Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
|
|
|
- Collin Hampton
- 6 years ago
- Views:
Transcription
1 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
2 Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical Care Assistant Professor Yale School of Medicine New Haven, CT
3 Disclosure I have no conflicts of interest to disclose
4 Evidence Outline Learning objectives ARDS Background Diagnosis & Treatment Pulmonary edema Background Diagnosis & Treatment Summary
5 Learning Objectives Define Acute Respiratory Distress Syndrome (ARDS) Identify causes of ARDS and pulmonary edema Understand diagnostic evaluation and treatment options
6 ARDS: Background
7 Case Scenario
8 35yo G1P0 IVF twin gestation EGA 26w admitted for worsening PNA. Increasing O2 requirement despite appropriate culture guided antibiotic therapy. BMI 38 kg/ m2. What must you be suspicious of? Drug resistant organism Poor med compliance Undiagnosed infection ARDS
9 ARDS: Background Berlin Definition (2012 task force): Respiratory failure not explained by cardiac failure or fluid overload Occurs within one week of known insult or new/ worsening respiratory symptoms Unexplained bilateral opacities (CXR or CT) Three severity categories based on PaO2/ FIO2 ratio
10 ARDS: Background 60-day mortality rate: 22% ARDS Network trials: NIH Heart, Lung and Blood Institute Responsible for up to 19% obstetric ICU admissions
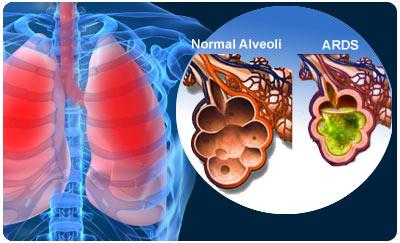
11 ARDS: Pathophysiology Alveolar lung injury causes diffuse alveolar damage Release of pro-inflammatory cytokines Tumor necrosis factor (TNF), interleukin (IL)-1, IL-6, IL-8 Neutrophil recruitment Subsequent damage to capillary endothelium and alveolar epithelium
12 ARDS: Pathophysiology Protein escapes from vascular space, then oncotic gradient is lost, then air spaces contain proteinaceous fluid and debris Loss of surfactant ARDS effects Impairment of gas exchange Decreased lung compliance Increased pulmonary arterial pressure
13 What was/were her risk factor(s)? Multiple gestation AMA Pneumonia IVF Obesity
14 ARDS: Causes More than 60 attributable causes identified Sepsis most common etiology Aspiration One-third of hospitalized that have aspirated Pneumonia Community-acquired pneumonia most common cause outside of hospital Massive transfusion, >15 units red cells Transfusion-related acute lung injury Severe trauma Other: obesity, pancreatitis, contrast, drugs
15 ARDS: Causes Unique to pregnancy Preeclampsia/ eclampsia Tocolytic-induced pulmonary edema Chorioamnionitis Amniotic fluid embolism Placental abruption Obstetric hemorrhage and resuscitation Endometritis Retained products of conception Septic abortion

16 ARDS: Stages Exudative stage Day 1 to day 7-10 Alveolar damage
17 ARDS: Stages Proliferative phase Resolution of pulmonary edema Proliferation of type II alveolar cells Fibrotic stage Obliteration of normal lung architecture Diffuse fibrosis Cyst formation
18 ARDS: Diagnosis & Treatment
19 ARDS: Diagnosis Hypoxemia appears within 6 to 72 hours of inciting event Dyspnea, cyanosis, and diffuse crackles Rapid progression Diagnosis ARDS versus cardiogenic pulmonary edema Physical exam Brain natriuretic peptide (BNP), < 100 pg/ml Echocardiogram may be helpful

20 ARDS Chest X-ray
21 35yo G1P0 IVF twin gestation EGA 26w admitted for worsening PNA. Increasing O2 requirement despite appropriate culture guided antibiotic therapy. BMI 38 kg/ m2. Nonproductive cough. T 99F HR 120 RR 32 BP 110/60 90% (4L) What is your next intervention? Broaden antibiotic coverage and wait for response Oxygen supplementation via nonrebreather facemask Rapid Response Team activation Transfer to ICU and intubate
22 ARDS: Treatment Supplemental oxygen High flow oxygen, 70% via facemask ARDS usually requires higher concentration Mechanical ventilation
23 ARDS: Treatment Mechanical Ventilation Low tidal volume ventilation V T 4 to 6 ml/kg predicted body weight (PBW) Plateau pressure < 30 cmh 2 O RR titrated to maintain ph Appropriate fraction of inspired (F IO2 ) and positive endexpiratory pressure (PEEP) No published studies in pregnant women Pre-ARDSnet data suggesting more barotrauma with higher V T
24 She is now in the ICU. Her mental status has declined and she is unable to protect her airway. Intubation occurs without difficulty. The RT asks for vent parameters. The intensivist, nurse, and RT all look over at you What parameters will you need to specify? Mode of ventilation Respiratory rate FIO2 PEEP All of the above
25 Key Points: Gravid Patient Respiratory changes in pregnancy 20% increase in O 2 consumption 15% increase in metabolic rate V E increases, RR stable VT increase by 40% over baseline ABG: respiratory alkalosis compensated by metabolic acidosis Stable ph PaCO2: 28 to 32 mmhg
26 Helpful Definitions Minute Ventilation (V E ) Amount of gas that moves in or out of lung in one minute V T x rate = V E Tidal Volume (V T ) Amount of gas that moves in or out of lung in one breath
27 Endotracheal Intubation Indicated with inability to maintain airway or adequate oxygenation or ventilation Respiratory rate (RR) > 30/min Inability to maintain arterial O 2 saturation > 90% with FIO2 > 0.60 PCO2 > 50 mmhg with ph < 7.25
28 Goals Ventilator Settings V E adjusted to maintain PaCO 2 30 to 32 mmhg ph 7.40 to 7.47 PaCO 2 < 30 mmhg may decrease uterine blood flow due to significant respiratory alkalosis
29 Other Considerations Gravid Patient Permissive hypercapnia Does not appear to adversely affect fetus (CO 2 level 60 mmhg) Positive End-Expiratory Pressure (PEEP) Added to mitigate end-expiratory alveolar collapse, usually 5 cm H 2 O Higher levels may be required in thirdtrimester
30 Other Considerations Most medications for analgesia, sedation, paralysis reach fetal circulation Analgesia Opioids acceptable, avoid NSAIDs
31 ARDS: Treatment Permissive hypercapnia (PaCO 2 >60 mmhg) Results from lower V T and minute ventilation Causes vasodilation, tachycardia, hypotension Does not appear to adversely affect fetus Increases uterine vascular resistance No human data regarding permissive hypercapnia in pregnancy
32 She is now intubated and respiratory status critical but stable. What other interventions are indicated at this time? Bicarbonate therapy PEEP of 2 cm H 2 O Prone positioning Fluid conservative management Corticosteroids
33 ARDS: Treatment Bicarbonate solution Advocated by some to correct acidosis Placental transfer not well studied Positive End-Expiratory Pressure (PEEP) Mitigate end-expiratory alveolar collapse, usually 5 cm H 2 O May need higher levels in third-trimester Increased intra-thoracic pressure and decreased venous return
34 ARDS: Treatment Prone positioning Data supports this in refractory hypoxemia to improve oxygenation Not shown to improve overall mortality In pregnancy, meticulous positioning and fetal monitoring required
35 ARDS: Treatment Appropriate treatment of precipitating event Fluid and hemodynamic management Lowest intravascular volume to maintain adequate tissue perfusion Urine output, acid-base status, CVP monitoring Vasopressors/ inotropes as needed Nutrition Enteral route preferred Corticosteroids Controversial benefit
36 Fetal Monitoring Best judgement
37 Pulmonary Edema
38 Pulmonary Edema: Background Occurs in 0.08% of normal pregnancies Occurs in 3.4% of preeclamptic pregnancies Occurs in 5% preterm labor situations In all affected pregnancies Tocolytic therapy or cardiac disease: 50% Preeclampsia (PEC) or iatrogenic volume overload: 50%
39 Pulmonary Edema: Risk Factors CATEGORY Prepregnancy conditions Pregnancy-specific diseases Pharmacological agents Iatrogenic volume overload Fetal conditions SPECIFIC RISK FACTORS Cardiovascular diseases Obesity Increased maternal age Endocrine disorders PEC Cardiomyopathy Sepsis Preterm labor Amniotic fluid embolism Pulmonary embolism Beta-agonists Corticosteroids Magnesium sulfate Illicit drugs Multiple gestation
40 Pulmonary Edema: Presentation Clinical presentation Tachypnea Dyspnea Hypoxemia Tachycardia Diffuse crackles Imaging findings
41 Pulmonary Edema: Tocolytic Therapy Tocolytic therapy Beta-2 agonists Calcium channel blockers Magnesium sulfate Contributing factors Multiple gestation, maternal infection Simultaneous administration of multiple medications Fluid overload Cardiac dysfunction Capillary permeability
42 Pulmonary Edema: Tocolytic Therapy No definitive diagnostic tests Diagnosis of exclusion in those receiving tocolytic therapy
43 Pulmonary Edema: Tocolytic Therapy Treatment Discontinuation of offending agent Supplemental oxygen Fluid restriction Diuresis Mechanical ventilation as necessary
44 Pulmonary Edema: Cardiogenic 23 per 1,000 deliveries during delivery 11 per 1,000 deliveries during postpartum Due to preexisting or new cardiac disease
45 Pulmonary Edema: Preeclampsia Uncommon complication Risk factors Older Multigravid In presence of additional organ system dysfunction
46 Pulmonary Edema: Preeclampsia Multifactorial Etiology Volume overload Decreased plasma oncotic pressure Increased capillary permeability Increased pulmonary capillary hydrostatic pressure
47 Pulmonary Edema: Diagnosis & Treatment
48 Pulmonary Edema: Diagnosis Physical exam CXR Blood studies Electrolytes, creatinine, protein Urinalysis Arterial blood gas (ABG)
49 Pulmonary Edema: Diagnosis EKG Echocardiogram Myocardial, valvular, structural pathologies
50 40yo G1P0 EGA 34w admitted for superimposed PEC evaluation in the setting of new onset dyspnea, cough and office BP 152/90 mmhg. Bilateral crackles on PE. P 115 BP RR 20 What is your next step? Obtain CXR Expanded history and exam Administer furosemide 40 mg IV Prepare for delivery in light of PEC


51 Pulmonary Edema Image courtesy Sherif R. Zaki, MD, Ph.D.


52 Pulmonary Edema Chest X-ray (CXR) CT Chest, coronal
53 Pulmonary Edema: Treatment Treatment Discontinuation of offending agent Treatment of underlying condition Supplemental oxygen Fluid restriction Diuresis Mechanical ventilation as necessary
54 Summary
55 Summary Respiratory failure in pregnancy is rare ARDS is a type of respiratory failure, with acute onset of bilateral infiltrates and hypoxemia ARDS causes impaired gas exchange, decreased compliance, increased pulmonary arterial pressure More than 60 possible causes of ARDS have been identified Mechanical ventilation with low V T strategy is standard management
56 Summary Permissive hypercapnia and increased PEEP may be considered. Pulmonary edema is most often secondary to tocolytic therapy, cardiac failure, severe preeclampsia, or eclampsia. Treatment of respiratory failure involves treatment of the underlying cause, oxygenation/ ventilatory support, sedation, analgesia, volume management, hemodynamic support, nutritional support, DVT prophylaxis.
57 Summary Acute respiratory failure requiring endotracheal intubation is notable for: respiratory rate (RR) > 30/min inability to maintain arterial O 2 saturation > 90% with FIO 2 > 0.60 (PaO 2 <55 mmhg) PaCO 2 > 50 mmhg with ph < 7.25
58 Summary Multiple modes of ventilation may be used in pregnancy Ventilator goals for the gravid patient: V E adjusted to maintain PaCO 2 30 to 32 mmhg ph 7.40 to 7.47
59 Thank You for Your Attention! Planning Committee Mike Foley, Director Shad Deering, co-director Helen Feltovich, co-director Bill Goodnight, co-director Loralei Thornburg, Content co-chair Deirdre Lyell, Content co-chair Suneet Chauhan, Testing Chair Mary d Alton Daniel O Keeffe Andrew Satin Barbara Shaw
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Acute Postpartum Pulmonary Edema: A Case Report
 Postpartum pulmonary edema 157 Acute Postpartum Pulmonary Edema: A Case Report Min-Po Ho 1, Wing-Keung Cheung 2, Kaung-Chau Tsai 1 Acute pulmonary edema after pregnancy is rare. Pulmonary emobolism, pneumonia,
Postpartum pulmonary edema 157 Acute Postpartum Pulmonary Edema: A Case Report Min-Po Ho 1, Wing-Keung Cheung 2, Kaung-Chau Tsai 1 Acute pulmonary edema after pregnancy is rare. Pulmonary emobolism, pneumonia,
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Medical Treatment for acute Decompensated Heart Failure. Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011
 Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Medical Treatment for acute Decompensated Heart Failure Vlasis Ninios Cardiologist St. Luke s s Hospital Thessaloniki 2011 2010 HFSA guidelines for ADHF 2009 focused update of the 2005 American College
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
to optimize By Jin Xiong Lian, BSN, RN, CNS
 Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
10/17/16. Acute Respiratory Failure in the Acute Care Setting. Margaret Rosales, APRN-CNP, FNP
 Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Acute Respiratory Failure in the Acute Care Setting Margaret Rosales, APRN-CNP, FNP Margaret_r1965@yahoo.com 918-448-5887 1 Definition: Respiratory failure is a syndrome in which the respiratory system
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
to optimize mechanical ventilation
 ILLUSTRATION BY ROY SCOTT Using ABGs to optimize mechanical ventilation Three case studies illustrate how arterial blood gas analyses can guide appropriate ventilator strategy. By Jin Xiong Lian, BSN,
ILLUSTRATION BY ROY SCOTT Using ABGs to optimize mechanical ventilation Three case studies illustrate how arterial blood gas analyses can guide appropriate ventilator strategy. By Jin Xiong Lian, BSN,
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy
 A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
A Challenging Case: Von Willebrand Disease and Pulmonary Hypertension in Pregnancy Diana S. Wolfe, MD, MPH Assistant Professor Department of Obstetrics & Gynecology and Women s Health Associate Fellowship
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
Blood Gases / Acid-Base
 Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,