on right, decreased breath sounds on left Abd: soft, NT, NT, normal BS Ext: no edema, cyanosis, clubbing


5 PPD: positive 10mm Sputum AFB: negative x3 CBC: 9.88>12.9/41.8<302 BMP: 136/4.2/100/27/11/0.98/69/9.1 Coag: 11.7/20.9/1.1 RA ABG: 7.43/34.1/110/99/23.8/-1.2

6
7
8 Pre-Rx Post-Rx Best % Predicted Best % Predicted % Change FVC FEV FEV1/FVC FEF25-75% PEF FET100%
9 Lung Volumes Best % Predicted Diffusion Best % Predicted VC TLC DLCO DLCO/VA RV RV/TLC 51 FRC
10 Gross bronchiectasis of LUL and lingula with completely destroyed and shrunken left lung No excess secretions, purulent discharge, fungal growth, or blood BAL culture: pan-sensitive Pseudomonas Negative for malignancy Negative for viral inclusions AFB and GMS stain negative for organisms Treated with Levofloxacin 2 weeks Cough, SOB, and chest pain resolved Pt returned to baseline level of activity

11 Bronchoscopy Left thoracotomy 5 th rib resection Partially extrapleural pneumonectomy Lung was dissected extrapleurally Hilar structures identified intrapericardially and followed out to the pleural space and then divided Pericardial patch
12 POD 1: Extubated, chest tube removed, diet advanced POD 3: Transferred to floor POD 6: Started on zosyn for persistent leukocytosis and OR culture with pseudomonas POD 7: Tachycardic to 115, SO2 85% CTA negative for PE, Transferred to SICU Improved with O2 face mask, chest PT, and continued abx CXR: RLL opacification


13 POD 12: Abdomen distended Disimpacted and enema given CT: cecal volvulus OR for ex lap, right hemicolectomy POD 25: Discharged home POD 32: Seen in clinic, doing well.

14 Hypoplastic lung with marked cystic bronchiectasis and fibrosis Chronic active follicular bronchitis and bronchiolitis

15
16 Pulmonary hypoplasia is rare in adults, usually diagnosed in childhood Patients usually die before adulthood Lung infections Other congenital anomalies Left side is involved more often than right In utero, gas exchange is performed by the placenta Substantial abnormalities may be present with minimal symptoms until the neonate is delivered Mármol E, Martínez S, Baldo X, Rubio M, Sebastián F. [Pulmonary hypoplasia in the adult]. Cir Esp Oct;88(4): Epub 2010 Mar 4. Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp ,




17 Faruqi S, Varma R, Avery G, Kastelik J. Pulmonary Hypoplasia. Intern Med. 2011;50(10):1129. Epub 2011 May 1.

18 Static lung expansion Epithelial cells secrete fluid into the lung lumen Distends future air spaces to a fluid volume that approximates postnatal FRC Inadequate production or excessive drainage leads to pulmonary hypoplasia Dynamic lung expansion Fetal breathing movements Absent or abnormal breathing leads to pulmonary hypoplasia Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp ,



19 Pulmonary agenesis/aplasia is due to arrest of development at the embyonic stage Pulmonary agenesis: bronchial tree, pulmonary parenchyma, or pulmonary vasculature does not develop Absence of carina; trachea into single bronchus Pulmonary aplasia: there is a rudimentary bronchial pouch with absence of distal lung Secretions can pool in the stump and become infected May involve one lobe or the entire lung Associated with other non-pulmonary anomalies Bilateral defects are rare and invariably lethal Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp , Wilmott R, Boat T, Bush A, Chernick V. Kendig's Disorders of the Respiratory Tract in Children, 7 th ed. Congenital Lung Disease: p 297. Backer CL, Kelle AM, Mavroudis C, Rigsby CK, Kaushal S, Holinger LD. Tracheal reconstruction in children with unilateral lung agenesis or severe hypoplasia. Ann Thorac Surg Aug;88(2):624-30; discussion
 Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp 596-597, 599-600.")
20 Pulmonary hypoplasia can occur at any time during gestation Hypoplastic lungs are small in volume Have decreased numbers of alveoli, bronchioles and arterioles Primary pulmonary hypoplasia is rare Usually occurs in conjunction with another abnormality (secondary pulmonary hypoplasia) Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp ,


