Transcatheter heart valve thrombosis
|
|
|
- Laurence Harrell
- 6 years ago
- Views:
Transcription
1 Transcatheter heart valve thrombosis Jeroen J Bax Dept Cardiology Leiden, The Netherlands New York, 2017 The department of Cardiology of the Leiden University Medical center received research grants from Boston Scientific, Biotronik, Medtronic and Edwards Lifesciences
2 When everything was simple: AV mean gradient after TAVR PARTNER 1-cohort A Mack et al. Lancet et al 2015
3 When everything was simple: EROA after TAVR PARTNER 1-cohort A Mack et al. Lancet et al 2015
4 TIA stroke rate Between 1 and 2 years, 8 strokes occurred (4 in the TAVR group and 4 in the surgery group) and 3 transient ischemic attacks (2 in the TAVR group and 1 in the surgery group). PARTNER 1-cohort A Kodali et al. NEJM 2012

 with or")
 (2D")
5 CT post-tavr however showed. hypo-attenuated leaflet thickening (HALT) with or without restricted leaflet motion (HAM) (2D and 4D) suggesting thrombosis..


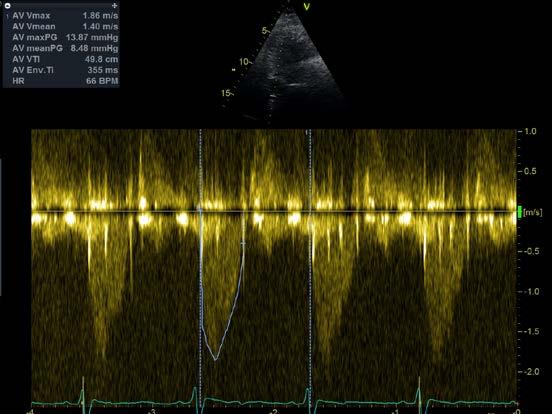
6 Normal: CT vs Echo (mean 8 mmhg)


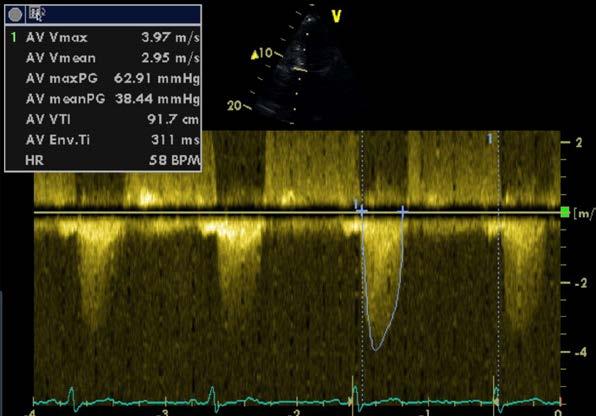

7 Abnormal: CT vs Echo (mean 38 mmhg)
8 One of the first studies N = 156, 46% male TAVI with SAPIEN 3 THV CT 5 days (median) after TAVI HALT 10.3% of patients Echo 5 days (median) after TAVI mean gradient 8±3.5 mmhg Pache et al Eur Heart J 2016
function Mean gradient 25")
9 Some show: Matched anatomy and (dys)function Mean gradient 25 mmhg

