Update on Gastrointestinal Bleeding COPYRIGHT. Update in Internal Medicine 5 th December, 2016
|
|
|
- Alban Hines
- 6 years ago
- Views:
Transcription
. Charlotte F.")

1 Update on Gastrointestinal Bleeding Update in Internal Medicine 5 th December, 2016 Simon C. Robson. MD, PhD, FRCP (UK). Charlotte F. and Irving W. Rabb Professor of Medicine Liver and Gastroenterology, Beth Israel Deaconess Medical Center Harvard Medical School Boston MA
2 Conflicts and Disclosures Royalties/Consultant Nanopharma, PureTech, Chugai Pharma, Gilead, ebioscience, MSD Pharma, Mesana Therapeutics & ebiolegend Funding NIH NHLBI/NCI/NIDDK, JDRF, Tizona, Helmsley Charitable Trust, PRIA Foundation & Boston Biomedical
3 Learning Objectives Revise and update major causes of upper and lower GI bleeding Discuss important elements of the history; of the physical exam; diagnostic evaluations and use of patient risk stratifications. Study and apply updated guidelines (ACG/AASLD/NICE updates) for the medical management and treatment of upper and lower GI bleeding; inclusive of variceal hemorrhage Review briefly clotting mechanisms and address new direct oral anticoagulants (DOAC), and consider differential impact on risks for gastrointestinal bleeding and thromboembolic risk Discuss case histories showing impact of oral anticoagulants and antiplatelet drugs on GI bleeding
4 Incidence and Significance 1-2% of all hospital admissions and increasing with greater application and use of new DOAC Most common diagnosis amongst ICU admissions Circa 5-10% require operative, surgical interventions after initial endoscopic evaluations and treatment 85% stop bleeding, medical therapies effective 7-12% mortality ,000 deaths per annum Up to 40% for recurrent bleeding Patients with massive bleeding need urgent intervention, often complicated by comorbidities Economic impact - 300,000 hospitalizations per year, cost estimates at around $2.5 billion
5 Anatomical sites Upper Esophageal Stomach Duodenum Hepatic Pancreatic Mid-lower Small bowel Colon and rectum Anus
6 Upper Types of Bleeding Proximal to Ligament of Treitz Melena (>200 cc of blood, acid/pepsin) Azotemia Nasogastric aspirate with blood Lower Also distal to Ligament of Treitz Hematochezia Rare (<5-10%) mid-bowel sources typically small bowel sources -- obscure GI bleeds (OGIB)
7 Predictors of mortality Renal disease 29% - acute renal failure 63% Liver disease >25% -- Role of coagulopathy still unclear Pulmonary disease 23% with respiratory failure 57% Cardiac disease 13% with CHF 28% Risk stratification scores Rockall (age, shock, co-morbidity, diagnosis and EGD) Modified Glasgow-Blatchford (blood urea, Hb, BP and pulse) AIMS65 (Alb, INR, mental status, systolic BP and age)
8 Clinical Presentation Hematemesis: bloody vomitus (bright red or coffee-grounds) Melena: black, tarry, foul-smelling stool Hematochezia: bright red or maroon blood per rectum Occult: positive guaiac test in subacute/chronic presentations Symptoms of anemia and blood loss: angina, dyspnea, or lightheadedness, syncope and potentially death
9 Acute UGIB Differential diagnosis usual suspects. Peptic ulcer disease Gastric ulcer Duodenal ulcer Mallory-Weiss tear Portal hypertension Esophagogastric varices Gastropathy Esophagitis Dieulafoy s lesion Vascular anomalies Hemobilia Hemorrhagic gastropathy Aortoenteric fistula Neoplasms Gastric cancer Kaposi s sarcoma
10 Diagnostics Large caliber NGT not required in all cases Coffee grounds or gross blood identified Can be used for lavage prior to endoscopy Upper endoscopy acute indications and timing Melena or hematochezia with hypotension Hematemesis NGT with guaiac positive fluid Should be completed in <24 hrs for stable patients
11 Gastrointestinal bleeding Prognostic Indicators NASOGASTRIC ASPIRATE Clear STOOL COLOR Red, brown, or black MO RTALITY RATE (%) Coffe e Grounds Brown or black Red 20 Red Blood Black 10 Brown 20 Red 30 Tedesco et al. ASGE Bleeding Survey. Gastro Endo


