Mitral club: From clinical practice to guidelines: the world upside down
|
|
|
- Vincent McKenzie
- 6 years ago
- Views:
Transcription
1 Mitral club: From clinical practice to guidelines: the world upside down Christina Chrysohoou Heart Failure Unit 1rst Cardiology Clinic, University of Athens Hippokratio Hospital, Greece

2 Stages of Chronic MR 2017 AHA/ACC Focused Update on VHD
3 Stages of Chronic MR The best therapy for chronic secondary MR is not clear because MR is only 1 component of the disease, with clinical outcomes also related to severe LV systolic dysfunction, coronary disease, idiopathic myocardial disease, or other diseases affecting the heart muscle There are instances in which both primary and secondary MR are present. In patients with secondary MR, compared with primary MR, adverse outcomes are associated with a smaller calculated effective regurgitant orifice N Engl J Med. 2016;374:
4 Why secondary MR has worse prognosis? Severity of secondary MR may increase over time because of the associated progressive LV systolic dysfunction Doppler methods for calculations of effective regurgitant orifice area by the flow convergence method may underestimate severity because of the crescentic shape of the regurgitant orifice, and multiple parameters must be used to determine the severity of MR Even so, on the basis of the criteria used for determination of severe MR in RCTs of surgical intervention for secondary MR, the recommended definition of severe secondary MR is now the same as for primary MR (effective regurgitant orifice 0.4 cm2 and regurgitant volume 60 ml), with the understanding that effective regurgitant orifice cutoff of >0.2 cm2 is more sensitive and >0.4 cm2 is more specific for severe MR Am Coll Cardiol. 2000;36:
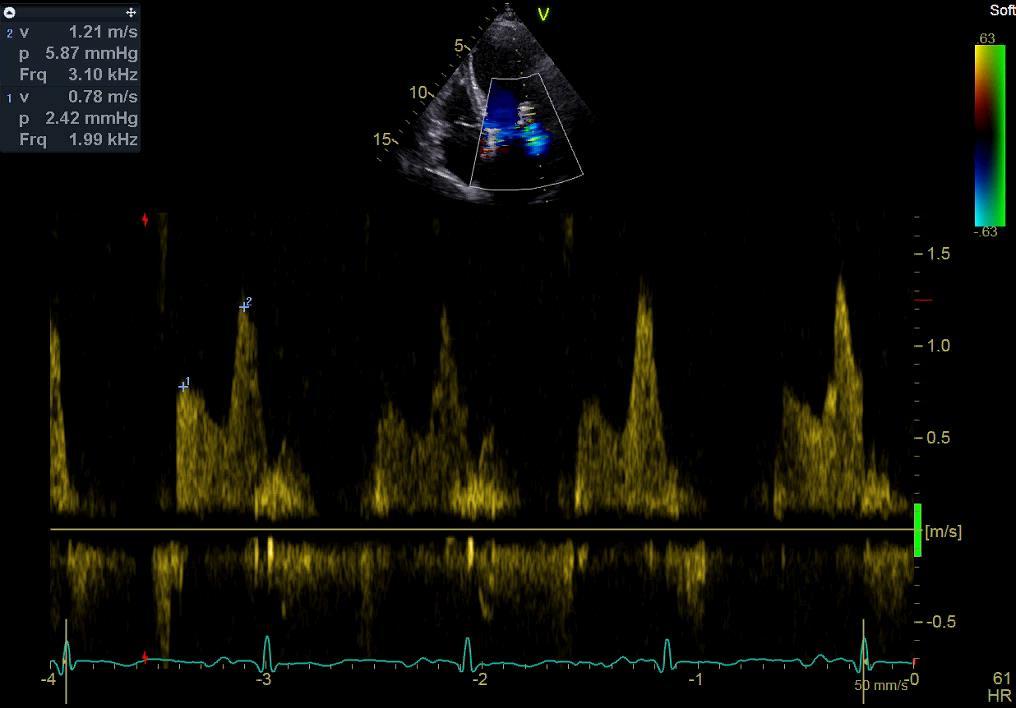
5 MR quantification comments.. Quantitative parameters for severe MR included RF >50%, RVol >60 ml, and EROA >0.4 cm2. These values were derived from a single-center observational study comparing RVol and EROA calculated by the proximal isovelocity surface area (PISA) method, quantitative Doppler, or the average of both methods to angiographic grading in 180 consecutive patients (Circulation 1997;96: ). LV angiography and echocardiography were performed within 3 months of each other. JA C C V O L. 6 4, N O. 2 5,
6

7 Chronic Primary MR -Recommendations Nishimura, et al AHA/ACC Focused Update on VHD
8 Ανεπάρκεια μιτροειδούς βαλβίδας Αναστολείς νευροορμονικού άξονα CRT Χειρουργική αντιμετώπιση Mitral clip
 because MR cannot exceed 100% of total LV stroke An underappreciated dependence of both EROA and RVol on LVEDV is")
9 Hemodynamic Considerations An EROA >0.6 cm2 is nearly impossible in secondary MR (unless the LV is extremely large) because MR cannot exceed 100% of total LV stroke An underappreciated dependence of both EROA and RVol on LVEDV is evident, such that an EROA of 0.2 cm2 can be associated with RF >50% when LVEDV is normal, but is typically 0.3 cm2 at moderately dilated LVEDV values (220 to 240 ml) typical of most clinical trials in heart failure. Only at very large LVEDV values is EROA 0.4 cm2 associated with RF >50%. J A C C V O L. 6 4, N O. 2 5,

10 Hemodynamic Considerations Furthermore, the relationship between EROA and LVEDV is influenced by the mean systolic pressure gradient between the LV and LA, with higher EROA values in decompensated HF patients with hypotension and elevated LA pressure compared with hypertensive patients with normal LA pressure. LVEF has an important role (60 ml RVol presumes LVEF is 40% or more and dilated LV ;RVol <30 ml can be associated with RF >50% in smaller ventricles or very low LVEF ) J Am Coll Cardiol 2013;62:e

11 The Dynamic Nature of Secondary MR EROA also varies notoriously with loading conditions, commonly seen during hypertensive crises and heart failure exacerbations. Functional MR severity changes over time with medical therapy, revascularization, and cardiac resynchronization therapy. The guidelines do not address how to approach the dynamic nature of secondary MR. Circulation 2011; Suppl:S Circulation 2011;124:912 9.

12 The gap between evidence (guidelines) and clinical practice Appropriate settings for optimal follow-up of these patients are not ubiquitous. A substantial number of patients are referred for surgery too late in the disease course with longstanding and advanced symptoms, resulting in increased operative risk and suboptimal long-term outcomes. Stated reasons for deferring surgery, such as older age, co-morbidities, and poor left ventricular (LV) function, illustrate the knowledge gap in the management of VHD as many of these are not considered contraindications to valve intervention. In the Euro Heart Survey, surgery was denied to 33% of elderly patients with severe symptomatic aortic stenosis and to 50% of patients with severe symptomatic mitral regurgitation; a high proportion of patients with symptomatic VHD were, thus, inappropriately treated medically. European Heart Journal (2013) 34,
 of patients, whereas 53% (577 of 1,095) of patients were unoperated and medically managed Over a mean follow-up period of 4.")
13 Prevalence and Outcomes of Unoperated Patients With Severe Symptomatic MR and Heart Failure In 5,737 patients, FMR (74%) and degenerative MR (DMR) (21%) were the predominant mechanisms of MR. MV surgery was performed in 47% (518 of 1,095) of patients, whereas 53% (577 of 1,095) of patients were unoperated and medically managed Over a mean follow-up period of 4.5 years, ACE-I (31% to 63%), ARB(13% to 25%), BB(35% to 82%), and MRA(13% to 33%). CRT (17%), PCI (10%). JACC Vol. 63, No. 2, 2014
14 Independent prognostic value of functional mitral regurgitation in patients with heart failure Severe FMR was defined quantitatively as ERO>0.2 cm2 or RV>30 ml or VC>0.4 cm. FMR is strongly associated with outcome after adjustment for LVEF and restrictive mitral filling pattern (Dec E<140msec) in patients with both ischaemic and nonischaemic DCM. Heart 2011;97:1675e1680

15 Prognostic implications of functional mitral regurgitation according to the severity of the underlying chronic heart failure: a long-term outcome study Acker et al. found that in dilated hearts, mitral valve repair had effects only in modest LV remodeling. Similarly, Braun et al. demonstrated in a cohort of patients with ischaemic mitral regurgitation that LV reverse remodelling occurred in the group with an LV end-diastolic diameter <65 mm, while no benefit was demonstrated for patients with an LV end-diastolic diameter >65 mm FMR was independently associated with increased risk of death and heart transplantation in patients with less severe CHF symptoms and in patients at lower overall risk. European Journal of Heart Failure (2010) 12, Thorac Cardiovasc Surg 2006;132: , e561 e564. Ann Thorac Surg 2008;85: , discussion


16 Percutaneous mitral valve repair: The last chance for symptoms improvement in advanced refractory chronic heart failure? Seventy-five consecutive patients with FMR grade 3+ and severe HF symptoms despite optimal medical therapy and CRT underwent PMVR with the MitraClip system (mean age: 67±11 yrs, logeuroscore =23±18%, LVEF= 30±9%). Int J of Cardiol 228 (2017)


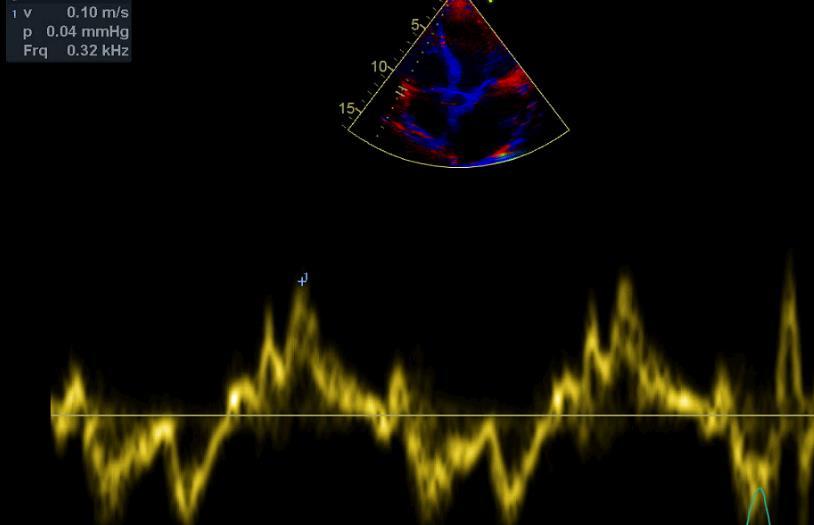
17 Ασθενής 60 ετών, CABG, CRT-D, EF=20%, συχνές νοσηλείες με οιδήματα ανά σάρκα, ασκίτη, ισχαιμική ηπατίτιδα ΟΝΑ, εκφορτίσεις απινιδωτή, σοβαρή MVR
18 Day 1st 2nd 4th 5th 6th 7th 8th Hb Ht Glu Urea Creat UA Na/K 127/ /3,9 128/3,7 131/3,8 130/3,6 129/3,3 131/3,8 γgt Billirubin SGOT/SGPT 1286/ / / / / / /212 ΒΝΡ pg/ml Med treat Lasix 180 ιv Aldactone 50mg, noradrenaline 5μg/Kg/min ACE, b blocker was discontinued. Lasix 180 ιv Aldactone 50 Noradrenaline, dobutamine, N/S Indapamide 2.5mg Lasix ; Aldactone, noradrenaline, dobutamine, N/S Indapamide 2.5mg Lasix ; Aldactone, noradrenaline, dobutamine, N/S Lasix 120mg indapamide Aldactone 50, Levosimemdan 0.1 μg/kg/min, carvedilol Lasix 120mg, indapamide Aldactone 50, carvedilol Lasix 120mg, indapamide Aldactone, noradrenaline, levosimendan, V urine (ml) Weight (kg)

19 23/08/2016 ΝΥΗΑ Ι-ΙΙ, 80 mg furosemide, eplerenone 25 mg, carvedilol 25 mg, valsartan 40-60mg Creatinine=1.9 mg/dl
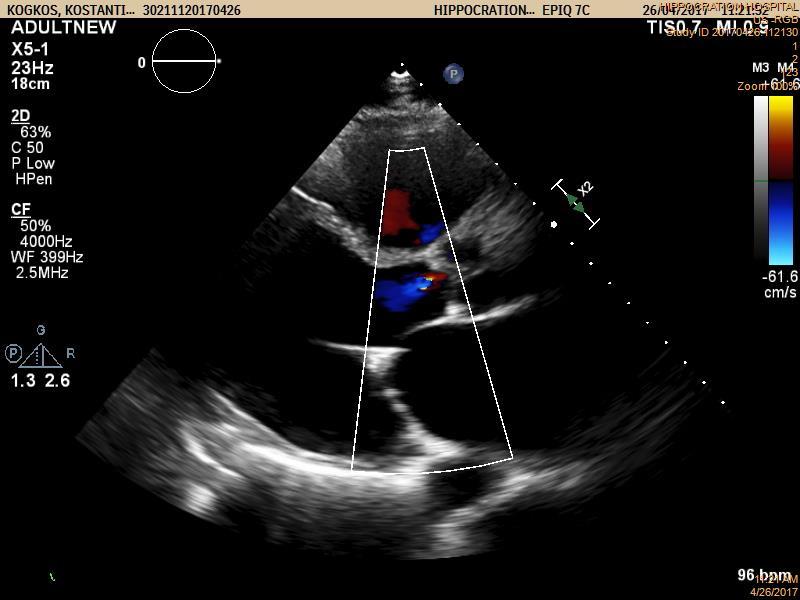

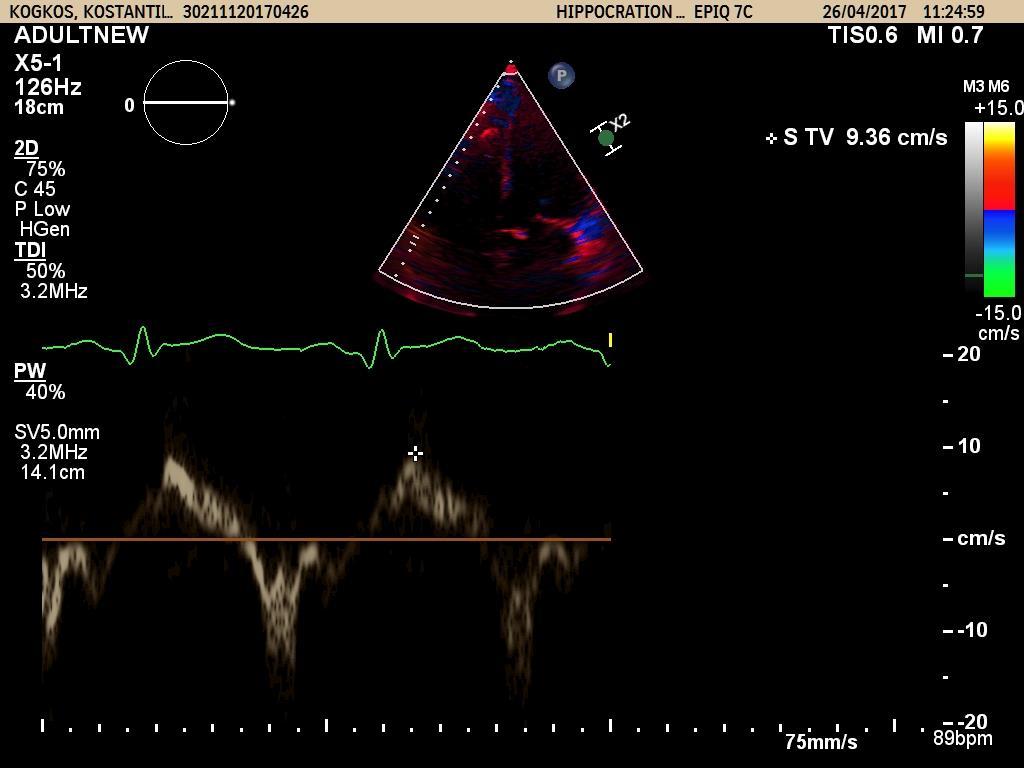
20 Επανελεγχος 26/4/2017 σε ΝΥΗΑ ΙΙ

21 Your text here

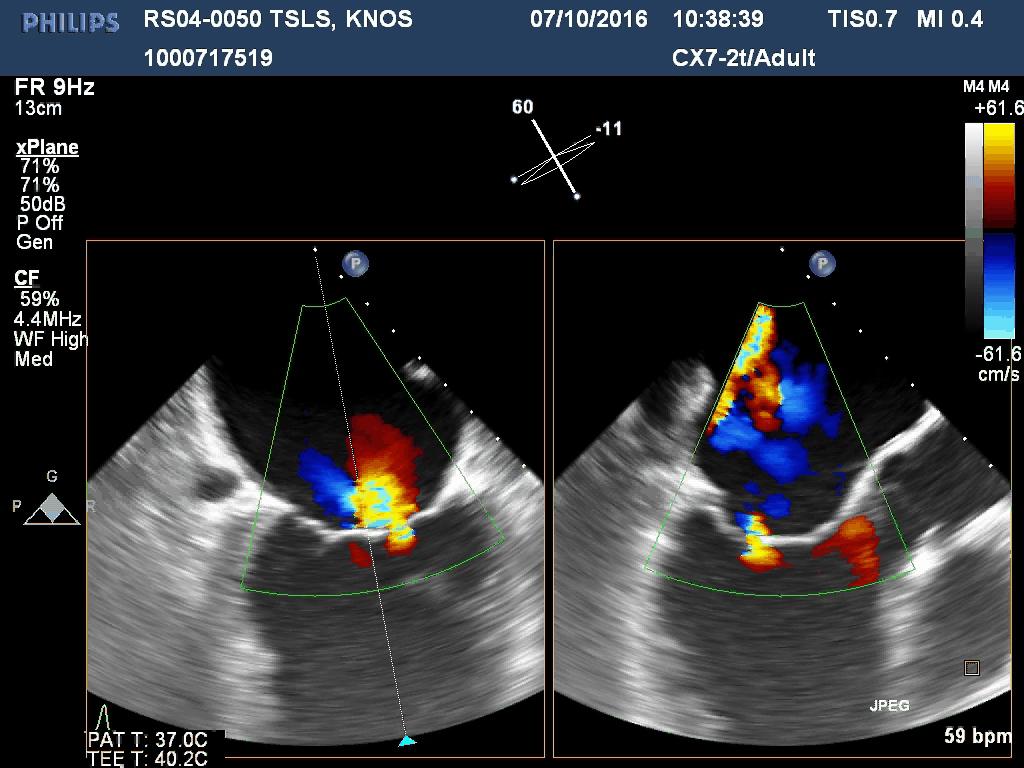
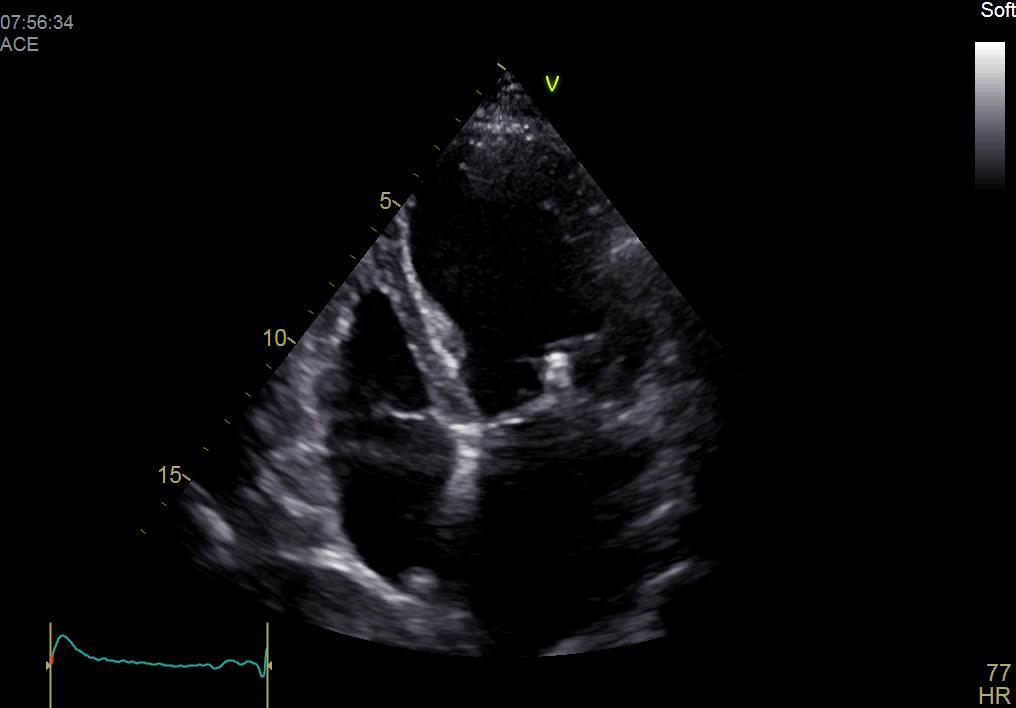
22 Ασθενής 77 ετών με χειρουργηθείσα στεφανιαια νόσο, ΝΥΗΑ IV, υπο πλήρη φαρμακευτικη αγωγή με συχνές μηνιαίες νοσηλείες για απορρύθμιση κλινικού σταδίου. ΚΕ=30%, πνευμονική υπέρταση, Σοβαρή MR M Chrysocheris
23


24
25

26 Percutaneous mitral valve repair

27 From: Secondary Mitral Regurgitation in Heart Failure: Pathophysiology, Prognosis, and Therapeutic Considerations Secondary MR in Heart Failure: Interaction Between the Etiology of MR and the Relative Success Rates of MV Surgery and MitraClip in the Randomized EVEREST II Trial Success was defined as freedom from the combined outcome of death, MV surgery, or reoperation, or MR >2+ (echocardiographic core laboratory determination). Adapted with permission from Feldman et al. (88) and Mauri et al. (89). EVEREST II = Endovascular Valve Edge-to-Edge REpair Study; MR = mitral regurgitation; MV = mitral valve. Date of download: 10/3/2015 JACC 2015;65(12):
28 The MITRACLIP evidence base: Trials and Registries The EndovalvularValve Edge-to-Edge Repair Study (EVEREST) phase I study enrolled 107 low-risk patients with either primary or secondary MR and established the safety and efficacy of MitraClip, although 25% underwent surgery at 3 years because of recurrent MR The EVEREST II study randomized 279 low-to intermediate-risk patients in a 2 : 1 fashion to either MitraClip or isolated mitral surgery. Patients had either primary (73%) or secondary (27%) MR and had conventional indications for surgery;. At 5-year follow-up, there was no difference in survival between the MitraClip and surgical arms for either primary or secondary MR. However, freedom from surgery was significantly worse in primary MR patients assigned to MitraClip (69 vs. 95%), whereas no difference was seen in those with secondary MR Patients with a successful index MitraClip procedure had similar freedom from surgery to the surgical arm, highlighting the importance of patient selection and operator experience in procedural outcomes.
; type IIIb, restricted leaflet motion in systole, seen in ischemic cardiomyopathy.")
29 Spectrum of diseases treatable with MitraClip Carpentier type I, normal leaflet motion with annular dilation; type II, increased leaflet motion (leaflet prolapse or flail); type IIIb, restricted leaflet motion in systole, seen in ischemic cardiomyopathy. Eur Heart J 2011; 32:


30 Mitral clip clinical trials
31 A Randomized Study of the MitraClip Device in Heart Failure Patients With Clinically Significant Functional Mitral Regurgitation (RESHAPE- HF) This trial is a randomized study of the MitraClip device in heart failure patients with clinically significant functional mitral regurgitation. A hierarchical composite of allcause mortality and recurrent heart failure hospitalizations is hypothesized to occur at a lower rate with the use of the MitraClip device in addition to optimal standard medical therapy compared to optimal standard of care therapy alone.
32
33 More mitral-clip evidence A recent meta-analysis of 875 patients from nine studies investigated the impact of MitraClip on secondary MR. On an average, 1.48 clips were implanted/patient and after a median follow-up of 9 months, 78% were NYHA I/II and 89% had less than 2þ mitral regurgitation, with 15% mortality. Moreover, 6-min walk test improved by 100 m, and a significant reduction in LV volumes and pulmonary pressures was seen. Increased LV systolic volumes at baseline were associated with a significant reduction in volumes after MitraClip, whereas baseline atrial fibrillation reduced the positive effect of MitraClip on ejection fraction and LV volumes. Am J Cardiol 2015;116:
34 A meta-analysis of MitraClip system versus surgery for treatment of severe mitral regurgitation Mortality reoperation Patients in the MitraClip group were older, had a higher EuroSCORE and a lower LVEF at baseline. The number of patients with post-procedure residual MR severity >2 was significantly higher in the MitraClip Ann Cardiothorac Surg 2013;2(6):

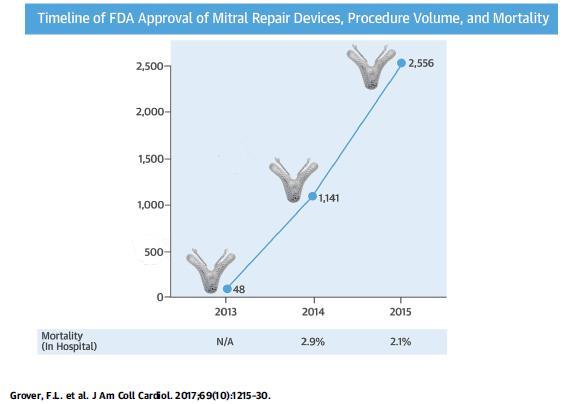
35 Mitral clip in clinical practice JACC VOL. 6 9, NO. 1 0,
36
37


 J A C C : C A R D I O V A S C U L A R I M A G I N G, V O L.")
38 Role of Echocardiography in Percutaneous Mitral Valve Interventions Assessing the mechanism of MR Quantitating the severity of MR Guiding transseptal crossing Aligning the delivery system perpendicular to the mitral plane at the location of the MR jet Alignment of clip s arms perpendicular to MV coaptation line Determining success of grasping both leaflets Verification of clip stability after release from delivery system Reassessing MR severity Locating of persistent leak(s) J A C C : C A R D I O V A S C U L A R I M A G I N G, V O L. 5, N O. 7,
39 Predictors of outcome in patients undergoing MitraClip implantation: An aid to improve patient selection The 2-year survival was 81%. Predictors for two-year mortality in multivariate analysis were : Baseline NT-proBNP 5000 μg/l (HR: 5.4, 95% CI: ), Previous valve surgery (HR: 4.5, 95% CI: ), Tricuspid regurgitation (TR) grade 3 prior tomci (HR: 2.8, 95% CI: ) and Absence of MR reduction after MCI (HR: 2.1, 95% CI: ). The 2-year survival of patients with 0, 1 or 2 of these predictors was: 87%; 78% and 38% IJC:189 (2015)
40 Conclusions Mitral valve surgery is recommended in patients with severe symptomatic MR. Quantification of MR severity is an imperfect art The role of MV surgery is unclear in patients with severe MR secondary to left ventricular dysfunction. (the heart is sick) The current class IIb recommendation for MV surgery in the presence of LV dysfunction is based on lack of survival benefit and a high recurrence rate of MR Many patients with severe MR are at high surgical risk due to advanced age, LV dysfunction, or comorbidities. The MitraClip device provides a novel percutaneous option for patients with severe MR with significant improvement (less re-hospitalizations) Recent data from the MitraClip device clinical trials show significant LV and LA remodeling in secondary MR when MR is reduced from severe (as previously defined) to either mild or moderate Circulation 2013;128:
Prognostic Impact of FMR
 Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Secondary Mitral Valve Regurgitation in Heart Failure, Age 60 Years From Medical Therapy to Surgical Repair to Transcatheter Intervention The Interventionalist s View Samin K Sharma, MD, FACC, FSCAI Director
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair
 Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Percutaneous Mitral Valve Repair MitraClip: Procedure, Data, Patient Selection Chad Rammohan, MD FACC Director, Cardiac Cath Lab El Camino Hospital Mountain View, California Mitral Regurgitation MitraClip
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ
 Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Τελικά επιδιόρθωση, αντικατάσταση ή clip στην ισχαιμική ανεπάρκεια Μιτροειδούς; ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ Carpentier MV Classification- Leaflet Mobility Normal Increased Decreased Mobility
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Catheter-based mitral valve repair MitraClip System
 Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Percutaneous Mitral Valve Repair: Results of the EVEREST II Trial William A. Gray MD Director of Endovascular Services Associate Professor of Clinical Medicine Columbia University Medical Center The Cardiovascular
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT
 Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Transcatheter Mitral Valve Repair and Replacement: Where is the Latest Randomized Evidence Taking US Mitral-Fr, COAPT and Saibal Kar, MD, FACC, FSCAI Professor of Medicine Director of Interventional Cardiac
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC
 TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
TREATMENT OF MITRAL REGURGITATION RAJA NAZIR FACC NATURAL HISTORY OF MITRAL REGURGITATION Abdallah El Sabbagh et al. JIMG 2018;11:628-643 TREATMENT OPTIONS SURGERY REPAIR REPLACEMENT PERCUTANEOUS INTERVENTIONS
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL
 PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
PERCUTANEOUS MITRAL VALVE THERAPIES 13 TH ANNUAL CARDIAC, VASCULAR AND STROKE CARE CONFERENCE PIEDMONT ATHENS REGIONAL DISCLOSURES I WILL BE DISCUSSING OFF-LABEL USAGE OF DEVICES RELATED TO TMVR OBJECTIVES
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream
 Going Mainstream") The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ;
 CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
CLIP ΜΙΤΡΟΕΙ ΟΥΣ: ΠΟΥ ΒΡΙΣΚΟΜΑΣΤΕ; Επιµορφωτικά Σεµινάρια Ειδικευοµένων Καρδιολογίας 7 Απριλίου 2012 M Chrissoheris MD FACC THV Department HYGEIA Hospital Degenerative MR (DMR) Usually refers to an anatomic
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Burden of Mitral Regurgitation (MR) in the US Why is This Important?
 in the US Why is This Important?") Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Secondary (Functional) Mitral Regurgitation as a Target for Heart Failure Therapy William T. Abraham, MD, FACP, FACC, FAHA, FESC, FRCP Professor of Medicine, Physiology, and Cell Biology Chair of Excellence
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Management of TR in Patients Undergoing Mitral Interventions
 Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Management of TR in Patients Undergoing Mitral Interventions Stephen H. Little, MD John S. Dunn Chair in Cardiovascular Research and Education, Associate professor, Weill Cornell Medicine shlittle@houstonmethodist.org
Mitral Valve Disease, When to Intervene
 Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Mitral Valve Disease, When to Intervene Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Current ACC/AHA guideline Stages
Steven F Bolling Professor of Cardiac Surgery University of Michigan
 Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Optimal Treatment of Functional MR Steven F Bolling Professor of Cardiac Surgery University of Michigan Functional MR Functional MR in Ischemia Badhwar, Bolling, chapter in: Advances in Heart Failure,
Mitral Regurgitation
 Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
Mitral Regurgitation Focus on Percutaneous Repair Steven J. Yakubov, MD FACC FSCAI System Chief, Structural Heart Diseaese, OhioHealth John H. McConnell Chair of Advanced Structural Heart Disease Medical
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F.
 Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Minimally invasive therapies for the mitral valve: How will you incorporate into your clinical practice? Guilherme F. Attizzani, MD UH Harrington Heart and Vascular Institute Interventional Cardiologist/Structural
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain
 Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Disclosure Statement of Financial Interest Saibal Kar, MD, FACC
 MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
MitraClip Therapy Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Program Director, Interventional Cardiology Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP
 ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
ΔΙΑΔΕΡΜΙΚΗ ΑΝΤΙΜΕΤΩΠΙΣΗ ΔΟΜΙΚΩΝ ΠΑΘΗΣΕΩΝ: Ο ΡΟΛΟΣ ΤΗΣ ΑΠΕΙΚΟΝΙΣΗΣ ΣΤΟ ΑΙΜΟΔΥΝΑΜΙΚΟ ΕΡΓΑΣΤΗΡΙΟ ΣΤΗΝ ΤΟΠΟΘΕΤΗΣΗ MITRACLIP ΒΛΑΣΗΣ ΝΙΝΙΟΣ MD MRCP ΚΛΙΝΙΚΗ ΑΓΙΟΣ ΛΟΥΚΑΣ ΘΕΣΣΑΛΟΝΙΚΗ CONFLICT OF INTEREST PROCTOR
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott. Chairperson: M. Haude Panellists: A. Al Nooryani, M.
 Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
Transcatheter Mitral Valve Repair: today and tomorrow Sponsored by Abbott Chairperson: M. Haude Panellists: A. Al Nooryani, M. Al Otaiby Session objectives To learn about the clinical patient profile for
I have financial relationships to disclose Honoraria from: Edwards
 I have financial relationships to disclose Honoraria from: Edwards Mitral Valve Annuloplasty in Ischemic Mitral regurgitation Jean François Avierinos Hôpital Timone Marseille August 28, 2012 Ischemic MR
I have financial relationships to disclose Honoraria from: Edwards Mitral Valve Annuloplasty in Ischemic Mitral regurgitation Jean François Avierinos Hôpital Timone Marseille August 28, 2012 Ischemic MR
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας
 Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Χειρουργική Αντιμετώπιση της Ανεπάρκειας της Μιτροειδούς Βαλβίδας Dr Χρήστος ΑΛΕΞΙΟΥ MD, PhD, FRCS(Glasgow), FRCS(CTh), CCST(UK) Consultant Cardiothoracic Surgeon Normal Mitral Valve Function Mitral Regurgitation
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Outline 9/17/2016. Advances in Percutaneous Mitral Valve Repair and Replacement. Scope of the Problem and Guidelines
 Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Advances in Percutaneous Mitral Valve Repair and Replacement Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando,
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Functional Mitral Regurgitation
 Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Club 35 - The best in heart valve disease - Functional Mitral Regurgitation Steven Droogmans, MD, PhD UZ Brussel, Jette, Belgium 08-12-2011 Euroecho & other Imaging Modalities 2011 No conflicts of interest
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA
 & FDA") Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas, Nevada December 8 11 th, 2013 Ted Feldman MD, FACC, FESC,
Status Of The MitraClip: Trials (EVEREST II & COAPT) & FDA Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital SCAI Fall Fellows Course Las Vegas, Nevada December 8 11 th, 2013 Ted Feldman MD, FACC, FESC,
Use of MitraClip Beyond Everest Criteria
 Use of MitraClip Beyond Everest Criteria Takashi Matsumoto, MD Sendai Kousei Hospital Sendai, Japan No Disclosure of Financial Interest Introduction The efficacy and safety of the MitraClip therapy was
Use of MitraClip Beyond Everest Criteria Takashi Matsumoto, MD Sendai Kousei Hospital Sendai, Japan No Disclosure of Financial Interest Introduction The efficacy and safety of the MitraClip therapy was
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
GDMT for percutaneous mitral valve repair
 GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
GDMT for percutaneous mitral valve repair Ted Feldman, M.D., MSCAI FACC FESC Evanston Hospital The 11th Annual Innovations & Trends in Cardiovascular Care New Brunswick, NJ October 18 th 2014 Ted Feldman
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
What is the Role of Surgical Repair in 2012
 What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
What is the Role of Surgical Repair in 2012 The Long-Term Results of Surgery Raphael Rosenhek Department of Cardiology Medical University of Vienna European Society of Cardiology 2012 Munich, August 27th
Functional Mitral Regurgitation; therapeutic continuum overview. Michele Senni. Cardiologia 1 Scompenso e Trapianti di Cuore A.O. PAPA GIOVANNI XXIII
 Functional Mitral Regurgitation; therapeutic continuum overview Michele Senni Cardiologia 1 Scompenso e Trapianti di Cuore A.O. PAPA GIOVANNI XXIII Functional Mitral Regurgitation FMR is not the result
Functional Mitral Regurgitation; therapeutic continuum overview Michele Senni Cardiologia 1 Scompenso e Trapianti di Cuore A.O. PAPA GIOVANNI XXIII Functional Mitral Regurgitation FMR is not the result
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
The Key Questions in Mitral Valve Interventions. Where Are We in 2018?
 The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
The Key Questions in Mitral Valve Interventions Where Are We in 2018? Gilles D. DREYFUS, MD, FRCS, FESC Professor of Cardiothoracic Surgery 30 GIORNATE CARDIOLOGICHE TORINESI - OCT 2018 Are guidelines
Case Report. Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure. Introduction. Case Report. Keywords
 Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure Petherson Susano Grativvol, 1,2 Katiuska Massucatti Grativvol, 1,2 Alberto de Paula Nogueira Jr., 1,2 João Eduardo Tinoco
Percutaneous Mitral Repair with MitraClip as an Adjunct Therapy of Heart Failure Petherson Susano Grativvol, 1,2 Katiuska Massucatti Grativvol, 1,2 Alberto de Paula Nogueira Jr., 1,2 João Eduardo Tinoco
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
MitraClip World Wide Commercial Experience
 MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral
MitraClip World Wide Commercial Experience Valves Repaired. Lives Improved. Carlos G. Hernandez, MBA Sr. Product Manager, Strategic Planning Abbott Vascular October, 2014 MitraClip Transcatheter Mitral
MitraClip in the ICCU: Which Patient will Benefit?
 MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
MitraClip in the ICCU: Which Patient will Benefit? DAVID MEERKIN STRUCTURAL A ND CONGENITAL HEART DISEASE UNIT SHAARE ZEDEK MEDICAL CENTER JERUSALEM Conflict of Interest No relevant disclosures Complex
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Percutaneous mitral valve repair: current techniques and results
 Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S.
 ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
ACC 2015 LBCT Outcomes of the Initial Experience with Commercial Transcatheter Mitral Valve Repair in the U.S. A report from the STS/ACC TVT Registry Paul Sorajja, MD, Saibal Kar, MD, Amanda Stebbins,
Current status: Percutaneous mitral valve therapy
 Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Current status: Percutaneous mitral valve therapy Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital ESC Stockholm 2010 Disclosures Research Grants Abbott, Edwards Consultant Abbott, Edwards 2 Percutaneous
Treatment for functional mitral regurgitation
 Transcatheter Leaflet Repair for Functional MR What will randomized trials mean for the future of mitral intervention? BY TED FELDMAN, MD, FESC, FACC, MSCAI; PAUL SORAJJA, MD, FACC, FSCAI; PAUL GRAYBURN,
Transcatheter Leaflet Repair for Functional MR What will randomized trials mean for the future of mitral intervention? BY TED FELDMAN, MD, FESC, FACC, MSCAI; PAUL SORAJJA, MD, FACC, FSCAI; PAUL GRAYBURN,
Secondary MR joint with the mitral academy. What is new in our understanding of this disease? Luc Pierard University Hospital, Liège
 Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Secondary MR joint with the mitral academy What is new in our understanding of this disease? Luc Pierard University Hospital, Liège Faculty disclosure Luc Pierard I have no financial relationships to disclose.
Percutaneous Repair for MR:
 Percutaneous Repair for MR: Follow-up and longer term outcomes Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital 16th ANGIOPLASTY SUMMIT TCT Asia Pacific 2011 April 27-29 th Seoul, Korea Ted Feldman
Percutaneous Repair for MR: Follow-up and longer term outcomes Ted Feldman, M.D., FSCAI FACC FESC Evanston Hospital 16th ANGIOPLASTY SUMMIT TCT Asia Pacific 2011 April 27-29 th Seoul, Korea Ted Feldman
Treatment options in ischaemic mitral regurgitation: surgery, clips, devices?
 Treatment options in ischaemic mitral regurgitation: surgery, clips, devices? Francisco Leyva Conflicts of interest: FL has received advisory board fees from Medtronic Inc, Sorin, St Jude Medical and Abbot.
Treatment options in ischaemic mitral regurgitation: surgery, clips, devices? Francisco Leyva Conflicts of interest: FL has received advisory board fees from Medtronic Inc, Sorin, St Jude Medical and Abbot.
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Mitral Valve Disease. James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN
 Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
Mitral Valve Disease James Hermiller, MD, FACC, FSCAI St Vincent Heart Center Indianapolis, IN Disclosures Affiliation/Financial Relationship Consulting Fees/Honoraria Speaker Bureau Company Abbott, BSC,
PERCUTANEOUS MITRAL VALVE REPAIR IN HIGH RISK PATIENTS - THE SWISS EXPERIENCE AFTER THE FIRST 100 PATIENTS
 PERCUTANEOUS MITRAL VALVE REPAIR IN HIGH RISK PATIENTS - THE SWISS EXPERIENCE AFTER THE FIRST 100 PATIENTS Potential conflicts of interest Speaker s name: Daniel Sürder, MD Cardiocentro Ticino, Lugano
PERCUTANEOUS MITRAL VALVE REPAIR IN HIGH RISK PATIENTS - THE SWISS EXPERIENCE AFTER THE FIRST 100 PATIENTS Potential conflicts of interest Speaker s name: Daniel Sürder, MD Cardiocentro Ticino, Lugano
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII
 Bichat hospital University Paris VII") When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation
 Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Contemporary Management of Mitral Regurgitation Tailoring Treatment to The Patient Subset & Clinical Situation Hatim Al Lawati MD, FRCPC, FACC Consultant Interventional Cardiology Sultan Qaboos University
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy
 Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Dialysis-Dependent Cardiomyopathy Patients Demonstrate Poor Survival Despite Reverse Remodeling With Cardiac Resynchronization Therapy Evan Adelstein, MD, FHRS John Gorcsan III, MD Samir Saba, MD, FHRS
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Quality Outcomes Mitral Valve Repair
 Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
Quality Outcomes Mitral Valve Repair Moving Beyond Reoperation Rakesh M. Suri, D.Phil. Professor of Surgery 2015 MFMER 3431548-1 Disclosure Mayo Clinic Division of Cardiovascular Surgery Research funding
Guidelines in perspective?
 EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
EuroValve 2016 Challenges in the management Secondary MR Guidelines in perspective? Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology, Liège, Belgium Heart Valve Clinic,
Percutaneous Mitral Valve Repair
 Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Indiana Chapter of ACC November 15 th,2008 Percutaneous Mitral Valve Repair James B Hermiller, MD, FACC The Care Group, LLC St Vincent Hospital Indianapolis, IN Mechanisms of Mitral Regurgitation Mitral
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων. Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος
 Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
Surgical repair techniques for IMR: future percutaneous options?
 Surgical repair techniques for IMR: can this teach us about future percutaneous options? Genk - Belgium Prof. Dr. R. Dion KULeu Disclosure slide Robert A. Dion I disclose the following financial relationships:
Surgical repair techniques for IMR: can this teach us about future percutaneous options? Genk - Belgium Prof. Dr. R. Dion KULeu Disclosure slide Robert A. Dion I disclose the following financial relationships:
Intermittent inotropic infusions for the treatment of refractory end stage heart failure: a randomized clinical study
 Intermittent inotropic infusions for the treatment of refractory end stage heart failure: a randomized clinical study M. Bonios, J. Terrovitis, S. Drakos H. Pozios, F. Katsaros, C. Pantsios, J. Kanakakis,
Intermittent inotropic infusions for the treatment of refractory end stage heart failure: a randomized clinical study M. Bonios, J. Terrovitis, S. Drakos H. Pozios, F. Katsaros, C. Pantsios, J. Kanakakis,
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Next Generation Therapies: Aortic, Mitral and Beyond
 Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Next Generation Therapies: Aortic, Mitral and Beyond Scott M Lilly, MD PhD Medical (Interventional) Director, Structural Heart Program Heart Summit, Lima OH August 26 th, 2017 Next Generation Therapies:
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous mitral valve leaflet repair for mitral regurgitation Mitral regurgitation
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of percutaneous mitral valve leaflet repair for mitral regurgitation Mitral regurgitation
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Imaging in dilated cardiomyopathy : factors associated with a poor outcome
 Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Imaging in dilated cardiomyopathy : factors associated with a poor outcome Johan De Sutter, MD, PhD, FESC AZ Maria Middelares Gent and University Gent - Belgium Dilated cardiomyopathy Cardiomyopathy with
Euro Heart Survey New Programme Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI
 Carlo Di Mario, London, UK President EAPCI") Euro Heart Survey New Programme 2009-2012 Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI Alan Cribier, Rouen, France Andreas Gruentzig Award 2010 Cardiogenic
Euro Heart Survey New Programme 2009-2012 Sentinel Registry Transcatheter Valve Treatment (TCVT) Carlo Di Mario, London, UK President EAPCI Alan Cribier, Rouen, France Andreas Gruentzig Award 2010 Cardiogenic
Simultaneous Double Clipping Delivery Guide Strategy for Treatment of Severe Coaptation Failure in Functional Mitral Regurgitation
 Heart, Lung and Circulation (2015) 24, 98 102 1443-9506/04/$36.00 http://dx.doi.org/10.1016/j.hlc.2014.09.008 HOW-TO-DO-IT Simultaneous Double Clipping Delivery Guide Strategy for Treatment of Severe Coaptation
Heart, Lung and Circulation (2015) 24, 98 102 1443-9506/04/$36.00 http://dx.doi.org/10.1016/j.hlc.2014.09.008 HOW-TO-DO-IT Simultaneous Double Clipping Delivery Guide Strategy for Treatment of Severe Coaptation
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Ischemic Mitral Regurgitation
 Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
Ischemic Mitral Regurgitation Jean-Louis J. Vanoverschelde, MD, PhD Université catholique de Louvain Brussels, Belgium Definition Ischemic mitral regurgitation is mitral regurgitation due to complications
MitraClip: Why, How, and For Whom?
 MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
MitraClip: Why, How, and For Whom? Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief, JAMA Cardiology
EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018
 1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
1 EVALUATION OF CHRONIC MITRAL REGURGITATION: ASSESSING MECHANISMS AND QUANTIFYING SEVERITY 2018 STRUCTURAL HEART DISEASE CONFERENCE June 1, 2018 David A. Orsinelli, MD, FACC, FASE Professor, Internal
Ischemic Mitral Valve Disease: Repair, Replace or Ignore?
 Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Ischemic Mitral Valve Disease: Repair, Replace or Ignore? Fabio B. Jatene Full Professor of Cardiovascular Surgery, Medical School, University of São Paulo, Brazil DISCLOSURE I have no financial relationship
Advanced Evaluation of Left Ventricular Function in Degenerative MR. Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium
 Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
Advanced Evaluation of Left Ventricular Function in Degenerative MR Dr Julien Magne, PhD University of Liege, CHU Sart Tilman, Liege, Belgium Conflict of Interest Disclosure None Case Clinical data Previous
LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR?
 LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR? Juan Cinca Department and Chair of Cardiology Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona
LEFT BUNDLE BRANCH BLOCK- BENIGN OR A HARBINGER OF HEART FAILURE? PROGNOSTIC INDICATOR? Juan Cinca Department and Chair of Cardiology Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona