Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery
|
|
|
- Gary Cameron
- 6 years ago
- Views:
Transcription

1 Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients with congenital heart lesions has allowed this patient population to survive into adulthood, even with the most complex congenital lesions. As a result, patients with patients with congenital heart lesions are increasingly encountered in the adult perioperative setting for laparoscopic, obstetric, plastic, spine, and other non-cardiac procedures. In the adult population, repaired or chronic non-palliated congenital heart lesions offer unique challenges. Therefore, adult anesthesiologists must be familiar with the anatomy, long-term manifestations, and unique perioperative management of adults with congenial heart disease. Shunting Lesions: Intracardiac shunts, or communications between atria (atrial septal defects, ASD), ventricles (ventricular septal defects (VSD), or great vessels (patent ductus arteriosus, e.g.) are the most common type of congenital heart lesions. These communications allow shunting of blood from areas of high to low pressure, typically left to right. While many are repaired surgically, these lesions may go unrecognized until adulthood. The common consideration for shunting lesions is structural changes in the pulmonary vasculature resulting in pulmonary hypertension with subsequent right ventricular failure. Chronic severe pulmonary hypertension in the context of shunting lesions may result in Eisenmenger syndrome with reversal of shunt (right to left) and Figure 1: Sinus venosus ASD, an example of a shunting lesion. Large defects as shown cause significant RV volume overload and pulmonary hypertension. SVASD is also associated with anomalous pulmonary venous return (not shown). hypoxemia. Preoperative evaluation should include a thorough history and physical, with particular attention to pulmonary hypertension and right ventricular failure. Right ventricular failure is heralded by elevated jugular venous pressure, hepatomegaly, hepatic dysfunction, or peripheral edema. 12-lead electrocardiogram is useful to detect atrial fibrillation or flutter, common with atrial enlargement in these patients. Patients with previous VSD repair may have heart block from patching proximal to the conduction system. These patients may have a permanent pacemaker, which requires interrogation and proper programming in the perioperative setting. Right heart catheterization useful for determining preoperative pulmonary artery pressures. The primary goals for the anesthesiologist caring for these patients include avoidance of intravascular air, decreasing pulmonary vascular resistance, and maintaining adequate right ventricular function. Adequate ventilation and oxygenation is paramount to the care of these patients. Hypercarbia secondary to excessive premedication with midazolam or narcotics can result in right ventricular failure and cardiovascular collapse in patients with severe pulmonary hypertension. Similar effects may be seen with induction-induced apnea. Avoidance of sympathetic-

2 Page 2 induced pulmonary vasoconstriction with adequate anesthesia, analgesia, and normothermia is recommended. Inhaled prostaglandins or nitric oxide are useful for reversible pulmonary hypertension. Right ventricular dysfunction in this setting may require inodilator drugs, such as milrinone or dobutamine. Figure 2: Treatment for pulmonary hypertension in the perioperative setting. Complex lesions of the great vessels: Lesions of the great vessels include transposition of the great arteries (TGA) and truncus arteriosus (TA). Critical for survival, these lesions require intracardiac shunting for mixing of blood and adequate oxygenation. Left unrepaired, these lesions typically result in severe pulmonary hypertension and are usually fatal. TGA is a discordance of the ventricles and great vessels, resulting in a parallel circulation. To simplify, oxygenated blood from the lungs takes the following route: pulmonary veins left atrium left ventricle pulmonary artery lungs. Deoxygenated blood enters right atrium right ventricle aorta. Early repairs, such as the Mustard or Sennig procedures, involved an intra-atrial baffle or tunnel that redirects blood to the anatomically correct side. In these patients, the right ventricle is remains the systemic ventricle. Considerations for these patients are right ventricular failure and atrial arrhythmias from the baffle suture lines. Repair of TGA since the mid-1980s is via the arterial switch procedure, where the pulmonary artery and aorta are surgically reversed. Unique considerations include stenosis at the anastamotic sites (PA or aorta) and pulmonary valve or aortic insufficiency.


3 Page 3 Similarly, repair of truncus arteriosus involves separation of the great vessels to their respective ventricles and VSD repair. Considerations are anastamotic strictures, aortic valve insufficiency, persistent VSD, and ventricular arrhythmias. Note that congenitally corrected TGA (left atrium right ventricle aorta; right atrium left ventricle pulmonary artery) does not require surgical correction. However, the anatomic right ventricle serves as the systemic ventricle, resulting in an increased incidence of heart failure over time. Cardiac MRI is a useful tool for delineating the anatomy and identification of conduit or vessel abnormalities. Tetralogy of Fallot: TOF is one of the most commonly encountered adult congenital heart lesions. TOF is defined by the presence of a VSD, overriding aorta, right ventricular outflow tract obstruction (or pulmonary valve stenosis), and right ventricular hypertrophy. Most patients encountered have received a definitive repair of this lesion, though there exists a rare population of unrepaired TOF. Unrepaired lesions, unlike our previous categories, obstruction to pulmonary flow is protective against pulmonary overload and pulmonary hypertension. However, right ventricular failure secondary to RVOT obstruction is common. Further, bidirectional or right to left shunting through the VSD may result in profound hypoxemia. This is treated by intravascular volume expansion, beta blockade, and phenylephrine. These maneuvers decrease RVOT obstruction and increase systemic vascular resistance, promoting left to right shunting. More commonly encountered is the patient with repaired TOF with a VSD patch and augmentation of the RVOT or pulmonic valve. A common surgical method to augment the RVOT is transannular patching. These repairs have resulted in severe pulmonary valve insufficiency, RV volume overload, and right ventricular failure. The combination of RV enlargement and RV scarring at the ventriculotomy site causes localized slowing of the conduction system and malignant ventricular arrhythmias. A QRS interval > 180 ms is predictive of re-entrant monomorphic ventricular tachycardia. It is not uncommon for patients with repaired TOF to have an implantable cardioverter defibrillator (ICD). In addition, the overriding aorta may result in aortic insufficiency over time. VSD patch leak is also a consideration. Intravascular air should always be avoided in congenital heart patients, even with repaired lesions. A. B. B Figure 3: Sequelae of TOF repair. A. TEE modified RV outflow tract view with dilated right ventricle, RVOT and pulmonic valve. B. Same TEE view with severe pulmonic insufficiency by color Doppler. C. Left ventricular outflow tract TEE view with dilated RV, VSD patch, and overriding aorta.


4 Page 4 C. Complex congenital cardiac lesions: Several types of complex congenital heart lesions exist where preservation of biventricular function is not feasible. These lesions include hypoplastic left heart syndrome, tricuspid atresia, unbalanced atrio-ventricular septal defects, double inlet left ventricle, double outlet right ventricle, and some forms Figure 4: A variety of complex congenital defects that often lead to Fontan palliation. HLHS: hypoplastic left heart syndrome, TA: tricuspid atresia, AVSD: atrioventricular septal defects, DILV: double inlet left ventricle, DORV: double outlet right ventricle of heterotaxy syndrome. While the initial anatomy of complex congenital heart lesions is rather variable, surgical treatment often results in the common endpoint, Fontan palliation. Regardless of the initial congenital lesion, there are two essential components of Fontan physiology: 1) the presence of a single systemic ventricle (SV), either an anatomic right or left ventricle, and 2) systemic venous return enters the pulmonary artery without ventricular assistance.
 and the inferior vena cava (IVC) to the pulmonary artery.")
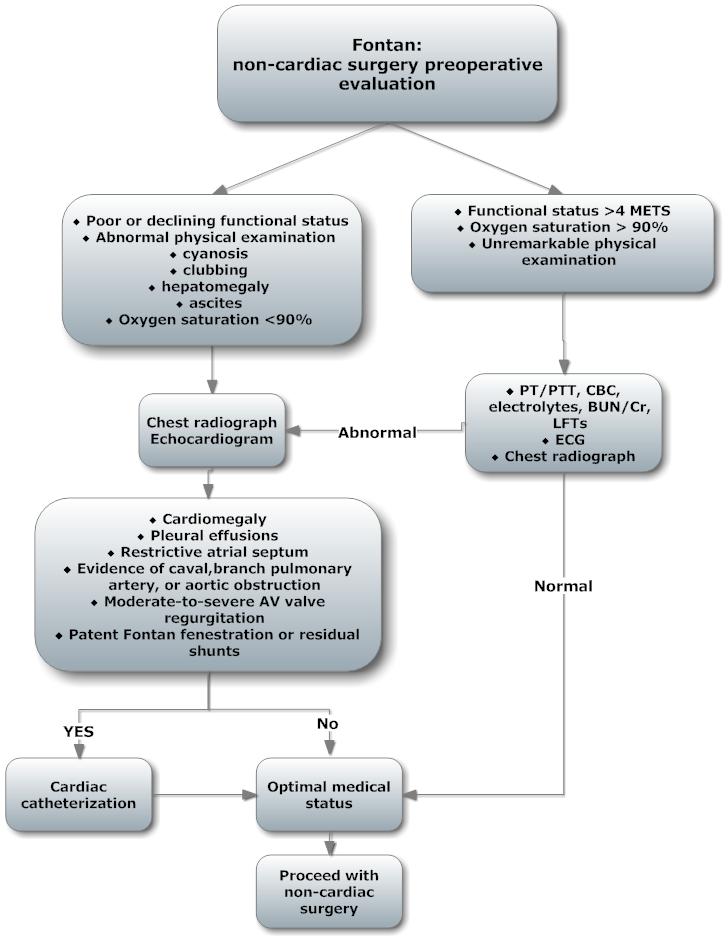
5 Page 5 The second point is the result of surgical reconstruction in a staged fashion. Over the past several decades, a total cavopulmonary connection (TCPC) is the method of choice. TCPC involves surgical anastamosis of the superior vena cava (SVC) and the inferior vena cava (IVC) to the pulmonary artery. Figure 5: Fontan schematic in patient with hypoplastic left heart syndrome: Salient features are total cavopulmonary return, atrial communication, and right ventricle as systemic ventricle. SVC: superior vena cava; IVC: inferior vena cava; PA: pulmonary artery; PV: pulmonary veins; LA: left atrium; RA: right atrium; ASD: atrial septal defect; RV: right ventricle; Ao: aorta Evaluation of the adult with Fontan physiology involves a thorough history and physical examination. Medical records, most recent catheterization, cardiac MRI, and laboratory data are invaluable to elucidate cardiac anatomy, oxygen saturation, pressure data, and SV function. Medical history should focus on current and changes in health status, exercise capacity, recent hospitalization, and current medications. Physical examination of a well-functioning Fontan patient should be relatively unremarkable. Fontan patients are expected to be normothermic and acyanotic; peripheral arterial pulses are palpable and precordial auscultation is devoid of murmurs. Normal oxygen saturation by pulse oximetry ranges from 90 to 95% in patients with a wellfunctioning Fontan, due to a small shunt via the coronary sinus. Chest radiography should reveal a normal cardiac silhouette; normal sinus rhythm on electrocardiography (ECG) is expected. Without the presence of a ventricle, pulmonary blood flow is dependent upon the maintenance of a transpulmonary gradient (TPG) a 5 to 8 mmhg gradient between the central venous system and the left atrium. Decreases in transpulmonary gradient occur with inadequate preload, depressed ventricular function, or increases in pulmonary or systemic vascular resistance. Decreased TPG results in decreased cardiac output, systemic hypotension, and poor tissue perfusion. Induction of anesthesia, hypoventilation / hypoxemia, postoperative pain, inadequate anesthesia / sympathetic stimulation, prolonged NPO status may all result in a decreased TPG. Standard intraoperative monitoring is adequate for patients with a well-functioning Fontan, particularly for procedures where minimal hemodynamic derangements or fluid shifts are expected. Upper extremity blood pressure measurements should be taken on the opposite side of a previous Blalock-Taussig (subclavian artery to pulmonary artery) shunt to avoid an artificially low blood pressure. Central venous access risks TCPC thrombosis, endocarditis, and vascular or intrathoracic injury. Achieving adequate cardiac output is the mainstay of anesthetic management of patients with Fontan physiology. Conservative administration of intravenous fluids prior to induction of anesthesia may be prudent to counteract NPO status and venodilation from anesthetic agents. While there is predilection of volatile anesthetics and positive pressure ventilation to cause hypotension in Fontan patients, general anesthesia must be adequate to prevent sympathetic stimulation leading to detrimental increases in pulmonary vascular resistance. Similarly, inadequate
6 Page 6 tidal volumes lead to atelectasis, hypoxemia, and hypercarbia. Since the majority of venous return with intermittent positive pressure ventilation occurs during expiration, inspiratory time should be shortened accordingly. Caution must be taken with monitored anesthesia care (MAC) since hypoventilation leads to increased PVR. Epidurals have been used successfully in the perioperative management of Fontan patients. Epidural dosing is progressively titrated to minimize sympatholytic effects, venodilation, and decreased pulmonary return. Endocarditis prophylaxis is recommended Fontan patients, due to increased endocarditis risk with palliative shunts and conduits. In spite of excellent survival rates, Fontan patients are at progressive risk for failing palliation. Preoperative findings indicative of a failing Fontan include fatigue, decreased activity level, weight gain or volume retention, palpitations, syncopal or pre-syncopal episodes, oxygen saturation below 90%, and dyspnea. Physical findings are often secondary to SV failure, atrial arrhythmias or sinus node dysfunction, AV valve dysfunction, infectious processes, protein-losing enteropathy and systemic-to-pulmonary artery collaterals. Abnormalities on chest radiography consistent with failing Fontan include cardiomegaly, pulmonary edema, and pleural effusions. Figure 6: Multi-organ dysfunction associated with failing Fontan palliation. The incidence of arrhythmias, particularly atrial tachyarrhythmias, increases with time. An arrhythmia somewhat unique to Fontan patients is intra-atrial reentrant tachycardia (IART. IART is a slow atrial flutter with 2:1 AV conduction. The diagnosis is often elusive as the second p wave is buried within the QRS complex or the T-wave. Protein-losing enteropathy (PLE) is an enigmatic problem with a significant mortality and no clear treatment modality. Pleural effusions, decreased, SpO2, peripheral edema, and ascites are consistent findings in patients with PLE. Decreased levels of albumin and total protein, and stool positive for alpha-1 antitrypsin confirm the diagnosis of PLE. Hepatic cirrhosis is a commonly associated with failing Fontan palliation. Coagulopathy and esophageal varices may be present in these patients. Thromboembolic events, including pulmonary embolism and cerebral vascular accidents, occur in up to 25% of patients, and are a source of significant morbidity and mortality for patients with Fontan physiology. Prior to elective cardioversion, intracardiac thrombi should be excluded by TEE.
7 Page 7 Plastic bronchitis, a late finding after Fontan palliation, consists of obstructive bronchial casts within the tracheobronchial tree. Once new-onset or worsening failed Fontan physiology is evident, elective surgery should be postponed for further investigation. Recently published guidelines for preoperative evaluation of adults with Fontan physiology are as follows:
8 Page 8
9 Disclosure This speaker has indicated that he or she has no significant financial relationship with the manufacturer of a commercial product or provider of a commercial service that may be discussed in this presentation.
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Anesthetic Considerations in Adults with Congenital Heart Disease
 CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Perioperative Management of DORV Case
 Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Adult Congenital Heart Disease Certification Examination Blueprint
 Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Pulmonic Ventricular Dysfunction Adult with Congenital Heart Disease
 Pulmonic Ventricular Dysfunction Adult with Congenital Heart Disease Louise Callow, RN, MSN, CPNP Pediatric Cardiac Surgery Nurse Practitioner University of Michigan, CS Mott Children s Hospital Ann Arbor,
Pulmonic Ventricular Dysfunction Adult with Congenital Heart Disease Louise Callow, RN, MSN, CPNP Pediatric Cardiac Surgery Nurse Practitioner University of Michigan, CS Mott Children s Hospital Ann Arbor,
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease II: The Repaired Adult
 Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Review Article An Adult Patient with Fontan Physiology: A TEE Perspective
 Anesthesiology Research and Practice Volume 2012, Article ID 475015, 5 pages doi:10.1155/2012/475015 Review Article An Adult Patient with Fontan Physiology: A TEE Perspective Edward Gologorsky, 1 Angela
Anesthesiology Research and Practice Volume 2012, Article ID 475015, 5 pages doi:10.1155/2012/475015 Review Article An Adult Patient with Fontan Physiology: A TEE Perspective Edward Gologorsky, 1 Angela
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS
 ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS V.S. Mahadevan, MD, F.R.C.P. Director, Structural and Adult congenital Interventional Cardiology Program William W
ADULT CONGENITAL HEART DISEASE AN UPDATE FOR CARDIOLOGISTS AND PRIMARY CARE PHYSICIANS V.S. Mahadevan, MD, F.R.C.P. Director, Structural and Adult congenital Interventional Cardiology Program William W
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Congenital Heart Disease An Approach for Simple and Complex Anomalies
 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1 ASCeXAM Contains
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
The Double Switch Using Bidirectional Glenn and Hemi-Mustard. Frank Hanley
 The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
CONGENITAL HEART LESIONS ((C.H.L
 CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
CONGENITAL HEART LESIONS ((C.H.L BY THE BOOKS: 0.8 IN FACT: 3-5% INCLUDING: - BICUSPID AORTIC VALVE MITRAL VALVE PROLAPSE LATE DIAGNOSIS - :INCREASED INCIDENCE IN ADULTS BETTER DIAGNOSIS IN INFANCY BETTER
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Adults With Congenital Heart. Disease. An Expanding Population. In this article:
 Adults With Congenital Heart Disease An Expanding Population Continued progress in diagnosing and managing infants and children with congenital heart disease will likely result in a better prognosis and
Adults With Congenital Heart Disease An Expanding Population Continued progress in diagnosing and managing infants and children with congenital heart disease will likely result in a better prognosis and
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Multimodality Imaging of Septal Defects
 Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
2018 Guideline for the Management of Adults with Congenital Heart Disease
 2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
2018 Guideline for the Management of Adults with Congenital Heart Disease A Selection of Tables and Figures ACC.org/GMSACHD 2018 Guideline for the Management of Adults with Congenital Heart Disease A report
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray
 Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Chapter 2 Cardiac Interpretation of Pediatric Chest X-Ray Ra-id Abdulla and Douglas M. Luxenberg Key Facts The cardiac silhouette occupies 50 55% of the chest width on an anterior posterior chest X-ray
Cardiovascular MRI of Adult Congenital Heart Disease
 Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Paediatric Cardiology. Acyanotic CHD. Prof F F Takawira
 Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Paediatric Cardiology Acyanotic CHD Prof F F Takawira Aetiology Chromosomal Down syndrome, T13, T18 Genetic syndromes (gene defects) Velo-Cardio-facial (22 del) Genetic syndromes (undefined aetiology)
Dear Parent/Guardian,
 Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Dear Parent/Guardian, You have indicated on school records that your child has an ongoing health problem that may require medication and/or treatment during the school day with rescue medication. Attached
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Surgical Management Of TAPVR. Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital
 Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Surgical Management Of TAPVR Daniel A. Velez, M.D. Congenital Cardiac Surgeon Phoenix Children s Hospital No Disclosures Goals Review the embryology and anatomy Review Surgical Strategies for repair Discuss
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Objectives Part 1. Objectives Part 2. Fetal Circulation Transition to Postnatal Circulation Normal Cardiac Anatomy Ductal Dependence and use of PGE1
 Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Cardiac Physiology Gia Marzano, AC PNP Pediatric Cardiac Surgery Rush Center for Congenital Heart Disease Rush University Medical Center Objectives Part 1 Fetal Circulation Transition to Postnatal Circulation
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
Pituitary adenomas represent 10 15% of intracranial neoplasms.
 PART ONE Disease 2 ADRENAL & PITUITARY DISEASE overview GIUDITTA ANGELINI, MD Pituitary adenomas represent 10 15% of intracranial neoplasms. Prevalence is 200/1,000,000; post-mortem incidence is 10 27%.
PART ONE Disease 2 ADRENAL & PITUITARY DISEASE overview GIUDITTA ANGELINI, MD Pituitary adenomas represent 10 15% of intracranial neoplasms. Prevalence is 200/1,000,000; post-mortem incidence is 10 27%.
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Fontan Deterioration in Pediatric Cardiologist s s View. Pusan National University Hospital Hyoung Doo Lee M.D.
 Fontan Deterioration in Pediatric Cardiologist s s View Pusan National University Hospital Hyoung Doo Lee M.D. Outcomes of Fontan operation JTCS 2006:131;172-80 Mitchell ME et al Jan. 1992~Dec. 1999, 332
Fontan Deterioration in Pediatric Cardiologist s s View Pusan National University Hospital Hyoung Doo Lee M.D. Outcomes of Fontan operation JTCS 2006:131;172-80 Mitchell ME et al Jan. 1992~Dec. 1999, 332
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Adult congenital heart disease Complex plumbing made simple
 Adult congenital heart disease Complex plumbing made simple James Oliver Leeds Bayer Disclosures Q 1. With respect to atrial septal defects: 1. Severe right heart volume loading is generally a contraindication
Adult congenital heart disease Complex plumbing made simple James Oliver Leeds Bayer Disclosures Q 1. With respect to atrial septal defects: 1. Severe right heart volume loading is generally a contraindication
Admixture lesions in congenital cyanotic heart disease
 HEMODYNAMIC ROUNDS Admixture lesions in congenital cyanotic heart disease Jaganmohan A Tharakan Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum,
HEMODYNAMIC ROUNDS Admixture lesions in congenital cyanotic heart disease Jaganmohan A Tharakan Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum,
Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia
 Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
Surgical Procedures. Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder
 PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
ASCeXAM / ReASCE. Practice Board Exam Questions. Tuesday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
Research Presentation June 23, Nimish Muni Resident Internal Medicine
 Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service
 Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service Objective 1 Hyperlipidemia does NOT cause congenital heart
Ascot Cardiology Symposium 2014 Adult Congenital Heart Disease What should GP s know? Boris Lowe, MB ChB, FRACP Green Lane Cardiovascular Service Objective 1 Hyperlipidemia does NOT cause congenital heart
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Adult with Cyanotic Congenital Heat Disease
 Adult with Cyanotic Congenital Heat Disease Savitri Srivastava Director, Pediatric & Congenital Heart Disease Fortis Escorts Heart Institute Okhla Road, New Delhi Cyanotic Adult WCC & IVUS 2015 Adult Cyanotic
Adult with Cyanotic Congenital Heat Disease Savitri Srivastava Director, Pediatric & Congenital Heart Disease Fortis Escorts Heart Institute Okhla Road, New Delhi Cyanotic Adult WCC & IVUS 2015 Adult Cyanotic
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of