2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
|
|
|
- Gavin Fitzgerald
- 6 years ago
- Views:
Transcription
1 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Presented by Robert H. Eckel, M.D. Professor of Medicine Division of Endocrinology, Metabolism & Diabetes Divsion of Cardiology Professor of Physiology and Biophysics Charles A. Boettcher II Chair in Atherosclerosis Director, Lipid Clinic University of Colorado Hospital University of Colorado Anschutz Medical Campus Aurora, Colorado
2
3 Scope of the CVD Problem ( )
4 Learning Objectives 1. To update you on the ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. 2. To discuss the controversial issues related to interpretation of the Guideline and how it influences the practice of preventive cardiology.
5 ACC/AHA Blood Cholesterol Guideline Panel Members Neil J. Stone, MD, MACP, FAHA, FACC, Chair Jennifer G. Robinson, MD, MPH, FAHA, Vice Chair Alice H. Lichtenstein, DSc, FAHA, Vice Chair Anne C. Goldberg, MD, FACP, FAHA Conrad B. Blum, MD, FAHA Robert H. Eckel, MD, FAHA, FACC Daniel Levy, MD* David Gordon, MD* C. Noel Bairey Merz, MD, FAHA, FACC Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA J. Sanford Schwartz, MD Patrick McBride, MD, MPH, FAHA Sidney C. Smith, Jr, MD, FACC, FAHA Karol Watson, MD, PhD, FACC, FAHA Susan T. Shero, MS, RN* Peter W.F. Wilson, MD, FAHA *Ex-Officio Members. Acknowledgements Methodology Members Karen M. Eddleman, BS Nicole M. Jarrett Ken LaBresh, MD Lev Nevo, MD Janusz Wnek, PhD National Heart, Lung, and Blood Institute Glen Bennett, M.P.H. Denise Simons-Morton, MD, PhD
6 Conflict of Interest/Relationships With Industry 1) All panel members disclosed conflict of interest information to the full panel in advance of the deliberations 2) Members with conflicts recused themselves from voting on any aspect of the guideline where a conflict might exist 3) All 16 members of the NHLBI ATP IV Panel transitioned to the ACC/AHA guideline Expert Panel 4) Independent contractors performed the systematic review with the assistance of the Expert Panel and provided methodological guidance to the Expert Panel
7 Conflict of Interest/Relationships With Industry Advisory Boards or Consultant Abbott Foodminds Merck Pfizer
8 NHLBI Charge to the Expert Panel Evaluate higher quality randomized controlled trial (RCT) evidence for cholesterol-lowering drug therapy to reduce ASCVD risk Use Critical Questions (CQs) to create the evidence search from which the guideline was developed Cholesterol Panel: 3 CQs Risk Assessment Work Group: 2 CQs Lifestyle Management Work Group: 3 CQs RCTs and systematic reviews/meta-analyses of RCTs independently assessed as fair-to-good quality Develop recommendations based on RCT evidence Less expert opinion than in prior guidelines
9 Systematic Review Process The Expert Panel constructed CQs relevant to clinical practice. The Expert Panel identified (a priori) inclusion/exclusion (I/E) criteria for each CQ. An independent contractor developed a literature search strategy, based on I/E criteria, for published clinical trial reports for each CQ. An independent contractor executed a systematic electronic search of the published literature from relevant bibliographic databases for each CQ. The date for the overall literature search was from January 1, 1995 through December 1, However, RCTs with the ASCVD outcomes of MI, stroke, and cardiovascular death published after that date were eligible for consideration until July 2013.

10 Classification of Recommendations and Levels of Evidence Size of Effect Certainty A recommendation with Level of Evidence B or C does not imply that the recommendation is weak. Many important clinical questions addressed in the guidelines do not lend themselves to clinical trials. Although randomized trials are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective. *Data available from clinical trials or registries about the usefulness/ efficacy in different subpopulations, such as sex, age, history of diabetes, history of prior myocardial infarction, history of heart failure, and prior aspirin use. For comparative effectiveness recommendations (Class I and IIa; Level of Evidence A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
11 Guideline Scope Focus on treatment of blood cholesterol to reduce ASCVD risk in adults Emphasize adherence to a heart healthy lifestyle as foundation of ASCVD risk reduction See Lifestyle Management Guideline Identify individuals most likely to benefit from cholesterol-lowering therapy 4 statin benefit groups Identify safety issues
12 4 Statin Benefit Groups Clinical ASCVD* LDL C >190 mg/dl, Age >21 years Primary prevention Diabetes: Age years, LDL C mg/dl Primary prevention - No Diabetes : 7.5%10-year ASCVD risk, Age years, LDL C mg/dl *Atherosclerotic cardiovascular disease Requires risk discussion between clinician and patient before statin initiation. Statin therapy may be considered if risk decision is uncertain after use of ASCVD risk calculator.
13 Reduction in Major Vascular Events by Statins is Independent of Baseline LDL-C CTT 2010: Meta-analysis of 26 RCTs (170,000 Participants) LDL-C Cholesterol Treatment Trialists (CTT) Collaboration. Lancet 2010; 376:
14 Cholesterol Treatment Trialist s 2010 Meta-analysis (26 Trials, 170,000 Participants) Cholesterol Treatment Trialists. Lancet 2010; 376:
15 Vignettes: Putting a face on patients in whom ASCVD risk reduction works 63 yo man with STEMI, discharged on a highintensity statin 26 yo woman with an LDL C of 220 mg/dl, noted in teens + family history CHD 44 yo woman with diabetes, well-controlled hypertension and micro-albuminuria 56 yo African-American woman with multiple ASCVD risk factors
16 Case 1 A 48 year old white woman with diabetes and microalbuminuria has a lipid panel: TC 197; TG 300; HDL-C 42; LDL-C 95 Her BMI is 34; weight up 4 lbs. Systolic BP 134. A1c 8.4%. Non-smoker In addition to adherence to an optimal lifestyle what is the next step to reduce her risk for heart attack and stroke?
17 Case 1 A. Moderate intensity statin; no follow up lipids needed. B. No need to use the risk estimator; she has diabetes. C. Moderate intensity statin, regular lipid follow ups to determine adherence and response to therapy. D. US guidelines don t allow a non-statin to be added. E. Time spent on adherence not useful; missing 25% of doses per month not likely to affect potential for benefit.
18 Case 1 Answer is C. She s in a statin benefit group. Why not an LDL-C or non HDL-C? The evidence points to proper intensity of therapy Why not high intensity statin therapy? The 10 year risk is 3.1%. Had she been a smoker, her risk would be 9.3%. Then tobacco cessation + intensive statin therpy if tolerated would be appropriate Non-statins can be used in any of the high risk groups if statin therapy gives a less than anticipated response.
19 Case 2 79 yo man had AMI & received a stent to his LAD. Home on atorvastatin 40 mg daily & usual 2 o prevention Rx TC 150; TG 150; HDL-C 45; LDL-C 75; Non HDL-C 105 Which of these is a true statement? A. Getting under 70 mg/dl will provide an outcomes difference for him B. Statin dose should be atorvastatin 80 mg or rosuvastatin 40 mg/d C. Guidelines recommend lipids monitored periodically to assess adherence to statin/lifestyle; also for safety issues D. No need to have lipids checked. It's a set it and go on strategy
20 Case 2 Answer is C. Since he is over 75, use of 40 mg atorvastatin would be reasonable, even though there are data to support high dose statin after age 75. The issue of competing co-morbidities, multiple medications, and greater potential for side-effects with a high-intensity statin affect the decision here. What is crucial is to monitor lipids periodically and discuss safety issues. After checking lipids 4-12 weeks after the statin is started, they should be checked at 3-12 months regularly with the interval dependent on how likely the patient is to have problems with adherence or safety issues.