21 Space occupying lesions Oligohydramnios Diaphragmatic hernia Leakage (PROM) Massive pleural effusion Underproduction (renal dysplasia) Inadequate vascular supply PA atresia Hypoplastic right heart Inadequate thoracic cage Asphyxiating thoracic dystrophy Tetralogy of Fallot Lack of fetal breathing movements Chromosomal abnormalities Achondrogenesis Trisomy 13 or 18 Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp , Lutterman J, Jedeikin R, Cleveland DC. Horseshoe lung with left lung hypoplasia and critical pulmonary venous stenosis. Ann Thorac Surg Mar;77(3):


22 Wilmott R, Boat T, Bush A, Chernick V. Kendig's Disorders of the Respiratory Tract in Children, 7 th ed. Congenital Lung Disease: p 297.

23 Infants generally have respiratory failure in the newborn period Reduced lung volumes impair ventilation and lead to hypercarbia Decreased surface area for gas leads to hypoxemia Decreased cross-sectional area of vasculature makes these infants susceptible to pulmonary hypertension Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp ,


24 Supportive Outcome depends on severity of hypoplasia and associated anomalies Lungs may be extremely difficult to ventilate Pneumothorax is common due to high distending pressures HFV with low tidal volumes may be effective Treat infections with antibiotics Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp ,

25 Pulmonary hypoplasia is usually a disease of infants High mortality Usually associated with other anomalies Secondary pulmonary hypoplasia is more common than primary Treatment is supportive Can lead to recurrent infections
26
27 Incidence of pulmonary complications is directly related to proximity of procedure to diaphragm Pulmonary, esophageal and other thoracic procedures are high risk for pulmonary complications FRC declines by 35% after thoracotomy with lung resection and 30% after upper abdominal surgery When FRC approaches closing volumes, atelectasis occurs Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
28 History and physical exam Labs: CBC, BMP, LFT, PT/PTT, T&C Imaging studies Blood gases Pulmonary function testing Quantitative V/Q scan if needed Exercise test if needed Echocardiogram/cardiac evaluation in at risk patients Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.

 have better predictive value for morbidity and mortality Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L.")
29 Type of operation and incision have varying effects on pulmonary function FRC is important lung volume measurement associated with pulmonary complications Reduction in FRC results in premature airway closure and atelectasis Timed measurements (e.g. FEV1) have better predictive value for morbidity and mortality Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.

30 Unlikely to contribute for mediastinoscopy, pleural effusions, pleural biopsy, esophageal surgery with no hx of lung disease Appropriate in patients with dyspnea, significant functional limitation, prior pulmonary resection, COPD with change in functional capacity Mandatory in patients being considered for pulmonary resection Two tests with best predictive value for post op M&M FEV1 and DLCO Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
31 Simple calculation ppo-fev 1 = FEV 1 [1 (number of segments resected x )] Similar for DLCO Regional assessment of lung function Quantitative V/Q scan is the current standard Reported as percent function contributed by 6 regions ppo value = baseline value x (100 percent ventilation or perfusion in the region of planned resection)/100 Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.

32 Lung function and calculation of post op function can reliably identify patients at low risk They do less well at defining high risk patients For refinement of risk, assessment of functional capacity is needed Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
33 Stair climbing Incremental cardiopulmonary exercise testing Measures maximal oxygen uptake rate (MVO2) Predicted post op exercise capacity (ppo-mvo2) There is no concensus to the sequence of testing Whether exercise testing or quantitative V/Q scan is done first is a matter of local practice and availability Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
34 Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed.

35 Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
 If borderline then get quantitative V/Q scan and recalculate Still unsure? Get exercise testing Need ppo-vo2max > 10 ml/kg/min Need ppo-fvc > 1.")
36 FEV1 > 2L : proceed with pneumonectomy FEV1 > 1L : proceed with lobectomy Need ppo-fev1 > 0.8 (40% pred.) Need ppo-dlco > ml/min/mmhgco (40% pred.) If borderline then get quantitative V/Q scan and recalculate Still unsure? Get exercise testing Need ppo-vo2max > 10 ml/kg/min Need ppo-fvc > 1.5L No resection if pco2 > 45 or po2 < 50
![Mármol E, Martínez S, Baldo X, Rubio M, Sebastián F. [Pulmonary hypoplasia in the adult]. Cir Esp. 2010 Oct;88(4):274-6. Epub 2010 Mar 4. Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed.](/docs-images/77/74805434/images/37-3.jpg "Neonatal Respiratory diseases: pp 596-597, 599-600. Wilmott R, Boat T, Bush A, Chernick V. Kendig's Disorders of the Respiratory Tract in Children, 7 th ed. Congenital Lung Disease: p 297.")
37 Mármol E, Martínez S, Baldo X, Rubio M, Sebastián F. [Pulmonary hypoplasia in the adult]. Cir Esp Oct;88(4): Epub 2010 Mar 4. Fuhrman B, Zimmerman J. Pediatric Critical Care, 4 th ed. Neonatal Respiratory diseases: pp , Wilmott R, Boat T, Bush A, Chernick V. Kendig's Disorders of the Respiratory Tract in Children, 7 th ed. Congenital Lung Disease: p 297. Lutterman J, Jedeikin R, Cleveland DC. Horseshoe lung with left lung hypoplasia and critical pulmonary venous stenosis. Ann Thorac Surg Mar;77(3): Faruqi S, Varma R, Avery G, Kastelik J. Pulmonary Hypoplasia. Intern Med. 2011;50(10):1129. Epub 2011 May 1. Backer CL, Kelle AM, Mavroudis C, Rigsby CK, Kaushal S, Holinger LD. Tracheal reconstruction in children with unilateral lung agenesis or severe hypoplasia. Ann Thorac Surg Aug;88(2):624-30; discussion Sugarbaker D, Bueno R, Krasna M, Mentzer S, Zellos L. Adult Chest Surgery, 1 st ed. Shields T, LoCicero J, Reed C, Feins R. General Thoracic Surgery, 7 th ed.
SUNY Downstate Department of Surgery
 Christopher Lau Kings County Hospital Center SUNY Downstate Department of Surgery November 10, 2011 xx year old female first presented in mm/dd/yyyy with cough, SOB, left sided pleuritic chest pain Symptoms
Christopher Lau Kings County Hospital Center SUNY Downstate Department of Surgery November 10, 2011 xx year old female first presented in mm/dd/yyyy with cough, SOB, left sided pleuritic chest pain Symptoms
Preoperative Workup for Pulmonary Resection. Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016
 Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative Workup for Pulmonary Resection Kristen Bridges, M.D. Richmond University Medical Center January 21, 2016 Patient Presentation 50 yo male with 70 pack year smoking history Large R hilar lung
Preoperative assessment for lung resection. RA Dyer
 Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
Preoperative assessment for lung resection RA Dyer 2016 The ideal assessment of operative risk would identify every patient who could safely tolerate surgery. This ideal is probably unattainable... Mittman,
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
SURGERY FOR GIANT BULLOUS EMPHYSEMA
 SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
SURGERY FOR GIANT BULLOUS EMPHYSEMA Dr. Carmine Simone Head, Division of Critical Care & Thoracic Surgeon Department of Surgery December 15, 2006 OVERVIEW Introduction Classification Patient selection
Molla Teshome MD, Habtamu Belete MD Aurora Health Care Internal Medicine Residency Program
 Molla Teshome MD, Habtamu Belete MD Aurora Health Care Internal Medicine Residency Program History 32 year-old male who presented with a 4 days history of: Productive cough Right sided pleuritic chest
Molla Teshome MD, Habtamu Belete MD Aurora Health Care Internal Medicine Residency Program History 32 year-old male who presented with a 4 days history of: Productive cough Right sided pleuritic chest
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada. Slide Tracheoplasty
 90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
90 th Annual Meeting The American Association for Thoracic Surgery May 1, 2010 Toronto, Ontario, Canada Congenital Skills Course Slide Tracheoplasty Carl Lewis Backer, MD A.C. Buehler Professor of Surgery
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
PULMONARY VENOLOBAR SYNDROME. Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital.
 PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
PULMONARY VENOLOBAR SYNDROME Dr.C.Anandhi DNB Resident, Southern Railway Headquarters Hospital. Presenting complaint: 10 yrs old girl with recurrent episodes of lower respiratory tract infection from infancy.
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
COMPREHENSIVE RESPIROMETRY
 INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
INTRODUCTION Respiratory System Structure Complex pathway for respiration 1. Specialized tissues for: a. Conduction b. Gas exchange 2. Position in respiratory pathway determines cell type Two parts Upper
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011
 Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Dyspnea in the Cancer Patient 33 rd Annual PSONS Nursing Symposium April 1, 2011 Kathy Witmer, MN, ARNP Swedish Cancer Institute Thoracic Surgery - Oncology Dyspnea The word denotes disordered breathing
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
GOALS AND INSTRUCTIONAL OBJECTIVES
 October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
October 4-7, 2004 Respiratory GOALS: GOALS AND INSTRUCTIONAL OBJECTIVES By the end of the week, the first quarter student will have an in-depth understanding of the diagnoses listed under Primary Diagnoses
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Objectives. What is a Chest X Ray? CXR Workshop. Definition (diagnostic tool/internal PE) Types. Cost
 Types. Cost") Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Objectives CAPA 2011 Christy Wilson, PA C Georgia Lung Associates Identify the radiographic landmarks on a chest radiograph Recognize identifiers of poor quality on the chest radiograph Outline an approach
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Congenital Diaphragmatic Hernia information for parents. David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix
 Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Short Cases M I CHA E L DE RYNCK, M D U N I V ERSITY OF CA LG A RY F E BR UA RY
 Short Cases MICHAEL DERYNCK, MD UNIVERSITY OF CALGARY FEBRUARY 15 2018 Case 1: Beyond Bronchiolitis Presentation 2 month old, term girl Cough and rhinitis, increased work of breathing, wheeze and apnea
Short Cases MICHAEL DERYNCK, MD UNIVERSITY OF CALGARY FEBRUARY 15 2018 Case 1: Beyond Bronchiolitis Presentation 2 month old, term girl Cough and rhinitis, increased work of breathing, wheeze and apnea
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Levine Children s Hospital. at Carolinas Medical Center. Respiratory Care Department
 Page 1 of 7 at Carolinas Medical Center 02.04 Pediatric Patient-Centered Respiratory Care Protocol Application of Chest Physical Therapy Created: 1/98 Reviewed: 4/03, 1/05, 6/08 Revised: Purpose: To describe
Page 1 of 7 at Carolinas Medical Center 02.04 Pediatric Patient-Centered Respiratory Care Protocol Application of Chest Physical Therapy Created: 1/98 Reviewed: 4/03, 1/05, 6/08 Revised: Purpose: To describe
Chapter 16. Lung Abscess. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Chapter 16 Lung Abscess 1 EDA PM C AFC RB A B Figure 16-1. Lung abscess. A, Cross-sectional view of lung abscess. B, Consolidation and (C) excessive bronchial secretions are common secondary anatomic alterations
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay
 Congenital Malformation of the Lung and Airways HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay DivisiRespirologiDepartemenIlmuKesehatanAnak FakultasKedokteran Universitas Sumatera
Congenital Malformation of the Lung and Airways HelmiLubis, RidwanMuchtarDaulay, WismanDalimunthe, Rini Savitri Daulay DivisiRespirologiDepartemenIlmuKesehatanAnak FakultasKedokteran Universitas Sumatera
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT
 PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
PBL RESPIRATORY SYSTEM DR. NATHEER OBAIDAT Dr started to talk about his specialty at the hospital which is (ICU-Pulmonary-Internal Medicine). Pulmonary medical branch is a subspecialty of internal medicine.
Pulmonary Agenesis sentations picked up over a period of 4 years. These cases were suspected and then documented during life.
 Pulmonary Agenesis sentations picked up over a period of 4 years. These cases were suspected and then documented during life. B. Rajshekhar Case Reports Sunil Gomber Anurag Krishna* Five cases of pulmonary
Pulmonary Agenesis sentations picked up over a period of 4 years. These cases were suspected and then documented during life. B. Rajshekhar Case Reports Sunil Gomber Anurag Krishna* Five cases of pulmonary
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
WORKSHOP OF LUNG FUNCTION TEST. Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau
 WORKSHOP OF LUNG FUNCTION TEST Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau Big three in Respiratory Medicine Lung Function Test Chest imaging Bronchoscopy Table of Content Section
WORKSHOP OF LUNG FUNCTION TEST Dr. Lo Iek Long, Department of Respiratory Medicine, CHCSJ, Macau Big three in Respiratory Medicine Lung Function Test Chest imaging Bronchoscopy Table of Content Section
Chapter 24. Kyphoscoliosis. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 24 Kyphoscoliosis 1 A Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary
Chapter 24 Kyphoscoliosis 1 A Figure 24-1. Kyphoscoliosis. Posterior and lateral curvature of the spine causing lung compression. Excessive bronchial secretions (A) and atelectasis (B) are common secondary
Tubes and lines in neonatal chest radiograph
 Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Tubes and lines in neonatal chest radiograph Poster No.: C-1008 Congress: ECR 2014 Type: Educational Exhibit Authors: R. TUMMA, N. AHMED, V. Prasad ; Hyderabad/IN, 1 2 1 1 2 HYDERABAD, ANDHRA PRADESH/IN
Lung sequestration and Scimitar syndrome
 Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Lung sequestration and Scimitar syndrome Imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Rotterdam, The Netherlands Pulmonary sequestration Pulmonary sequestration (PS)
Lung Transplant Case Presentation
 Lung Transplant Case Presentation Errol L. Bush, MD Assistant Professor of Surgery Heart and Lung Transplantation UCSF Medical Center Update in Advanced Lung Disease May 9, 2015 LP 47y F never smoker w/
Lung Transplant Case Presentation Errol L. Bush, MD Assistant Professor of Surgery Heart and Lung Transplantation UCSF Medical Center Update in Advanced Lung Disease May 9, 2015 LP 47y F never smoker w/
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Congenital Lung Malformations: Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 51-60, Abr.-Jun., 2006 Congenital Lung Malformations: Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Imaging of the Lung in Children
 Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
Imaging of the Lung in Children Imaging methods X-Ray of the Lung (Anteroposterior, ) CT, HRCT MRI USG Congenital developmental defects of the lungs Agenesis, aplasia, hypoplasia Tension pulmonary anomalies
Chapter 10 The Respiratory System
 Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Chapter 10 The Respiratory System Biology 2201 Why do we breathe? Cells carry out the reactions of cellular respiration in order to produce ATP. ATP is used by the cells for energy. All organisms need
Interpreting Spirometry. Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG
 RGN Respiratory Nurse Consultant G & W`CCG") Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
Interpreting Spirometry Vikki Knowles BSc(Hons) RGN Respiratory Nurse Consultant G & W`CCG Why Spirometry? supports diagnosis classifies defect - obstructive/restrictive assesses -severity of defect -
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Exam 1 Review. Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies
 Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Exam 1 Review Cardiopulmonary Symptoms Physical Examination Clinical Laboratory Studies WBC Count Differential A patient had been admitted to the hospital for acute shortness of breath. A CXR examination
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Case Presentation. Alireza Sadeghi MD Lutheran Medical Center University Hospital of Brooklyn Downstate Medical Center March 10 th 2006
 Case Presentation Alireza Sadeghi MD Lutheran Medical Center University Hospital of Brooklyn Downstate Medical Center March 10 th 2006 Case Presentation xx years old Caucasian Male History of Stage III
Case Presentation Alireza Sadeghi MD Lutheran Medical Center University Hospital of Brooklyn Downstate Medical Center March 10 th 2006 Case Presentation xx years old Caucasian Male History of Stage III
The Goal of the Respiratory Assessment. Two Parts of the Respiratory Assessment
 The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
The Respiratory System Respiratory Assessment of the Adult Patient Mary Douglas, MSN, RN Nurse Educator Minneapolis VA Health Care System Respiratory system: moves oxygen into the body and carbon dioxide
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Anatomy. The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs.
 Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Respiratory System Anatomy The respiratory system starts from the nose, mouth, larynx, trachea, and the two lungs. Within the lungs, the bronchi transport air with oxygen to the alveoli on inspiration
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital
 Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
Prapaporn Pornsuriyasak, M.D. Pulmonary and Critical Care Medicine Ramathibodi Hospital Only 20-30% of patients with lung cancer are potential candidates for lung resection Poor lung function alone ruled
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
Reporting SPECT-VQ. Alp Notghi
 Reporting SPECT-VQ Alp Notghi 20 year old female 24 weeks pregnant Clinical History : SOB and chest pain for past 3 days.?pe Doppler USS excluded DVT Case 4413041 Normal Case 4413041 CXR report: The heart
Reporting SPECT-VQ Alp Notghi 20 year old female 24 weeks pregnant Clinical History : SOB and chest pain for past 3 days.?pe Doppler USS excluded DVT Case 4413041 Normal Case 4413041 CXR report: The heart
Pulmonary Hypoplasia and Postnatal Lung Growth. Howard B. Panitch, M.D. Division of Pulmonary Medicine The Children s Hospital of Philadelphia
 Pulmonary Hypoplasia and Postnatal Lung Growth Howard B. Panitch, M.D. Division of Pulmonary Medicine The Children s Hospital of Philadelphia Pulmonary Hypoplasia CDH GO Lung Lesion (CPAM) PHP Enrollment
Pulmonary Hypoplasia and Postnatal Lung Growth Howard B. Panitch, M.D. Division of Pulmonary Medicine The Children s Hospital of Philadelphia Pulmonary Hypoplasia CDH GO Lung Lesion (CPAM) PHP Enrollment
Pneumothorax lecture no. 3
 Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Pneumothorax lecture no. 3 Is accumulation of air in a pleural space or accumulation of extra pulmonary air within the chest, Is uncommon during childhood, may result from external trauma, iatrogenic,
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Basic approach to PFT interpretation. Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic
 Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
Basic approach to PFT interpretation Dr. Giulio Dominelli BSc, MD, FRCPC Kelowna Respiratory and Allergy Clinic Disclosures Received honorarium from Astra Zeneca for education presentations Tasked Asked
HOSPITAL RECORD ABSTRACTION FORM
 HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
HOSPITAL RECORD ABSTRACTION FORM ID NUMBER: VERSION: A 10/23/2015 0a. Form Completion Date... / / 0b. Staff Code... 0c. Event ID: 0d. Event Date: / / Instructions: Answers are derived from the medical
Objectives. Pulmonary Assessment 12/13/2017
 Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Pulmonary Assessment Reid Blackwelder, MD, FAAFP Professor and Chair, Family Medicine Quillen Colege of Medicine, ETSU Objectives Understand anatomy and physiology of pulmonary assessment techniques Remember
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days
 1 week b) 24 days") Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
Semiology of respiratory system in children Simple choice 1. Mark the intrauterine age of lung development onset from the gut: a) 1 week b) 24 days c) 6 weeks d) 12 weeks e) 35 weeks 2. Stridor is not
63-year old female with dyspnea
 Indiana University Pulmonary and Critical Care Fellowship Fellows Case Archive Case #1 63-year old female with dyspnea Gabriel Bosslet, MD; Chadi Hage MD A 63-year-old female presented to pulmonary clinic
Indiana University Pulmonary and Critical Care Fellowship Fellows Case Archive Case #1 63-year old female with dyspnea Gabriel Bosslet, MD; Chadi Hage MD A 63-year-old female presented to pulmonary clinic
X-Rays. Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady
 X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
X-Rays Prepared by Prof.Dr. Magda Hassab Allah Assist.lecturer Marwa Al Hady CHEST X-RAYS Normal Chest X-ray Comments on chest X ray includes examination of 1- Bony cage (ribs,clavicles &vertebral column
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology
 Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
Title: Spirometry Teacher : Dorota Marczuk Krynicka, MD., PhD. Coll. Anatomicum, Święcicki Street no. 6, Dept. of Physiology I. Measurements of Ventilation Spirometry A. Pulmonary Volumes 1. The tidal
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
A Case of Pediatric Plasma Cell Granuloma
 August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
August 2001 A Case of Pediatric Plasma Cell Granuloma Nii Tetteh, Harvard Medical School Year IV Our Patient 8 year old male with history of recurrent left lower lobe and lingular pneumonias since 1994.
REQUISITION FOR DIAGNOSTIC SERVICES
 2300 McPhillips Street, Winnipeg, Manitoba R2V 3M3 REQUISITION FOR DIAGNOSTIC SERVICES PATIENT NAME ADDRESS BIRTH M.H.# P.H.I.N.# TELEPHONE HOME BUSINESS MALE FEMALE POSTAL CODE HOSPITAL USE ONLY ACCOUNT
2300 McPhillips Street, Winnipeg, Manitoba R2V 3M3 REQUISITION FOR DIAGNOSTIC SERVICES PATIENT NAME ADDRESS BIRTH M.H.# P.H.I.N.# TELEPHONE HOME BUSINESS MALE FEMALE POSTAL CODE HOSPITAL USE ONLY ACCOUNT
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
Diseases of the Lung and Respiratory Tract, Part I. William Bligh-Glover M.D. Department of Anatomy, CWRU
 Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
Diseases of the Lung and Respiratory Tract, Part I William Bligh-Glover M.D. Department of Anatomy, CWRU Educational objectives: Distinguish the types of atelectasis and their etiologies Distinguish the
PULMONARY MEDICINE BOARD REVIEW. Financial Conflicts of Interest. Question #1: Question #1 (Cont.): None. Christopher H. Fanta, M.D.
: None. Christopher H. Fanta, M.D.") PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
PULMONARY MEDICINE BOARD REVIEW Christopher H. Fanta, M.D. Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Financial Conflicts of Interest
disease, bronchopulmonary dysplasia, pulmonary hypoplasia and congenital diaphragmatic hernia.
 Neonatal Chest Imaging - What the Nurse Should Know Expires Monday, April 30, 2018 Nursing Michael J. Diament, M.D. Objectives 1. Describe a good technique for positioning a neonate for the purpose of
Neonatal Chest Imaging - What the Nurse Should Know Expires Monday, April 30, 2018 Nursing Michael J. Diament, M.D. Objectives 1. Describe a good technique for positioning a neonate for the purpose of
Anatomy & Physiology 2 Canale. Respiratory System: Exchange of Gases
 Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Anatomy & Physiology 2 Canale Respiratory System: Exchange of Gases Why is it so hard to hold your breath for Discuss! : ) a long time? Every year carbon monoxide poisoning kills 500 people and sends another
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
-Tamara Wahbeh. -Razan Abu Rumman. Dr. Mohammed Al-Muhtaseb
 -2 -Tamara Wahbeh -Razan Abu Rumman Dr. Mohammed Al-Muhtaseb I tried to include everything the doctor mentioned in both the lecture and his slides in the simplest way possible, so hopefully there would
-2 -Tamara Wahbeh -Razan Abu Rumman Dr. Mohammed Al-Muhtaseb I tried to include everything the doctor mentioned in both the lecture and his slides in the simplest way possible, so hopefully there would
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Pediatric Pulmonology Content Outline
 Pediatric Pulmonology Content Outline In-Training, Initial Certification, and Maintenance of Certification Exams Effective for exam administered beginning November 1, 2018 THE AMERICAN BOARD of PEDIATRICS
Pediatric Pulmonology Content Outline In-Training, Initial Certification, and Maintenance of Certification Exams Effective for exam administered beginning November 1, 2018 THE AMERICAN BOARD of PEDIATRICS
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Pulmonary Function Test
 Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Spirometry: Introduction Dr. Badri Paudel GMC Spirometry Pulmonary Function Test! Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after
Pitfalls of the Pediatric Chest and Abdomen SPR 2017
 Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pitfalls of the Pediatric Chest and Abdomen SPR 2017 Richard I. Markowitz, MD, FACR Children s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania No Disclosures Cognitive Perceptual
Pulmonary Function Testing. Ramez Sunna MD, FCCP
 Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Pulmonary Function Testing Ramez Sunna MD, FCCP Lecture Overview General Introduction Indications and Uses Technical aspects Interpretation Patterns of Abnormalities When to perform a PFT 1. Evaluation
Reducing lung volume in emphysema Surgical Aspects
 Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
Reducing lung volume in emphysema Surgical Aspects Simon Jordan Consultant Thoracic Surgeon Royal Brompton Hospital Thirteenth Cambridge Chest Meeting April 2015 Surgical aspects of LVR Why we should NOT
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it