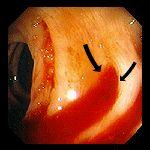
12 Mallory-Weiss tear and ooze


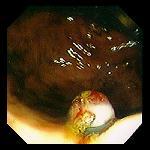
13 Acute arterial-type bleeding Dieulafoy s lesion Don t panic. Adams, Douglas. ( ). The Hitchhiker's Guide to the Galaxy All bleeding will stop. Anonymous
14 Upper GI hemorrhage probabilities Etiology frequencies Peptic ulcer disease - 50% Varices 10-20% Gastritis 10-25% Mallory-Weiss 8-10% Esophagitis 3-5% Malignancy 3% Dieulafoy s lesions 1-3% Aorto-duodenal/enteric fistulae - <1% Other obscure causes, lymphoma - 1-3%

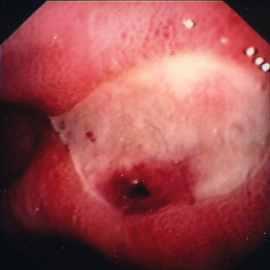
15 Endoscopic appearance of peptic ulcers
16 Peptic ulcer hemorrhage Characteristics 20% of patients bleed at least once Hemorrhage is most lethal complication Vessel is usually <1mm diameter Underlying causes H. pylori 40-50%...cure feasible NSAID s 40-50%...avoidance/Cox2 drugs Other (e.g. Z-E syndrome) Factors ppt hemorrhage unclear.?
17 Management of upper GI bleeding ABC, hemodynamic status/stratify risks Resuscitate (IVF, PRBC, FFP and platelets) to achieve Hb above 7 g/dl. A threshold of 9 g/dl should be considered in patients with massive bleeding, significant comorbid illness (especially cardiovascular ischemia) or possible endoscopic delays Treat initially as peptic ulcer disease (PPI) and in instance of chronic liver disease, add in specific therapies.. Early endoscopy to direct Rx - <24 hours Consider intubation airway protection and nasogastric tube to evaluate bleeding
18 Nasogastric tubes low quality evidence Pro s : Suctioning blood from the stomach may improve endoscopic visualization. Large amount of red blood is highly specific for large UGIB requiring early endoscopy - and gets everyone s attention Con s : Endoscopy is diagnostic/therapeutic procedure of choice, period. Sensitivity/specificity of NG lavage alone for active bleeding is poor and inadequate alone to guide management Not always required putative benefit from IV erythromycin
19 August 2000 RCT : IV omeprazole (80mg x 1 + 8mg/hr) vs. placebo AFTER endoscopy 240 patients with endoscopic evidence of active or recent ulcer bleeding..putative impact of ph on hemostasis and bleeding.. Findings: IV PPI after endoscopic treatment decreased risk of recurrent bleeding during the 30 day study period (22.5% vs. 6.5%).
20 April 2007 RCT : IV omeprazole (80mg x1 + 8mg/hr) vs. placebo BEFORE endoscopy [then all patients got PPI after the endoscopy] Study of 638 patients presenting to ED with UGIB. Excluded patients with refractory hypotension and ASA users Findings: IV PPI before EGD downstaged the ulcer, decreased need for endoscopic treatment (i.e. epi, endoclips); but DID NOT change mortality/recurrent bleeding within 30 days
21 Management of peptic ulcer hemorrhage Endoscopic intervention success 95% initially 20% will rebleed. Predictors at EGD Repeat treatment after rebleed will salvage around 50% patients --- Increased risk of mortality with rebleeding..
22 Ulcer appearance and risk of re-bleeding Clean based Prevalence % Risk of rebleeding % Forrest et al. Lancet 1974

23 Ulcer appearance and risk of re-bleeding Prevalence % Pigmented spot Risk of bleeding % Forrest et al. Lancet 1974
24 Ulcer appearance and risk of re-bleeding Prevalence % Adherent clot Risk of bleeding % Forrest et al. Lancet 1974
25 Ulcer appearance and risk of re-bleeding Prevalence % Visible vessel Risk of bleeding % Forrest et al. Lancet 1974
26 Ulcer appearance and risk of re-bleeding Prevalence % Active bleeding Risk of bleeding % Forrest et al. Lancet 1974
27 NIH consensus - endoscopic therapy Stops active bleeding Significantly decreases risk of rebleeding Limits levels of blood transfusion Decreases need for surgical management.
28 Endoscopic therapies Bipolar and multipolar electrocoagulation Heater probes, Argon plasma coagulator Hemoclips and Band ligation Injection (Epi, sclerosant, EtOH, saline) Several RCTs show Epi + 2 nd Rx improves hemostasis vs. Epi alone Epi always be followed by 2 nd modality (thermal, sclerosant)



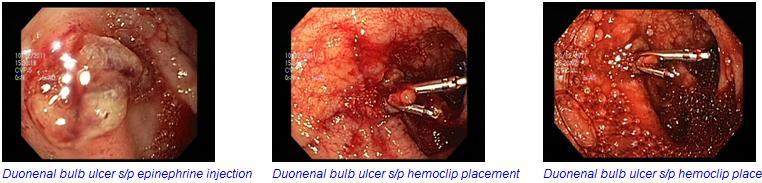
29 Injection, Multipolar Coagulation and Clipping

30 GI hemorrhage, coagulation and clipping
31 Dieulafoy's lesion




32 Gralnek I et al. N Engl J Med 2008;359: Jenson, DM. et al. Gastrointest Endosc 2005 Kovacs, TO. et al. Curr Treat Options Gastroenterol 2007
33 Case Presentation 67 yr man taking NSAIDs for the past 2 wks and developed epigastric pain Passage of black tarry stools..2 days PMHx: Not significant other than episodic lower back ache; potential insulin resistance, over weight but no other comorbidities SHx/FHx: Neg Vitals: BP 105/75 P 90 BMI 30 PE: otherwise normal, abdomen unremarkable, no overt features of liver disease but palpable liver edge
34 Patient Assessment Hemodynamic status crucial Localization of bleeding source CBC, PT, Platelets, PTT, LFTs, Renal function tests, rule out myocardial ischemia in elderly or cardiac issues Risk factors with use of validated score Rockall (age, BP, co morbidity, diagnosis and EGD - ABCDE) pre EGD score 1-4 points (2.4-25% mortality) Modified Glasgow-Blatchford score 7 50% need of intervention..
35 Resuscitation and Medical management Monitored bed or ICU Oxygen and NBM until stabilized, Glucose monitoring and control 2 large bore peripheral 16 G IV lines and/or CVP Normal saline with IV PPI Packed RBCs to maintain Hb over 7 g/dl, given caveat of active bleeding; those with unstable angina may require Hb >9. Correct coagulopathy Endoscopy and additional diagnostic tests

36 Esophageal Varices



37 Chronic liver disease.. Plan B
38 Upper GI bleeding in portal hypertension if you suspect variceal bleed* 1) Resuscitation, urgent triage. 2) IV Octreotide (50mcg + 50mgc/hr for 5 days) 3)? NG tube 4) Antibiotic treatment (IV ceftriaxone as prophylaxis for SBP) and lactulose once stabilized 5) Urgent endoscopy for banding/sclerotherapy/ evaluation for endotracheal intubation 6) Balloon tamponade 7) Recurrent/massive bleeding or earlier pre-emptive decision à Transcutaneous Intrahepatic Portosystemic Shunt viz. TIPS * Known varices, known cirrhosis, or exam/imaging/lab findings concerning for cirrhosis with portal hypertension (low plts, low albumin, coagulopathy ); portal hypertension alone
39 Acute Variceal Bleeding: Endoscopic Therapy and Octreotide/Somatostatin Addition of octreotide or somatostatin to endoscopic therapy decreases further bleeding and transfusion requirements over 5 days (or hospitalization) Terlipressin..in USA trials Besson et al., NEJM 1995 Sung, et al., Lancet 1995 Avgerinos et al, Lancet 1997
 Final result. Endoscope is then withdrawn through overtube, reloaded, and further bands applied to other variceal cords Wiliams et al.")
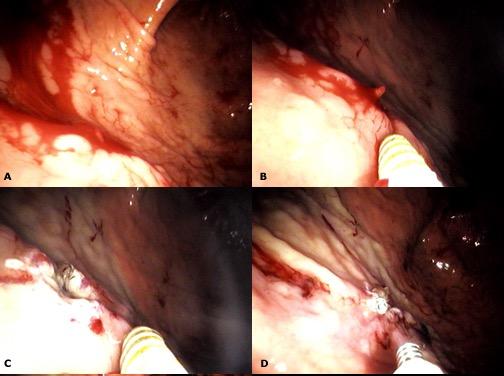
40 Endoscopic banding ligation (A) Identification of bleeding varix; (B) Application of ligating attachment to varix; (C) Application of suction through endoscope; (D) Traction on trip wire, resulting in release of prestressed rubber band and ligation of varix; (E) Final result. Endoscope is then withdrawn through overtube, reloaded, and further bands applied to other variceal cords Wiliams et al. BMJ 1994

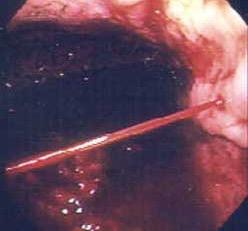
41 Variceal band ligation in action


42 Bleeding varix Esophageal Varices After endoscopic banding

43 Balloon Tamponade Krige et al. BMJ 2001

44 TIPS Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group N Engl J Med 2010; 362: Copyright 2001 BMJ Publishing Group Ltd.
45 Gastric varices and glue ablation
46 Synopsis Upper GIB Initial focus on resuscitation, risk-stratification based on features such as hemodynamic status, comorbidities, age and laboratory tests. Consider ulcer treatment unless specific evidence of cirrhosis or portal hypertension (ascites, low platelets, spleen enlargement, poor synthetic function) NG tubes may be placed, even in patient with varices - only exception is patients with banding in the last ~1 week main function to remove blood clots, facilitate endoscopy Involve the surgeons and interventional radiologists early multi-disciplinary team management In presentation with massive LGIB, ALWAYS evaluate for any upper GI source
47 Acute lower GI bleeds Differential Diagnosis Diverticulosis Colitis IBD (UC>>CD) Ischemia Infection Vascular anomalies Neoplasia Anorectal Hemorrhoids Fissure Dieulafoy s lesion Varices Small bowel Rectal Aortoenteric fistula Kaposi s sarcoma Other obscure UPPER GI BLEED
48 Acute Lower GI Bleed Diagnoses with hemodynamic compromise. DIAGNOSES % OF TOTAL Diverticulosis Vasc. anomalies 2-30 Colitis 9-21 Neoplasia/ polypectomy Anorectal 4-10 Upper GI sites <11 Zuccaro. ASGE Clinical Update
49 Acute Lower GI Bleed Key management points Resuscitation Exclude UGI source Most of the bleeding ceases spontaneously. circa 5% mortality Colonoscopy early, as feasible, with no role for barium studies - <24 hours CT angiography and angiography highly useful. Surgery in consultation
50 Diverticular disease and hemorrhage

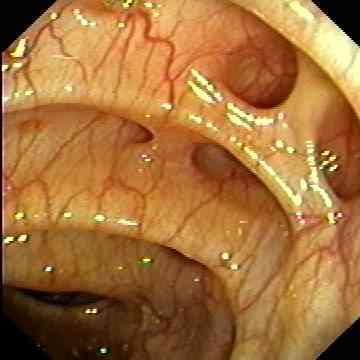
51 Colonic arteriovenous malformations
 Typically 9 mo to 5 years")
")
52 Radiation Proctitis 1-5% of all lower GI bleeds (tenesmus) Typically 9 mo to 5 years post-irradiation for pelvic malignancy Friable mucosae and telangiectasis (angiogenesis) Treatment (vexation)



53 Hemorrhoids
54 Non-Colonoscopy Interventions Surgical consultation in patients with high-risk clinical features and ongoing bleeding therapeutic options failing and comorbid disease Localize the possible source of bleeding before surgical resection to avoid continued bleeding Radiographic interventions in patients with highrisk clinical features and ongoing bleeding. Computed tomographic (CT) angiography for localization of the bleeding site before interventional angiography Other tests.. directed at subacute bleeding
, more than 1 episode of overt bleeding and use of CE within 2 weeks of the bleeding episode Sidhu, R., et al.")
55 Indications for capsule endoscopy Obscure gastrointestinal bleeding Small intestinal sources Maximize likelihood of positive finding in pt with Hb < 10, longer duration of bleeding (>6 months), more than 1 episode of overt bleeding and use of CE within 2 weeks of the bleeding episode Sidhu, R., et al. Gut, 2008:57(1);


56 Indications for enteroscopy Diagnostic Obscure gastrointestinal bleeding Exploration of radiographic abnormalities Investigation of small bowel tumors Therapeutic Surveillance Sidhu, R., et al. Gut, 2008:57(1);



57 Single balloon enteroscopy


58 Targets of new anticoagulant drugs Mackman N, and Becker R C Arterioscler Thromb Vasc Biol 2010;30:
:105-112 OR for GI bleeding among patients taking these new drugs is 1.45 (95% confidence interval 1.07 1.97). Aisenberg.")
59 Targets of new anticoagulant drugs - increased risk of GI bleeding? Holster et al Gastroenterology. 2013;145(1): OR for GI bleeding among patients taking these new drugs is 1.45 (95% confidence interval ). Aisenberg. American Journal of GASTROENTEROLOGY Supplements DOAC focus.
60 DOAC - Synopsis Direct oral anticoagulants becoming popular choices for stroke and thromboembolism protection Highly predictable fixed dosing without the necessity for monitoring of anticoagulant effect. Greater risk of gastrointestinal (GI) bleeding about 30% Age > 65 years, hepatorenal dysfunction, lower body weight, other prescription of antiplatelet agents, or nonsteroidal anti-inflammatory drugs, and/or drugs interacting with P-glycoprotein/cytochrome P450 system impact therapeutic effectiveness of DOACs and increase rates of GI bleeding
61 DOAC Use in Cardiac Disease and risk GI Bleeds Prevalence of e.g. atrial fibrillation amongst patients > 65 years in USA approximates 3.4 million patients (around 1 in 100 citizens) Relative to general population, atrial fibrillation patients have an increased risk of GI bleeding ( % per year vs. 0.1 % per year) just with chronic use of warfarin.. Dabigatran and rivaroxaban - associated with circa 30 % increase in GI bleeding over warfarin Estimates of % of patients will experience a DOACrelated GI bleed, which rounds off at 15,000 20,000 DOACrelated GI bleeds per year.. Am J Gastroenterol Suppl 2016; 3:2 12; doi: /ajgsup
62 Bleeding risk, hemostasis and coagulation tests Endoscopic hemostasis may be considered with INR of with reversal before endoscopy in patients with an INR >2.5 Platelet transfusion to maintain a platelet count of >50K with severe bleeding and prior to endoscopic hemostasis Platelet and plasma transfusions should be considered in patients who receive massive transfusions In patients on (new) anticoagulant agents, a multidisciplinary approach (with colleagues in hematology, cardiology, neurology, and gastroenterology) should be used to discontinue medications/use reversal agents to balance risk of ongoing bleeding vs. risk of thromboembolic events


63 Thrombus formation in injured blood vessels Bright Field Tissue factor Platelets Fibrin Merge
64 Case II Antiplatelet drugs and GI bleeding 79 yrs woman with HTN, ESRD on HD; who developed an episode of aphasia during dialysis Concern for TIA --- ASA 325 mg daily Soon after she was noted to have an episode of hematemesis and some hematochezia and dark stool.. Denies any prior GI bleeding, no lightheadedness, weakness, nausea Denies any OTC NSAIDs, and no alcohol No further bowel movements
65 ED course Vitals: HR 69 BP 132/54 Hct 23.5, post dialysis Head CT showed no acute process NG lavage scant coffee grounds, cleared with small amount of saline Patient was treated with: 1 to 2 units PRBC Protonix infusion Octreotide infusion Patient transferred to BIDMC
66 BIDMC Course Vitals: HR 100 BP 120/40 RR 16, 100% on room air Pt appears well in no acute distress NG tube Cardiac: 2/6 crescendo murmur at LUSB Lungs: CTA bilaterally ABD: Soft nt/nd, no stigmata of chronic liver issues Rectal: scant amount of clotted blood, no stool Noted to be DNI/DNR Glasgow-Blanchard Score 14 high risk

67 First EGD Repeat Hct at dawn decreasing..

68 GI bleeding and ASA usage Huang, ES et al. The American Journal of Medicine. 2011
69 Recurrent upper GI bleed within 30 days - non significant differences between continued use of ASA and placebo Sung J J et al. Ann Intern Med 2010;152:1-9

70 Repeat EGD Epi + Clips
71 Risk rebleeding higher in patients with ESRD on HD and she did so Wu, CY. et al. Gut 2011

72 Where available, percutaneous embolization can be considered as an alternative to surgery for patients for whom endoscopic therapy has failed. She underwent selective vessel embolization experienced repeat hemorrhage.surgical consult. Barkun, A. et al Annals of Internal Medicine 2010
73 Lau JY et al. N Engl J Med 1999;340:
74 Summary Surgery consulted again Vagotomy/pyoloroplasty/oversewing ulcer/j-tube placed Synopsis: 4 x EGD (4 clips, cautery, injections) 1 x IR placed 14 coils 34 units of PRBC 13 units of FFP 5 units Platelets 6 units Cryoprecipitate 1 x Surgery
75 Take away points.. Aspirin carries risk of ulceration and bleeding Consider early reintroduction and use of PPI in appropriate patients - secondary prophylaxis Risks of rebleeding? (as per Macbeth - "they say, blood will have blood" ( )). General risk based on visualization of ulcer Risks also dictated by patient and co morbidity Massive GI bleed - involve multidisciplinary team: Role of ICU, Nursing staff, PCP, GI, Surgery, IR..in all cases
76 Acknowledgements Joe Feuerstein Tyler Berzin Ram Chuttani Ken Bauer Colleagues in GI and Liver BIDMC
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding
 ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
ACG Clinical Guideline: Management of Patients with Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG 1 and Ian M. Gralnek, MD, MSHS 2 1 Division of Gastroenterology, University of Washington
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
Nothing to disclose. Annually ~ 300,000 hospitalizations and ~ 20,000 deaths in US*
 Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
Gastrointestinal Bleeding Disclosures Nothing to disclose Bennie Ray Upchurch III, MD, FACP, FASGE Clinical Associate Professor of Medicine Division of Gastroenterology, Hepatology & Nutrition The Ohio
High Value Care of GI Bleeding
 High Value Care of GI Bleeding Bennie R. Upchurch MD, FACP, FASGE, AGAF, FACG Medical Director, GI Bleeding Program, Division of Gastroenterology, Nutrition, and Hepatology Ohio State University Wexner
High Value Care of GI Bleeding Bennie R. Upchurch MD, FACP, FASGE, AGAF, FACG Medical Director, GI Bleeding Program, Division of Gastroenterology, Nutrition, and Hepatology Ohio State University Wexner
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding
 ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
CHAPTER 30 Gastrointestinal Bleeding
 CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants
 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants Wednesday, May 9, 2018, 12:00PM ET Guest Author: Adam Cuker, MD Presenter: Tracy Minichiello, MD
Acute Gastrointestinal Haemorrhage. Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield
 Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Guidelines for the Management of Upper gastrointestinal bleeding
 Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Management of acute upper gastrointestinal bleeding
 1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Role of radiology in colo-rectal bleedings. Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE
 Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
Role of radiology in colo-rectal bleedings Alban DENYS MD FCIRSE EBIR CHUV LAUSANNE Epidemiology Lower GI bleeding accounts for 20-25% of all GI bleeding Annual incidence in USA :21-27/100000 Longstreth
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
The Usefulness of Capsule Endoscopy
 The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding
 PRACTICE GUIDELINES nature publishing group 459 CME ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG1 and Ian M. Gralnek, MD, MSHS2
PRACTICE GUIDELINES nature publishing group 459 CME ACG Clinical Guideline: Management of Patients With Acute Lower Gastrointestinal Bleeding Lisa L. Strate, MD, MPH, FACG1 and Ian M. Gralnek, MD, MSHS2
Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit
 Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit Authors Shahrad Hakimian 1, Salmaan Jawaid 2, Yurima Guilarte-Walker 3, Jomol Mathew
Video capsule endoscopy as a tool for evaluation of obscure overt gastrointestinal bleeding in the intensive care unit Authors Shahrad Hakimian 1, Salmaan Jawaid 2, Yurima Guilarte-Walker 3, Jomol Mathew
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
New Techniques. Incidence of Peptic Ulcer. Changing. Contents - with an emphasis on peptic ulcer bleeding. Cause of death in peptic ulcer bleeding
 Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Bleeding Case Presentation and Review of the Literature Case Presentation
10/1/2018. Case. History. Initial Assessment. Vital Signs. Factors predictive of UGI source. Gastrointestinal Hemorrhage
 Case 79 yo M transferred from OSH with blood per rectum Gastrointestinal Hemorrhage Piroska Kopar MD Assistant Professor of Surgery Section of Acute and Critical Care Surgery 4u prbc 2u FFP Mentating,
Case 79 yo M transferred from OSH with blood per rectum Gastrointestinal Hemorrhage Piroska Kopar MD Assistant Professor of Surgery Section of Acute and Critical Care Surgery 4u prbc 2u FFP Mentating,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
UPPER AND LOWER GASTROINTESTINAL BLEEDING. Prof. G. Zuliani
 UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
But.. Capsule Endoscopy. Guidelines (OMED ECCO) Why is Enteroscopy so Important? 4/19/2017
 Why is Enteroscopy so Important? 4/19/2017") Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
GASTROINTESTINAL BLEEDING. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
Upper Gastrointestinal Bleeding. December 4, 2018 & December 11, 2018 Sonia Lin
 Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
Upper Gastrointestinal Bleeding December 4, 2018 & December 11, 2018 Sonia Lin Roadmap Evaluation of acute GIB Causes of upper GI bleeding Initial management of upper GI bleed Case 1 Case 2 Questions!
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Gastrointestinal bleed- what saves life?
 Gastrointestinal bleed- what saves life? Prof Sauid Ishaq Gastroenterologist, DGH BCU, SGU and Fudan University Physician Associates conference Friday 16 February 2018 Reality What is the mortality of
Gastrointestinal bleed- what saves life? Prof Sauid Ishaq Gastroenterologist, DGH BCU, SGU and Fudan University Physician Associates conference Friday 16 February 2018 Reality What is the mortality of
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
True obscure causes hemobilia, hemosuccus pancreaticus, vasculitis
 Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
Endoscopic Techniques for Small Bowel Imaging Going Where No Man Has Gone Before! Jonathan A. Leighton, MD, FACG, FASGE Mayo Clinic in Arizona 2014 ACG Governors/ASGE Best Practices Course January 2014
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING
 Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Antiplatelets in cardiac patients with suspected GI bleeding
 Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
CLINICAL VIGNETTE 2015; 1:3
 CLINICAL VIGNETTE 2015; 1:3 UPPER GASTRO INTESTINAL BLEEDING Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers
CLINICAL VIGNETTE 2015; 1:3 UPPER GASTRO INTESTINAL BLEEDING Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:151 158 Long-term Outcome of Patients With Obscure Gastrointestinal Bleeding Investigated by Double-Balloon Endoscopy SATOSHI SHINOZAKI, HIRONORI YAMAMOTO,
GASTROINTESTINAL HEMORRHAGE
 Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy
 Original article Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy Authors Yeong Jin Kim, Jun Chul Park, Eun Hye Kim, Sung Kwan Shin,
Original article Hemostatic powder application for control of acute upper gastrointestinal bleeding in patients with gastric malignancy Authors Yeong Jin Kim, Jun Chul Park, Eun Hye Kim, Sung Kwan Shin,
Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A Retrospective Study
 Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Case Report imedpub Journals http://www.imedpub.com/ Medical Case Reports DOI: 10.21767/2471-8041.100062 Upper Gastrointestinal Bleeding and the Importance of an Early Endoscopic Study for Diagnosis: A
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Peri-Endoscopic Period. Neena S. Abraham MD, MSCE, FACG
 How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
How to Manage Antiplatelet Therapy in the Peri-Endoscopic Period Neena S. Abraham MD, MSCE, FACG Michael E. DeBakey Veterans Affairs Medical Center Sections of Gastroenterology & Health Services Research
ACUTE UPPER GASTROINTESTINAL HEMORRHAGE: PHARMACOLOGIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Moderators: Steven Fern, DO Sreenivas Jonnalagada, MD
 Moderators: Steven Fern, DO Sreenivas Jonnalagada, MD Case 1 42 year old male with intermittent bright red blood per rectum and melena EGD and colonoscopy at OSH unremarkable Meckels scan negative CT scan
Moderators: Steven Fern, DO Sreenivas Jonnalagada, MD Case 1 42 year old male with intermittent bright red blood per rectum and melena EGD and colonoscopy at OSH unremarkable Meckels scan negative CT scan
Gastrointestinal Hemorrhage
 Gastrointestinal Hemorrhage Quality Measures Length of Stay RCC Costs per Case Mortality Rate Eligible Readmission Within 30 Days. Critical Event(s) Evaluation Phase/Acute Phase Baseline pain assessment
Gastrointestinal Hemorrhage Quality Measures Length of Stay RCC Costs per Case Mortality Rate Eligible Readmission Within 30 Days. Critical Event(s) Evaluation Phase/Acute Phase Baseline pain assessment
Upper GI Bleeds. AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM
 Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Occult and Overt GI Bleeding: Small Bowel Imaging. Outline of Talk
 Occult and Overt GI Bleeding: Small Bowel Imaging Lauren B. Gerson MD, MSc Director of Clinical Research, GI Fellowship Program California Pacific Medical Center San Francisco, CA Outline of Talk Definition
Occult and Overt GI Bleeding: Small Bowel Imaging Lauren B. Gerson MD, MSc Director of Clinical Research, GI Fellowship Program California Pacific Medical Center San Francisco, CA Outline of Talk Definition
35 Practical Approach to Blood Vomiting
 C H A P T E R 35 Practical Approach to Blood Vomiting Jatinder K Mokta INTRODUCTION Hematemesis is defined as vomiting of blood, which is indicative of bleeding from the esophagus, stomach, or duodenum.
C H A P T E R 35 Practical Approach to Blood Vomiting Jatinder K Mokta INTRODUCTION Hematemesis is defined as vomiting of blood, which is indicative of bleeding from the esophagus, stomach, or duodenum.
Nonvariceal Upper Gastrointestinal Bleeding
 Nonvariceal Upper Gastrointestinal Bleeding Stephen R. Rotman and John R. Saltzman 2 Introduction Upper gastrointestinal bleeding (UGIB) is defined as bleeding in the gastrointestinal tract originating
Nonvariceal Upper Gastrointestinal Bleeding Stephen R. Rotman and John R. Saltzman 2 Introduction Upper gastrointestinal bleeding (UGIB) is defined as bleeding in the gastrointestinal tract originating
Upper and Lower GI Bleeding
 Upper and Lower GI Bleeding John Poneros MD, FASGE, NYSGEF Associate Professor Columbia University College of Physicians and Surgeons Acting Director, Endoscopy Unit New York Presbyterian/Columbia UGIB
Upper and Lower GI Bleeding John Poneros MD, FASGE, NYSGEF Associate Professor Columbia University College of Physicians and Surgeons Acting Director, Endoscopy Unit New York Presbyterian/Columbia UGIB
Introduction. Methods. Introduction. Methods. Methods. Journal reading Transfusion Strategies for Acute Upper Gastrointestinal Bleeding
 Journal reading Transfusion Strategies for Acute Upper Gastrointestinal Bleeding N Engl J Med 2013;368:11-21. Hospital de la Santa Creu i Sant Pau, Barcelona, Spain Càndid Villanueva, M.D., Alan Colomo,
Journal reading Transfusion Strategies for Acute Upper Gastrointestinal Bleeding N Engl J Med 2013;368:11-21. Hospital de la Santa Creu i Sant Pau, Barcelona, Spain Càndid Villanueva, M.D., Alan Colomo,
Occult small bowel bleeding - Video capsule first
 Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
Lower gastrointestinal bleeding (LGIB) is a common
 is a common") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:485 490 Early Predictors of Severe Lower Gastrointestinal Bleeding and Adverse Outcomes: A Prospective Study FERNANDO S. VELAYOS,* ANN WILLIAMSON, KAREN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:485 490 Early Predictors of Severe Lower Gastrointestinal Bleeding and Adverse Outcomes: A Prospective Study FERNANDO S. VELAYOS,* ANN WILLIAMSON, KAREN
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
ORIGINAL INVESTIGATION. Early Predictors of Severity in Acute Lower Intestinal Tract Bleeding
 ORIGINAL INVESTIGATION Early Predictors of Severity in Acute Lower Intestinal Tract Bleeding Lisa L. Strate, MD, MPH; E. John Orav, PhD; Sapna Syngal, MD, MPH Background: Identification of high-risk patients
ORIGINAL INVESTIGATION Early Predictors of Severity in Acute Lower Intestinal Tract Bleeding Lisa L. Strate, MD, MPH; E. John Orav, PhD; Sapna Syngal, MD, MPH Background: Identification of high-risk patients