21 What s Similar to ATP-III? Emphasis on lifestyle measures as crucial Focus on treatment of LDL-C Greatest intensity of treatment for patients at highest risk Preference for statins over other medications that lower LDL-C Although this is more emphasized in the new ACC/AHA Guideline
22 New Perspective on LDL C & Non-HDL C Goals Lack of RCT evidence to support titration of drug therapy to specific LDL C and/or non-hdl C goals Strong evidence that appropriate intensity of statin therapy should be used to reduce ASCVD risk in those most likely to benefit Quantitative comparison of statin benefits with statin risk Nonstatin therapies did not provide ASCVD risk reduction benefits or safety profiles comparable to statin therapy LDL-C <40 mg/dl is too low - reduce statin dose
23 Why Not Continue to Treat to Target? Major difficulties: 1. Current RCT data do not indicate what the target should be 2. Unknown magnitude of additional ASCVD risk reduction with one target compared to another 3. Unknown rate of additional adverse effects from multidrug therapy used to achieve a specific goal 4. Therefore, unknown net benefit from treat-totarget approach
24 Important to Note No Evidence could be There is no evidence, or The existing evidence is inconclusive We treat people not populations. Goal-setting is not precluded; It s just not evidence-based.

25 4 Statin Benefit Groups IA IA IB IA *Percent reduction in LDL C can be used as an indication of response and adherence to therapy, but is not in itself a treatment goal. 1 IIaB
26 Circulation,JACC 2013 Nov 12







27 Maintain an Overall Healthy Diet!
28
29 Nutrition Lifestyle Recommendations Dietary patterns emphasis-based: DASH and Mediterranean eating plans Fruits, vegetables, and whole grains 30 35% fat intake of monounsaturated fats (low saturated fats, no trans fats) Low sodium (<2400 mg/day) Cut out processed or pre-prepared food Healthy eating for a lifetime
30 Dietary Pattern Recommendations for LDL-C Lowering Advise adults who would benefit from LDL-C lowering to: Choose a heart-healthy dietary pattern. Reduce % of calories from saturated fat. 5% to 6% of calories. Reduce % of calories from trans fat. Strength of evidence: IA Eckel RH et al, Circulation; JACC, In Press, 2014
31 Physical Activity Recommendations Goal is minutes / day, 150 minutes per week Minimum 3 days per week F I T (frequency / intensity / time) Variety including strength, flexibility, and endurance Prescription Just Do It!
32 Physical Activity Guidelines: Lipids and BP Advise adults to engage in aerobic physical activity 3 to 4 sessions a week lasting on average 40 min per session involving moderate-to-vigorous intensity physical activity. Strength of evidence IIA Eckel RH et al, Circulation; JACC, In Press, 2014
.")
33 4 Statin Benefit Groups (con t) IA Before writing the prescription for statin therapy, clinicians and patients should engage in a discussion that focuses on issues related to ASCVD risk reduction and statin appropriateness, which include safety and patient preferences (see Figure 4). For those in whom a risk assessment is uncertain, factors such as family history of premature ASCVD, lifetime risk of ASCVD, LDL C 160 mg/dl, hs-crp 2.0, CAC score 300 Agatston units, and ABI 0.90 may be considered to inform the treatment decision. IA The Pooled Cohort Equations can be used to estimate 10-year ASCVD risk in individuals with and without diabetes. A downloadable spreadsheet enabling estimation of 10-year and lifetime risk for ASCVD and a web-based calculator are available at and The calculator was designed to inform decision making in primary prevention patients not on a statin. Primary LDL C 160 mg/dl or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, highsensitivity C-reactive protein >2 mg/l, CAC score 300 Agatston units or 75 percentile for age, sex, and ethnicity, ankle-brachial index <0.9, or elevated lifetime risk of ASCVD.
34 Intensity of Statin Therapy *Individual responses to statin therapy varied in the RCTs and should be expected to vary in clinical practice. There might be a biologic basis for a less-than-average response. Evidence from 1 RCT only: down-titration if unable to tolerate atorvastatin 80 mg in IDEAL (Pedersen et al). Although simvastatin 80 mg was evaluated in RCTs, initiation of simvastatin 80 mg or titration to 80 mg is not recommended by the FDA due to the increased risk of myopathy, including rhabdomyolysis.
35 Clinical ASCVD Initiating Statin therapy *Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-hdl C >220 mg/dl may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dl, a fasting lipid panel is required. It is reasonable to evaluate the potential for ASCVD benefits and for adverse effects, and to consider patient preferences, in initiating or continuing a moderate- or high-intensity statin, in individuals with ASCVD >75 years of age.
36 Primary Prevention Initiating Statin Therapy *Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-hdl C >220 mg/dl may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dl, a fasting lipid panel is required.

37 Primary Prevention Initiating Statin Therapy (con t) The Pooled Cohort Equations can be used to estimate 10-year ASCVD risk in individuals with and without diabetes. A downloadable spreadsheet enabling estimation of 10-year and lifetime risk for ASCVD and a web-based calculator are available at ator and These factors may include primary LDL C >160 mg/dl or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, sensitivity-creactive protein >2 mg/l 300 Agatston units or 75 percentile for age, sex, and ethnicity (For additional information, see ABI <0.9, or lifetime risk of ASCVD. Additional factors that may aid in individual risk assessment may be identified in the future. 1) Potential ASCVD risk reduction benefits (e.g., absolute risk reduction from moderate- or high-intensity statin therapy can be approximated by using the estimated 10-year ASCVD risk and the relative risk reduction of ~30% for moderate-intensity statin or ~45% for high-intensity statin therapy. 2) Potential adverse effects. The excess risk of diabetes is the main consideration in ~0.1 excess case per 100 individuals treated with a moderate-intensity statin for 1 year and ~0.3 excess cases per 100 individuals treated with a high-intensity statin treated patients for 1 year. Note: a case of diabetes is not considered equivalent to a fatal or nonfatal MI or stroke. Both statin-treated and placebo-treated participants experienced the same rate of muscle symptoms. The actual rate of statin-related muscle symptoms in the clinical population is unclear. Muscle symptoms attributed to statin should be evaluated in Table 8, Safety Rec 8.
38 Primary Prevention Global Risk Assessment To estimate 10-year ASCVD* risk New Pooled Cohort Risk Equations White and black men and women More accurately identifies higher risk individuals for statin therapy Focuses statin therapy on those most likely to benefit You may wish to avoid initiating statin therapy in highrisk groups found not to benefit (higher grades of heart failure and hemodialysis) *10-year ASVD: Risk of first nonfatal myocardial infarction, coronary heart disease death, nonfatal or fatal stroke
39 Primary Prevention Statin Therapy Thresholds for initiating statin therapy derived from 3 exclusively primary prevention RCTs Before initiating statin therapy, clinicians and patients engage in a discussion of the potential for ASCVD risk reduction benefits, potential for adverse effects, drug-drug interactions, and patient preferences
40 Individuals Not in a Statin Benefit Group In those not clearly in 1 of 4 statin benefit groups, additional factors may inform treatment decisionmaking: Family history of premature ASCVD Elevated lifetime risk of ASCVD LDL C 160 mg/dl hs-crp 2.0 mg/l Subclinical atherosclerosis CAC score 300 or ABI<0.9 Discussion of potential for ASCVD risk reduction benefit, potential for adverse effects, drug-drug interactions, and patient preferences
41 Safety RCTs & meta-analyses of RCTs used to identify important safety considerations Allow estimation of net benefit from statin therapy o ASCVD risk reduction versus adverse effects Expert guidance on management of statin-associated adverse effects, including muscle symptoms Advise use of additional information including pharmacists, manufacturers prescribing information, & drug information centers for complex cases
42
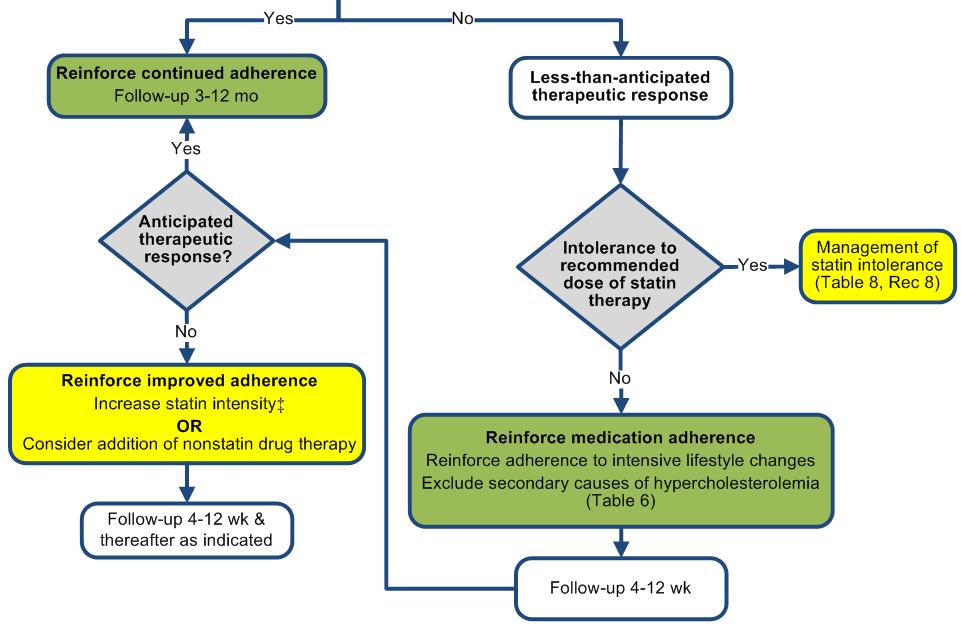
43 Statin Therapy: Monitoring Response and Adherence
44
45 Management of Muscle Symptoms on Statin Therapy It is reasonable to evaluate and treat muscle symptoms including pain, cramping, weakness, or fatigue in statin-treated patients according to the management algorithm To avoid unnecessary discontinuation of statins, obtain a history of prior or current muscle symptoms to establish a baseline before initiating statin therapy
46 Management of Muscle Symptoms on Statin Therapy (con t) If unexplained severe muscle symptoms or fatigue develop during statin therapy: Promptly discontinue the statin Address possibility of rhabdomyolysis with: CK Creatinine Urine for myoglobinuria
47 Management of Muscle Symptoms on Statin Therapy (con t) If mild-to-moderate muscle symptoms develop during statin therapy: Discontinue the statin until the symptoms are evaluated Evaluate the patient for other conditions* that might increase the risk for muscle symptoms If after 2 months without statin Rx, muscle symptoms or elevated CK levels do not resolve completely, consider other causes of muscle symptoms *Hypothyroidism, reduced renal or hepatic function, rheumatologic disorders such as polymyalgia rheumatica, steroid myopathy, vitamin D deficiency or primary muscle diseases
48 Patient Types Diagnostic Strategies Therapeutic Options Asymptomatic Mildly Symptomatic Moderate to Severely Symptomatic CK in high risk patients only CK measured: < 5 x normal Stop Statin: CK measured, hydrate if creatinine Symptoms worse: repeat CK & Stop or Reduce Statin Dose Symptoms gone: CK & creat Red yeast rice, bid Eckel RH, JCEM 95:2015, 2010 Titrate Statin Dose to reach LDL and non- HDL-C goals Ezetimibe and/or BAS Fluvastatin or pravastatin, 20 mg per night or every other night Fluvastatin XL 80 mg per night Rosuvastatin 5 mg daily, every other day, or weekly
49 Statin Benefits Compared to Adverse Effects 2013 Cochrane Review *(18 RCTs, 19 trial arms n=56,394) 14 trials recruited patients with specific conditions (raised lipids, DM, HTN, microalb) 14% mortality 27% CHD (fatal and non fatal) events 22% in stroke (fatal and non fatal) 33% in nonfatal MI 38% in revascularization 18% in diabetes (2.8% on statin vs. 2.4% controls) No significant increase in short-term risk of - Muscle adverse events - Liver adverse events - Cancer, memory loss - Hemorrhagic stroke Taylor F, Huffman M et al Cochrane 2013.
50 Future Updates to the Blood Cholesterol Guideline This is a comprehensive guideline for the evidencebased treatment of blood cholesterol to reduce ASCVD risk These guidelines represent a change from previous guidelines For primary prevention, they are patient-centered Guidelines will change in the future as high-quality data will improve future cholesterol treatment guidelines
51 Major Controversies Risk calculator validation Threshold of 7.5% 10-year CVD event risk for statins in primary prevention Bias within committee and comparisons to other guidelines dismissed No LDL-C or non-hdl-c goals
52 Major Controversies Risk calculator validation
53 Risk Calculator: The Controversy? Risk Calculator from NHANES Very diverse U.S. population 12 years of follow-up When low risk populations are studied using this it can overestimate It is to be used as a guide, not a substitute for clinical decision making
54 Risk Assessment (i.e. risk calculation) has proven in RCTs to effectively identify those who benefit most from treatment
55 Includes: Risk Calculator Race Gender Age Total cholesterol HDL Blood pressure / Use of BP medicines Diabetes status Smoking status Guidelines_UCM_457698_SubHomePage.jsp

56 ACC/AHA Risk Calculator

57 Emphasis on Healthy Lifestyle For those risk estimator provides lifetime risk estimate Better in women? This is intended to drive discussions of greater adherence to heart-healthy lifestyle Part of risk discussion
58 2013 ACC/AHA GUIDELINE: Is the Risk Estimator Useful? Claim: Pooled Cohort Equations overestimate ASCVD risk by % Claim based on analyses of Women s Health Study, Physician s Health Study, Women s Health Initiative Observational Study, but: *Ridker PM and Cook NR. Lancet 382: , These studies lacked active surveillance for ASCVD events (can lead to ~30% undercounting of events**) **Hlatky MA et al. Circulation: Cardiovsc Qual Outcomes.7:157, High prevalence of statin use in contemporary cohorts may cause participants to underperform in ASCVD event generation Risk factor levels were self-reported in these studies The participants in these studies (esp. PHS) were not broadly representative of the US population
59 Primary Prevention Statin Therapy Thresholds for initiating statin therapy derived from 3 exclusively primary prevention RCTs Placebo group 10 yr event rates: JUPITER 7.6%; MEGA 5.1%; AFCAPS-TEXCAPS 6.9% Guideline Panel s recommendation: As a matter of caution, to avoid over-treating, the Panel identified those with risk 7.5% as a group in which statins provide benefit.

60 Muntner P et al, JAMA 311:1406, 2014 Reasons for Geographic and Racial Difference in Stroke
61 Observed and Predicted ASCVD Events in REGARDS Subjects n=10,997 Muntner P et al, JAMA 311:1406, 2014
62
63 Percent of US Adults Who Would be Statin Eligible for Primary Prevention Pencina MJ et al, NEJM 370:1422, 2014
64 Risk Assessment Recommended every 5 years For year olds Gives 10 year and lifetime risk Includes heart attack, all heart disease, and stroke risk Can be integrated into an electronic medical record
65 Major Controversies Risk calculator validation Threshold of 7.5% 10-year CVD event risk for statins in primary prevention
66 Moderate Intensity Statin Treatment Assumes a 35% relative risk reduction in ASCVD from moderate intensity statin therapy. NNT to prevent 1 ASCVD event varies by baseline estimated 10-year ASCVD risk. NNH based on 1 excess case of incident diabetes per 100 individuals; for myopathy or rhabdomyolysis; 0.01 for hemorrhagic stroke.
67 120 Moderate Intensity Statin Treatment NNT to prevent 1 ASCVD event over 10 years % 5.0% 7.5% 10.0% Stone NJ et al. Circ. Nov12, Sattar N et al. Lancet. 2010;375:735; Ridker P et al NEJM. 2008;359:2195 ; Cholesterol Treatment Trialists Collaborators. Lancet. 2012, 9841:581. NNT= % 20.0% 25.0% 0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 10 year ASCVD risk
68 Adjudication for the 7.5% 10-Year Risk The benefit of statins actually extended down to a global risk of 5%; thus, this more than adjusts for any overestimation when 7.5% is used. A number of other factors were identified that could be used when there is concern of overtreatment in borderline and/or elderly patients: CAC score, ABI, hscrp, family history of premature ASCVD, elevated lifetime risk and/or LDL-C 160 A risk discussion was repeatedly emphasized. The intersection between not just the evidence, but also clinical judgment based on individual patient factors and informed patient choice.
69 Major Controversies Risk calculator validation Threshold of 7.5% 10-year CVD event risk for statins in primary prevention Bias within committee and comparisons to other guidelines dismissed
70 Bias and Comparisons Response Free-standing and unique committee Different societies working separately COIs upfront Recusals when voting All but one potent statin generic Independent process Other guidelines not considered
71 Major Controversies Risk calculator validation Threshold of 7.5% 10-year CVD event risk for statins in primary prevention Bias within committee and comparisons to other guidelines dismissed No LDL-C or non-hdl-c goals
72 No LDL-C or non-hdl-c goals Not evidence-based Not precluded Performance measures Secondary prevention Optimal lifestyle and maximum tolerated statin prescribed Follow-up lipids - adherence and responsiveness Primary prevention Risk estimation Heart-healthy lifestyle Risk/benefit of statins discussion Informed patient preference
73 Emerging from these documents and others is a sense that guidelines should inform but not dictate, guide but not enforce, and support but not restrict Harlan Krumholz, MD, SM Yale University School of Medicine JAMA March 29, 2014


74 Thank you!
75 Thank You!
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL
 THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
THE 2013 ACC/AHA GUIDELINES ON THE TREATMENT OF BLOOD CHOLESTEROL Anne Carol Goldberg, MD, FACP, FAHA, FNLA Associate Professor of Medicine Washington University School of Medicine National Lipid Association
Understanding US Lipid Guidelines-2013:
 Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Presentation to NLA Symposium: May 3 2014 Understanding US Lipid Guidelines-2013: Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago, Il
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
ACC-AHA Prevention Guidelines: Evidence Continues to Lead the Way
 IAS- Amsterdam -2015 ACC-AHA Prevention Guidelines: Evidence Continues to Lead the Way Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago,
IAS- Amsterdam -2015 ACC-AHA Prevention Guidelines: Evidence Continues to Lead the Way Neil J. Stone MD, MACP, FACC Bonow Professor of Medicine Feinberg School of Medicine Northwestern University Chicago,
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
2.3 CONTACT HOURS. Managing. By Kristine Anne Scordo, PhD, RN, ACNP-BC, FAANP
 2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
2.3 CONTACT HOURS 2.3 CONTACT HOURS Managing hyperlipidemia The updated cholesterol treatment guidelines Abstract: The ACC/AHA 2013 cholesterol treatment guidelines focus on lowering the risk of heart
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2014 Update in Medicine Update in Cholesterol Management. Donald L. Lappé MD, FACC, FAHA October 31, 2014
 2014 Update in Medicine Update in Cholesterol Management Donald L. Lappé MD, FACC, FAHA October 31, 2014 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
2014 Update in Medicine Update in Cholesterol Management Donald L. Lappé MD, FACC, FAHA October 31, 2014 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Controversies in Preventative Cardiology
 Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
Controversies in Preventative Cardiology Francisco Lopez-Jimenez, M.D., M.Sc, FACC, FAHA Professor of Medicine, Mayo Medical School Chair, Division of Preventive Cardiology Co-Director, Artificial Intelligence
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Ten Year Risk for CVD Event by Systolic HTN and CVD Risk Factors (Where s Age?)
") Prevention and Treatment of CVD in Older Patients with Diabetes and Pre Diabetes: Hypertension and Dyslipidemia ASP Workshop on Diabetes Mellitus and Cardiovascular Disease in Older Adults Pentagon City
Prevention and Treatment of CVD in Older Patients with Diabetes and Pre Diabetes: Hypertension and Dyslipidemia ASP Workshop on Diabetes Mellitus and Cardiovascular Disease in Older Adults Pentagon City
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Treatment of Cholesterol in 2018: Time to Level Up. Most Important Slide. Three Things Learned that Will be Applied
 Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
It is the policy of health plans affiliated with PA Health & Wellness that Vytorin is medically necessary when the following criteria are met:
 Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
2013 Lipid Guidelines Practical Approach. Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS
 2013 Lipid Guidelines Practical Approach Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS EVIDENCE BASED MEDICINE Case #1 - LB 42 yo Asian/American female who was
2013 Lipid Guidelines Practical Approach Edward Goldenberg, MD FACC,FACP, FNLA Medical Director of Cardiovascular Prevention CCHS EVIDENCE BASED MEDICINE Case #1 - LB 42 yo Asian/American female who was
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
ManageMent Review. Boback Ziaeian, MD, 1,2 John Dinkler, MD, MPH, 1,2 Karol Watson, MD, PhD 1,3 1
 ManageMent Review Implementation of the 2013 American College of Cardiology/American Heart Association Blood Cholesterol Guideline Including Data From the Improved Reduction of Outcomes: Vytorin Efficacy
ManageMent Review Implementation of the 2013 American College of Cardiology/American Heart Association Blood Cholesterol Guideline Including Data From the Improved Reduction of Outcomes: Vytorin Efficacy
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Learning Objectives
 Learning Objectives Utilize evidence-based lipoprotein management strategies for non-ldl-c lipid targets Describe the risk factors, disease spectrum, and appropriate management of familial hypercholesterolemia
Learning Objectives Utilize evidence-based lipoprotein management strategies for non-ldl-c lipid targets Describe the risk factors, disease spectrum, and appropriate management of familial hypercholesterolemia
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus
 Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
ACC/AHA Prevention Guideline
 ACC/AA Prevention Guideline Downloaded from http://circ.ahajournals.org/ by guest on March 30, 2017 2013 ACC/AA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
ACC/AA Prevention Guideline Downloaded from http://circ.ahajournals.org/ by guest on March 30, 2017 2013 ACC/AA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
9/3/ AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis. Disclosure
 2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk
 Accepted Manuscript 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk David C. Goff, J r, MD, PhD, FACP, FAHA Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Glen Bennett, MPH Christopher J. O
Accepted Manuscript 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk David C. Goff, J r, MD, PhD, FACP, FAHA Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Glen Bennett, MPH Christopher J. O
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient?
 Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Implementation of CV Risk and. Dyslipidemia Guidelines. Impact on Americans 11/25/2014. Summary Implementing new. Dyslipidemia Guidelines
 Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
The Clinical Debates
 The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES
 DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists:
DYSLIPIDEMIA TREATMENT: HYBRIDIZING CLINICAL PRACTICE GUIDELINES SATURDAY/4:30-5:30PM ACPE UAN: 0107-9999-17-249-L01-P 0.1 CEU/1.0 hr Activity Type: Knowledge-Based Learning Objectives for Pharmacists: