K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease
|
|
|
- Timothy Mason
- 6 years ago
- Views:
Transcription
1 K/DOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease GUIDELINE 1: GOALS OF ANTIHYPERTENSIVE THERAPY IN CKD Hypertension is common in CKD, and is a risk factor for faster progression of kidney disease and development and worsening of CVD. Some antihypertensive agents also slow the progression of kidney disease by mechanisms in addition to their antihypertensive effect. 1.1 Antihypertensive therapy should be used in CKD to: 1.1.a Lower blood pressure (A); 1.1.b Reduce the risk of CVD, in patients with or without hypertension (B) (see Guideline 7); 1.1.c Slow progression of kidney disease, in patients with or without hypertension (A) (see Guidelines 8, 9,10). 1.2 Modifications to antihypertensive therapy should be considered based on the level of proteinuria during treatment (C) (see Guidelines 8, 9, 10,11). 1.3 Antihypertensive therapy should be coordinated with other therapies for CKD as part of a multi-intervention strategy (A). 1.4 If there is a discrepancy between the treatment recommended to slow progression of CKD and to reduce the risk of CVD, individual decision-making should be based on risk stratification (C). INTRODUCTION CKD is a world-wide public health problem, with increasing incidence and prevalence, high cost, and poor outcomes. The major outcomes of CKD are loss of kidney function and development of CVD. Increasing evidence indicates that the adverse outcomes of CKD can often be prevented or delayed through early detection and treatment. Hypertension is both a cause and a complication of CKD; more than 50% to 75% of patients with CKD have blood pressure >140/90 mm Hg. In addition, hypertension is a risk factor for progression of kidney disease and for CVD. The goals of antihypertensive therapy in CKD are to lower blood pressure, reduce the risk of CVD, and slow progression of CKD. BACKGROUND The Joint National Committee (JNC) for Prevention, Detection, Evaluation and Treatment of High Blood Pressure issues regular reports that are meant to provide guidance for primary-care
2 clinicians. The seventh report (JNC 7), issued in 2003, suggests stratification of risk for CVD in individuals with high blood pressure to determine the intensity of treatment. Individuals at highest risk should receive most intensive treatment, including prompt pharmacological therapy, a lower blood pressure goal, and use of specific antihypertensive agents for "compelling indications," including CKD. 5,5a Hypertension is common in CKD, affecting 50% to 75% of individuals. The Work Group for this K/DOQI Guideline on Hypertension and Antihypertensive Agents in CKD proposes recommendations for all patients with CKD, whether or not they have hypertension. Guideline 1 reviews the goals of antihypertensive therapy; multi-intervention strategies for CKD; and possible discrepancies between goals of slowing progression of CKD and reducing CVD risk. It concludes with a review of key recommendations of the guidelines and compares the recommendations to those made by the JNC 7, as well as with previous reports by the NKF and ADA. Limitations, implementation issues, and research recommendations are covered in subsequent guidelines. RATIONALE Definitions Antihypertensive therapy includes lifestyle modifications and pharmacological therapy that reduce blood pressure, in patients with or without hypertension. Lifestyle modifications include changes in diet, exercise, and habits that may slow the progression of CKD or lower the risk of CVD. These guidelines focus specifically on lifestyle modifications that lower blood pressure. Lifestyle modifications are discussed in more detail in Guideline 6. Pharmacological therapy includes selection of antihypertensive agents and blood pressure goals. Antihypertensive agents are defined as agents that lower blood pressure and are usually prescribed to hypertensive individuals for this purpose. Other agents may also lower blood pressure as a side-effect. It is important to note that antihypertensive agents may have salutary effects on CKD and CVD in addition to lowering systemic blood pressure, such as reducing proteinuria, slowing GFR decline, and inhibiting other pathogenetic mechanisms of kidney disease progression and CVD. General principles of pharmacological therapy and target blood pressure for reducing CVD risk are discussed in Guideline 7. "Preferred agents." Classes of antihypertensive agents that have beneficial effects on progression of CKD or reducing CVD risk, in addition to their antihypertensive effects, are defined as "preferred agents" for those conditions. Preferred agents for specific types of CVD are discussed in Guideline 7. In certain types of CKD, specific classes of antihypertensive agents, notably those that inhibit the renin-angiotensin system (RAS), are preferred agents for slowing progression of kidney disease. Thus, the guidelines recommend the use of specific classes of antihypertensive agents in certain types of CKD, even if hypertension is not present. These agents also reduce proteinuria and may be considered for this purpose as well. Preferred agents
. Patients with CKD are at increased risk of CVD. Hypertension is a risk factor for CVD events in CKD.")
3 for CKD are discussed in Guidelines 8 through 10. ACE inhibitors and angiotensin receptor blockers are discussed in Guideline 11, and diuretics are discussed in Guideline 12. Strength of Evidence Patients with CKD are in the "highest-risk" group for CVD (Strong). Patients with CKD are at increased risk of CVD. Hypertension is a risk factor for CVD events in CKD. However, there have been few controlled trials to demonstrate the efficacy of blood pressure lowering to reduce the risk of CVD in CKD; therefore, the Work Group made recommendations for CKD based on extrapolation from evidence on the efficacy of antihypertensive therapy in the general population. Because of the high risk of CVD in CKD, the Work Group concluded that individuals with CKD should be included in the "highest-risk group" for implementation of antihypertensive therapy to reduce CVD risk. Table 42 shows recommendations from JNC 7 for the highest-risk group. Guideline 7 discusses the appropriate blood pressure target to reduce risk of CVD in the highest-risk group. Some classes of antihypertensive agents are preferred in certain types of CKD (Strong). Most patients with CKD experience progressive GFR decline over time. Hypertension is a risk factor for faster progression of kidney disease. In addition, some other modifiable risk factors (proteinuria and activity of the RAS) are also affected by antihypertensive therapy. RCTs demonstrate that some classes of antihypertensive agents (notably, those that inhibit the RAS) are "preferred agents" for slowing progression of specific types of CKD. In addition, for some types of CKD, the blood pressure goal recommended for CVD risk reduction in high-risk groups has been shown to slow the progression of CKD. Thus, the Work Group recommended that antihypertensive therapy in CKD also be guided by the type of kidney disease. Table 43 shows general recommendations to slow the progression of CKD. Guidelines 8 through 10 discuss specific types of CKD. Level of proteinuria and changes in the level of proteinuria may be a guide to modifications of antihypertensive therapy (Weak). Proteinuria is important in CKD for a number of reasons. It is a marker for kidney damage, a clue to the type (diagnosis of CKD), and a risk factor for faster progression of kidney disease and development of CVD, and it identifies patients who benefit more from preferred agents and a lower target blood pressure (Table 29). In addition, it has been hypothesized that changes in the level of proteinuria during treatment may be a surrogate

4 outcome for kidney disease progression. The Work Group concluded that there is not yet sufficient evidence to confirm this hypothesis. However, it was the opinion of the Work Group that proteinuria should be monitored during the course of CKD, and that under some circumstances it would be appropriate to consider modifications to antihypertensive therapy, such as a lower blood pressure goal or measures to reduce proteinuria, such as increasing the dosage of preferred agents and selection of additional antihypertensive agents (Table 44). These measures are discussed in more detail in Guidelines 8 through 11. In general, these measures should be undertaken in consultation with a kidney disease specialist. The Work Group strongly recommended further research on this topic. Approach to hypertension and use of antihypertensive agents in CKD (Strong). Figure 28 and Table 45 describe a the general approach recommended by the Work Group to integrate goals of lowering blood pressure, reducing CVD risk, slowing progression of kidney disease, and considerations regarding proteinuria. Fig 28. General approach to hypertension and use of antihypertensive agents in CKD. Diamonds indicate decisions. Rectangles indicate actions. Superscripts refer to items listed in Table 45. A more detailed approach to decision-making and protocols for action are given in later sections. Most patients with CKD will require multiple interventions to slow progression of CKD and prevent development or worsening of CVD (Strong). Most patients with CKD have multiple risk

5 factors for progression of kidney disease and for development or deterioration of CVD. 3,4 Optimal management of CKD requires coordination of antihypertensive therapy with other therapies, such as smoking cessation, lipid-lowering therapy, and management of diabetes, and other dietary and life-style modifications, which is best accomplished by a coordinated effort among practitioners, either in an individual or a team setting 101,102 For example, the ADA recommends a multidisciplinary team approach for management of diabetes, 6 and some studies show improved outcomes for diabetic kidney disease, using a multidisciplinary approach to deliver multiple interventions. 103,104 The Work Group recommended coordination of antihypertensive therapy with other therapies for CKD and CVD as part of a multi-intervention strategy, using the resources of a multidisciplinary team, if available. A multidisciplinary team could include one or more of the following in addition to the physician: nurse practitioner, registered nurse, registered dietitian, masters prepared social worker, pharmacist, and physician assistant. Individual decision-making is necessary to resolve discrepancies between recommendations for slowing CKD progression and reducing CVD risk (Strong). The Work Group accepted the principle that recommendations should maximize net health benefits for the target population (see Appendix 1). Having defined the goals for antihypertensive therapy to include slowing progression of CKD and reducing CVD risk in addition to lowering blood pressure, the Work Group searched for evidence in the target population for each clinical outcome. In general, there were few studies that adequately assessed both outcomes; thus, the Work Group made recommendations on the basis of separate studies on each outcome. This is a reasonable approach, if the recommendations to slow progression of CKD and reduce risk of CVD agree; however, if there is a discrepancy between recommendations, this approach may not be adequate. Other approaches, such as decision analysis, with or without regard to cost, could be useful to determine net health benefits in this situation.
6 In general, the Work Group found few examples of such discrepancies. However, it should be noted that most clinical studies (observational studies and controlled trials) do not provide an adequate framework for examining the possibility of conflicts. Nonetheless, there are inconsistent results among some recent controlled trials with regard to the beneficial effect of ACE inhibitors aside from their antihypertensive effect on slowing progression of CKD and reducing risk of CVD Pertinent results will be discussed in later guidelines, but some general comments are appropriate here. In part, differences among studies may be related to differences in study populations and definition and ascertainment of endpoints. For example, studies on the progression of CKD have included patients with either markers of kidney damage (eg, diabetic patients with proteinuria) or decreased GFR (eg, most studies of nondiabetic kidney disease) and have carefully measured kidney function. On the other hand, studies of CVD risk reduction have generally excluded patients with elevated serum creatinine, did not routinely measure urine protein, and concentrated on ascertainment of CVD events. Thus, it is likely that studies on CKD enrolled patients at greater risk for progression of CKD than for CVD events and had greater statistical power to detect effects on CKD progression than on CVD events. Similarly, studies on CVD enrolled patients at greater risk for CVD events than for progression of CKD and had greater statistical power to detect effects on CVD events than progression of CKD. Hence, the Work Group generally restricted the interpretation of these studies to the primary outcome, as specified in advance by the authors. Differences in study design are discussed in an attempt to resolve discrepancies in findings and, in some studies, secondary outcomes are discussed. Overall recommendations are based on the sum of evidence, after taking into consideration all these factors. In clinical practice, health-care providers must be concerned with all outcomes of care, not just a "primary outcome." Health-care providers caring for patients with CKD routinely encounter patients at high risk of both progression of CKD and CVD events and must make decisions about the implementation of recommendations about lifestyle modifications, blood pressure targets, and classes of antihypertensive agents that affect both outcomes. For example, should a patient with Stage 3 CKD due to Type 1 diabetes, a recent myocardial infarction, and Stage 1 hypertension be treated with an ACE inhibitor, beta-blocker, or diuretic? All classes of agents may be indicated, but if the blood pressure is too low, which agents should be used preferentially? Where recommendations are discrepant, health-care providers must make decisions to maximize the net health benefits for the individual patient. The Work Group recommends that such individual decision-making be based on risk stratification. In general, the selection of antihypertensive therapy should be directed to the clinical condition that is most likely to occur and that has the most serious consequences on overall survival and quality of life of the individual patient. Clinical practice guidelines cannot substitute for individual decisionmaking in patients with complex medical problems. Comparison to Other Guidelines In addition to the JNC, several organizations have issued recommendations for blood pressure management in CKD. Previous recommendations by the NKF and other groups are listed in Table 46. 1,15, Guidelines for CVD risk reduction in individuals without CKD are reviewed in Guideline 7. Guidelines for individuals with CKD are reviewed in Guidelines 8 through 10. In this discussion, the focus is on recommendations by JNC and ADA because these are the most
. JNC 6 suggested risk stratification of individuals with hypertension for therapeutic decisions.")
7 widely used guidelines for treatment of individuals with hypertension and diabetes the two most common causes of CKD. During the Work Group s meetings, JNC 6 15 and ADA ,116 were available. Risk stratification (Table 47). JNC 6 suggested risk stratification of individuals with hypertension for therapeutic decisions. 15 Although JNC 7 simplified this classification, the Work Group found the concepts useful in its deliberations. There is a spectrum of risk from very high to low, and patients were classified into three general risk categories. Patients at "low risk" (Group A) were defined as those without pre-existing CVD or target organ damage, without diabetes, and with no other risk factors for CVD other than hypertension. Patients at "high risk" (Group B) were defined as those without CVD or target organ damage, without diabetes, but with one or more with other risk factors for CVD. Patients at "very high risk" (Group C) were defined as those with CVD, target organ damage, or compelling indications, such as diabetes and CKD. Because there are few studies of antihypertensive therapy on CVD in CKD and because patients with CKD are in the highest-risk category for CVD, the Work Group recommends extrapolating the results from studies in the general population and other highest-risk populations to CKD (see Guideline 7).

8 Recommendations for low- and high-risk groups. JNC 6 and JNC 7 focus on therapeutic strategies to achieve target blood pressure level. The recommended goal of antihypertensive therapy in patients in risk groups A and B is to maintain SBP and DBP <140 mm Hg and <90 mm Hg, respectively. These definitions and goals do not differ according to age (among adults), gender, or race. Lifestyle modification is recommended for 6 to 12 months, followed by antihypertensive therapy if blood pressure remains above goal. The recommended initial antihypertensive agent is generally a diuretic, in combination with an ACE inhibitor, ARB, ß- adrenergic blocker, or a calcium-channel blocker if more than one agent is necessary to reach the target blood pressure. Recommendations for the highest-risk group (Table 48). JNC 7 identifies the highest-risk group as those with "compelling indications" for antihypertensive therapy. Recommendations include prompt initiation of pharmacological therapy simultaneously with lifestyle modification, a lower blood pressure goal (<130/80 mm Hg), and antihypertensive medications specific to the comorbid conditions. In particular, ACE inhibitors and ARBs are recommended for patients with heart failure, diabetes, and CKD. 5,5a

9 The 2003 ADA guidelines for treatment of hypertension in diabetic kidney disease recommend a blood pressure goal of <130/80 mm Hg and preferential use of ACE inhibitors in all diabetic patients with hypertension or CKD. ARBs are preferred in patients with macroalbuminuria and decreased GFR due to type 2 diabetes. 6,121 A draft of the 2004 ADA guidelines available at the time the K/DOQI Guidelines contained similar recommendations. Guidelines proposed by the NKF-K/DOQI Work Group on Hypertension and Antihypertensive Agents in CKD supersede those proposed by previous NKF groups 1,3,4,112 and are largely consistent with recommendations by JNC 7 and ADA. GUIDELINE 3: MEASUREMENT OF BLOOD PRESSURE IN ADULTS Blood pressure can be determined by resting blood pressure measurement in the healthcare provider s office (casual blood pressure [CBP]), self-measured blood pressure (SMBP), or ambulatory blood pressure monitoring (ABPM).
10 3.1 Blood pressure should be measured according to the recommendations for indirect measurement of arterial blood pressure of the American Heart Association and Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC 7) (A). 3.2 Patients should be taught to measure and record their blood pressure, whenever possible (C). 3.3 Ambulatory blood pressure monitoring should be considered for patients with CKD for the following indications (C): 3.3.a Suspected white coat hypertension 3.3.b Resistant hypertension 3.3.c Hypotensive symptoms while taking antihypertensive medications 3.3.d Episodic hypertension 3.3.e Autonomic dysfunction BACKGROUND CBP recorded in a clinic/office setting is the standard technique for measurement of blood pressure. Techniques for this measurement are well detailed in the Seventh Report of the Joint National Committee (JNC) on the Prevention, Detection, Evaluation and Treatment of High Blood Pressure 5,5a as well as many recent reviews The purpose of Guideline 3 is to review the recommended measurement methods for adults, particularly in relation to CKD. A discussion of blood pressure measurement and interpretation in children is given in Guideline 13. The measurement of blood pressure in this technological age has never been more confusing or difficult. The currently available CVD risk prediction data come from studies that primarily used an auscultation technique with mercury manometer. 144 Environmental concerns have led to the abolishment of mercury columns in many US and most European health-care facilities. 145 Aneroid manometers can be accurate if maintained by an intensive and difficult to achieve calibration and maintenance program. Automated devices using oscillometric technology have gained great popularity due to ease of use and improved interobserver variability. Not surprisingly, these devices that measure vessel oscillations do not always correlate well with auscultatory techniques 146 and also require frequent calibrations performed by the manufacturer. Thus, from a clinical perspective, it is not clear which are the best monitors to use for CBP measurement. However, even if CBP measurement by standardized protocols is performed under ideal circumstances, they have a number of limitations, especially in conditions, such as CKD, in which known aberrations in circadian blood pressure patterns exist. SMBP provides multiple blood pressure measurements in the patient s own environment but is a technique with many
11 technical and reporting reliability issues. Studies relating the SMBP data to target organ damage are lacking. ABPM provides objective blood pressure measurements in the patient s own environment over the full circadian period and correlates well with target organ damage. Normative data, based on epidemiological studies, outcome measures, and cardiovascular events, have now been developed for ABPM. Guideline 3 briefly summarizes more recent data on SMBP and ABPM, with a more detailed discussion in Appendix 3. As technology advances, the ultimate goal for antihypertensive therapy is to develop what has been termed "the virtual hypertension clinic" 147 using CBP for screening, ABPM for initial diagnosis, and monitoring changes in treatment; and SMBP with electronic linkage between the patient and the health-care provider for maintenance and follow-up. RATIONALE Definitions Casual blood pressure (CBP): CBP refers to a blood pressure measurement taken in the physician s office or clinic setting using one of several techniques. Auscultatory techniques with aneroid or mercury manometers and automatic oscillometric devices are most commonly used. Measurement under standardized conditions should be taken at least twice and an average of the two recorded at every health-care encounter. 5 Multiple measurements at different encounters are required for accurate correlation to end-organ damage. Self-measured blood pressure (SMBP): SMBP refers to blood pressure measurements taken by the patient in his/her usual environment. SMPB devices 142 are varied in design from manual to fully automated and in blood pressure measurement technique (mercury, aneroid, oscillometric). Little is known about the accuracy, reliability, and predictive value of SMBP, especially in CKD patients. Patients performing SMBP should be trained and periodically monitored. Ambulatory blood pressure monitoring (ABPM): A variety of fully validated, reliable, automated, and accurate monitors are available. Blood pressure measurements taken every 15 to 20 minutes are recorded over 24 to 48 hours. Oscillometric monitors are most commonly used and auscultatory monitors with or without ECG gating also give excellent results. Data downloaded from the monitor are generally divided into day (diurnal) or night (nocturnal) periods. Daytime (awake) ambulatory blood pressure (ABP) values are lower than clinic readings, 10% to 20% higher than nighttime (asleep) readings, and provides measures of SBP and DBP load (percentage of blood pressure readings exceeding the upper limits of normal for a given time period). As blood pressure is more closely related to the sleep-wake cycle rather than day and night, as illustrated by the blood pressure rhythm following the inverted cycle of activity in night-shift workers, the time of sleep and wake during ABPM should be recorded in the patient diary or objectively determined with a motion-logger (actigraph). Recently, monitoring has been approved for reimbursement in selected settings including the identification of whitecoat hypertension (WCH). A consensus view on ABPM technique is available. 148 While reproducibility on repeated ABPMs for group data is excellent, concerns regarding individual patient reproducibility have been raised. 149
12 Ambulatory hypertension: Ambulatory hypertension is most commonly diagnosed by a mean SBP or DBP exceeding normal values for the full 24-hour period. Other definitions include blood pressure values that exceed normal during the waking period (diurnal hypertension) or the sleep period (nocturnal or sleep hypertension). Blood pressure load has a strong predictive value for end-organ damage. Other promising analytic techniques need further validation, such as the cosinor analysis, modified LMS of Cole and Green (where the distribution of a measurement Y is described by its median [M], the coefficient of variation [S], and a measure of skewness [L] required to transform the data to normality), 150 blood pressure index, and hyperbaric index. White coat hypertension (WCH): WCH refers to a condition in which blood pressure is repeatedly elevated on CBP measurement in the presence of a health-care professional but normal by ABP or SMBP. WCH for adults is defined by CBP >140 mm Hg, but a mean blood pressure by ABPM of <135/85 mm Hg for the wake period or <135/80 mm Hg for the full day. Some consider that the criteria include a blood pressure load <25%. Whether WCH is associated with end-organ damage is controversial and definition-dependent. Patients with WCH defined by 24-hour mean blood pressure <135/85 mm Hg have a prevalence of end-organ damage or CV events not different from normotensive patients. However, WCH may prove to be a prehypertensive state. Dipping: Dipping describes an ABP pattern in which the mean wake SBP or DBP falls at least 10% during sleep. A sleep-related blood pressure reduction that is greater than 20% to 30% has been termed super-dipping, which is associated with neurological sequelae. 151 Nondipping: Nondipping describes a pattern of a blunted sleep-related fall in mean SBP or DBP (<10%). This pattern is commonly seen in CKD. The most severe form is a reversal of blood pressure in which the sleep blood pressure is equal or higher to awake values. Some have termed this "reverse dipping" and connotes a very high risk for end-organ damage. Scope of Work Studies reviewed for this guideline included authoritative reviews, including JNC 6 15 and JNC 7 5,5a ; a meta-analysis conducted for AHRQ 142 National High Blood Pressure Educational Program (NHBPEP)/National Heart, Lung and Blood Institute, 152 and American Heart Association (AHA) Working Meeting on Blood Pressure Measurement and its summary report 144 ; AHA recommendations for indirect measurement of arterial blood pressure, 153 European Society of Hypertension recommendations for conventional, ambulatory, and home blood pressure measurement 143 ; and an international conference on ABPM in More detailed information about blood pressure measurement techniques can be found in these reports. Strength of Evidence Accurate measurement of blood pressure is important for detection, evaluation, and treatment of hypertension (Strong). JNC 7 provides a new, simplified classification of hypertension severity for adults aged 18 years and older (Table 23). The classification is based on the average of two or more properly measured seated blood pressure readings on each of two or more office
13 visits. When SBP and DBP fall into different categories, the higher category should be selected to classify the individual. Accurate measurement in CKD is especially important, because hypertension is more common in CKD, and because JNC 7 identifies CKD as a "compelling indication" for more aggressive antihypertensive therapy because of the higher risk of CVD in CKD than in the general population. Accurate assignment of blood pressure status is crucial from a public health standpoint. 144 The risk associated with increasing blood pressure is graded and continuous and begins at 115/75 mm Hg. Overestimating or underestimating blood pressure by even 5 mm Hg can mislabel over 20 million persons as having high normal blood pressure rather than hypertension; conversely, another 20 to 30 million could be misclassified as hypertensive exposing these persons to the expense and adverse effects of treatment. This issue is compounded by the challenge of the "white coat" or "office" effect. Misclassification in CKD can be compounded by altered circadian blood pressure rhythms such as a nondipping pattern. The following techniques that are recommended for accurate measurement of casual blood pressure in the general population are also recommended in CKD (Strong). The following issues are common to all measurements and all devices. Issues related to type of blood pressure measurement and specific devices are discussed next. Patients should be seated quietly for at least 5 minutes in a chair (rather than on an exam table) with their backs supported and their arms bared and supported at heart level. Patients should refrain from smoking or ingesting caffeine during the 30 minutes preceding the measurement. Each patient should be provided, verbally and in writing, with their specific blood pressure numbers and blood pressure goals. Correct measurement of blood pressure requires the use of a cuff that is appropriate to the size of the upper right arm. The right arm is preferred for consistency and comparison with the standard tables. A technique to establish an appropriate cuff size is to choose a cuff having a bladder width that is approximately 40% of the arm circumference midway between the olecranon and the acromion. Issues of cuff size are especially important in children (see Guideline 13) and obese adults. With the increasing prevalence of obesity, many adults will require a large adult cuff. Those with large, conical arms >41 cm in circumference may require the blood pressure to be measured on their forearms. Too small an inflatable bladder can lead to false readings of elevated blood pressure in the range of 3.2/2.4 mm Hg to 12/8 mm Hg with as much as 30 mm Hg in the obese. An excessively large bladder may lead to falsely low readings in the range of 10 to 30 mm Hg. The bladder within the cuff should encircle at least 80% of the arm. The bell of the stethoscope should be lightly placed over the brachial artery pulse, proximal and medial to the cubital fossa, and below the bottom edge of the cuff (ie, about 2 cm above the cubital fossa). The cuff should be inflated to 30 mm Hg above palpated SBP and deflated at a rate of 2 to 3 mm Hg/second. Both SBP and DBP should be recorded. The first appearance of sound (phase 1) is used to define SBP. The disappearance of sound (phase 5) is used to define DBP in adults. It has been suggested that a detailed accounting of blood pressure on the initial visit include position of individual; arm selected; blood pressure monitor used; blood pressure measured on both arms; arm circumference and cuff used; if
14 auscultatory Korotkoff sounds IV and V, presence of auscultatory gap; emotional state of individual; and time of drug ingestions. 143 Two or more readings separated by 2 minutes should be averaged. If the first two readings differ by more than 5 mm Hg, additional readings should be obtained and averaged. Elevated blood pressure must be confirmed on repeated visits before characterizing an individual as having hypertension. Blood pressure at the high levels tends to fall on subsequent measurement as the result of (1) an accommodation effect (ie, reduction of anxiety by the patient from one visit to the next) and (2) regression to the mean, a nonbiological phenomenon that derives, in part, from mathematical considerations. Blood pressure level is not static but varies even under standard resting conditions. Therefore, a more precise characterization of an individual s blood pressure level is an average of multiple blood pressure measurements taken repeatedly over several weeks to months. Especially among older persons and children, SBP is a better predictor of end-organ damage and events (coronary heart disease, CVD, heart failure, stroke, kidney failure, and all-cause mortality) than is DBP. Recently, it has become clear that an elevated pulse pressure (SBP minus DBP), which indicates reduced vascular compliance in large arteries, may be an even better marker of increased cardiovascular risk than either SBP or DBP alone. New, noninvasive techniques are being validated that can accurately measure vascular compliance. Early evidence suggests the presence of reduced vascular compliance in CKD. 155 Under special circumstances, measuring blood pressure in the supine, sitting, and standing positions (standing quietly for 2 to 5 minutes) may be indicated and helpful in detecting evidence of autonomic dysfunction. A decrease in standing SBP >10 mm Hg when associated with dizziness or fainting is more frequent in older patients with systolic hypertension, diabetes, and those taking diuretics, venodilators (eg, nitrates, alphablockers, and sildenafil-like drugs), and some psychotropic drugs. This same recommendation is made for patients taking drugs that exaggerate postural changes in blood pressure (peripheral adrenergic blockers, alpha-blockers, and high-dose diuretics). ABPM may be especially helpful in this situation. Blood pressure must be measured in older persons with special care as some older persons have pseudohypertension (falsely high sphygmomanometer readings) due to excessive vascular stiffness as determined for example by using pulse wave pressure. In addition, older persons with hypertension, especially women, may have WCH and excessive variability in SBP. In the absence of target-organ damage, clinicians should consider pseudohypertension or WCH. ABPM may be helpful in this instance. Casual blood pressure measurement using the mercury manometer is the "gold standard" for clinical studies, but has important limitations in clinical practice (Strong). One of the most controversial areas is the choice of equipment for blood pressure measurement. Measurements should be taken preferably with a mercury sphygmomanometer if available. Otherwise, a calibrated aneroid manometer or a validated electronic device can be used. Technical problems exist with all forms of blood pressure measurement. Even the gold standard of intra-arterial blood pressure measurement has technical problems and variability depending on the chosen artery, catheter positioning within the artery, and equipment used. The two major noninvasive

15 CBP measurement techniques are auscultatory and oscillometric. The hybrid manometer and devices based on wideband K2 method are future technologies that may be helpful. 143 CBP measurements can be misleading due to errors from lack of observer training, incorrect cuff size, incorrect patient position, rapid cuff deflation, terminal digit preferences, monitor not kept at eye level (parallax), and inadequate premeasurement rest as well as the stress of the office setting (Table 73). The aforementioned problems have led to a proliferation of easier-to- use automated devices using oscillometric technologies. Users of these devices need to realize that the oscillometric technique is not based on the same physiological observation as auscultation 144 and thus may yield different results. Even if office blood pressure measurements follow standardized protocols under ideal circumstances, the measurements are limited by tremendous variability. Use of a single measurement to characterize the chronic behavior of a continuous variable may be unrealistic. Further, the measurement may not be representative of blood pressure levels in the patient s own environment and at different times of day. This is especially true when known aberrations in circadian blood pressure patterns exist in a given clinical condition, such as in CKD. Whatever the chosen device, the guidelines of the future should be evidence-based rather than consensusbased. Regulatory agencies need to establish standards for the use of validated devices, the frequency of calibration, and the continued certification of observers using manual devices. The use of automated devices does not eliminate all major sources of human error and thus observers still require training. Manufacturers of automated devices should validate their algorithms in special populations such as the elderly and those with CKD. Mercury manometers. Despite their status as the gold standard, mercury manometers, when systematically evaluated, have a significant number of problems that may preclude accurate use, even if the observer and patient issues are overcome. In several studies, a high prevalence of technical problems (18% to 38%) was noted, such as dirty columns, oxidized mercury, faded column markings, air mixed in the mercury column, or mercury leakage leading to inaccurate measurement in 21% of monitors In a systematic evaluation of sphygmomanometers, none of the 356 instruments tested met all standards and 86% did not meet safety standards. 159 In
16 addition, because of the environmental hazard posed by mercury, most mercury manometers in hospitals and other health care facilities in the United States are being replaced by other instruments. Aneroid manometers. The aneroid manometer functions by use of a system comprised of a metal bellows, a mechanical amplifier, springs, and a gauge that displays the pressure in the cuff and tubing of the sphygmomanometer. Aneroid devices are often felt to be less accurate than mercury columns because they are so difficult to keep in calibration. 153 Aneroid manometers were evaluated in many of the same studies cited for the assessment of mercury manometers and demonstrate even more inaccuracies than with mercury. Oscillometric devices. Oscillometric monitors measure the mean arterial pressure by determining the maximum oscillations in the vessel. The device then calculates SBP and DBP from proprietary algorithms. There is great variability in blood pressure readings among available devices. We have no standards for normal blood pressure based on this technology. Further, there are concerns that increased arterial stiffness as seen in CKD and the elderly can lead to greater variations in blood pressure results by oscillometry compared to auscultation. Some companies are developing special algorithms for these situations. Self-measured blood pressure is a useful adjunct to casual blood pressure monitoring (Moderately Strong). Self-measurement of blood pressure has five general advantages: (1) distinguishing sustained hypertension from WCH; (2) assessing response to antihypertensive medication; (3) interpreting symptoms that may be due to hypotension; (4) improving patient adherence to treatment; and (5) potentially reducing costs. The blood pressure of persons with hypertension tends to be higher when measured in the clinic than outside of the office. There is no universally agreed-on upper limit of normal home blood pressure, but readings of 135/85 mm Hg or greater should be considered elevated. 5 The techniques of a well-performed CBP should be used with SMBP including a 5-minute rest before the sitting measurement. The technique is carefully outlined in the European Society of Hypertension Report. 143 Choice of monitors for personal use. A mercury sphygmomanometer is generally not practical for home use. Therefore, either validated electronic devices (oscillometric) or aneroid sphygmomanometers are recommended for use along with appropriately sized cuffs. Finger and wrist monitors are inaccurate. Periodically, the accuracy of any device should be checked by comparing readings with simultaneously recorded auscultatory readings taken with a mercury device. Few of the many self monitors on the market have passed British Hypertension Society 160 /Association for the Advancement of Medical Instrumentation standards. 161 A Task Force of the European Society of Hypertension has suggested new criteria for this assessment. 162 A review of available monitors has been published recently. 160,163 Comparison of SMBP with CBP measurement and ABPM. Blood pressure measured by any technique outside of the physicians office tends to have lower values. In six studies comparing SMBP and CBP, a consistently lower blood pressure by SMBP (SBP 5.4 ± 17.7 mm Hg and DBP 1.5 ± 6.3 mm Hg) was demonstrated. Three studies comparing ABPM and SMBP show similar daytime blood pressure results. While ABPM is the gold standard for the determination of WCH, SMBP is comparable to ABPM for prevalence of WCH (approximately 20%). The
17 published literature is insufficient to provide an answer to the predictive ability of SMBP for target-organ damage or clinical events. Interventions that included SMBP for assessment of antihypertensive effect showed improved blood pressure control in 6 of 12 trials. 142 Of the two trials that used technology storing the blood pressure data in the monitor, significantly reduced blood pressure was seen. Thus, while the results are inconsistent, there is promise especially with report-generating monitors that SMBP can lead to reduced blood pressure. SMBP reliability. The reliability of the patient recording of the blood pressure measurement is critical if this technique is to be trusted. Patients consistently misreport the results of the monitor when patient manual recordings are compared to a device that stored readings unbeknownst to the patient. Patient reports had mean differences in blood pressure of at least 10 mm Hg for SBP and 5 mm Hg for DBP compared to stored readings. 164 In another study, 36% of patients underreported and 9% overreported blood pressure readings. Log books also had phantom readings noted; conversely, patients failed to report measurements that were taken and stored. 165 Similar findings were observed with other monitoring technologies such as glucometers for diabetic patients 166 and for recording metered dose inhaler usage in asthmatic patients. 167 Thus, objective recording of the data is strongly advised. The Work Group concluded that SMBP is a useful adjunct to CBP measurement with properly validated monitors, can be performed by many patients, and is consistent with the goal of self-management. ABPM is useful to identify abnormal blood pressure patterns in CKD and is closely correlated with target-organ damage (Strong). Monitoring of blood pressure in an ambulatory setting provides multiple, objective blood pressure measurements in the patient s own environment over a full circadian period. 168 While ABPM has become a valuable clinical and research tool, it has yet to gain wide acceptance in the United States due to reimbursement issues, equipment expenses, and time efforts to train patients in monitor use. The Center for Medicare and Medicaid Services (CMS) has approved ABPM use for patients suspected of white coat hypertension. 169 In Europe, however, ABPM has become a mainstay of blood pressure diagnosis and management. WHO-ISH suggests it be used for unusual variability of blood pressure, office hypertension in low-risk patients, symptoms suggesting hypotensive episodes, and resistant hypertension. JNC 7 suggests ABPM can be useful for suspected WCH, resistant hypertension, hypotensive symptoms while taking antihypertensives, episodic hypertension, and autonomic dysfunction. Recent authoritative reviews suggest advantages of ABPM in essential hypertension. 142 ABPM facilitates the diagnosis of WCH, a prehypertensive state that shows a lack of end-organ damage similar to that seen in normotensive individuals. 170 Conversely, it has been reported that as many as 9% of patients may have normal office blood pressure but elevations during ABPM; a condition termed "masked hypertension" which is also associated with end-organ damage Among persons with hypertension, an extensive and very consistent body of evidence indicates that ambulatory blood pressure correlates more closely than casual blood pressure with a variety of measures of target-organ damage such as left ventricular hypertrophy. 15,174 Ambulatory blood pressure values are usually lower than clinic readings. While awake, individuals with hypertension have an average blood pressure of more than 135/85 mm Hg and during sleep, more than 120/75 mm Hg (Table 74). In most individuals, blood pressure decreases
18 by 10% to 20% during the night; those in whom such reductions are not present are at increased risk for cardiovascular events. CKD is commonly associated with alterations in the circadian patterns of blood pressure; the most frequent of these rhythm abnormalities is nocturnal (sleep) period hypertension and a nondipping blood pressure pattern As stated in JNC 7, the level of mean ABP or blood pressure load correlates better than office measurements with target organ injury. Abnormal ambulatory patterns have been shown to be related to varying degrees of abnormal protein excretion, 179 to more rapid progression of kidney disease, and to CV damage and events. 183 Due to these abnormal patterns, the correlation between CBP and ABP is poor, as is the relationship of CBP to end-organ damage. 178,184 Several ABPM patterns noted in CKD patients and not detected by CBP measurement can impact therapeutic decisions. First, the requirement for antihypertensive therapy may be affected by the diagnosis of WCH. 185 Secondly, the identification of a nondipping, reverse dipping, or nocturnal hypertension may lead to more aggressive antihypertensive regimen and affect the timing of dosing. 180 Further, a recent study of treated hypertensive patients 172 suggests that ambulatory blood pressure of >130/80 mm Hg is associated with cardiovascular events even with a normal office blood pressure. Thus, data are accumulating, but are not yet conclusive for the usefulness of routine ABPM for antihypertensive therapy. In summary, ABPM is a powerful tool that has a close correlation with end-organ damage, including progression of kidney disease, and cardiovascular and cerebrovascular outcomes. It is of particular benefit in patients with CKD who have a known alteration in the circadian blood pressure pattern. The presence of a nondipping pattern or nocturnal hypertension in a patient with CKD places an already high-risk patient into an even higher risk level. Possibly, this knowledge can be helpful in suggesting an even more intensive therapeutic regimen. However, the Work Group did not find a sufficient number of large studies demonstrating an additional benefit of ABPM over CBP measurements in the management of hypertension in CKD. Thus, the Work Group concluded that additional evidence is required to recommend ABPM as a routine diagnostic tool or as a guide to blood pressure management in CKD. Until such evidence is available, health-care providers may find benefit in choosing to recommend ABPM for patients with CKD. 186 Circumstances for effective utilization of ABPM in patients with CKD are seen in Table 75.


19 SUMMARY A summary of special considerations in blood pressure measurement for patients with CKD is found in Table 76. LIMITATIONS AND IMPLEMENTATION ISSUES ABPM is becoming more widely used, yet important limitations remain such as the expense of equipment and software, and personnel required to apply the equipment; high test-retest variability in some individuals, and reimbursement issues. While reimbursement for the use of ABPM in diagnosing white coat hypertension has been approved by the Center for Medicare and Medicaid Services, it is not yet approved for conditions with altered patterns of blood pressure as in CKD. Self-measurement of blood pressure has a much lower cost and few side-effects. It allows improved assessment of blood pressure and its control but the technology requires more careful scrutiny of quality and accuracy and the use of devices to objectively record the data to improve reporting. Digital read-out devices simplify SMBP. Clinicians need to devote time for teaching and assessing patient accuracy. Development of instructional material for patients with a wide range of educational levels and cultural backgrounds will be important. The disappearance of mercury manometry will lead to new challenges and opportunities. We may be entering a new age of blood pressure measurement with the introduction of innovative technologies that will allow not only accurate, noninvasive measurement of blood pressure but
20 also an assessment of blood pressure as a dynamic process with the ability to measure the cardiac and vascular components of blood pressure, thereby bringing new understanding and opportunities for early diagnosis and therapies. RESEARCH RECOMMENDATIONS There are many unanswered questions related to the measurement of blood pressure in the CKD population. Research should specifically be performed in the patients with CKD who have been documented to have abnormal vascular compliance, to determine if oscillometric monitors for casual measurements give accurate results. If differences are noted, oscillometric normal values should be developed as they were for ABPM. Controlled trials need to be performed to determine if blood pressure management in CKD patients with ABPM is superior to CBP guided therapy More research into the prognostic ability of SMBP is needed. A systematic attempt should be made to test all home blood pressure monitors for accuracy especially when used for patients with CKD. Should all patients with CKD, especially those with higher stages of CKD have ABPM, even if normotensive, to determine the presence of dipper status? Does WCH predispose to sustained hypertension? Should the definition of WCH take into account sleep blood pressure measurements for CKD patients? The data that alterations in circadian blood pressure rhythms are related to end-organ damage are strong, but would they benefit from a large multicenter study in CKD characterized by CKD stages? Does the normalization of circadian blood pressure pattern confer any protection? How would this be accomplished? Are some antihypertensive agents superior in this regard? What should be the dosage timing? More research using ABPM to adjust antihypertensive therapy is required. Research into the mechanisms of the abnormal blood pressure patterns coupled to the increase in endorgan damage is required and may lead to the development of new therapies. GUIDELINE 7: PHARMACOLOGICAL THERAPY: USE OF ANTIHYPERTENSIVE AGENTS IN CKD All antihypertensive agents can be used to lower blood pressure in CKD. Multidrug regimens will be necessary in most patients with CKD to achieve therapeutic goals. Patients with specific causes of kidney disease and CVD will benefit from specific classes of agents. 7.1 Patients with CKD should be considered in the "highest-risk" group for CVD for implementing recommendations for pharmacological therapy, irrespective of cause of CKD (A). 7.2 Target blood pressure for CVD risk reduction in CKD should be <130/80 mm Hg (B).
 and to avoid side-effects and interactions (B). 7.")
21 7.3 Antihypertensive agents should be prescribed as follows, when possible: 7.3.a Preferred agents for CKD should be used first (see Guidelines 8, 9, 10, 11) (A); 7.3.b Diuretics should be included in the antihypertensive regimen in most patients (A). 7.3.c Choose additional agents based on cardiovascular disease-specific indications to achieve therapeutic and preventive targets (Table 86) and to avoid side-effects and interactions (B). 7.4 The antihypertensive regimen should be simplified as much as possible (B). 7.4.a Long-acting (once-daily agents) should be used when possible (B). 7.4.b Two agents, either as separate prescriptions or as a fixed-dose combination containing preferred agents, may be considered as initial therapy for SBP >20 mm Hg above goal according to the stage of CKD and CVD risk (C). 7.4.c Fixed-dose combinations may be used for maintenance therapy after the antihypertensive regimen has been established (B). BACKGROUND The goals of antihypertensive therapy in CKD patients are to lower blood pressure, reduce the risk of CVD, and slow progression of CKD. Guideline 7 reviews the use of antihypertensive agents in CKD to lower blood pressure and reduce CVD risk. Use of antihypertensive agents to slow the progression of kidney disease is reviewed in Guidelines 8, 9, and 10. Numerous studies have documented the high risk of CVD in patients with CKD. There are several reasons for the high risk of CVD in particular, the older age of patients, the higher prevalence of traditional CVD risk factors (such as hypertension, diabetes and hyperlipidemia), and the presence of CKD-related risk factors such as coronary calcifications from an elevated calcium-phosphorous product. Because of their high risk of CVD, all individuals with CKD are included in the highest-risk group for CVD. A multipronged strategy is necessary to reduce the risk of CVD in this patient population, and hypertension is only one of the therapeutic areas that

22 need to be addressed. The NKF-K/DOQI guidelines on dyslipidemia and bone metabolism will include information on additional strategies to reduce CVD risk in patients with CKD. 285a,291 A large number of controlled trials have examined the efficacy of antihypertensive agents on reducing the risk of CVD, and many guidelines have been published on the use of antihypertensive agents to reduce CVD risk. Unfortunately, relatively few patients with CKD have been included in controlled trials of CVD risk reduction. Therefore, recommendations in JNC 6 and other guidelines available at the time of the Work Group review were not developed specifically for patients with CKD. The 1998 report of the Task Force for Cardiovascular Disease in Chronic Renal Disease developed criteria for extrapolation of recommendations on risk factor reduction from the general population to patients with CKD. 3 The Task Force concluded that recommendations for target blood pressure and antihypertensive agents in the general population could be extrapolated to patients with CKD. This section provides a review of the guidelines for the treatment of hypertension as well as a summary of the antihypertensive agents that can be used to achieve these therapeutic goals. "Preferred antihypertensive agents" are defined as antihypertensive agents that reduce CVD risk or slow the progression of certain types of kidney disease by mechanisms in addition to lowering blood pressure. Thus, preferred agents may be indicated in patients either with or without hypertension. The tables included in Guideline 7 show classes of antihypertensive agents and the indications for these agents in CKD, in addition to their effect on blood pressure. RATIONALE Criteria for Extrapolation of Recommendations From the General Population to CKD The Work Group adopted the criteria developed by the NKF Task Force on Cardiovascular Disease in Chronic Renal Disease for extrapolating evidence from the general population to the target population (Table 87). 1. The mechanism and expression of CVD in CKD should be similar to those observed in the general population. Specifically, the features of CVD, the relationship of CVD outcomes to hypertension, the mechanism of blood pressure lowering, and the responsiveness of risk factors to lifestyle modifications and pharmacological therapy should be similar in patients with CKD and the general population. 2. Therapies in patients with CKD should be as safe, or nearly so, as in the general population. In particular, there should not be additional adverse effects of a specific therapy that limits its
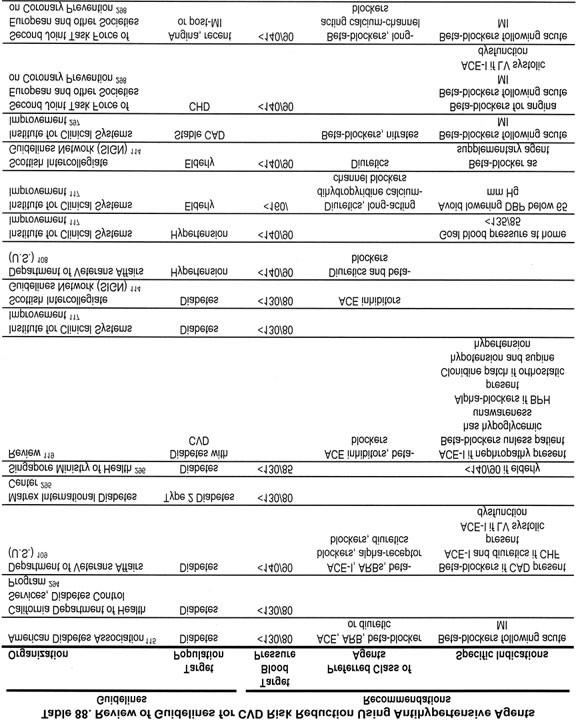
23 usefulness in patients with CKD, either because of altered pharmacokinetics, drug interactions, or increased risk of toxicity to the kidney. 3. The duration of therapy required to improve CVD outcomes in the general population should not exceed the life expectancy of patients with CKD. Numerous studies of CVD in the general population have shown a benefit of interventions within 2 to 5 years, with greater and earlier benefits in patients at highest risk. Thus, it is likely that patients with CKD Stages 1-4 could benefit from more effective treatment of CVD. Scope of Work There are few controlled trials comparing levels of blood pressure or classes of antihypertensive agents to reduce CVD risk in CKD. Thus, the Work Group extrapolated from guidelines of highrisk patients in the general population. The Work Group was convened in 2001, after the release of JNC 6 but prior to the release of JNC 7 in May The Work Group elected to review recommendations in JNC 6, as well as other guidelines for the treatment of hypertension and CVD that were published since JNC 6. Guidelines were identified by a review of guidelines listed in the National Guideline Clearinghouse ( A total of 21 guidelines were retrieved, of which 5 were found not to be relevant for this review. The remaining guidelines are summarized in Table 88.
24
 were able to review data from a subgroup of ALLHAT participants with CKD (defined as estimated GFR <60 ml/min/1.")
25 During the Work Group s deliberations, results of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) were reported, and JNC 7 was released. Some members of the Work Group (A.S.L. and M.V.R.) were able to review data from a subgroup of ALLHAT participants with CKD (defined as estimated GFR <60 ml/min/1.73 m 2 ), which was later reported in abstract form. 292,293 Thus, the Work Group also relied on evidence contained in the ALLHAT report, the ALLHAT CKD subgroup, some of the key clinical trials included in JNC 7, as well as recommendations of JNC 7. Clinical trials in the general population were abstracted or compiled in evidence tables. The Work Group also summarized information on antihypertensive drug classes in the general population, including indications, recommended doses, contraindications, side-effects, and interactions. In addition to the sources described above, textbooks and reviews were used as source material for this section. Diuretics and beta-blockers are discussed first, since these were the first agents tested in clinical trials of CVD. Newer agents, ACE inhibitors and ARBs, and calcium-channel blockers are discussed next, because there have been a large number of clinical trials in the general population to determine whether these agents are preferred for specific CKD and CVD indications. Agents that act on the alpha-adrenergic system and directly acting vasodilators are discussed briefly. Recently, there has been increased interest in aldosterone antagonists, which are discussed last. Strength of Evidence General principles in the use of antihypertensive agents in CKD (Fig 34 and Table 89) (Moderately Strong). All classes of antihypertensive agents are effective in lowering blood pressure in CKD. Figure 34 and Table 89 summarize these principles.
.")
26 Fig 34. Hypertension and antihypertensive agents in CKD. Superscripts refer to items in Table 89. Patients with CKD should be considered in the "highest-risk" group for CVD for implementing recommendations for pharmacological therapy, irrespective of cause of CKD (Strong). As noted earlier, patients with CKD have rates of CVD that are 5 to 500 times higher than age- and sex-matched controls in the general population (Fig 4). Thus, it is of the utmost importance to reduce the risk of CVD in patients with CKD. Target blood pressure for CVD risk reduction in CKD should be <130/80 mm Hg (Moderately Strong). Numerous epidemiological studies show a graded, independent, and strong relationship between the level of arterial blood pressure and CVD. Above a SBP of 115 mm Hg, and above a DBP of 75 mm Hg, the risk of CVD doubles with each increment of SBP of 20 mm Hg or DBP
27 of 10 mm Hg. In persons over age 50, SBP greater than 140 mm Hg is a critical and more important CVD risk factor than DBP. Controlled trials in essential hypertension conclusively show a beneficial effect of lowering blood pressure to <140/90 mm Hg. Controlled trials in high-risk individuals with diabetes or heart failure suggest beneficial effects of reduction of blood pressure to even lower values. Based on these studies, and on observational studies, a number of guidelines for patients with either diabetes mellitus or congestive heart failure recommend a goal blood pressure of <130/80 mm Hg (Table 88). There are few studies regarding blood pressure goals for CVD risk reduction in patients with CKD. Thus, the Work Group elected to extrapolate the recommendations for high-risk patients to patients with CKD. Based on the summary of guidelines in Table 88, the Work Group recommendations to reduce the risk of CVD in CKD are an SBP <130 mm Hg and a DBP <80 mm Hg. In certain select cases, it may be appropriate to maintain a blood pressure higher than the recommended goal of <130/80 mm Hg. These conditions include orthostatic hypotension, postprandial hypotension, autonomic dysfunction, and severe peripheral vascular disease that is exacerbated by a blood pressure less than 130/80 mm Hg. Based on studies of the relationship of SBP and kidney disease outcomes reviewed in Guidelines 8 and 9, the Work Group recommended caution in lowering SBP <110 mm Hg and more frequent monitoring in patients treated with antihypertensive agents and SBP <120 mm Hg. Frequency of monitoring blood pressure in CKD depends on blood pressure level (Weak). Table 90 provides recommendations for frequency of monitoring blood pressure and adjustment of antihypertensive drug regimen, depending on baseline SBP. This protocol has not been studied, but appears reasonable in the opinion of the Work Group. Some classes of antihypertensive agents are "preferred" for reducing CVD risk and progression of CKD (Strong). A "preferred" agent is a class of antihypertensive agent that has a beneficial effect to reduce the risk of CVD or slow the progression of kidney disease by mechanisms in addition to lowering blood pressure. Preferred agents may be indicated for patients with or without hypertension. In patients with hypertension, a preferred agent should be the initial antihypertensive agent to be used for the specific type of CVD or CKD. Table 86 shows preferred agents to reduce the risk of CVD. Guidelines 8, 9, and 10 review preferred agents to slow the progression of kidney disease. For each patient, the clinician should determine if there is an indication for a preferred agent based on the type of CKD, coexisting CVD, and other comorbid conditions, and determine the therapeutic goals for each indication. Table 91 lists CKD and CVD indications for classes of antihypertensive agents. In individuals with more than one indication, treatment decisions should be individualized, based on stratification of risk for progression of CKD, reducing the risk of

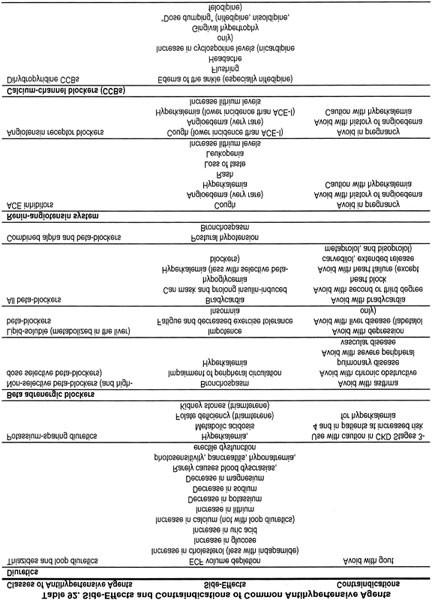
28 CVD, or other outcomes, as discussed in the Background. If there is no preferred agent for a specific type of CKD or CVD or other condition, then antihypertensive therapy is indicated only if blood pressure exceeds the target level. Classes of antihypertensive agents (Strong). This section provides an overview of each of the major classes of antihypertensive agents. Table 91 summarizes the CKD and CVD indications for each class of agents. Table 92 summarizes side-effects and contraindications of classes of antihypertensive agents. Tables 93 through 99 list doses of most common agents in each class. More detailed discussions of ACE inhibitors and ARBs and of diuretics are provided in Guidelines 11 and 12, respectively.
29


30 Diuretics (Table 93). Fluid retention is one of the major causes of hypertension in CKD. Thus, almost all patients with CKD will require the use of a diuretic in order to achieve the blood pressure goal. Three major classes of diuretics can be used to treat hypertension: thiazide, loop, and potassium-sparing diuretics. Aldosterone antagonists are considered separately. Available thiazide diuretics include hydrochlorothiazide and chlorthalidone.
31 Thiazide diuretics have a long history of effectiveness in blood pressure reduction and CVD risk reduction. 5,5a The purpose of ALLHAT was to compare newer antihypertensive agents to thiazide diuretics, as single agents, in controlling blood pressure and preventing clinical CVD events in high-risk patients with hypertension. 107 Altogether, 42,419 patients were randomly assigned to treatment with a thiazide diuretic chlorthalidone, an ACE inhibitor lisinopril, a dihydropyridine calcium-channel blocker amlodipine, or a peripheral alpha blocker doxazosin. Add-on therapy in all groups consisted of beta-blockers, alpha-adrenergic agents, and directly acting vasodilators. The doxazosin arm was stopped early because of an increased risk of nonfatal myocardial infarction. The rates of the primary outcome, coronary heart disease and nonfatal myocardial infarction, were similar among the other treatment arms (Fig 35). Blood pressure control rates were slightly better in patients treated with chlorthalidone (Fig 36), and patients treated with chlorthalidone had lower rates of combined CVD outcomes and heart failure compared to patients treated with lisinopril and lower rates of heart failure compared to patients treated with amlodipine. 107,301 Patients treated with chlorthalidone, especially African- Americans, had lower blood pressure and lower rates of stroke than African-Americans treated with lisinopril. Based on these data, JNC 7 recommends a thiazide-type diuretic as the preferred agent to lower blood pressure and to reduce CVD risk in patients at increased risk of coronary heart disease. Fig 35. Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack (ALLHAT) Trial. Mean systolic and diastolic blood pressure by year during follow-up. Number measured at 6 years for chlorthalidone, amlodipine, and lisinopril are 2,721, 1,656, and 1,551, respectively. Reprinted with permission. 107
32 Fig 36. Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack (ALLHAT) Trial. Cumulative event rates for primary outcome (fatal coronary heart disease or nonfatal myocardial infarction) by treatment group. No significant difference was observed for amlodipine (relative risk [RR], 0.98; 95% confidence interval [CI], 0.90 to 1.07; P = 0.65) or lisinopril (RR, 0.99; 95% CI, 0.91 to 1.09; P = 0.81) versus chlorthalidone with a mean follow-up of 4.9 years. Reprinted with permission. 107 ALLHAT included 7,110 patients (17.6% of the total) with an estimated GFR <60 ml/min/1.73 m 2 at enrollment, which represents a large "CKD subgroup." 302 Analysis of patients with CKD Stage 3 (GFR 30 to 59 ml/min/1.73 m 2 ) assigned to chlorthalidone, lisinopril, or amlodipine (n = 2,492) showed similar findings as in the whole group with respect to CVD. 292 In addition, rates of kidney failure, and substantial decline in estimated GFR did not differ significantly among the three drug classes in the CKD subgroup, including analyses stratified by presence or absence of diabetes. 293 However, the kidney failure event rate was low (approximately 5%), limiting statistical power for determination of the effect on this outcome. ALLHAT differs in some important ways from other studies of antihypertensive agents in CKD. First, the ACE inhibitor and dihydropyridine calcium-channel blocker were prescribed without a diuretic. By contrast, other studies in CKD have compared classes of antihypertensive agents usually prescribed in combination with a diuretic. Second, the risk of kidney failure was lower than observed in other studies in CKD. Third, proteinuria was not measured in ALLHAT, either in baseline or in follow-up. By contrast, most studies in CKD have included patients with proteinuria. Thus, differences between ALLHAT and other studies in CKD may be due to the study design and the type of patient enrolled, rather than true differences in efficacy of combinations of antihypertensive agents used in CKD in slowing progression of kidney disease. Loop diuretics have not been studied in large hypertension trials in the general population; thus, their effectiveness in reducing CVD risk is not known. However, they are effective in reducing ECF volume and have been used in combination with other antihypertensive agents in many studies in CKD. Loop diuretics have a shorter duration of action than thiazide diuretics; hence, they are less effective in patients with normal kidney function, unless they are given in multiple daily doses. 303,304 However, since thiazide diuretics are of minimal effectiveness for ECF volume
33 reduction at low levels of GFR, 305 a loop diuretic is preferred for this purpose in patients with GFR less than 30 ml/min/1.73 m 2. Patients with resistance to loop diuretics may benefit from a combination of a loop diuretic with metolazone, which has a mechanism of action at several sites in the renal tubule. 306 As in patients without CKD, volume depletion may occur from the use of diuretics. Thiazide and loop diuretics increase the delivery of sodium to the distal tubule, thereby increasing urinary potassium excretion. This may be a useful side-effect in CKD, especially in patients treated with an ACE inhibitor or ARB. Nonetheless, hypokalemia can occur, and if not treated appropriately, poses the same potential risks as in patients without CKD. Other sideeffects of thiazide and loop diuretics include hyperuricemia and gout, hyperglycemia, and increased LDL cholesterol. Potassium-sparing diuretics, triamterene and amiloride, are less effective as single agents in reducing ECF volume than thiazide and loop diuretics. They are generally used as an adjunct to thiazide and loop diuretics for prevention and treatment of diuretic-induced hypokalemia and in patients with edematous states. They are generally not used as antihypertensive agents in patients with CKD due to the increased risk of hyperkalemia. Aldosterone antagonists also act as potassium-sparing diuretics and can be used in the same circumstances as triamterene and amiloride. 307 Beta-adrenergic blockers (Table 94). There are several classes of beta-blockers that differ in both clinical benefits and adverse effects. First, beta-blockers can be classified based on their effect on alpha and beta adrenergic receptors. Beta-1 receptors are found mostly in heart muscle. Activation of beta-1 receptors results in an increase in AV nodal conduction, contractility, and heart rate as well as a decrease in AV node refractoriness. Beta-2 receptors are found in bronchial and peripheral vascular smooth muscle in higher numbers than in heart muscle. Activation of beta-2 receptors results primarily in vasodilatation and bronchodilation. Selective beta-blockers are those agents that preferentially block the beta-1 receptor, while nonselective beta-blockers block both the beta-1 and beta-2 receptors. Due to their effect on beta-2 receptors, nonselective beta-blockers can cause bronchoconstriction and worsening of symptoms of severe peripheral vascular disease and can mask signs of hypoglycemia that are sympathetically mediated. These side-effects can also be seen when selective beta-blockers are used in high doses.

34 Beta receptors also stimulate cellular uptake of glucose and potassium. Beta-blockers can cause hyperkalemia due to altered transcellular distribution of potassium. Selective beta-blockers may cause lesser elevation in serum potassium than nonselective beta-blockers. All beta-blockers can cause an increase in serum levels of plasma glucose and triglyceride levels and in insulin resistance and a decrease in HDL cholesterol levels. 308 Some beta-blockers also block the alpha receptor, and they may share some properties with alpha blockers, as described below. Both labetolol and carvedilol block beta receptors nonselectively and also block alpha receptors. Other beta-blockers have intrinsic sympathomimetic activity (ISA), causing activation of the beta-receptor, while also preventing catecholamines from binding to the receptor site. Acebutolol and pindolol have ISA. These agents may be associated with an increased risk of arrhythmias due to beta-receptor stimulation. Second, beta-blockers can be classified by their solubility properties and routes of metabolism. Lipid soluble beta-blockers are eliminated by hepatic metabolism, have a short half-life, and do not require dose adjustment in CKD. However, their metabolism is slowed in heart failure and in the elderly, and they can accumulate causing an increased incidence of side-effects. In addition, they can enter the central nervous system in high concentrations, and are associated with a higher incidence of insomnia, hallucinations, nightmares and depression. Propranolol and metoprolol are examples of lipid soluble beta-blockers. Water-soluble beta-blockers are excreted by the kidney, have a longer half-life, and may accumulate in CKD. They do not readily enter the CNS. Atenolol and sotalol are water soluble. Esmolol has a half life of less than 10 minutes due to rapid metabolism by both hepatic esterases and blood tissue. Beta-blockers were often used in combination with thiazide diuretics in early clinical trials. 5,15 However, without diuretics, the effects have been mixed. 309 In the Medical Research Council trial of middle-aged patients with a diastolic blood pressure between 90 and 109 mm Hg, there

35 was no difference in overall outcome between patients receiving either a thiazide diuretic or propranolol. 310 Carvedilol, extended release metoprolol, and bisprolol are effective agents for the treatment of both essential hypertension and congestive heart failure The results of trials comparing beta-blockers to other agents are discussed in subsequent sections. Thus, beta-blockers are beneficial in patients with a prior history of angina, myocardial infarction, congestive heart failure (due to diastolic dysfunction and for certain agents also for systolic dysfunction), resting tachycardia, migraine headaches, and glaucoma. 15,314,315 Conversely, beta-blockers should in general not be used in patients with bradycardia, second- or third-degree heart block, asthma, chronic obstructive pulmonary disease, severe peripheral vascular disease, or depression, as ß-adrenergic tone is beneficial in these circumstances. 15,316,317 In addition, beta blockade may mask some of the early symptoms of hypoglycemia. Finally, propranolol can interact with a number of other medications, due to metabolism of propranolol by the cytochrome P-450 system and by decreasing hepatic blood flow Other beta-blockers may also be substrates for cytochrome P-450 system interactions. 321 In addition, the abrupt withdrawal of most (and perhaps all beta-blockers) can lead not only to rebound hypertension, but also to worsening angina, myocardial infarction, and even death The mechanism of action is felt to be increased sympathetic activity due to adrenergic receptor upregulation during the period of sympathetic blockade. 325 ACE inhibitors and ARBs (Table 95). ACE inhibitors and ARBs have many potential advantages for patients with CKD and associated comorbid medical conditions. 326 As discussed in Guidelines 8 and 9, they slow the progression of diabetic kidney disease and nondiabetic kidney disease with proteinuria, and in addition, they reduce proteinuria, irrespective of the type of kidney disease. 139,316,
36 There is widespread agreement on the beneficial effect of ACE inhibitors and ARBs in heart failure and in patients with postmyocardial infarction It is suggested that they regress LVH more effectively than other classes of antihypertensive agents. 349 ACE inhibitors and ARBs may have a beneficial effect in preventing heart disease in high-risk patients. In the Captopril Prevention Project (CAPP), patients with a DBP of 100 mm Hg were randomly assigned to either captopril or a beta-blocker (the latter with or without a diuretic). There was no difference between the two groups in regard to the event rate for either fatal or nonfatal myocardial infarction. 350 A subsequent subgroup analysis found that patients with diabetes mellitus, however, had a 40% reduction in the relative risk of all primary endpoints if they were randomized to the captopril group. 351 In the HOPE trial, patients aged >55 years with diabetes and one or more CVD risk factors, or without diabetes but a history of CVD, had improved survival when treated with an ACE inhibitor. 352 These findings are in contrast to ALLHAT, where lisinopril had a higher rate of combined CVD outcomes, stroke, and heart failure compared to patients treated with chlorthalidone. 107 In low-risk patients, the Second Australian National Blood Pressure Study (ANBP2) showed a reduced risk of CVD in patients treated with an ACE inhibitor compared to a diuretic. 352a Beneficial effects in stroke prevention remain controversial. In CAPP, there was a mild increase in the risk of stroke in the group receiving captopril. 350 The Losartan Intervention for Endpoint reduction (LIFE) study randomly assigned patients with markedly elevated blood pressures (SBP of 160 to 200 mm Hg and DBP of 95 to 115 mm Hg) and evidence of LVH on electrocardiogram to either losartan or atenolol therapy. The losartan group had a lower rate of the primary endpoint of cardiovascular death, myocardial infarction, or stroke compared to the atenolol group. 134 This reduction in the primary endpoint was more pronounced in patients with diabetes mellitus. 353 ACE inhibitors and ARBs have fewer metabolic side-effects than diuretics and beta-blockers. They do not cause ECF volume depletion or changes in serum cholesterol, triglyceride, or plasma glucose levels. 354 However, they have other side-effects that limit their use. They cannot be used in pregnant women due to risks to the fetus. 355 ACE inhibitors can cause a dry cough or angioedema due to inhibition of converstion of bradykinin to inactive metabolites. ARBs have a decreased incidence of cough and can be used in patients who do not tolerate an ACE inhibitor because of cough. Both ACE inhibitors and ARBs can cause hyperkalemia and mild decrease in GFR in CKD. The uses and side-effects of ARBs are discussed in more detail in Guideline 11. Calcium-channel blockers (Table 96). The calcium-channel blockers can be subdivided into dihydropyridine and nondihydropyridine agents. The dihydropyridines preferentially block L- type calcium channels. They are potent vasodilators with little or no effect on cardiac contractility or cardiac conduction. The nondihydropyridines include verapamil, a cardiac depressant, and diltiazem, which has both mild vasodilator and cardiac depressant activity. In general, calcium-channel blockers are of particular benefit in patients with angina pectoris, recurrent supraventricular tachycardia (verapamil only), Raynaud s phenomenon (dihydropyridines only), congestive heart failure due to diastolic dysfunction, migraine headaches, and esophageal spasm. 356 Neither class causes an increase in cholesterol or triglyceride levels or in insulin resistance. 308

37 The nondihydropyridine calcium-channel blockers have beneficial effects on CKD and CVD. As discussed in Guidelines 8 and 9, diltiazem and verapamil are effective in decreasing proteinuria in diabetic kidney disease. 337, In addition, the combination of lisinopril and verapamil resulted in a greater reduction in proteinuria than using either drug at twice the dose used in combination therapy. 358 Similar findings were seen with a combination of trandolapril and verapamil. 360 A nonsignificant effect of ve rapamil on mortality was seen in the Danish Ve rapamil Infarction Trial II (DAVIT II) study in patients after myocardial infarction without a history of congestive heart failure. 361 In two studies, CONVINCE 362a and INVEST, 362 including more than 38,000 hypertensive patients, CVD mortality was similar in the calcium-channel blocker and beta-blocker arms. In the Multicenter Diltiazem Post Infarction Trial Research group study, post-mi patients randomized to diltiazem (versus placebo) showed a nonsignificant trend for lower mortality in patients who did not have evidence of pulmonary congestion on chest x- ray. Conversely, there was an excess of deaths in diltiazem-treated patients with pulmonary congestion. 363 In the Nordic Diltiazem (NORDIL) trial, more than 10,000 patients with diastolic blood pressure greater than 100 mm Hg were randomly assigned to either diltiazem or standard therapy, consisting of a diuretic, a beta-blocker, or both agents. There was no difference in the rate of the primary combined endpoint of stroke, myocardial infarction, or other cardiovascular death between the two randomized groups. Secondary analyses suggested, however, that the rate for stroke alone was less in the diltiazem group than in the beta-blocker and/or diuretic group. 364 Nondihydropyridine calcium-channel blockers can diminish cardiac contractility and slow cardiac conduction. 356 Therefore, these agents should not be used in patients with severe left ventricular dysfunction, sick sinus syndrome, or second- or third-degree heart block. 365 In addition, constipation can be seen in up to 25% of patients prescribed verapamil. 356 In ALLHAT, patients treated with amlodipine had a higher rate of heart failure compared to patients treated with chlorthalidone. 107 In addition, in the Appropriate Blood Pressure Control in Diabetes (ABCD) trial, hypertensive diabetic patients who were treated with nisoldipine had a higher risk of fatal and nonfatal myocardial infarction compared to patients treated with enalapril. 366 In the Intervention as a Goal in Hypertension Treatment (INSIGHT) study, patients
38 with hypertension and at least one other cardiovascular risk factor were randomized to either amiloride with hydrochlorothiazide versus nifedipine Gastrointestinal Therapeutic System (GITS). There was no difference in the primary outcome of cardiovascular death, myocardial infarction, heart failure, or stroke between the two randomized groups. However, there was an increase in the rates of fatal myocardial infarction and nonfatal heart failure in the group receiving nifedipine GITS. 367 Finally, in the Fosinopril Amlodipine Cardiovascular Events Trial (FACET) trial, patients prescribed amlopidine had increased cardiovascular complications compared to patients prescribed fosinopril. 368 In contrast, the Syst-Eur 369 and Syst-China 370 studies showed a decrease in both fatal and nonfatal coronary events in patients prescribed nitrendipine. In the Hypertension Optimal Treatment (HOT) trial, a lower coronary event rate was seen in patients prescribed a higher dose of felodipine. 371 Overall, controlled trial results are not altogether consistent, but it appears that dihydropyridine calcium-channel blockers, in association with a diuretic, are effective in lowering blood pressure and reducing CVD risk, but are less effective in the absence of a diuretic. There are a number of dihydropyridine agents. Some have cardiac depressant activity, such as short-acting nifedipine, and longer-acting felodipine, isradipine, nicardipine, nisoldipine, and long-acting nifedipine. Long-acting agents that do not have cardiac depressant effects include amlodipine and lacidipine. In general, longer acting agents without cardiac depressant effects are preferred. The dihydropyridines are associated with a number of other side-effects due to direct vasodilatation and can cause peripheral edema, dizziness, headache, and flushing. 356 In one study there was less edema when dihydropyridines were used in combination with ACE inhibitors compared to use of dihydropyridines alone. 372 Alpha-adrenergic agents (Table 97). Both centrally acting sympatholytic agents (methyldopa, clonidine, guanfacine and guanabenz) and selective a-1 blockers have beneficial effects on lipid metabolism (increase HDL cholesterol levels and decrease LDL cholesterol levels) and improve insulin sensitivity. In general, these agents should not be used as a first-line therapy for hypertension due to the relatively high incidence of side-effects. Side-effects of the centrally acting agents include dry mouth, sedation, and sexual dysfunction 373 and for clonidine, sideeffects are rebound hypertension after sudden discontinuation of therapy 325 and sometimes even with gradual withdrawal of therapy. 374,375 Side-effects of the selective a-1 blockers include headache, weakness, dizziness, and on rare occasions syncope. Dizziness and syncope can be minimized by starting with a low dose of a long-acting agent such as doxazosin and administering the initial dose at bedtime. 376 The selective a-1 blockers may be of benefit in men with symptomatic benign prostatic hyperplasia. This benefit is balanced by the observation in ALLHAT that the use of doxazosin increased the risk of developing congestive heart failure compared to patients treated with the diuretic chlorthalidone. 377


39 Peripheral vasodilators (Table 98). Minoxidil is a powerful vasodilator that can cause lower extremity edema, tachycardia, hirsutism, and in rare cases pleural or pericardial effusions, at therapeutic doses. 378 The incidence of pericardial effusion in CKD patients is higher than that seen in the general population This agent is almost always used in combination with a beta-blocker and loop diuretic in order to minimize reflex tachycardia and lower extremity edema. In one controlled trial of captopril versus minoxidil, improvement in blood pressure in the captopril group resulted in regression of LVH at 6 months while regression did not occur in the minoxidil-treated group. 382 Therefore, minoxidil should be reserved for those patients who cannot obtain blood pressure control with the preferred agent and at least two of the other recommended agents. Aldosterone antagonists (Table 99). Aldosterone plays a role in numerous cardiovascular effects, such as LVH, CHF, and vascular fibrosis, necrosis, and inflammation. Aldosterone receptor antagonists can be classified as "selective" (blocking the mineralocorticoid receptor) or "nonselective" (blocking the glucocorticoid, progesterone, and androgen receptors as well as mineralocorticoid receptors). Recently, aldosterone receptor antagonists have been identified as a treatment for congestive heart failure. In the Randomized Aldactone Evaluation Study (RALES), patients receiving the nonselective agent spironolactone compared to those receiving placebo had a reduction in mortality of 30%. 383 Small doses of spironolactone resulted in an improvement in ventricular function and enhanced exercise tolerance. In the Eplerenone Post Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS), patients with a left ventricular ejection fraction of 40% or lower and symptoms of heart failure were randomly assigned to receive the selective agent eplerenone an average of 7 days after they had had a myocardial infarction or placebo. 384 During a mean follow-up of 16 months, the relative risk of death was reduced by 15% among patients receiving eplerenone and the risk of hospitalization for heart failure was reduced by 15% with eplerenone. 385 There was a significantly greater increase in the serum creatinine concentration in the eplerenone group than in the placebo group, however, and

40 hyperkalemia occurred in 5.5% of patients in the eplerenone group, as compared with 3.9% of patients in the placebo group. However, the study included only patients with CKD Stages 1-2. Side-effects are likely to be more frequent in CKD Stages 3-5. Guidelines from the American Heart Association and the American College of Cardiology recommend considering low-dose spironolactone in patients with recent or current symptoms of systolic heart failure at rest despite the use of digoxin, diuretics, an ACE inhibitor, and a betablocker. 300 These guidelines urge caution in prescribing spironolactone to patients with baseline elevations of either serum potassium or creatinine. In animal models, it appears that aldosterone receptor antagonists reduce proteinuria, nephrosclerosis, and glomerulosclerosis; however, clinical trials using these agents in patients with CKD have only recently been initiated. 386 Thus, caution should be used when these agents are prescribed in patients with CKD. Initiation and selection of antihypertensive agents in CKD (Moderately Strong). The algorithm in Fig 34 illustrates decision-making in initiation and selection of antihypertensive agents in CKD. Initiation of therapy and dose-escalation with preferred agents. In patients not previously treated with antihypertensive agents, an agent from the preferred class for CKD is the first agent to be used (generally on ACE inhibitor or ARB). In patients already treated for CKD with other antihypertensive agents or other medications that lower blood pressure, an agent from the preferred class should be added to the regimen. Other agents may need to be reduced in dosage or discontinued in order to add the preferred agent. In patients already treated with an agent from the preferred class, consideration should be given to increasing the dosage. This may require reduction in dosage or discontinuation of other agents.. Monitoring the response to preferred agents. After the initiation of therapy, patients should be monitored for effects on blood pressure, for kidney function, and for agent-specific side-effects. Detailed protocols for monitoring response to ACE inhibitors and ARBs and to diuretics are given in Guidelines 11 and 12, respectively. An often-used "rule of thumb" is that addition of a

41 new antihypertensive agent in appropriate dosage lowers systolic blood pressure by approximately 10 mm Hg. If blood pressure does not decline, then the clinician should consider nonadherence to medications or the use of medications that can raise blood pressure. A list of strategies to improve adherence is shown in Table 100, and a list of medications that can raise blood pressure is shown in Table 101. After exclusion or correction of these causes, the dose of the preferred agent should be increased. Dosage should not be escalated more frequently than every 4 weeks. If the response to the preferred agent does not achieve the desired blood pressure response, then a diuretic is usually added as the second agent, and the dose is increased until the patient is euvolemic, target blood pressure is achieved, adverse effects are noted, or a high dose has been reached. A diuretic should be considered in patients for whom a single agent does not achieve blood pressure target even if there is no evidence on physical examination of volume overload. Thiazide diuretics are preferred in patients with GFR 30 ml/min/1.73 m 2 because of their longer duration of action. Loop diuretics are preferred in patients with GFR <30 ml/min/1.73 m 2, but may need to be given twice daily to achieve the desired natriuresis. Higher doses of loop diuretics are required in patients with lower GFR. Potassium-sparing diuretics should be avoided in patients with GFR <30 ml/min/1.73 m 2 and in patients taking ACE inhibitors or ARBs. See Guideline 12 for a more detailed discussion on the use of diuretics in CKD. Addition of other agents. Additional agents are selected based on CVD-specific indications to achieve therapeutic and preventive targets, and on avoidance of drug interactions or known sideeffects (Table 86). Many patients with CKD, especially those with a GFR <30 ml/min/1.73 m 2, require three or four antihypertensive agents in order to reach the desired blood pressure goals. 387 Some antihypertensive agents have adverse interactions and should be used in combination with caution (Table 102). In addition, there are also a few specific instances where a combination of specific antihypertensive agents has been shown to be beneficial in specific patient populations. Additional antihypertensive agents should be started one at a time, at the lowest recommended dose, then escalated at intervals of 4 to 8 weeks until either the desired blood pressure goal is achieved, a high dose is reached, or a side-effect occurs.
42 The antihypertensive regimen should be simplified as much as possible (Moderate). Patients have been shown to have a lower rate of compliance with medications prescribed once per day compared to medications prescribed more than once per day. In addition, antihypertensive medications that have a half-life of greater than 24 hours are more likely to sustain a significant and sustained decrease in blood pressure over a 24-hour period compared to antihypertensive medications with a half-life of less than 24 hours. In patients who are at least 20 mm Hg above their goal blood pressure, it is unlikely that a single agent will be effective in reaching the target blood pressure, even at maximal dosages. In these situations, it may be beneficial to initiate therapy with two agents either as separate prescriptions or as a fixed-dose combination containing a preferred agent as initial therapy. 5,5a For patients with GFR >30 ml/min/1.73 m 2, a preferred agent in combination with a thiazide diuretic is often an appropriate choice. After therapeutic goals are reached, it may be more convenient to change to a fixed-dose, oncedaily combination of antihypertensive agents. Pharmaceutical companies produce a variety of combination antihypertensive agents. These combinations can be used to simplify the antihypertensive regimen and are shown in Table 103.

43 LIMITATIONS There are few studies on the treatment of hypertension in CKD. Most of the largest clinical studies in patients with CKD were designed to evaluate the efficacy of therapy in slowing the progression of CKD rather than reducing risk of CVD. Therefore, most of the recommendations in Guideline 7 are extrapolated from clinical studies performed in the general population. IMPLEMENTATION ISSUES Data from NHANES III document the low rate of control of hypertension in CKD (Figs 3, 4, and 5). The problem of attaining high rates of adherence to antihypertensive therapy for CKD is similar in many ways to that in the general population, in which careful studies report adherence
AFFORDABLE TECHNOLOGY
 World Health Organization AFFORDABLE TECHNOLOGY BLOOD PRESSURE MEASURING DEVICES FOR LOW RESOURCE SETTINGS CARDIOVASCULAR DISEASES Blood Pressure Measurement in Low Resource Settings Annex 1: Blood Pressure
World Health Organization AFFORDABLE TECHNOLOGY BLOOD PRESSURE MEASURING DEVICES FOR LOW RESOURCE SETTINGS CARDIOVASCULAR DISEASES Blood Pressure Measurement in Low Resource Settings Annex 1: Blood Pressure
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care
 Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
Quality ID #122: Adult Kidney Disease: Blood Pressure Management National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION*
 Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE
 GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Professor Medicine and Cardiovascular Diseases Director, Seinsheimer Cardiovascular Health
GETTING THE NUMBERS RIGHT: ACCURATE MEASUREMENT OF BLOOD PRESSURE Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Professor Medicine and Cardiovascular Diseases Director, Seinsheimer Cardiovascular Health
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right. Anthony J. Viera, MD, MPH, FAHA Professor and Chair
 Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Blood Pressure Competency Training
 Blood Pressure Competency Training WORKBOOK Table of Contents 3..... Introduction 4..... Background 6..... Equipment Accurate blood pressure What impacts a patient s blood pressure Strategies for proper
Blood Pressure Competency Training WORKBOOK Table of Contents 3..... Introduction 4..... Background 6..... Equipment Accurate blood pressure What impacts a patient s blood pressure Strategies for proper
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
Clinical Medical Policy Department Clinical Affairs Division DESCRIPTION
 Ambulatory Blood Pressure Monitoring (ABPM) [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr. go to Comunicados a Proveedores, and click Cartas Circulares.]
Ambulatory Blood Pressure Monitoring (ABPM) [For the list of services and procedures that need preauthorization, please refer to www.mcs.com.pr. go to Comunicados a Proveedores, and click Cartas Circulares.]
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK. Michael Smolensky, Ph.D. The University of Texas Austin & Houston
 AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences
Module 3.2. Management of hypertension at primary health care
 Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Summary of recommendations
 Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
Summary of recommendations Measuring blood pressure (BP) Use the recommended technique at every BP reading to ensure accurate measurements and avoid common errs. Pay particular attention to the following:
The measurement of blood pressure and hypertension. Handout Fenyvesi Tamás III.Department of Medicine
 The measurement of blood pressure and hypertension Handout Fenyvesi Tamás III.Department of Medicine 1 2 History of the blood pressure measurement direct Stephen HALES 1726 horse carotid indirect Riva-Rocci
The measurement of blood pressure and hypertension Handout Fenyvesi Tamás III.Department of Medicine 1 2 History of the blood pressure measurement direct Stephen HALES 1726 horse carotid indirect Riva-Rocci
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Data Collection Worksheet
 Data Collection Worksheet 1. Has a doctor or nurse ever said that you have: High blood pressure or hypertension? [ ] No [ ] Yes [ ] Not Sure 1.a. If Yes, then at what age were you first told this? Age
Data Collection Worksheet 1. Has a doctor or nurse ever said that you have: High blood pressure or hypertension? [ ] No [ ] Yes [ ] Not Sure 1.a. If Yes, then at what age were you first told this? Age
Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations
 Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls
 Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE. MEASURING BLOOD PRESSURE - MANUAL (equ04)
") SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: MEASURING BLOOD PRESSURE - MANUAL Nursing DATE: REVIEWED: PAGES: 2/80 7/17 1 of 5 RESPONSIBILITY: RN, LPN, Patient Care Technician Multi-skilled
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: MEASURING BLOOD PRESSURE - MANUAL Nursing DATE: REVIEWED: PAGES: 2/80 7/17 1 of 5 RESPONSIBILITY: RN, LPN, Patient Care Technician Multi-skilled
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Thesis for doctoral degree (Ph.D.) 2008 ROLE OF AMBULATORY BLOOD PRESSURE MONITORING AFTER PEDIATRIC RENAL TRANSPLANTATION Rafael Tomás Krmar
 2008 ROLE OF AMBULATORY BLOOD PRESSURE MONITORING AFTER PEDIATRIC RENAL TRANSPLANTATION Rafael Tomás Krmar") Thesis for doctoral degree (Ph.D.) 2008 Thesis for doctoral degree (Ph.D.) 2008 ROLE OF AMBULATORY BLOOD PRESSURE MONITORING AFTER PEDIATRIC RENAL TRANSPLANTATION Rafael Tomás Krmar ROLE OF AMBULATORY
Thesis for doctoral degree (Ph.D.) 2008 Thesis for doctoral degree (Ph.D.) 2008 ROLE OF AMBULATORY BLOOD PRESSURE MONITORING AFTER PEDIATRIC RENAL TRANSPLANTATION Rafael Tomás Krmar ROLE OF AMBULATORY
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Importance of Ambulatory Blood Pressure Monitoring in Adolescents
 Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Importance of Ambulatory Blood Pressure Monitoring in Adolescents Josep Redon, MD, PhD, FAHA Internal Medicine Hospital Clinico Universitario de Valencia University of Valencia CIBERObn Instituto de Salud
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Comparison of arbitrary definitions of circadian time periods with those determined by wrist actigraphy in analysis of ABPM data
 Journal of Human Hypertension (1999) 13, 449 453 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Comparison of arbitrary definitions of
Journal of Human Hypertension (1999) 13, 449 453 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Comparison of arbitrary definitions of
External Oscillatory Blood Pressure - EOBPTM
 External Oscillatory Blood Pressure - EOBPTM Development of Novel Principle To Measure Blood Pressure Mindaugas Pranevicius, M.D., Osvaldas Pranevicius, M.D., Ph.D. Pranevicius Biotech Inc., Forest Hills,
External Oscillatory Blood Pressure - EOBPTM Development of Novel Principle To Measure Blood Pressure Mindaugas Pranevicius, M.D., Osvaldas Pranevicius, M.D., Ph.D. Pranevicius Biotech Inc., Forest Hills,
Vital Signs. Vital Signs. Pulse. Temperature. Respiration. Blood Pressure
 Vital Signs Jarvis, Chapter 9 Vital Signs Classic Vital Signs TPR/BP Temperature Pulse Respirations Blood Pressure Additional Vital Signs Height Weight BMI (Kg/m2) or (702Xlbs/in2) Supine, orthostatic
Vital Signs Jarvis, Chapter 9 Vital Signs Classic Vital Signs TPR/BP Temperature Pulse Respirations Blood Pressure Additional Vital Signs Height Weight BMI (Kg/m2) or (702Xlbs/in2) Supine, orthostatic
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Chapter 08. Health Screening and Risk Classification
 Chapter 08 Health Screening and Risk Classification Preliminary Health Screening and Risk Classification Protocol: 1) Conduct a Preliminary Health Evaluation 2) Determine Health /Disease Risks 3) Determine
Chapter 08 Health Screening and Risk Classification Preliminary Health Screening and Risk Classification Protocol: 1) Conduct a Preliminary Health Evaluation 2) Determine Health /Disease Risks 3) Determine
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
STATE OF THE ART BP ASSESSMENT
 STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
KDIGO Controversies Conference on Blood Pressure in CKD
 KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
KDIGO Controversies Conference on Blood Pressure in CKD September 7-10, 2017 Edinburgh, Scotland Kidney Disease: Improving Global Outcomes (KDIGO) is an international organization whose mission is to improve
Taking and recording blood pressure and pulse. City Gate Training Centre all rights reserved
 Taking and recording blood pressure and pulse City Gate Training Centre all rights reserved Course Content: Definition of Blood Pressure Normal Blood Pressure Readings Systolic and Diastolic Blood Pressure
Taking and recording blood pressure and pulse City Gate Training Centre all rights reserved Course Content: Definition of Blood Pressure Normal Blood Pressure Readings Systolic and Diastolic Blood Pressure
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
ESSENTIAL HYPERTENSION
 E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Recommendations for Blood Pressure Measurement in Humans and Experimental Ani...
 Recommendations for Blood Pressure Measurement in Humans and Experimental Ani... Página 1 de 41 Published online before print December 20, 2004, doi:10.1161/01.hyp.0000150859.47929.8e (Hypertension. 2005;45:142.)
Recommendations for Blood Pressure Measurement in Humans and Experimental Ani... Página 1 de 41 Published online before print December 20, 2004, doi:10.1161/01.hyp.0000150859.47929.8e (Hypertension. 2005;45:142.)
Section 03: Pre Exercise Evaluations and Risk Factor Assessment
 Section 03: Pre Exercise Evaluations and Risk Factor Assessment ACSM Guidelines: Chapter 3 Pre Exercise Evaluations ACSM Manual: Chapter 3 Risk Factor Assessments HPHE 4450 Dr. Cheatham Purpose The extent
Section 03: Pre Exercise Evaluations and Risk Factor Assessment ACSM Guidelines: Chapter 3 Pre Exercise Evaluations ACSM Manual: Chapter 3 Risk Factor Assessments HPHE 4450 Dr. Cheatham Purpose The extent
Strategies for Managing Hypertension
 Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
Strategies for Managing Hypertension by Marsha K. Millonig, MBA, RPh President,Catalyst Enterprises, LLC E.L.F. Publications, Inc. is accredited by the Accreditation Council for Pharmacy Education as a
APPENDIX 1: METHODS USED FOR GUIDELINE DEVELOPMENT
 APPENDIX 1: METHODS USED FOR GUIDELINE DEVELOPMENT AIMS THE OVERALL AIM of the project was to develop evidence-based recommendations for blood pressure management in individuals with CKD. The Work Group
APPENDIX 1: METHODS USED FOR GUIDELINE DEVELOPMENT AIMS THE OVERALL AIM of the project was to develop evidence-based recommendations for blood pressure management in individuals with CKD. The Work Group
LEARNING OUTCOME The students will be able to elicit vital signs correctly on human volunteers/patients
 Vital signs (pulse, blood pressure, temperature, respiratory rate, pain) are physiological parameters that a healthcare professional requires when dealing with patients. Accurate measurement of vital signs
Vital signs (pulse, blood pressure, temperature, respiratory rate, pain) are physiological parameters that a healthcare professional requires when dealing with patients. Accurate measurement of vital signs
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
PLANK 1 Direct Care Staff Trained in Accurate BP Measurement
 Direct Care Staff Trained in Accurate BP Measurement 1. 2. 3. 5. 22 to 26 cm Small adult (12X22 cm) 27 to 34 cm Adult (16X30 cm) 35 to 44 cm Large adult (16X36 cm) 45 to 52 cm Adult thigh (16X42 cm) widths
Direct Care Staff Trained in Accurate BP Measurement 1. 2. 3. 5. 22 to 26 cm Small adult (12X22 cm) 27 to 34 cm Adult (16X30 cm) 35 to 44 cm Large adult (16X36 cm) 45 to 52 cm Adult thigh (16X42 cm) widths
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
BLOOD PRESSURE ASSESSMENT
 BLOOD PRESSURE ASSESSMENT Course Principles of Health Science Unit X Vital Signs Course Health Science Unit VI CPR / AED & First Aid Essential Question How do health care skills help to promote health
BLOOD PRESSURE ASSESSMENT Course Principles of Health Science Unit X Vital Signs Course Health Science Unit VI CPR / AED & First Aid Essential Question How do health care skills help to promote health
High Blood Pressure Blood Pressure Monitoring at Home -- F...
 Return to Web version High Blood Pressure Blood Pressure Monitoring at Home Why should I measure my blood pressure at home and keep a record of it? Measuring your blood pressure at home and keeping a record
Return to Web version High Blood Pressure Blood Pressure Monitoring at Home Why should I measure my blood pressure at home and keep a record of it? Measuring your blood pressure at home and keeping a record
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
OHTAC Recommendation: Twenty-Four-Hour Ambulatory Blood Pressure Monitoring in Hypertension. Ontario Health Technology Advisory Committee
 OHTAC Recommendation: Twenty-Four-Hour Ambulatory Blood Pressure Monitoring in Hypertension Ontario Health Technology Advisory Committee May 2012 Background Hypertension in Canada Hypertension occurs when
OHTAC Recommendation: Twenty-Four-Hour Ambulatory Blood Pressure Monitoring in Hypertension Ontario Health Technology Advisory Committee May 2012 Background Hypertension in Canada Hypertension occurs when
Hypertension: Management of hypertension in adults in primary care
 Hypertension: Management of hypertension in adults in primary care NICE guideline Second draft for consultation, February 2004 If you wish to comment on the recommendations, please make your comments on
Hypertension: Management of hypertension in adults in primary care NICE guideline Second draft for consultation, February 2004 If you wish to comment on the recommendations, please make your comments on
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
2020 HYPERTENSION HIGHLIGHTS
 2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
2020 HYPERTENSION HIGHLIGHTS A Practical Guide informed by the Hypertension Canada Guidelines for the Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension BLOOD PRESSURE MEASUREMENT TECHNIQUE
Hypertension Clinical Practice Guidelines
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Hypertension Clinical Practice Guidelines September 2016 Approved by Board Chair Signature Name (Please
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Hypertension Clinical Practice Guidelines September 2016 Approved by Board Chair Signature Name (Please
ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY. Introduction. Patients and Methods
 Vol. 2, Issue 1, pages 31-36 ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY By Alejandro de la Sierra, MD Luis M. Ruilope, MD Hypertension Units, Hospital Clinico, Barcelona & Hospital 12 de Octubre,
Vol. 2, Issue 1, pages 31-36 ORIGINAL ARTICLE AMBULATORY BLOOD PRESSURE IN OBESITY By Alejandro de la Sierra, MD Luis M. Ruilope, MD Hypertension Units, Hospital Clinico, Barcelona & Hospital 12 de Octubre,
Effective Health Care Program
 Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
Comparative Effectiveness Review Number 37 Effective Health Care Program Chronic Kidney Disease Stages 1 3: Screening, Monitoring, and Treatment Executive Summary Objectives This systematic review evaluates
Knowledge and implementation of the JNC VII guidelines for treatment of hypertension in the elderly by health care practitioners in northwest Ohio
 The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Knowledge and implementation of the JNC VII guidelines for treatment of hypertension in the elderly by
The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Knowledge and implementation of the JNC VII guidelines for treatment of hypertension in the elderly by
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
SECTION 16: BLOOD PRESSURE MEASUREMENT
 CHRONIC KIDNEY DISEASE IN CHILDREN COHORT STUDY SECTION 16: BLOOD PRESSURE MEASUREMENT 16.1 OVERVIEW OF BLOOD PRESSURE MEASUREMENT This section describes the procedures that are to be performed to obtain
CHRONIC KIDNEY DISEASE IN CHILDREN COHORT STUDY SECTION 16: BLOOD PRESSURE MEASUREMENT 16.1 OVERVIEW OF BLOOD PRESSURE MEASUREMENT This section describes the procedures that are to be performed to obtain
Blood Pressure Protocol Training
 Blood Pressure Protocol Training May 31, 2018 Pat Spier, RN-BC, PCMH-CCE Barb Rice, RN-BC BCBS of North Dakota Fargo, ND 2013 Template and icons provided by The Advisory Board Company. Hypertension Education
Blood Pressure Protocol Training May 31, 2018 Pat Spier, RN-BC, PCMH-CCE Barb Rice, RN-BC BCBS of North Dakota Fargo, ND 2013 Template and icons provided by The Advisory Board Company. Hypertension Education
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN?
 BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
Dual-Cuff Method Improves Accuracy of Blood Pressure and Hemodynamics Determination
 Dual-Cuff Method Improves Accuracy of Blood Pressure and Hemodynamics Determination JIRI JILEK 1, MILAN STORK 2 1 Carditech, Culver City, California, USA jilekj@usa.net 2 Dept. of Applied Electronics and
Dual-Cuff Method Improves Accuracy of Blood Pressure and Hemodynamics Determination JIRI JILEK 1, MILAN STORK 2 1 Carditech, Culver City, California, USA jilekj@usa.net 2 Dept. of Applied Electronics and
가정혈압의활용 CARDIOVASCULAR CENTER. Wook Bum Pyun M.D., Ph.D. HOME BLOOD PRESSURE MONITORING. Ewha Womans University, school of Medicine
 가정혈압의활용 HOME BLOOD PRESSURE MONITORING CARDIOVASCULAR CENTER Wook Bum Pyun M.D., Ph.D. pwb423@ewha.ac.kr Ewha Womans University, school of Medicine Non-Invasive Blood Pressure Measurement 5-20% Resistant
가정혈압의활용 HOME BLOOD PRESSURE MONITORING CARDIOVASCULAR CENTER Wook Bum Pyun M.D., Ph.D. pwb423@ewha.ac.kr Ewha Womans University, school of Medicine Non-Invasive Blood Pressure Measurement 5-20% Resistant
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
and bias, which are known to be present in self-home and in professional office BP measurements taken using the auscultatory technique [7].
![and bias, which are known to be present in self-home and in professional office BP measurements taken using the auscultatory technique [7].](/thumbs/86/94636218.jpg "and bias, which are known to be present in self-home and in professional office BP measurements taken using the auscultatory technique [7].") Devices and technology 37 Validation of the A&D UM-11 professional hybrid device for office blood pressure measurement according to the International Protocol George S. Stergiou, Periklis P. Giovas, Charilaos
Devices and technology 37 Validation of the A&D UM-11 professional hybrid device for office blood pressure measurement according to the International Protocol George S. Stergiou, Periklis P. Giovas, Charilaos
Importance Of Taking Manual Blood Pressure In Both Arms
 Importance Of Taking Manual Blood Pressure In Both Arms Its importance to health is now well-recognised, in that high blood pressure can lead to Have a look at our slide show on how to take a blood pressure
Importance Of Taking Manual Blood Pressure In Both Arms Its importance to health is now well-recognised, in that high blood pressure can lead to Have a look at our slide show on how to take a blood pressure
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Interested parties (organisations or individuals) that commented on the draft document as released for consultation.
 that commented on the draft document as released for consultation.") 23 June 2016 EMA/CHMP/345847/2015 Committee for Medicinal products for Human Use Overview of comments received on ''Guideline on clinical investigation of medicinal products in the treatment of hypertension'
23 June 2016 EMA/CHMP/345847/2015 Committee for Medicinal products for Human Use Overview of comments received on ''Guideline on clinical investigation of medicinal products in the treatment of hypertension'
2. Measure a subject's blood pressure and heart rate both at rest and during exercise.
 Lab Activity 11 The Cardiovascular System Student Learning Objectives After completing this lab, you should be able to: 1. Define, explain and correctly use the key terms. 2. Measure a subject's blood
Lab Activity 11 The Cardiovascular System Student Learning Objectives After completing this lab, you should be able to: 1. Define, explain and correctly use the key terms. 2. Measure a subject's blood
Impact of Recent Hypertension Guidelines on Clinical Practice
 C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Techniques of Vital Signs. John Gazewood, MD, MSPH Department of Family Medicine
 Techniques of Vital Signs John Gazewood, MD, MSPH Department of Family Medicine Objectives Define normal in several ways. Describe correct technique of measuring vital signs. Describe correct technique
Techniques of Vital Signs John Gazewood, MD, MSPH Department of Family Medicine Objectives Define normal in several ways. Describe correct technique of measuring vital signs. Describe correct technique