10 But most show: Mismatch anatomy and function Mean gradient 11 mmhg
11 What is in the literature? 12 studies Author (year) No Prevalence of thrombosis on MDCT (time) Prevalence of thrombosis on Echo (time) Mean gradient (mmhg) - EOA (cm 2 ) Latib et al (2015) 4266 NA 0.61% (median 181 days) Pacheet al (2016) % (median 5 days) NA (median 5 days) 40.5± NA 8±3.5 - NA Leetmaa et al(2016) 140 4% (1-3 months) NA (1-3 months) Del Trigo et al (2016) 1521 NA 4.5% (4 years) 26.1±11 - NA Hansson et al (2016) 405 7% (1-3 months) NA (1-3 months) 10±7-1.5±0.5 Makkaret al (2015) 55 40% (median 32 days) Makkaret al (2015) % (median 86 days) Yanagisawa et al(2017) % (1 year) Chakravarty et al (2017) % (median 58 days) Vollemaet al (2017) % (median 35 days) NA (30 days) NA (30 days) 9.2±4.9 - NA 8.4±2.9 - NA NA (1 year) 8.3± ±0.25 6% (median 58 days) 13.8± NA 3% (3years) 9.3± ± 0.56 Jose et al (2017) 642 9/10 (NA) 2.8% (median 181 days) 34± ±0.46 Sondergaard et al (2017) 61 11% (140±152 days) NA 7.0±3.2 - NA
12 What the literature tells us Author (year) No Prevalence of thrombosis on MDCT (time) Prevalence of thrombosis on Echo (time) Mean gradient (mmhg) - EOA (cm 2 ) Latib et al (2015) 4266 NA 0.61% (median 181 days) Pacheet al (2016) % (median 5 days) NA (median 5 days) 40.5± NA 8±3.5 - NA Leetmaa et al(2016) 140 4% (1-3 months) NA (1-3 months) Del Trigo et al (2016) 1521 NA 4.5% (4 years) 26.1±11 - NA Hansson et al (2016) 405 7% (1-3 months) NA (1-3 months) 10±7-1.5±0.5 Makkaret al (2015) 55 40% (median 32 days) Makkaret al (2015) % (median 86 days) Yanagisawa et al(2017) % (1 year) Chakravarty et al (2017) % (median 58 days) Vollemaet al (2017) % (median 35 days) NA (30 days) NA (30 days) 9.2±4.9 - NA 8.4±2.9 - NA NA (1 year) 8.3± ±0.25 6% (median 58 days) 13.8± NA 3% (3years) 9.3± ± 0.56 Jose et al (2017) 642 9/10 (NA) 2.8% (median 181 days) 34± ±0.46 Sondergaard et al (2017) 61 11% (140±152 days) NA 7.0±3.2 - NA
 THV thrombosis Median time to diagnosis 181 days 65% worsening dyspnea 31% subclinical (asymptomatic) No neurological events No")
13 N = (0.61%) THV thrombosis Median time to diagnosis 181 days 65% worsening dyspnea 31% subclinical (asymptomatic) No neurological events No thromboembolic events Mean aortic valve gradient 40.5±14.0 mmhg Anticoagulation effective treatment Latib et al. Circ Cv Intervent 2015
14 Latib et al. Circ CV Intervent 2015 Gradient vs anti-coagulation

15 N = (4.5%) Valve hemodynamic deterioration (VHD) Assessed with echocardiography. VHD was defined as a 10 mmhg increase in transprosthetic mean gradient during follow-up compared with discharge assessment. Follow-up 4 years Del Trigo et al. JACC 2016
16 What the literature tells us 12 studies Author (year) No Prevalence of thrombosis on MDCT (time) Prevalence of thrombosis on Echo (time) Mean gradient (mmhg) - EOA (cm 2 ) Latib et al (2015) 4266 NA 0.61% (median 181 days) Pacheet al (2016) % (median 5 days) NA (median 5 days) 40.5± NA 8±3.5 - NA Leetmaa et al(2016) 140 4% (1-3 months) NA (1-3 months) Del Trigo et al (2016) 1521 NA 4.5% (4 years) 26.1±11 - NA Hansson et al (2016) 405 7% (1-3 months) NA (1-3 months) 10±7-1.5±0.5 Makkaret al (2015) 55 40% (median 32 days) Makkaret al (2015) % (median 86 days) Yanagisawa et al(2017) % (1 year) Chakravarty et al (2017) % (median 58 days) Vollemaet al (2017) % (median 35 days) NA (30 days) NA (30 days) 9.2±4.9 - NA 8.4±2.9 - NA NA (1 year) 8.3± ±0.25 6% (median 58 days) 13.8± NA 3% (3years) 9.3± ± 0.56 Jose et al (2017) 642 9/10 (NA) 2.8% (median 181 days) 34± ±0.46 Sondergaard et al (2017) 61 11% (140±152 days) NA 7.0±3.2 - NA

17 N = (4%) THV thrombosis MDCT performed within 1-3 months of TAVI N = 1 heart failure symptoms N= 4 subclinical (asymptomatic) No neurological events No thromboembolic events Mean aortic valve gradient <20 mmhg in all Anticoagulation effective treatment Leetmaa et al. Circ Cv Intervent 2015

18 N = 55 TAVI clinical trial 22 (40%) N = 132 registry (TAVR or SAVR) 17 (13%) THV thrombosis Median time to MDCT: days Mean gradient <20 mmhg in all patients Anticoagulation effective treatment Makkar et al. New Engl J Med 2016
19 N = (12%) THV thrombosis Assessed with MDCT median follow-up of 35 days Mostly asymptomatic ( 1 patient with heart failure) Mean gradient 9.3±4.7 mmhg No association with increased risk of TIA and all strokes Vollema et al. Eur Heart J 2017
.")
20 COHORT OF THV 11% THV thrombosis scan 1 = 140 (STD 152) days scan <12 MONTHS First important observation: progression absent in all patients using anticoagulation. Second important observation: 61.9% of patients - normal valves at both 4D CT scans despite absence of oral anticoagulation. Third important observation: stability also noted in 41 patients using antiplatelet therapy (or no therapy). Implying that anticoagulation may not be warranted in all patients, but should be personalized to patients who need it. Sondergaard et al. Eur Heart J 2017
21 The definitions Echocardiography: Zoghbiet al (JASE 2009): definition for surgical bioprosthetic valve prostheses Possible stenosis: mean gradient mmhg effective orifice area (indexed for body surface area) cm2. Significant stenosis: mean gradient >35 mmhg effective orifice area (indexed for body surface area) <0.8 cm2. expanded by Lancellotti et al (EHJCVI 2016): possible obstruction: increase in mean gradient at follow-up between mmhg significant obstruction: increase in mean gradient at follow-up 20 mmhg.
22 The definitions CT: hypo-attenuated leaflet thickening (HALT) 2D with or without restricted leaflet motion 4D
23 Need for better definitions Dangas et al recently stated that prosthetic heart valve dysfunction can be seen as a continuum of the same pathological process with early thrombus formation (CT), later fibrotic pannus formation (echo), followed by degeneration / dysfunction (echo) JACC 2016

24 Open questions: Correlation between thrombosis rate based on imaging vs. stroke rate 10-15% 3-5% 5-7% HALT - CT Echocardiography Stroke/TIA
 Imaging surveillance? When? How often?")
25 Open questions: Resolution after anticoagulation Everyone anticoagulation? How long? When to start? (but a significant number of patients has indication) Imaging surveillance? When? How often? Which technique?
26 Source:
27 Source:
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD
 Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
Subclinical Thrombosis of Bioprosthetic Aortic Valves: Is It Clinically Relevant? Tarun Chakravarty, MD Interventional Cardiology Cedars-Sinai Heart Institute Disclosures Consultant and proctor for Edwards
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study
 Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study Meagan Sullivan, PharmD PGY2 Cardiology Pharmacy Resident University of Chicago Medicine
Should We Reconsider using Anticoagulation for Biological Tissue Valves
 Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
Should We Reconsider using Anticoagulation for Biological Tissue Valves No Disclosures Disclosures Watching grass grow Complete with audio 1 hour 8 minutes 9884 views Subclinical Leaflet Thrombosis in
TAVR Valve Thrombosis
 TAVR Valve Thrombosis Mohammed Balghith, MD, FACC, FRCPC, FACP, FESC Associate Professor KSAU-HS, Consultant Interventional Cardiologist Ministry of National Guard, King Abdulaziz Cardiac Center, Riyadh
TAVR Valve Thrombosis Mohammed Balghith, MD, FACC, FRCPC, FACP, FESC Associate Professor KSAU-HS, Consultant Interventional Cardiologist Ministry of National Guard, King Abdulaziz Cardiac Center, Riyadh
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Standarized definition of bioprosthetic valve deterioration and failure
 Translational aortic valve research. From biology to treatment Standarized definition of bioprosthetic valve deterioration and failure Anna Sonia Petronio, MD, FESC Head of Cardiac Catheterization Lab
Translational aortic valve research. From biology to treatment Standarized definition of bioprosthetic valve deterioration and failure Anna Sonia Petronio, MD, FESC Head of Cardiac Catheterization Lab
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVI limitations for low risk patients
 TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Transcatheter aortic valve replacement in intermediate and low risk patients-clinical evidence
 Perspective Transcatheter aortic valve replacement in intermediate and low risk patients-clinical evidence Sameer Arora, John P. Vavalle Division of Cardiology, University of North Carolina School of Medicine,
Perspective Transcatheter aortic valve replacement in intermediate and low risk patients-clinical evidence Sameer Arora, John P. Vavalle Division of Cardiology, University of North Carolina School of Medicine,
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Adjunctive Pharmacotherapy: Current Landscape for Patients Post TAVR
 Adjunctive Pharmacotherapy: Current Landscape for Patients Post TAVR George D. Dangas, MD, FACC, FAHA, FESC, MSCAI Professor of Medicine & Surgery Icahn School of Medicine at Mount Sinai The Mount Sinai
Adjunctive Pharmacotherapy: Current Landscape for Patients Post TAVR George D. Dangas, MD, FACC, FAHA, FESC, MSCAI Professor of Medicine & Surgery Icahn School of Medicine at Mount Sinai The Mount Sinai
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Is Stroke Frequency Declining?
 Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Is Stroke Frequency Declining? Etiologic Factors Clinical, Anatomic, Technique-related, and Device-specific Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac
Antithrombotic Rx in the Setting of TAVI
 Antithrombotic Rx in the Setting of TAVI George D. Dangas, MD, PhD, FESC, MSCAI Professor of Medicine & Surgery Icahn School of Medicine at Mount Sinai The Mount Sinai Hospital, New York, NY COI Research
Antithrombotic Rx in the Setting of TAVI George D. Dangas, MD, PhD, FESC, MSCAI Professor of Medicine & Surgery Icahn School of Medicine at Mount Sinai The Mount Sinai Hospital, New York, NY COI Research
TAVR in 2020: What is Next!!!!
 TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
DICE Session. The endocarditis team. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses
 Review Article Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses Dale J. Murdoch, John G. Webb Centre for Heart Valve Innovation, St. Paul s Hospital, Vancouver, Canada Contributions:
Review Article Transcatheter valve-in-valve implantation for degenerated surgical bioprostheses Dale J. Murdoch, John G. Webb Centre for Heart Valve Innovation, St. Paul s Hospital, Vancouver, Canada Contributions:
The SAPIEN 3 TAVI Advantage
 Edwards SAPIEN 3 Valve The SAPIEN 3 TAVI Advantage... The SAPIEN 3 TAVI Advantage The clear choice for your patients and your TAVI program Advanced valve and system designed to simplify procedures Consistent
Edwards SAPIEN 3 Valve The SAPIEN 3 TAVI Advantage... The SAPIEN 3 TAVI Advantage The clear choice for your patients and your TAVI program Advanced valve and system designed to simplify procedures Consistent
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
Vinod H. Thourani, MD, FACC, FACS
 Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison
 Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Outcome of Next-Generation Transcatheter Valves in Small Aortic Annuli: A Multicenter Propensity-Matched Comparison Mauri, V. et al.: Circ Cardiovasc Interv. 2017;10:e005013 All trademarks are the property
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
How to Prevent Thromboembolic Complications in TAVI
 How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
Antithrombotic. DAPT or OAC?
 Antithrombotic treatment after TAVI: DAPT or OAC? Striking the right balance. Pascal Vranckx MD, PhD. Hartcentrum Hasselt, Belgium. Disclosure of Interest Pascal Vranckx has the following potential conflicts
Antithrombotic treatment after TAVI: DAPT or OAC? Striking the right balance. Pascal Vranckx MD, PhD. Hartcentrum Hasselt, Belgium. Disclosure of Interest Pascal Vranckx has the following potential conflicts
Strokes After TAVR. Ioannis Iakovou, MD, PhD. Interventional Cardiology Onassis Cardiac Surgery Center
 Strokes After TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Strokes After TAVR How common is stroke after TAVR Is it increasing? Is it more with TF vs TA? Is it
Strokes After TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Strokes After TAVR How common is stroke after TAVR Is it increasing? Is it more with TF vs TA? Is it
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Embolic Protection Devices for Transcatheter Aortic Valve Replacement
 Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute
 Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
ANTICOAGULATION IN SPECIFIC POPULATIONS: BIOLOGICAL HEART VALVES, TAVI
 ESC Cardiovascular Round Table 27 March 2017, Amsterdam ANTICOAGULATION IN SPECIFIC POPULATIONS: BIOLOGICAL HEART VALVES, TAVI Stephan Windecker Department of Cardiology Swiss Cardiovascular Center Bern
ESC Cardiovascular Round Table 27 March 2017, Amsterdam ANTICOAGULATION IN SPECIFIC POPULATIONS: BIOLOGICAL HEART VALVES, TAVI Stephan Windecker Department of Cardiology Swiss Cardiovascular Center Bern
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
Transcatheter Aortic Heart Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications
 Accepted Manuscript Transcatheter Aortic Heart Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications Nicolaj C. Hansson, MD, Erik L. Grove, MD, PhD, Henning R. Andersen, MD, DMSc,
Accepted Manuscript Transcatheter Aortic Heart Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications Nicolaj C. Hansson, MD, Erik L. Grove, MD, PhD, Henning R. Andersen, MD, DMSc,
The Future of Medicine. Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy
 The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question.
 Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and
 Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
A review of the complications associated with Transcatheter Aortic Valve Implantation.
 A review of the complications associated with Transcatheter Aortic Valve Implantation. Dr Conor McQuillan Transcatheter Aortic Valve Implantation (TAVI) has become the standard of care for treating elderly,
A review of the complications associated with Transcatheter Aortic Valve Implantation. Dr Conor McQuillan Transcatheter Aortic Valve Implantation (TAVI) has become the standard of care for treating elderly,
Current Controversies. Subclinical and clinical valve thrombosis
 Chapter 19: Current controversies, ongoing trials, new valves, and future directions Sukhdeep S. Basra, MD, MPH, Michael J. Mack, MD The Heart Hospital Baylor Plano, Texas Transcatheter Aortic Valve Replacement
Chapter 19: Current controversies, ongoing trials, new valves, and future directions Sukhdeep S. Basra, MD, MPH, Michael J. Mack, MD The Heart Hospital Baylor Plano, Texas Transcatheter Aortic Valve Replacement
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients
 O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Makkar RR, Fontana G, Jilaihawi H, et al. Possible subclinical
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Makkar RR, Fontana G, Jilaihawi H, et al. Possible subclinical
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves
 The new england journal of medicine Original Article Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves R.R. Makkar, G. Fontana, H. Jilaihawi, T. Chakravarty, K.F. Kofoed, O. De Backer,
The new england journal of medicine Original Article Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves R.R. Makkar, G. Fontana, H. Jilaihawi, T. Chakravarty, K.F. Kofoed, O. De Backer,
New imaging modalities for assessment of TAVI procedure and results. R Dulgheru, MD Heart Valve Clinic CHU, Liege
 New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
New imaging modalities for assessment of TAVI procedure and results R Dulgheru, MD Heart Valve Clinic CHU, Liege Disclosure of Interest I, Raluca Dulgheru, DO NOT HAVE a financial interest/arrangement
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
TAVR: Review of the Robust Data from Randomized Trials
 TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
Imaging to select patients for Transcatheter TV
 Imaging to select patients for Transcatheter TV Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands San Diego, february 2018 Research grants: Medtronic, Biotronik, Boston Scientific,
Imaging to select patients for Transcatheter TV Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands San Diego, february 2018 Research grants: Medtronic, Biotronik, Boston Scientific,
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
TAVR for low-risk patients in 2017: not so fast.
 TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
TAVR for low-risk patients in 2017: not so fast. Enrico Ferrari, MD, FETCS Cardiac Surgery Department Cardiocentro Ticino Foundation Lugano, Switzerland Conflicts of Interest Consultant and proctor for
Results of Transfemoral Transcatheter Aortic Valve Implantation
 Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Disclosures. LGH TAVR: Presentation Outline 2/2/2016. Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience
 and the LGH Experience") Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
TAVR in 2017 What we know? What to expect?
 Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes
 SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies. Martin B. Leon, MD
 TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Disclosure Statement of
TAVR 2015: A Breakthrough Technology GOES VIRAL! Issues and Controversies Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City Disclosure Statement of
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
Current Evidence in TAVI patients using ACURATE and LOTUS valves
 Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification. Rheumatic Mitral Stenosis 76yo male
 MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
MITRAL STENOSIS: MANY FLAVORS Rheumatic and Calcification David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Rheumatic Mitral Stenosis
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Transcatheter Therapies For Aortic Valve Disease. March 2017 Brian Whisenant MD
 Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
Transcatheter Therapies For Aortic Valve Disease March 2017 Brian Whisenant MD Introduction I got into this field to protect my turf. I must say, I have come full circle... - Kent W. Jones I got into this
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Policy Specific Section: March 30, 2012 March 7, 2013
 Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
Medical Policy Transcatheter Aortic Valve Replacement for Aortic Stenosis Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date:
TAVR for Complex Aortic Valvular Conditions
 TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
Paravalvular Regurgitation is a Risk Factor Following TAVI
 Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Paravalvular Regurgitation is a Risk Factor Following TAVI Philippe Pibarot, DVM, PhD, FACC, FESC, FASE Canada Research Chair in Valvular Heart Disease INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE
Published Manuscripts Based in the STS/ACC TVT Registry
 Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Published Manuscripts Based in the STS/ACC TVT Registry June 2018 Legend Manuscript Status is designated as follows: Abbreviations: Published/Full Citation Provided: Manuscript is in print. In Press: Manuscript
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Aortic Valve Stenosis and TAVR: Putting it all together.
 Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Disclosures 4/16/2018. What s New in Valvularand Structural Heart Disease. None relevant to the presentation
 What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results
 The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results Nicolas M. Van Mieghem, MD, PhD, FESC Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Disclosure Statement
The Sentinel Dual Filter Device Design Features & EU Clinical Trial Results Nicolas M. Van Mieghem, MD, PhD, FESC Director of Interventional Cardiology Thoraxcenter, Erasmus MC Rotterdam Disclosure Statement
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate