|
|
|
- Peter Jones
- 6 years ago
- Views:
Transcription
1

2
3 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical needs, practical

4 European Heart Journal doi: /eurheartj/ehs092
5 Why is CVD prevention needed Atherosclerotic CVD, especially CHD, remains the leading cause of premature death worldwide. CVD affects both men and women; of all deaths that occur before the age of 75 years in Europe, 42% are due to CVD in women and 38% in men. Prevention works: over 50% of the reductions seen in CHD mortality relate to changes in risk factors, and 40% to improved treatments.

6 Prevention of cardiovascular disease Life expectancy in years for countries in WHO European Region Span 16 years
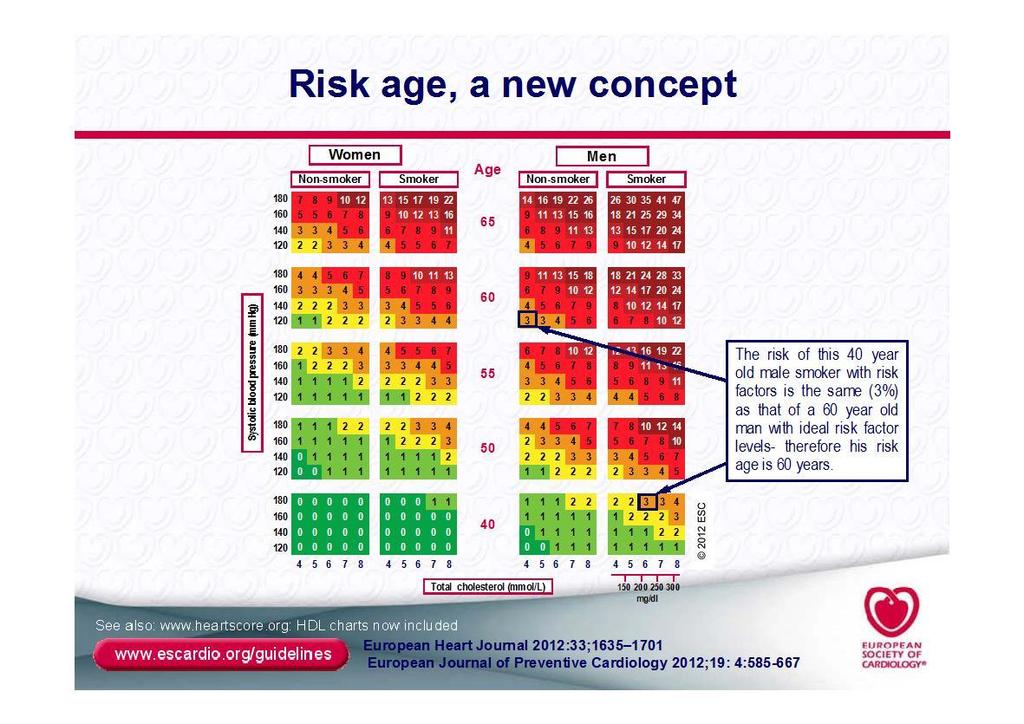
7 For whom is CVD prevention needed Recommendations regarding risk estimation Class Level GRADE Total risk estimation using multiple risk factors (such as SCORE) is recommended for asymptomatic adults without evidence of CVD High-risk individuals can be detected on the basis of established CVD, diabetes type 2 or type 1 with end-organ damage, moderate to severe renal disease, very high levels of individual risk factors or a high SCORE risk I C Strong I C Strong Risk factor screening including the lipid profile should be considered in adult men 40 years old and in women 50 years of age or postmenopausal The physician in general practice is the key person to initiate, coordinate and provide longterm follow-up for CVD prevention

8
9 Timeline atherosclerosis Foam cell Fatty streak Intermediary lesion Atheroma Fibrous plaque Complicated lesion/rupture First decennium Endothelial dysfunction From third dcennium From fourth decennium Growth mainly through lipid deposition Smooth muscle, collagene Thrombosis hematoma
10 Very high risk Subjects with any of the following: Documented CVD by invasive or non-invasive testing (such as coronary angiography, nuclear imaging, stress echocardiography, carotid plaque on ultrasound), previous myocardial infarction, ACS, coronary revascularization (PCI, CABG) and other arterial revascularization procedures, ischaemic stroke, peripheral artery disease Diabetes mellitus (type 1 or type 2) with one or more CV riskfactors and/or target organ damage (such as microalbuminuria: mg/24 h) Severe chronic kidney disease (CKD) (glomerular filtration rate (GFR] <30 ml/min/1.73 m 2 ). A calculated SCORE 10%.
11 Other risk groups High risk Markedly elevated single risk factors such as familial dyslipidaemias and severe hypertension. Diabetes mellitus (type 1 or type 2) but without CV riskfactors or target organ damage. Moderate chronic kidney disease (CKD) (glomerular filtration rate (GFR] ml/min/1.73 m 2 ). A calculated SCORE of 5% and <10% for 10-year risk of fatal CVD. Moderate risk Subjects are considered to be at moderate risk when their SCORE is 1 and <5% at 10 years. Many middle-aged subjects belong to this category. Low risk The low-risk category applies to individuals with a SCORE <1% and free of qualifiers that would put them at moderate risk.

12 Timeline atherosclerosis Foam cell Fatty streak Intermediary lesion Atheroma Fibrous plaque Complicated lesion/rupture Low risk Moderate risk High risk Very high risk Observe: the term primairy and secondairy Anpassad från Stary HC et al. Circulation. 1995;92: prevention has been replaced by four risk groups
13
14 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied Behavioural factors Risk factors 5. Where should CVD prevention be offered

15 Anyone for cigarettes?
16 Recommendations regarding smoking All smoking is a strong and independent risk factor for CVD and has to be avoided. Exposure to passive smoking increases risk of CVD and has to be avoided. Young people have to be encouraged not to take up smoking. All smokers should be given advice to quit and be offered assistance. Class Level GRADE I B strong I B strong I C strong I A strong
17 Recommendations regarding nutrition A healthy diet is recommended as being the cornerstone of CVD prevention Class Level GRADE I B strong Saturated fatty acids to account for <10% of total energy intake, through replacement by polyunsaturated fatty acids. Trans unsaturated fatty acids: as little as possible, preferably no intake from processed food, and <1% of total energy intake from natural origin <5 g of salt per day g of fibre per day, from wholegrain products, fruits and vegetables. 200 g of fruit per day (2-3 servings). 200 g of vegetables per day (2-3 servings). Fish at least twice a week, one of which to be oily fish. Consumption of alcoholic beverages should be limited to 2 glasses per day (20 g/d of alcohol) for men and 1 glass per day (10 g/d of alcohol) for women.
18 Recommendations regarding physical activity Healthy adults of all ages have to spend hours a week on physical activity or aerobic exercise training of at least moderate intensity, or hours a week on vigorous intense exercise. Class Level GRADE I A strong Sedentary subjects should be strongly encouraged to start light-intensity exercise programmes.
19 Recommendations on blood pressure Lifestyle measures such as weight control, increased physical activity, alcohol moderation, sodium restriction, and increased consumption of fruits, vegetables, and low-fat dairy products are recommended in all patients with hypertension and in individuals with high normal BP. All major antihypertensive drug classes (i.e. diuretics, ACE inhibitors, calcium antagonists, angiotensin receptor antagonists and beta-blockers) do not differ significantly in their BP-lowering efficacy and thus should be recommended for the initiation and maintenance of antihypertensive treatment Systolic BP should be lowered to <140 mmhg (and DBP <90 mmhg) in all hypertensive patients. Class Level GRADE I B strong I A strong IIa A strong

20 Lifestyle efforts first

21 Provide home measuring equipment, control product quality
22 Recommendations on diabetes mellitus The target HbA 1c for the prevention of CVD in diabetes of < 7.0% (<53 mmol/mol) is recommended. Statins are recommended to reduce cardiovascular risk in diabetes. BP targets in diabetes are recommend to be <140/80 mmhg Class Level GRADE I A Strong I A Strong I A Strong Weight control campaigns to fight type II DM Stimulate early detection of IGT in general practice
23 Target levels LDL In patients at very high risk the LDL-C goal is < 1.8 mmol/l and/or 50% LDL-C reduction when target level cannot be reached. In patients at HIGH CV risk an LDL-C goal < 2.5 mmol/l should be considered. In subjects at MODERATE risk an LDL-C goal < 3.0 mmol/l should be considered. See Euroaspire III, EURIKA: audit needed!
24 5: Where should CVD prevention programmes be offered? Class Level GRADE Actions to prevent CVD should be incorporated into everyone s daily lives, starting in early childhood and continuing throughout adulthood and senescence. Nurse-coordinated prevention programmes should be well integrated into healthcare systems. All patients with CVD must be discharged from hospital with clear guideline-orientated treatment recommendations to minimize adverse events. All patients requiring hospitalization or invasive intervention after an acute ischaemic event should participate in a cardiac rehabilitation programme to improve prognosis by modifying lifestyle habits and increasing treatment adherence IIa B Strong IIa B Strong I B Strong IIa B Strong
25 Further key messages Patients with cardiac disease may participate in self-help programmes to increase or maintain awareness of the need for risk factor management Non-governmental organisations are important partners to health care workers in promoting preventive cardiology The European Heart Health Charter marks the start of a new era of political engagement in preventive cardiology
26
27 In summary: the main messages Risk screening recommended, prime role of general practice Avoid second-hand smoke, quit smoking services Food: salt, transfatty acids, fruits and vegetables Physical activity: young generation No hypertension treatment without lifestyle counselling Home BP equipment: check quality, support purchase for patients Weight control campaigns, early detection of impaired glucose tolerance Audit achievement of target levels, espec. för lipids and blood pressure Promote nurse-coordinated prevention programmes
28 In summary: the main messages Risk screening recommended, prime role of general practice Avoid second-hand smoke, quit smoking services Food: salt, transfatty acids, fruits and vegetables Physical activity: young generation No hypertension treatment without lifestyle counselling Home BP equipment: check quality, support purchase for patients Weight control campaigns, early detection of impaired glucose tolerance WHO target: to reduce cardiovascular mortality with 25 % until 2015: 25 by 25 Audit achievement of target levels, espec. för lipids and blood pressure Promote nurse-coordinated prevention programmes Thank you!
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION
 Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Present state and future trends of prevention guidelines
 Present state and future trends of prevention guidelines Professor Željko Reiner MD, PhD, FRCP (Lond), FESC,FACC School of Medicine, University of Zagreb, Croatia History of European guidelines on CVD
Present state and future trends of prevention guidelines Professor Željko Reiner MD, PhD, FRCP (Lond), FESC,FACC School of Medicine, University of Zagreb, Croatia History of European guidelines on CVD
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
New ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Lipids. Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC
, FESC, FACC") New ES Guidelines on ardiovascular Disease Prevention in linical Practice Lipids Professor Željko Reiner, MD, PhD, FRP(Lond), FES, FA University Hospital enter Zagreb School of Medicine, University of
New ES Guidelines on ardiovascular Disease Prevention in linical Practice Lipids Professor Željko Reiner, MD, PhD, FRP(Lond), FES, FA University Hospital enter Zagreb School of Medicine, University of
7/6/2012. University Pharmacy 5254 Anthony Wayne Drive Detroit, MI (313)
") University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
Prevenzione cardiovascolare e cambiamento degli stili di vita. Gian Franco Gensini
 Prevenzione cardiovascolare e cambiamento degli stili di vita Gian Franco Gensini Main causes of death worldwide at all ages (year:: 2005) 17.5 milion Preventing Chronic Diseases A vital investiment. WHO
Prevenzione cardiovascolare e cambiamento degli stili di vita Gian Franco Gensini Main causes of death worldwide at all ages (year:: 2005) 17.5 milion Preventing Chronic Diseases A vital investiment. WHO
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
PREVENTION OF CARDIOVASCULAR DISEASES (CVD)
") PREVENTION OF CARDIOVASCULAR DISEASES (CVD) SIGNIFICANCE OF NON-COMMUNICABLE DISEASES Non-communicable diseases were responsible for 2/3 of all deathsglobally in 2011, up from 60% in 2000. High-income
PREVENTION OF CARDIOVASCULAR DISEASES (CVD) SIGNIFICANCE OF NON-COMMUNICABLE DISEASES Non-communicable diseases were responsible for 2/3 of all deathsglobally in 2011, up from 60% in 2000. High-income
Clinical Care Performance. Financial Year 2012 to 2018
 Clinical Care Performance Financial Year 2012 to 2018 SHP Clinical Care Performance Diabetes Mellitus Hyperlipidemia Hypertension Diabetes Mellitus Find out how our patients are doing for: HbA1C HbA1c
Clinical Care Performance Financial Year 2012 to 2018 SHP Clinical Care Performance Diabetes Mellitus Hyperlipidemia Hypertension Diabetes Mellitus Find out how our patients are doing for: HbA1C HbA1c
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
Guidelines for Integrated Management of. Cardiovascular Diseases and Diabetes. in Clinics and Ri-hospitals
 Guidelines for Integrated Management of Cardiovascular Diseases and Diabetes in Clinics and Ri-hospitals Ministry of Public Health DPR Korea January 2013 Rationale ncommunicable diseases such as cardiovascular
Guidelines for Integrated Management of Cardiovascular Diseases and Diabetes in Clinics and Ri-hospitals Ministry of Public Health DPR Korea January 2013 Rationale ncommunicable diseases such as cardiovascular
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Models of preventive care in clinical practice to achieve 25 by 25
 Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver)
") I. TEST YOUR KNOWLEDGE OF CHOLESTEROL Choose the correct answer. 1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver) 2. Only
I. TEST YOUR KNOWLEDGE OF CHOLESTEROL Choose the correct answer. 1. Most of your blood cholesterol is produced by: a. your kidneys b. your liver c. your pancreas d. food consumption (Your liver) 2. Only
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Reducing risk in heart disease
 Reducing risk in heart disease An expert guide to clinical practice for secondary prevention of coronary heart disease Prof Patricia Davidson (chair) Prof Nigel Stocks Dr Anu Aggarwal Ms Jill Waddell Ms
Reducing risk in heart disease An expert guide to clinical practice for secondary prevention of coronary heart disease Prof Patricia Davidson (chair) Prof Nigel Stocks Dr Anu Aggarwal Ms Jill Waddell Ms
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Professor Norman Sharpe. Heart Foundation West Coast
 Professor Norman Sharpe Heart Foundation West Coast Primary Care the Keystone to Heart Health Improvement Norman Sharpe June 2013 The heart health continuum and the keystone position The culprit disease
Professor Norman Sharpe Heart Foundation West Coast Primary Care the Keystone to Heart Health Improvement Norman Sharpe June 2013 The heart health continuum and the keystone position The culprit disease
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
2013 Hypertension Measure Group Patient Visit Form
 Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Clinical Practice Guideline
 Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY
 MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
MCC-006 POST GRADUATE DIPLOMA IN CLINICAL CARDIOLOGY (PGDCC) 00269 Term-End Examination December, 2009 MCC-006 : CARDIOVASCULAR EPIDEMIOLOGY Time : 2 hours Maximum Marks : 60 Note : There will be multiple
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
Blood Pressure Acre Surgery Diviash Thakrar
 Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Helen Williams Consultant Pharmacist for CV Disease - South London
 Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
National Strategy. for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain
 Kingdom of Bahrain Ministry of Health National Strategy for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain 2014 2025 Behavioural Risk Factors Tobacco Use Unhealthy Diets Physical
Kingdom of Bahrain Ministry of Health National Strategy for Control and Prevention of Non - communicable Diseases in Kingdom of Bahrain 2014 2025 Behavioural Risk Factors Tobacco Use Unhealthy Diets Physical
Diabetes and Heart Disease. Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center
 Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
ASSeSSing the risk of fatal cardiovascular disease
 ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
Session 21: Heart Health
 Session 21: Heart Health Heart disease and stroke are the leading causes of death in the world for both men and women. People with pre-diabetes, diabetes, and/or the metabolic syndrome are at higher risk
Session 21: Heart Health Heart disease and stroke are the leading causes of death in the world for both men and women. People with pre-diabetes, diabetes, and/or the metabolic syndrome are at higher risk
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Cardiovascular Disease Risk Factors:
 Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Heart Disease Genesis
 Heart Disease Genesis The Ultimate Lecture on CAD origins Petr Polasek MD FRCPC FACC Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Heart Disease Genesis The Ultimate Lecture on CAD origins Petr Polasek MD FRCPC FACC Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano alberico.catapano@unimi.it Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Prevention of Cardiovascular Disease
 Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Care Bundle. Adult patients with Type 2 Diabetes
 Care Bundle Adult patients with Type 2 Diabetes July 2014 What is a care bundle? A care bundle is a set of interventions that, when used together, significantly improve patient outcomes. The measures chosen
Care Bundle Adult patients with Type 2 Diabetes July 2014 What is a care bundle? A care bundle is a set of interventions that, when used together, significantly improve patient outcomes. The measures chosen
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
What s New? Hypertension Canada Guidelines for the Management of Hypertension
 What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
What s New? 2017 Hypertension Canada Guidelines for the Management of Hypertension What s New? About This Booklet This booklet highlights key advancements and important, enduring aspects of the Hypertension
EUROACTION A model for secondary and primary preventive care to achieve 25 by 25
 EUROACTION A model for secondary and primary preventive care to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health
EUROACTION A model for secondary and primary preventive care to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health
EVA, Metabolic Syndrome and rehabilitation
 Baltic Rehab Congress Tallinn 17th September 2010 EVA, Metabolic Syndrome and rehabilitation Peter Nilsson, MD, PhD Department of Clinical Sciences Lund University University Hospital, Malmo, Sweden Metabolic
Baltic Rehab Congress Tallinn 17th September 2010 EVA, Metabolic Syndrome and rehabilitation Peter Nilsson, MD, PhD Department of Clinical Sciences Lund University University Hospital, Malmo, Sweden Metabolic
Diet, Lifestyle and Obesity Management. Healthy behaviours and interventions remain the cornerstone of chronic disease management and
 Diet, Lifestyle and Obesity Management Healthy behaviours and interventions remain the cornerstone of chronic disease management and prevention. They should be universally applied to all of those with
Diet, Lifestyle and Obesity Management Healthy behaviours and interventions remain the cornerstone of chronic disease management and prevention. They should be universally applied to all of those with
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Ira S. Ockene, M.D. David and Barbara Milliken Professor of Preventive Cardiology University of Massachusetts Medical School
 Cardiovascular Disease: how did it become such a problem, what are the risk factors with particular emphasis on diabetes and obesity, and how public policy work can to improve the health of all Ira S.
Cardiovascular Disease: how did it become such a problem, what are the risk factors with particular emphasis on diabetes and obesity, and how public policy work can to improve the health of all Ira S.
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Prevention of Heart Disease. Giridhar Vedala, MD Cardiovascular Medicine
 Prevention of Heart Disease Giridhar Vedala, MD Cardiovascular Medicine What is Heart Disease? Heart : The most hard-working muscle of our body pumps 4-5 liters of blood every minute during rest Supplies
Prevention of Heart Disease Giridhar Vedala, MD Cardiovascular Medicine What is Heart Disease? Heart : The most hard-working muscle of our body pumps 4-5 liters of blood every minute during rest Supplies
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
ESSENTIAL HYPERTENSION
 E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
E S S E N T I A L H Y P E R T E N S I O N Elevated blood pressure is one of the most important causes of cardiovascular disease. J A Ker MB ChB, MMed, MD Professor and Deputy Dean Faculty of Health Sciences
The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention
 Brief Report The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention Kornelia Kotseva 1,2 ; on behalf of the EUROASPIRE Investigators 1 National Heart & Lung Institute, Imperial College
Brief Report The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention Kornelia Kotseva 1,2 ; on behalf of the EUROASPIRE Investigators 1 National Heart & Lung Institute, Imperial College
Cardiovascular disease, studies at the cellular and molecular level. Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009
 Cardiovascular disease, studies at the cellular and molecular level Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009 Content Introduction The number 1 killer in America Some statistics
Cardiovascular disease, studies at the cellular and molecular level Linda Lowe Krentz Bioscience in the 21 st Century September 23, 2009 Content Introduction The number 1 killer in America Some statistics
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People
 - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People") November September 23, 20, 20102012 Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People Eva Lonn, Jackie Bosch, Jane Castelli, Andrea
November September 23, 20, 20102012 Heart Outcomes Prevention Evaluation (HOPE) - 3 Combined Lipid Lowering and Blood Pressure Lowering in Moderate Risk People Eva Lonn, Jackie Bosch, Jane Castelli, Andrea
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Cardiovascular Disease: Prevention in General Practice
 Quality in Practice Committee Cardiovascular Disease: Prevention in General Practice AUTHORS Dr John Cox and Professor Ian Graham DISCLAIMER AND WAIVER OF LIABILITY Whilst every effort has been made by
Quality in Practice Committee Cardiovascular Disease: Prevention in General Practice AUTHORS Dr John Cox and Professor Ian Graham DISCLAIMER AND WAIVER OF LIABILITY Whilst every effort has been made by
Chapter 08. Health Screening and Risk Classification
 Chapter 08 Health Screening and Risk Classification Preliminary Health Screening and Risk Classification Protocol: 1) Conduct a Preliminary Health Evaluation 2) Determine Health /Disease Risks 3) Determine
Chapter 08 Health Screening and Risk Classification Preliminary Health Screening and Risk Classification Protocol: 1) Conduct a Preliminary Health Evaluation 2) Determine Health /Disease Risks 3) Determine
Dr G R Letchuman. Clogged by Cholesterol
 Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
14/15 Threshold 15/16 Points 15/16. Points. Retired Replaced by NM82/AF007. Replacement NO CHANGE
 SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
SUMMARY OF CHANGES TO QOF 2015/1 - ENGLAND KEY No change Retired/replaced Wording and/or change Point or threshold change Indicator ID change 14/15 QOF ID 15/1 QOF ID NICE ID Indicator wording Changes
PLEASE REMEMBER TO BRING TO EACH APPOINTMENT
 PLEASE REMEMBER TO BRING TO EACH APPOINTMENT Conversion table for HbA1c% to mmol/mol Old DCCT aligned HbA1c(%) New IFCC HbA1c (mmol/mol) 4.0 20 5.0 31 6.0 42 6.5 48 7.0 53 7.5 59 8.0 64 9.0 75 10.0 86
PLEASE REMEMBER TO BRING TO EACH APPOINTMENT Conversion table for HbA1c% to mmol/mol Old DCCT aligned HbA1c(%) New IFCC HbA1c (mmol/mol) 4.0 20 5.0 31 6.0 42 6.5 48 7.0 53 7.5 59 8.0 64 9.0 75 10.0 86
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Arteriosclerosis & Atherosclerosis
 Arteriosclerosis & Atherosclerosis Arteriosclerosis = hardening of arteries = arterial wall thickening + loss of elasticity 3 types: -Arteriolosclerosis -Monckeberg medial sclerosis -Atherosclerosis Arteriosclerosis,
Arteriosclerosis & Atherosclerosis Arteriosclerosis = hardening of arteries = arterial wall thickening + loss of elasticity 3 types: -Arteriolosclerosis -Monckeberg medial sclerosis -Atherosclerosis Arteriosclerosis,
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in