Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients:
|
|
|
- Frank Banks
- 6 years ago
- Views:
Transcription
1 Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van Mieghem, MD, PhD, FACC, FESC For the SURTAVI Investigators
2 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Financial Relationship Consultant (fees paid to institution) Grant/Research Support & consulting Fees Company Medtronic Abbott, Boston Scientific, Edwards Lifesciences, Medtronic, Acist, Claret, Terumo, PulseCath
 1, and is superior in patients at high risk for operative mortality at 30 days.")
3 Background Self-expanding transcatheter aortic valve replacement (TAVR) is preferred to medical therapy in patients with severe, symptomatic aortic stenosis (AS) deemed prohibitive for surgical aortic valve replacement (SAVR) 1, and is superior in patients at high risk for operative mortality at 30 days. 2 The comparative efficacy of TAVR and SAVR has been less well studied in patients at lower surgical risk. The SURTAVI trial was conducted to determine whether TAVR with a self-expanding CoreValve or Evolut R is non-inferior to surgical AVR for all-cause mortality or disabling stroke at 24 months in patients with severe AS at intermediate surgical risk. 1 Popma J, Adams D, Reardon M, et al. J Am Coll Cardiol Adams D, Popma J, Reardon M, et al. New Engl J Med


4 4 Bayesian Analysis of the 24-Month Primary Endpoint A pre-specified interim analysis occurred when 1400 patients reached 12-month follow-up. Observed 24-month outcomes Interim were Bayesian used Analysis to inform of the 2Year modeling. Primary Endpoint timed to occur when 1400 subjects Subjects have been who followed had for not 12 months reached Analysis 24-month using modeling follow-up to include had all patient their data outcomes imputed using their last known event status. Combining imputed and observed data, the posterior distribution of the difference in 24-month event rates was calculated.

5 Primary Endpoint This Bayesian method demonstrated that the trial met its primary endpoint 1 1 Reardon M, Van Mieghem N, Popma J, et al. New Engl J Med 2017
6 6 Objective The 1-year follow-up for all 1,660 patients treated in SURTAVI is now complete Also complete is the 30-day follow-up for 275 patients who underwent TAVR as part of a non-randomized continued access study The purpose of this presentation is to report the outcomes for both of these patient cohorts
7 Study Timeline 2012 June SURTAVI First patient enrolled CoreValve: 23, 26, 29 mm (US) April 2015 Evolut R (US) June Sept Dec Jul Oct CoreValve: 23, 26, 29 mm (CAN, EU) CoreValve: 31 mm (US, CAN, EU) SURTAVI RCT 2 Yr Outcomes TCT 2018 SURTAVI Enrollment complete CAS First patient enrolled Evolut R: 23, 26, 29 mm CoreValve: 31 mm Primary endpoint assessment CAS Enrollment complete SURTAVI 1-Year follow-up complete 7
 94% TF 4% DA 2% SCA Evolut R (n=139) 16%")
")
8 Study Features SURTAVI RCT 17 sites 65 sites 5 sites CoreValve (n=724) 94% TF 4% DA 2% SCA Evolut R (n=139) 16% second generation valves SURTAVI CAS 59 sites 95.6% TF 0.4% DA 4% SCA 93% second generation valves CoreValve (n=20) Evolut R (n=254) 8

9 Patient Flow Randomized Controlled Trial (RCT) 1746 patients Continued Access Study (CAS) 290 patients TAVR ITT group: N= not attempted: - 4 died - 6 withdrew consent - 5 physician withdrew TAVR mitt* group: N=864 SAVR ITT group: N= not attempted: - 4 died - 43 withdrew consent - 23 physician withdrew - 1 lost to follow-up SAVR mitt* group: N= not attempted: - 1 died - 2 withdrew consent - 11 physician withdrew - 1 pending procedure TAVR attempted implant: N=275 2 not implanted 1 went to SAVR 2 surgical patients received TAVR 1 not implanted 2 went to TAVR 1 TAVR patient received SAVR 1 not implanted TAVR implanted group: N=863 SAVR implanted group: N=794 TAVR implanted group: N=274 *The modified intention-to-treat (mitt) population includes all subjects with an attempted procedure 9
10 Baseline Characteristics n (%) or mean ± SD RCT* SAVR (N=796) TAVR (N=864) Age, years 79.7 ± ± 6.2 Male sex 438 (55.0) 498 (57.6) Body surface area, m ± ± 0.2 STS PROM, % 4.5 ± ± 1.5 Logistic EuroSCORE, % 11.6 ± ± 7.6 Diabetes mellitus 227 (34.8) 295 (34.1) Serum creatinine >2 mg/dl 17 (2.1) 14 (1.6) Prior stroke 57 (7.2) 57 (6.6) Prior TIA 46 (5.8) 58 (6.7) Peripheral vascular disease 238 (29.9) 266 (30.8) Pre-existing IPG / ICD 72 (9.9) 87 (10.1) *mitt population; no significant difference in any baseline characteristics CAS TAVR (N=275) 79.0 ± (46.2) 1.9 ± ± ± (36.4) 2 (0.7) 16 (5.8) 8 (2.9) 71 (25.8) 19 (6.9) 10
11 Baseline Frailty, Disabilities and Comorbidities* n (%) or mean ± SD RCT* CAS SAVR (N=796) TAVR (N=864) TAVR (N=275) Body mass index <21 kg/m 2 21 (2.6) 20 (2.3) Falls in past 6 months 101 (12.7) 102 (11.8) 5 meter gait speed >6 s 403 (52.9) 428 (51.8) 6 minute walk test (meters) ± ± Grip strength below threshold 489 (63.0) 519 (62.5) Does not live independently 22 (2.8) 18 (2.1) Chronic lung disease (mod/severe) 106 (13.3) 115 (13.3) Home oxygen 21 (2.6) 18 (2.1) Cirrhosis of the liver 5 (0.6) 4 (0.5) Immunosuppressive therapy 68 (8.5) 64 (7.4) 7 (2.5) 23 (8.4) 116 (44.3) ± (66.7) 7 (2.5) 50 (18.2) 2 (0.7) 2 (0.7) 16 (5.8) *mitt population; no significant difference in any baseline characteristics 11

12 RESULTS 12
13 All-Cause Mortality or Disabling Stroke 30% All-Cause Mortality or Disabling Stroke 25% 20% 15% 10% 5% TAVR SAVR P-value (log-rank) = % 7.8% No. at Risk SAVR TAVR 0% Months Post-Procedure
14 All-Cause Mortality 30% 25% TAVR All-Cause Mortality 20% 15% 10% 5% SAVR P-value (log-rank) = % 6.5% No. at Risk SAVR TAVR 0% Months Post-Procedure
15 Disabling Stroke 30% Disabling Stroke No. at Risk SAVR TAVR 25% 20% 15% 10% 5% 0% TAVR SAVR P-value (log-rank) = Months Post-Procedure % 2.1% 15
16 All Stroke 30% 25% TAVR All Stroke 20% 15% 10% 5% SAVR P-value (log-rank) = % 5.2% No. at Risk SAVR TAVR 0% Months Post-Procedure
17 NYHA Functional Class % of Patients 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% p=0.42 p<0.01 p= % 4.4% 54.7% 53.6% 40.0% 41.2% 0.3% 0.8% TAVR (N=860) Baseline SAVR (N=789) 0.2% 1.1% 0.4% 0.2% 5.6% 9.6% 4.2% 4.3% 30.7% 63.5% TAVR (N=822) 30 Days 36.4% 52.8% SAVR (N=708) 24.2% 25.6% 71.2% 70.0% TAVR (N=732) 1 Year SAVR (N=606) IV III II I 17

18 KCCQ Summary Score Over Time 100 KCCQ Summary Score Baseline 30 Days 6 Months 12 Months Change from Baseline TAVR 18.4 ± ± ± 22.3 SAVR 5.9 ± ± ± 22.2 P < TAVR SAVR 18
19 6 Minute Walk Test Change from Baseline p<0.01 p< N=709 N=624 N=501 N= Day 12 Months TAVR SAVR Change is increase or decrease in meters walked in 6 minutes 19
20 Procedural Overview % or mean ± SD RCT SAVR (N=796) TAVR (N=864) General anesthesia, % Procedure time, min ± ± 32.7 Total time in cath lab or OR, min ± ± 61.3 Pre-procedure BAV NA 47.2 Post-dilatation NA 29.0 More than 1 valve implanted, % NA 6.7 Length of index procedure hospital stay, days Length of ICU stay, hours 9.8 ± ± 4.9 (n=778) 70.4 ± 96.2 (n=767) 48.6 ± 44.0 Aortic cross-clamp time, min 74.3 ± 30.4 NA CPB time, min 97.8 ± 39.3 NA CAS TAVR (N=275) ± ± ± 2.6 (n=225) 32.8 ± 32.3 NA NA 20
21 Clinical Outcomes at 30 Days RCT CAS SAVR (N=796) TAVR (N=864) P All-cause mortality or disabling stroke All-cause mortality Disabling stroke All stroke Life-threatening or major bleeding Transfusion of PRBCs* -n(%) 328 (41.2) 108 (12.5) <0.01 Acute kidney injury, stage <0.01 Major vascular complications <0.01 Permanent pacemaker implant <0.01 Atrial fibrillation <0.01 Myocardial infarction *Percentage rates, all others are Kaplan-Meier rates TAVR (N=275) (5.1)
22 Hemodynamics* TAVR had significantly better valve performance over SAVR at all follow-up visits (P<0.001) Aortic Valve Area, cm TAVR SAVR TAVR CAS Baseline Discharge 6 Months 1 Year AV Mean Gradient, mm Hg *Core lab adjudicated 22
23 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Total Aortic Regurgitation* 0.7% 6.8% 92.5% SAVR (N=707) None/trace Mild Moderate Severe 0.2% 3.2% 35.9% 60.6% TAVR (N=832) 0.7% 8.3% 91.0% SAVR (N=602) 5.2% 34.0% 60.8% TAVR (N=718) RCT Discharge RCT 1 Year * Implanted population, core lab adjudicated 23
24 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Total Aortic Regurgitation* 0.7% 6.8% 92.5% SAVR (N=707) None/trace Mild Moderate Severe 0.2% 3.2% 35.9% 60.6% TAVR (N=832) 1.1% 22.6% 76.3% TAVR (N=266) RCT Discharge CAS Discharge * Implanted population, core lab adjudicated 24
25 Conclusion 25 The 1-year results from the SURTAVI randomized trial demonstrate that TAVR with the self-expanding Evolut R or CoreValve has similar outcomes compared to SAVR in terms of all-cause mortality or disabling stroke in patients at intermediate surgical risk TAVR patients had a faster improvement in quality of life, as well as superior functional status which was maintained to 1 year The 30-day results from the Continued Access Study demonstrate that the combination of operator experience and next-generation technology lead to fewer complications and improved clinical outcomes for patients
26 Functional Status after Transcatheter and Surgical Aortic Valve Replacement A sub-analysis from the SURTAVI Trial Jeffrey J. Popma, MD For the SURTAVI Investigators
27 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Financial Relationship Institutional Grants Institutional Grants; Medical Advisory Board Institutional Grants Institutional Grants; Consultant Company Medtronic Boston Scientific Abbott Edwards
28 Background The SURTAVI trial has shown that transcatheter aortic valve replacement (TAVR) is an alternative to surgery (SAVR) in intermediate-risk patients with severe, symptomatic aortic stenosis 1. Of specific interest is the clinical recovery pattern that patients experience following TAVR and SAVR. There are 2 goals to this sub-analysis from SURTAVI: to characterize how and when patients recover functionality and quality of life following aortic valve replacement To identify recovery patterns specifically related to transcatheter vs. surgical treatment 1 Reardon M, Van Mieghem N, Popma J, et al. New Engl J Med 2017
29 Patient Flow 1,746 patients randomized TAVR ITT group: N=879 SAVR ITT group: N= not attempted: - 4 died - 6 withdrew consent - 5 physician withdrew 71 not attempted: - 4 died - 43 withdrew consent - 23 physician withdrew - 1 lost to follow-up TAVR mitt* group: N=864 SAVR mitt* group: N=796 2 not implanted 1 went to SAVR 2 surgical patients received TAVR 1 not implanted 2 went to TAVR 1 TAVR patient received SAVR TAVR implanted group: N=863 SAVR implanted group: N=794 *The modified intention-to-treat (mitt) population includes all subjects with an attempted procedure
30 Methods Measures of functional status and quality of life were collected at baseline, 30 days, 6 months, and 1 year following treatment Patients were divided according to treatment arm, and then further separated into 3 categories based on meters walked in 6 minutes at baseline: <150 meters meters >400 meters For these patient groups, changes in meters walked at each time point relative to baseline were analyzed. These functional changes were then correlated to quality of life scores, as measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ)

31 Key Definitions Clinically meaningful improvement in functional status: either an increase in 40m walked in 6 minutes relative to baseline or a 10% relative improvement Meaningful improvement in KCCQ score: 10 points relative to baseline
32 Baseline 6 Minute Walk Test The 3 patient groups were well balanced between TAVR and SAVR, with the majority of patients walking between 150 and 400 meters at baseline Percent of Patients 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 8.4% 10.3% 72.7% 71.4% 19.0% 18.3% TAVR SAVR >400 m m <150 m
33 Baseline Characteristics TAVR (N=864) SAVR (N=796) n (%) or mean ± SD <150 m N= m N=583 >400 m N=67 <150 m N= m N=493 >400 m N=71 Age, years 80.7 ± ± ± ± ± ± 5.1 Male sex 63 (41.4) 349 (59.9) 55 (82.1) 53 (42.1) 288 (58.4) 48 (67.6) Body surface area, m ± ± ± ± ± ± 0.2 STS PROM, % 4.8 ± ± ± ± ± ± 1.7 Diabetes mellitus 54 (35.5) 199 (34.1) 16 (23.9) 65 (51.6) 163 (33.1) 15 (21.1) Serum creatinine >2 mg/dl 5 (3.3) 9 (1.5) 0 (0.0) 3 (2.4) 7 (1.4) 2 (2.8) Prior stroke 7 (4.6) 40 (6.9) 7 (10.4) 15 (11.9) 27 (5.5) 6 (8.5) Prior TIA 14 (9.2) 30 (5.1) 5 (7.5) 8 (6.3) 33 (6.7) 0 (0) Peripheral vascular disease 52 (34.2) 171 (29.3) 17 (25.4) 41 (32.5) 150 (30.4) 16 (22.5) Pre-existing IPG/ICD 19 (12.5) 57 (9.8) 5 (7.5) 13 (10.3) 53 (10.8) 1 (1.4)
34 Baseline Cardiac Risk Factors TAVR (N=864) SAVR (N=796) n (%) or mean ± SD <150 m N= m N=583 >400 m N=67 <150 m N= m N=493 >400 m N=71 Coronary artery disease 88 (57.9) 370 (63.5) 42 (62.7) 69 (54.8) 333 (67.5) 37 (52.1) Prior CABG 17 (11.2) 96 (16.5) 15 (22.4) 16 (12.7) 92 (18.7) 13 (18.3) Prior PCI 28 (18.4) 126 (21.6) 15 (22.4) 19 (15.1) 113 (22.9) 14 (19.7) Prior myocardial infarction 17 (11.2) 87 (14.9) 12 (17.9) 16 (12.7) 70 (14.2) 11 (15.5) Congestive heart failure 149 (98.0) 552 (94.7) 62 (92.5) 124 (98.4) 475 (96.3) 68 (95.8) History of arrhythmia 51 (33.6) 187 (32.1) 20 (29.9) 45 (35.7) 153 (31.0) 16 (22.5) Atrial fibrillation / flutter 44 (28.9) 165 (28.3) 19 (28.4) 41 (32.5) 127 (25.8) 12 (16.9) NYHA III / IV 118 (77.6) 333 (57.1) 31 (46.3) 98 (77.8) 267 (54.2) 27 (38.0)
35 Baseline Frailty, Disabilities and Comorbidities* TAVR (N=864) n (%) or mean ± SD <150 m N= m N=583 >400 m N=67 <150 m N=126 SAVR (N=796) m N=493 >400 m N=71 Body mass index <21 kg/m 2 1 (0.7) 17 (2.9) 2 (3.0) 2 (1.6) 9 (1.8) 5 (7.0) Falls in the past 6 months 30 (19.7) 63 (10.8) 1 (1.5) 17 (13.5) 61 (12.4) 3 (4.2) Grip strength below threshold Does not live independently Moderate / severe lung disease 107 (73.3) 337 (60.2) 31 (48.4) 82 (67.2) 306 (63.2) 29 (42.0) 5 (3.3) 7 (1.2) 3 (4.5) 4 (3.2) 12 (2.4) 3 (4.2) 21 (13.8) 77 (13.3) 9 (13.4) 18 (14.3) 65 (13.2) 5 (7.0) Home oxygen 8 (5.3) 8 (1.4) 0 (0.0) 5 (4.0) 7 (1.4) 0 (0.0)
36 RESULTS
37 6 Minute Walk Test Change from Baseline The degree of improved functionality and the time course of recovery differed according to treatment modality p< p< N=709 N=624 N=501 N= Days 1 Year Change is increase or decrease in meters walked in 6 minutes TAVR SAVR
38 6 Minute Walk Test At 30 days, almost 50% of TAVR patients experienced clinically meaningful improvement in functional status, as compared to 30% of SAVR patients 100% % patients with meaningful improvement 80% 60% 40% 20% 0% 47.8% 51.0% 44.5% 32.0% N=709 N=624 N=528 N=501 TAVR SAVR 30 Days 1 Year
39 Follow-up 6 Minute Walk Test Patients with the most limited mobility at baseline were the most likely to experience a meaningful improvement in mobility after treatment. Patients with the best mobility at baseline didn t have a measurable change following treatment 100% 80% 60% 40% 20% 0% 84.5% 84.4% 75.8% 58.1% 45.0% 47.1% 41.9% 29.2% 25.0% 13.1% 13.8% 9.8% N=128 N=97 N=86 N=77 N=520 N=471 N=377 N=363 N=61 N=56 N=65 N=61 TAVR SAVR TAVR SAVR TAVR SAVR <150 m m >400 m 30 Days 1 Year
40 KCCQ Summary Score Patients with a meaningful improvement in functional status had a better quality of life at both 30 days and 1 year % patients with KCCQ improvement 10 points at 30 days 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 73.4% 54.5% 64.5% 35.5% N=338 N=484 N=166 N=547 Yes No Yes No TAVR SAVR Meaningful Improvement in Functional Status
41 KCCQ Summary Score % patients with KCCQ improvement 10 points at 1 year 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 77.8% 74.1% 62.4% 59.2% N=317 N=420 N=221 N=407 Yes No Yes No TAVR SAVR Meaningful Improvement in Functional Status
42 Summary TAVR patients had significantly better functional status than SAVR patients at both 30 days and 1 year following treatment. The group of patients deriving the most functional improvement from aortic valve replacement had the most limited mobility at baseline. Prior to treatment, approximately 20% of patients were unable to walk 150 meters in 6 minutes. They were more often female, in NYHA Class III / IV, and frail relative to the rest of the SURTAVI population. More than half of them showed a clinically meaningful improvement as a result of treatment, regardless of modality.
43 Summary Patients with a clinically meaningful improvement in functional status had better quality of life than those patients that did not have improved functionality We conclude that in intermediate surgical risk severe aortic stenosis patients, functional status recovered more quickly and to a greater extent in TAVR patients as compared to SAVR patients. This translated into better quality of life for these patients.
44 30-Day Outcomes in Patients with a Society of Thoracic Surgeons Predicted Risk of Mortality < 3% from the Evolut R FORWARD Study Eberhard Grube, MD, PhD For the Evolut R FORWARD Study Investigators
45 BACKGROUND Benefits of TAVR include shorter length of stay, less AKI, less AF, quicker quality of life recovery and better hemodynamics than surgery. 1,2 TAVR is now an appropriate alternative to surgical AVR in patient at intermediate risk. 3,4 The multicenter Evolut R FORWARD Study assessed 1038 patients with symptomatic aortic stenosis at increased surgical risk who underwent transcatheter aortic valve replacement (TAVR) with the Evolut R valve in a routine hospital setting. The 30-day mortality rate was 1.9% and disabling stroke was 1.8%. In anticipation of the reporting from current randomized trials evaluating TAVR in patients at lower surgical risk, we performed a post-hoc analysis in patients with an STS predicted risk of mortality < 3.0%. 1 Adams DH, et al. N Engl J Med 2014; 270: ; 2 Smith CR, et al. N Engl J Med 2011;364: ; Leon MB, et al. 2016; 374: ; 4 Reardon MJ, et al. N Engl J Med 2017;376:

46 BACKGROUND 30-Day All-Cause Mortality in Intermediate Risk Reardon MJ, et al, JAMA Cardiol 2016;1:945-9; Wenaweser P, et al, Eur Heart J 2013; 34: ; Lange, et al, J Am Coll Cardiol 2012; 59: 280-7; Barbanti M, et al, Am J Cardiol 2016; 117: 820-7; Leon MB, et al, N Engl J Med 2016:374: ; Kodali S, et al., Eur Heart J 2016; 37: ; Reardon MJ, et al. N Engl J Med 2017; 376: ; Thourani VH, et al, Ann Thorac Surg 2015; 99:


47 CURRENT GUIDELINES RECOMMEND SURGERY FOR PATIENTS DEEMED AT LOW SURGICAL RISK 2017 ACC/AHA Focused Update ESC /EACTS Guidelines 2 Choice of intervention in symptomatic aortic stenosis Class Level SAVR is recommended in patients at low surgical risk (STS or EuroSCORE II< 4% or logistic EuroSCORE I< 10% and no other risk factors not included in these scores, such as frailty, porcelain aorta, sequelae of chest radiation). I B 1 Nishimura R, et al. J Am Coll Cardiol 2017;70: ; 2 Baumgartner H, et al. Eur Heart J 2017; Aug 26. doi: /eurheartj/ehx391. [epub ahead of print] TCT
48 DEFINING LOW-RISK PATIENTS FOR TAVR Ongoing randomized trials define low risk as: 1. Heart Team agreement of low 30-day risk (STS PROM < 3%) 1 OR 2. Operative mortality < 2% for SAVR 2 1 Medtronic TAVR in low risk (NCT ); 2 PARTNER 3 (NCT ) 5
49 METHODS The Evolut R FORWARD Study documented the safety and effectiveness of TAVR in patients undergoing TAVR in a routine hospital setting. Patient eligibility not solely based on STS Score* Age 80 years OR High risk for SAVR where high risk is defined as: STS PROM 8% OR Heart Team agreement of risk for SAVR due to frailty or comorbidities Post-hoc analysis of patients with an STS < 3% *Per protocol. CE Marking for patients at intermediate surgical risk was received during the trial. Inclusion eligibility was determined per local Instructions for Use. 6
50 BASELINE CHARACTERISTICS Characteristic, mean ± SD or % STS < 3% N=257 STS 3% N=781 P Value Age, years 77.9 ± ± 5.4 <0.001 Female < BSA, m ± ± 0.2 <0.001 STS PROM, % 2.2 ± ± 4.7 <0.001 Logistic EuroSCORE, % 11.3 ± ± 12.0 <0.001 EuroSCORE II, % 3.3 ± ± 5.3 <0.001 NYHA Class 0.06 I II III IV
51 STS BASELINE FACTORS Characteristic, % STS Factors STS < 3% N=257 STS 3% N=781 P Value Diabetes mellitus < Serum creatinine >2 mg/dl < Dialysis Chronic lung disease (COPD) < Peripheral arterial disease < Cerebrovascular disease Previous CABG Previous PCI Previous MI Atrial fibrillation
52 NON-STS BASELINE FACTORS Characteristic, % STS < 3% N=257 STS 3% N=781 P Value Non-STS Factors Katz score < Frailty Porcelain aorta Pulmonary hypertension Implanted cardiac device Evidence of radiation damage Abnormal chest wall anatomy Severely atherosclerotic aorta
53 PROCEDURAL OUTCOMES STS < 3% N=257 STS 3% N=781 P Value Characteristic, % Anesthesia < General Local/conscious sedation Access < Iliofemoral Subclavian Direct aortic Pre-BAV Post-BAV EnVeo InLine sheath Implanted Valve Size mm mm mm More than 1 valve implanted

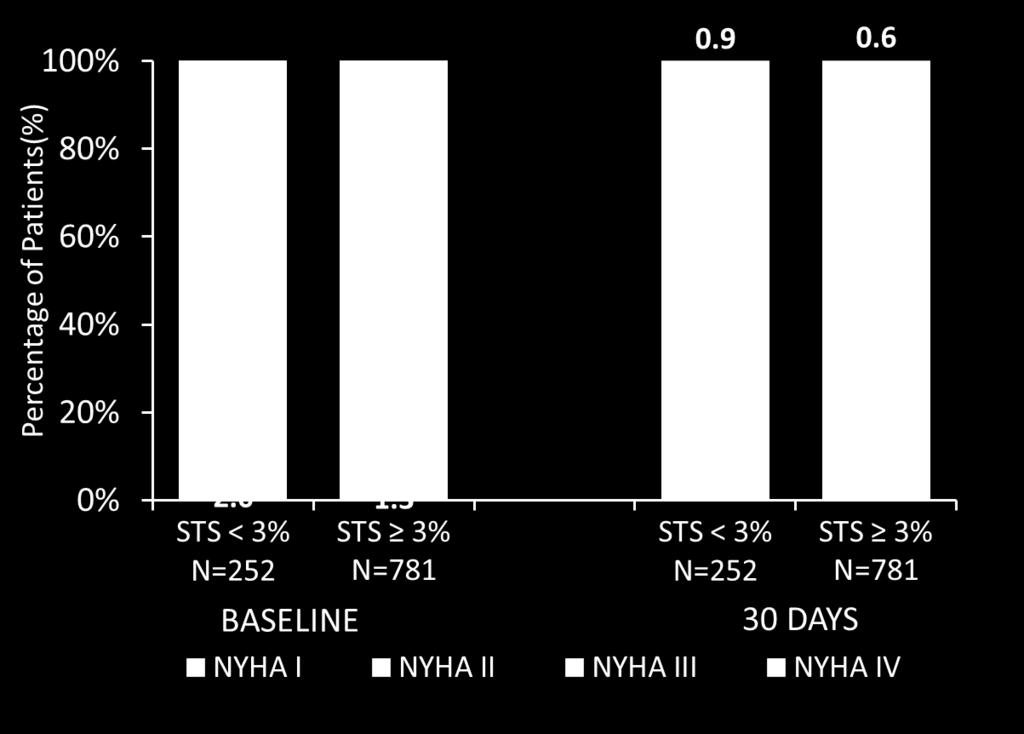
54 NYHA CLASSIFICATION 11

55 SAFETY OUTCOMES AT 30 DAYS Kaplan-Meier rates as %. 12
56 SUMMARY In this routine practice study, 25% of enrolled patients had an STS < 3%, yet they were considered at elevated operative risk: Nearly 30% were frail 40% had pulmonary hypertension >10% had porcelain aorta or significant aortic calcification Symptom improvement at 30 days was similar regardless of STS There were no differences in 30-day outcomes except major bleeding, which may be attributed to differences in vascular status as significantly more patients with an STS 3% had PVD. The Evolut R FORWARD Study did not assess low-risk patients. The feasibility of TAVR in low-risk patients needs to be confirmed in dedicated randomized trials. 13
LOW RISK TAVR. WHAT THE FUTURE HOLDS
 LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and
 Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
Outcomes in the Commercial Use of Self-expanding Prostheses in Transcatheter Aortic Valve Replacement: A Comparison of the Medtronic CoreValve and Evolut R platforms in the Society of Thoracic Surgeons/American
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the FORWARD Study
 30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
For the SURTAVI Investigators
 Neurological complications after transcatheter aortic valve implantation with a self-expanding bioprosthesis or surgical aortic valve replacement in patients at intermediate-risk for surgery A. Pieter
Neurological complications after transcatheter aortic valve implantation with a self-expanding bioprosthesis or surgical aortic valve replacement in patients at intermediate-risk for surgery A. Pieter
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Open vs TAVR vs Nothing
 Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI limitations for low risk patients
 TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes
 SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
SAPIEN 3: Evaluation of a Balloon- Expandable Transcatheter Aortic Valve in High-Risk and Inoperable Patients With Aortic Stenosis One-Year Outcomes Howard C. Herrmann, MD on behalf of The PARTNER II Trial
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation
 The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
The FORMA Early Feasibility Study: 30-Day Outcomes of Transcatheter Tricuspid Valve Therapy in Patients with Severe Secondary Tricuspid Regurgitation Susheel Kodali, MD Director, Structural Heart & Valve
TAVR: Review of the Robust Data from Randomized Trials
 TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Ian T. Meredith AM. MBBS, PhD, FRACP, FCSANZ, FACC, FAPSIC. Monash HEART, Monash Health & Monash University Melbourne, Australia
 Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
The Role of TAVI in high-risk and normal-risk Patients
 The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
TAVR in 2017 What we know? What to expect?
 Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Strokes After TAVR: Perspectives from the US CoreValve Trials
 Strokes After TAVR: Perspectives from the US CoreValve Trials Jeffrey J. Popma, MD Professor of Medicine Harvard Medical School Director, Interventional Cardiology Clinical Services Beth Israel Deaconess
Strokes After TAVR: Perspectives from the US CoreValve Trials Jeffrey J. Popma, MD Professor of Medicine Harvard Medical School Director, Interventional Cardiology Clinical Services Beth Israel Deaconess
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
Evolving and Expanding Indications for TAVR
 Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Transcatheter Aortic Valve Implantation for Aortic Stenosis Page 1 of 37 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Transcatheter Aortic Valve Implantation
Transcatheter Aortic Valve Implantation for Aortic Stenosis Page 1 of 37 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Transcatheter Aortic Valve Implantation
Vinod H. Thourani, MD, FACC, FACS
 Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Transcatheter Aortic-Valve Implantation for Aortic Stenosis
 Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 6/2018 Origination: 2/2012 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 6/2018 Origination: 2/2012 Next Review: 2/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Transcatheter Aortic-Valve Implantation for Aortic Stenosis
 Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 2/2019 Origination: 2/2012 Next Review: 2/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: 7.01.132 Last Review: 2/2019 Origination: 2/2012 Next Review: 2/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Strokes After TAVR Reasons for Declining Frequency
 Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y.
 Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
Appropriate Patient Selection or Healthcare Rationing? Lessons from Surgical Aortic Valve Replacement in The PARTNER I Trial Wilson Y. Szeto, MD on behalf of The PARTNER Trial Investigators and The PARTNER
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
TAVR for Complex Aortic Valvular Conditions
 TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
TAVR for Complex Aortic Valvular Conditions Wilson Y. Szeto, MD Professor of Surgery Chief, Cardiovascular Surgery at Penn Presbyterian Surgical Director, Transcatheter Cardio-Aortic Therapies Associate
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS
 Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Establishing a New Path Forward for Patients With Severe Symptomatic Aortic Stenosis THE PARTNER TRIAL CLINICAL RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T h e Pa
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
State of the Art and Future perspective
 State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
Current Evidence in TAVI patients using ACURATE and LOTUS valves
 Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Current Evidence in TAVI patients using ACURATE and LOTUS valves Giuseppe Tarantini, MD, PhD, FESC, Professor and Director of Interventional Cardiology University of Padua GISE President Potential conflicts
Results of Transfemoral Transcatheter Aortic Valve Implantation
 Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Results of Transfemoral Transcatheter Aortic Valve Implantation Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial. Martin B. Leon, MD
 8 mins Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City
8 mins Sentinel Dual Filter Device: Technology Overview and Status of the CLEAN-TAVI Randomized Trial Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New York City
L evoluzione nel management della valvulopatia aortica
 L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Transcatheter aortic valve replacement is considered investigational for all other indications.
 Medical Policy Original Policy Date: March 30, 2012 Effective Date: July 1, 2018 Section: 7.0 Surgery Page: Page 1 of 33 Policy Statement Transcatheter aortic valve replacement with an U.S. Food and Drug
Medical Policy Original Policy Date: March 30, 2012 Effective Date: July 1, 2018 Section: 7.0 Surgery Page: Page 1 of 33 Policy Statement Transcatheter aortic valve replacement with an U.S. Food and Drug
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
TAVI: Nouveaux Horizons
 TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Transcatheter Aortic-Valve Implantation for Aortic Stenosis
 Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: Original Effective Date: MM.06.019 10/01/2012 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 07/27/2018
Transcatheter Aortic-Valve Implantation for Aortic Stenosis Policy Number: Original Effective Date: MM.06.019 10/01/2012 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 07/27/2018
Eberhard Grube MD, FACC, FSCAI
 3 rd TAVI Summit Seoul, August 9/10, 2013 Eberhard Grube MD, FACC, FSCAI University Hospital, Dept of Medicine II, Bonn, Germany y p, p,, y Hospital Alemão Oswaldo Cruz, São Paulo, Brazil Stanford University,
3 rd TAVI Summit Seoul, August 9/10, 2013 Eberhard Grube MD, FACC, FSCAI University Hospital, Dept of Medicine II, Bonn, Germany y p, p,, y Hospital Alemão Oswaldo Cruz, São Paulo, Brazil Stanford University,
Early Experience of Transcatheter Mitral Valve Replacement Results from the Intrepid Global Pilot Study
 Early Experience of Transcatheter Mitral Valve Replacement Results from the Paul Sorajja, MD for the Investigators Presenter Disclosure Information Within the past 12 months, I or my spouse/partner have
Early Experience of Transcatheter Mitral Valve Replacement Results from the Paul Sorajja, MD for the Investigators Presenter Disclosure Information Within the past 12 months, I or my spouse/partner have
TAVR in 2020: What is Next!!!!
 TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
Update on the CoreValve Experience
 TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
TCT Asia Pacific April 22-24, 2009 Update on the CoreValve Experience Eberhard Grube HELIOS Klinikum, Germany Instituto Dante Pazzanese de Cardiología, São Paulo, Brazil Stanford University, Palo Alto,
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients
 O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
TAVR y Enfermedad Coronaria. Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine
 TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
TAVR y Enfermedad Coronaria Mauricio G. Cohen, MD, FACC, FSCAI Director, Cardiac Catheterization Lab Associate Professor of Medicine CAD and AS Similar Pathological Processes CAD in TAVR Patients (n=390)
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK
 Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK") Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system
 Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system Preliminary Results: Acute and 1-year Outcomes Ganesh Manoharan, MBBCh, MD, FRCP Consultant Cardiologist
Multicentre clinical study evaluating a novel resheatable self-expanding transcatheter aortic valve system Preliminary Results: Acute and 1-year Outcomes Ganesh Manoharan, MBBCh, MD, FRCP Consultant Cardiologist
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement with a Repositionable Self-expanding Bioprosthesis in Patients With Severe Aortic Stenosis Suboptimal for
 Transcatheter Aortic Valve Replacement with a Repositionable Self-expanding Bioprosthesis in Patients With Severe Aortic Stenosis Suboptimal for Surgery: One-Year Results from the Evolut R US Pivotal Study
Transcatheter Aortic Valve Replacement with a Repositionable Self-expanding Bioprosthesis in Patients With Severe Aortic Stenosis Suboptimal for Surgery: One-Year Results from the Evolut R US Pivotal Study
Accepted Manuscript. Sixteen Years Later and the Debate for TAVR or SAVR Remains Controversial. Saina Attaran, MD, Vinod H.
 Accepted Manuscript Sixteen Years Later and the Debate for TAVR or SAVR Remains Controversial Saina Attaran, MD, Vinod H. Thourani, MD PII: S0022-5223(18)30624-X DOI: 10.1016/j.jtcvs.2018.02.080 Reference:
Accepted Manuscript Sixteen Years Later and the Debate for TAVR or SAVR Remains Controversial Saina Attaran, MD, Vinod H. Thourani, MD PII: S0022-5223(18)30624-X DOI: 10.1016/j.jtcvs.2018.02.080 Reference:
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial
 Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
Health Status after Transcatheter Mitral- Valve Repair in Patients with Heart Failure and Secondary Mitral Regurgitation: Results from the COAPT Trial Suzanne V. Arnold, MD, MHA Saint Luke s Mid America
Strokes After TAVR. Ioannis Iakovou, MD, PhD. Interventional Cardiology Onassis Cardiac Surgery Center
 Strokes After TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Strokes After TAVR How common is stroke after TAVR Is it increasing? Is it more with TF vs TA? Is it
Strokes After TAVR Ioannis Iakovou, MD, PhD Interventional Cardiology Onassis Cardiac Surgery Center Strokes After TAVR How common is stroke after TAVR Is it increasing? Is it more with TF vs TA? Is it
How to Prevent Thromboembolic Complications in TAVI
 How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Disclosures. LGH TAVR: Presentation Outline 2/2/2016. Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience
 and the LGH Experience") Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era
 Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era Sebastian A. Iturra, Rakesh M. Suri, Kevin L. Greason, John
Outcomes of Surgical Aortic Valve Replacement in Moderate Risk Patients: Implications for Determination of Equipoise in the Transcatheter Era Sebastian A. Iturra, Rakesh M. Suri, Kevin L. Greason, John
CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE
 ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
ESC Congress 2011 27 Aug - 31 Aug 2011, Paris - France CARDIAC REHABILITATION AFTER TRANSCATHETER AORTIC VALVE IMPLANTATION: A SINGLE CENTRE EXPERIENCE N.Russo, L.Compostella, T.Setzu, M.Napodano, L.Testolin,
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Valve Stenosis and TAVR: Putting it all together.
 Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Repair or Replacement
 Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
Surgical intervention post MitraClip Device: Repair or Replacement Saudi Heart Association, February 21-24 Rüdiger Lange, MD, PhD Nicolo Piazza, MD, FRCPC, FESC German Heart Center, Munich, Germany Division
SOLVE-TAV. Holger Thiele, MD on behalf of the SOLVE-TAVI Investigators
 SOLVE-TAV A 2x2 Randomized Trial of Self-Expandable vs Balloon-Expandable Valves and General vs Local Anesthesia in Patients Undergoing Transcatheter Aortic Valve Implantation Holger Thiele, MD on behalf
SOLVE-TAV A 2x2 Randomized Trial of Self-Expandable vs Balloon-Expandable Valves and General vs Local Anesthesia in Patients Undergoing Transcatheter Aortic Valve Implantation Holger Thiele, MD on behalf
Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence
 Evidence") X Congreso Coilegio Colombiano Santiago de Cali, 29-31 Octubre des 2014 Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence Eberhard Grube MD, FACC, FSCAI University
X Congreso Coilegio Colombiano Santiago de Cali, 29-31 Octubre des 2014 Lotus Valve System for Transcatheter Aortic Valve Implantation/Replacement (TAVI/R) Evidence Eberhard Grube MD, FACC, FSCAI University
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR)
") Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Minimalist Transcatheter Aortic Valve Replacement (MA-TAVR) Jensen HA, Condado JF, Devireddy C, Binongo JN, Leshnower BG, Babaliaros V, Sarin EL, Lerakis S, Guyton RA, Stewart JP, Syed AQ, Mavromatis K,
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis
 Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Eberhard Grube, MD, FACC, FSCAI
 TCT Asia Seoul, April 29, 2010 MDT / Core Valve Device Evolution, Technique and Clinical Trial Update Eberhard Grube, MD, FACC, FSCAI Intl. Heart Center Rhein-Ruhr, Essen, Germany Hospital Oswaldo Cruz
TCT Asia Seoul, April 29, 2010 MDT / Core Valve Device Evolution, Technique and Clinical Trial Update Eberhard Grube, MD, FACC, FSCAI Intl. Heart Center Rhein-Ruhr, Essen, Germany Hospital Oswaldo Cruz
Prospective Evaluation of the Eyeball Test for Assessing Frailty in Elderly Patients with Valvular Heart Disease
 Prospective Evaluation of the Eyeball Test for Assessing Frailty in Elderly Patients with Valvular Heart Disease Background Frailty is a common occurrence in elderly patients Approximately half of the
Prospective Evaluation of the Eyeball Test for Assessing Frailty in Elderly Patients with Valvular Heart Disease Background Frailty is a common occurrence in elderly patients Approximately half of the
Percutaneous mitral valve repair: current techniques and results
 Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Percutaneous mitral valve repair: current techniques and results Ted Feldman, M.D., FSCAI, FACC Angioplasty Summit April 25-27 th th 2007 Seoul, Korea Ted Feldman MD, FACC, FSCAI Disclosure Information
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,