2/14/2018 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION. Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1
|
|
|
- Ralf Wilcox
- 6 years ago
- Views:
Transcription
1 CASE STUDIES: COMPLICATIONS OF MYOCARDIAL INFARCTION Judy Hung, MD Cardiology Division Massachusetts General Hospital Boston, MA CASE 1 1
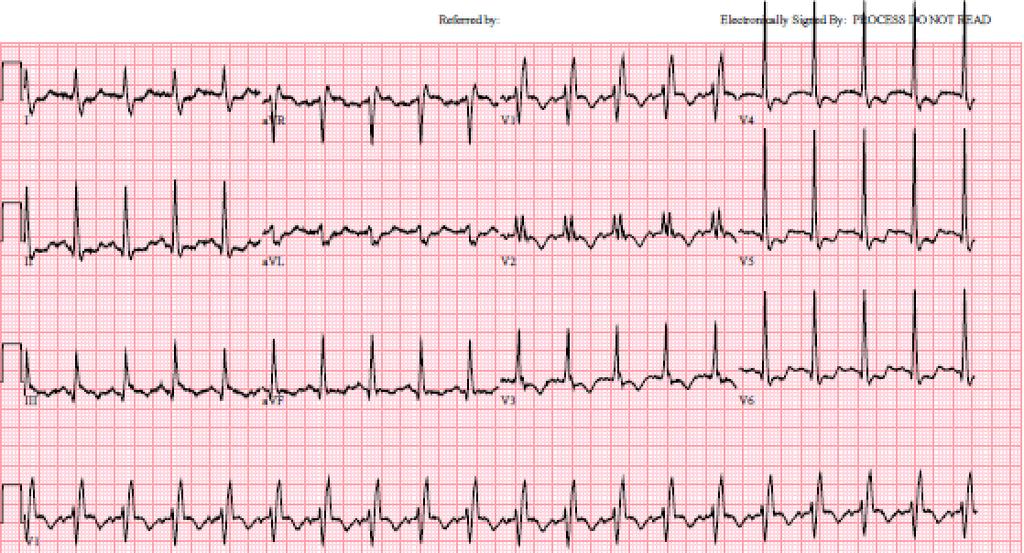
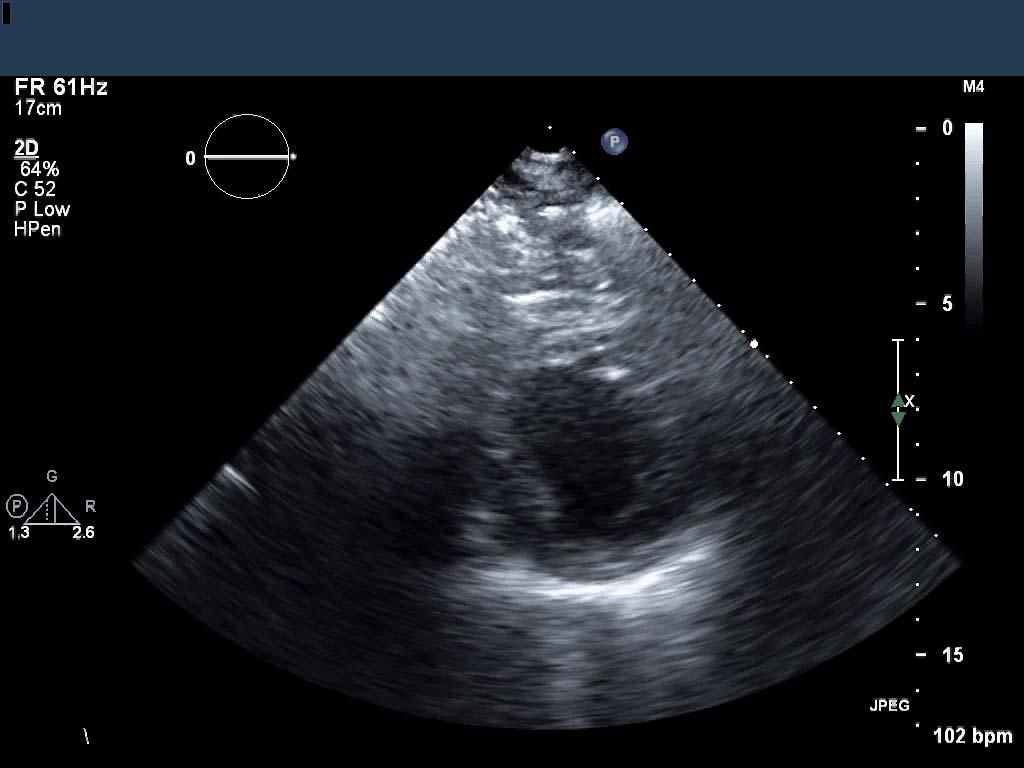
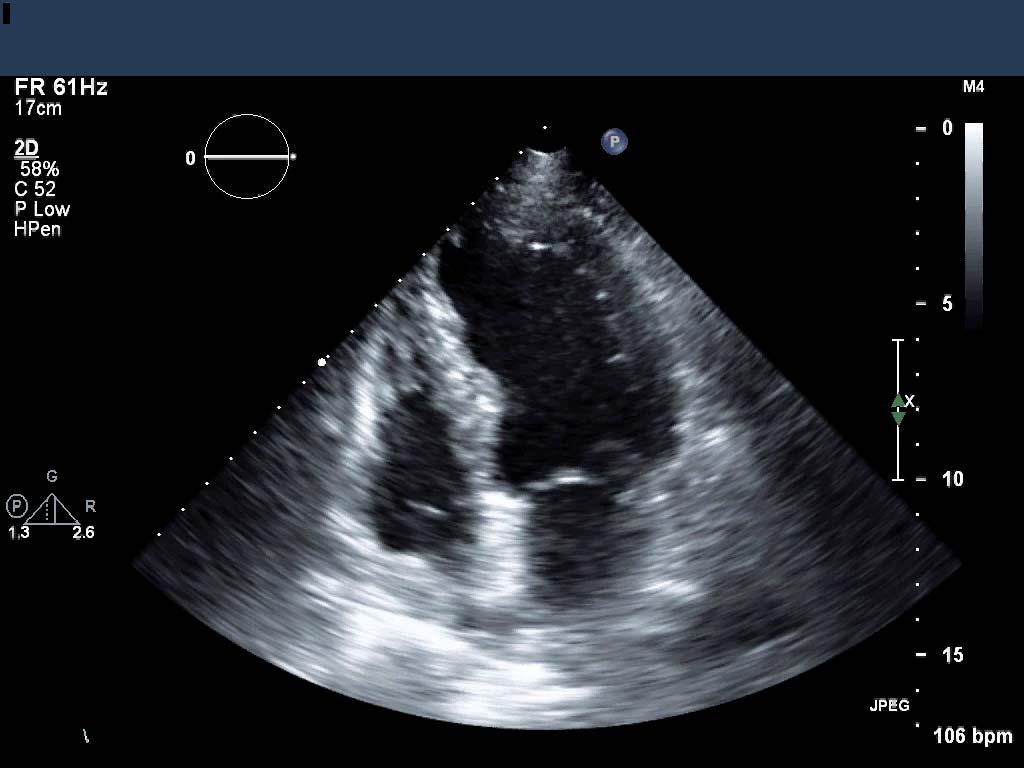
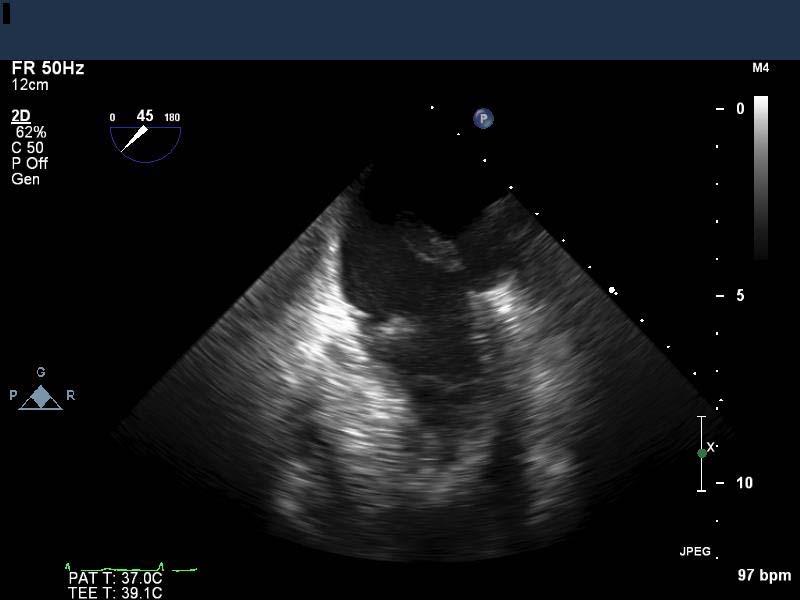
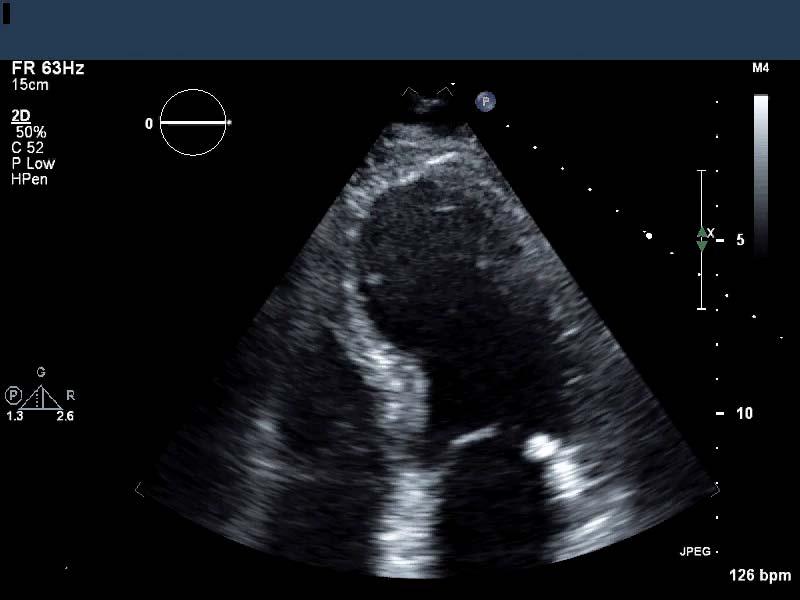
2 PRESENTATION 57 yo male with a past medical history of hypertension presented with fatigue and dyspnea on exertion 4 days prior to presentation the patient developed chest, back, and upper shoulder pain while digging a grave for his pet The next day he continued to not feel well with fatigue, nausea, and vomiting The next morning the patient reported that he felt better; however, the following morning he again started to feel unwell with fatigue and dyspnea on exertion The patient contacted his primary care physician who recommended that the patient be evaluated in the emergency department PRESENTATION The patient s vital signs upon arrival to the emergency department were: T: 97.6, HR: 116, BP: 116/84, RR: 24, Sp02: 98% RA Physical exam was notable for a harsh, holosystolic murmur heard throughout the precordium Initial lab work was notable for a troponin I of 5.6 ng/ml and elevated BUN/Cr of 72/4.2 2

3 3
4 4
5 5
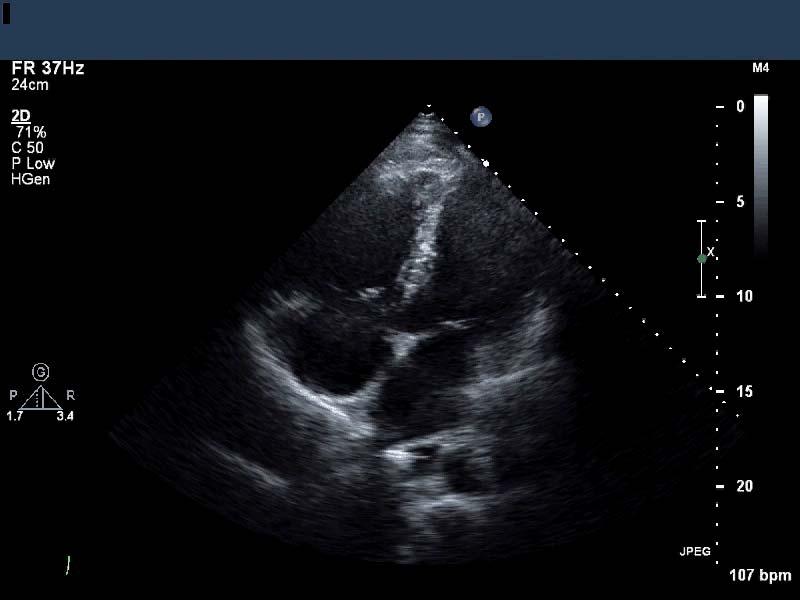
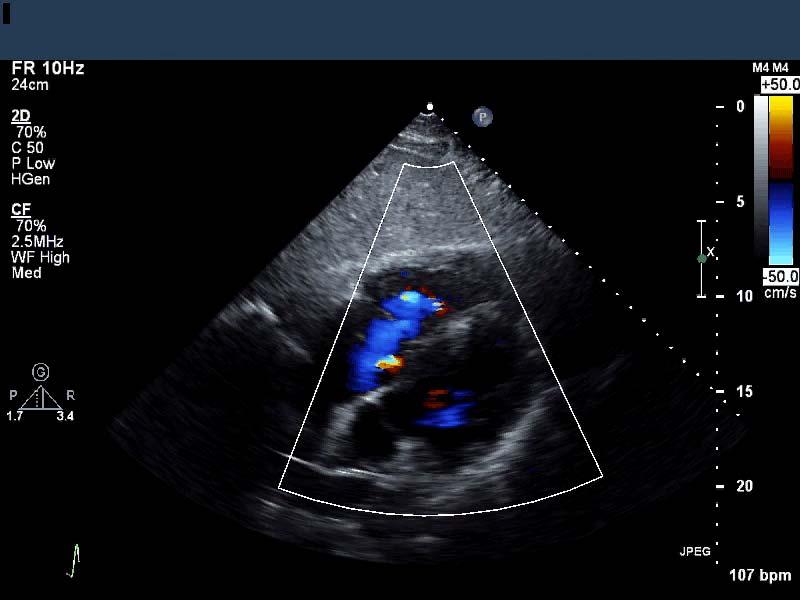
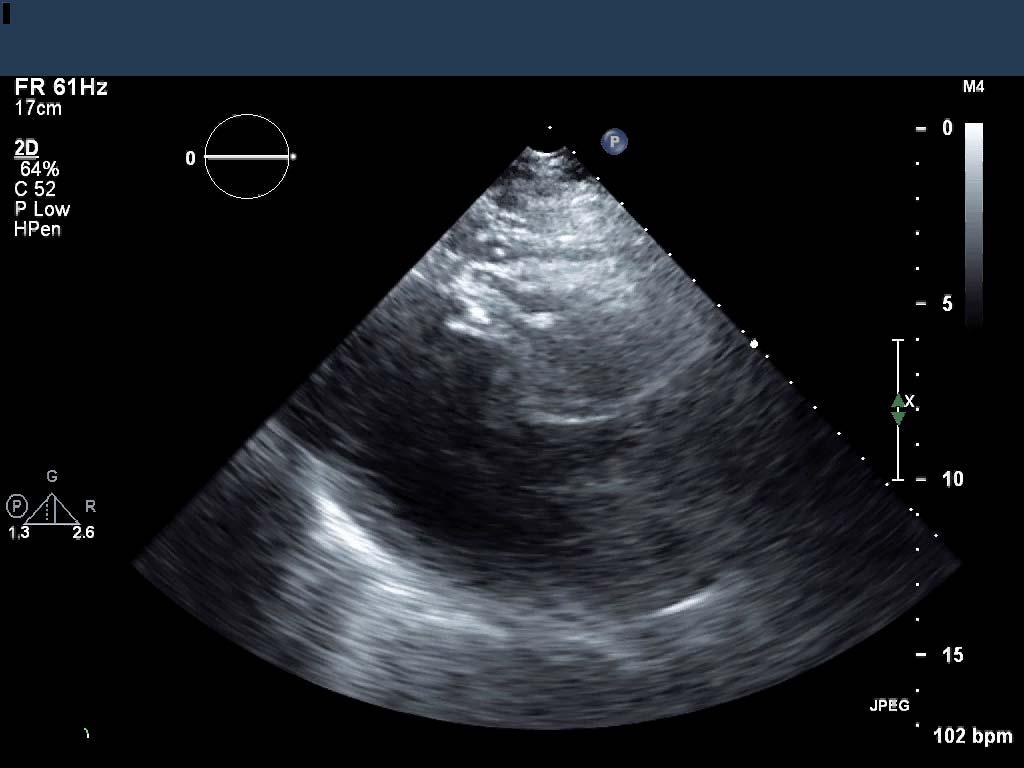
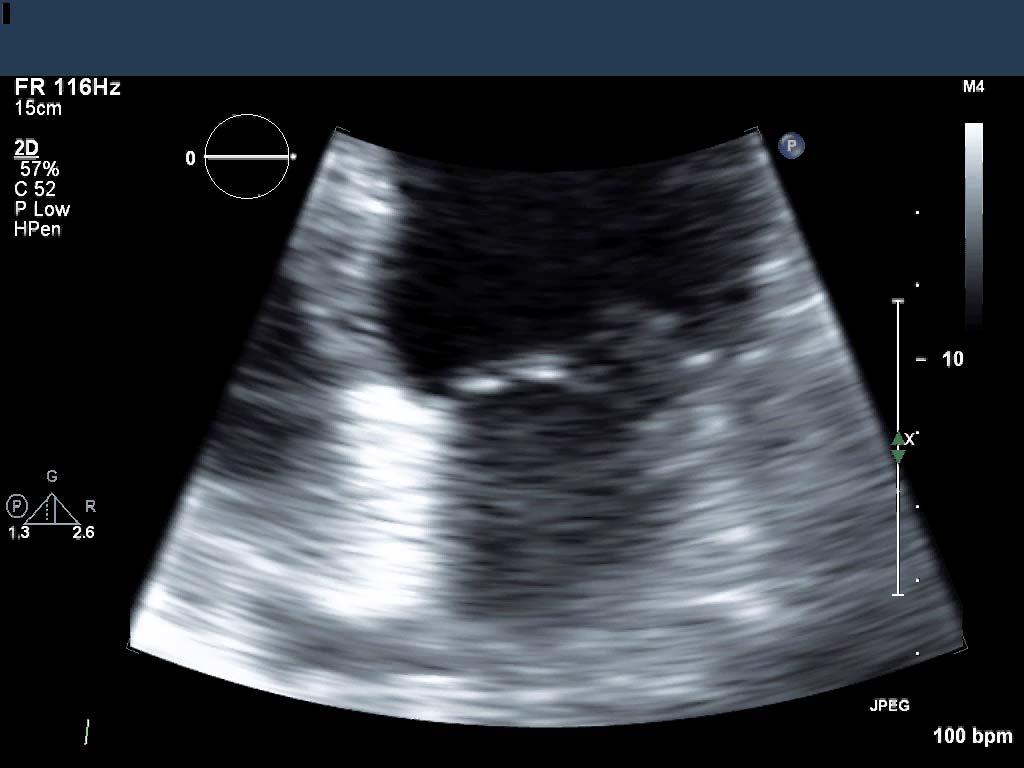
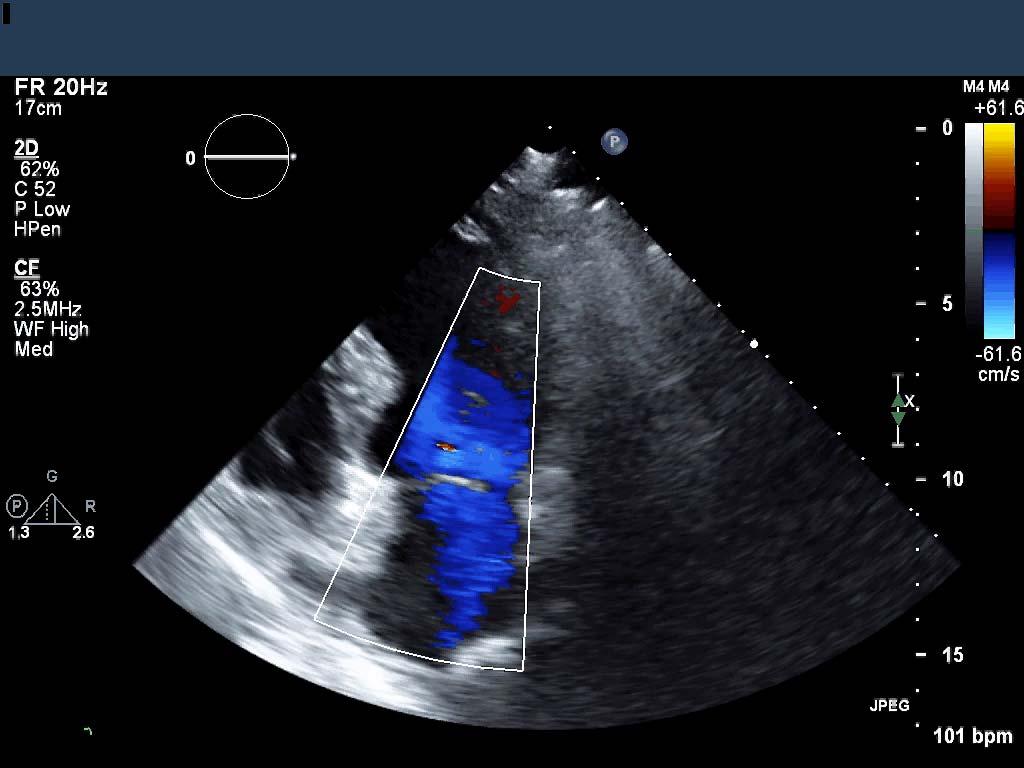
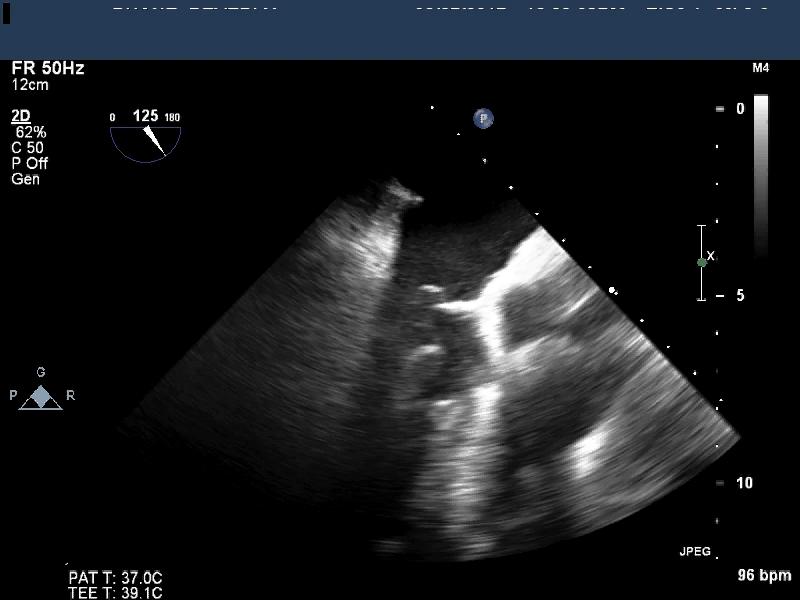
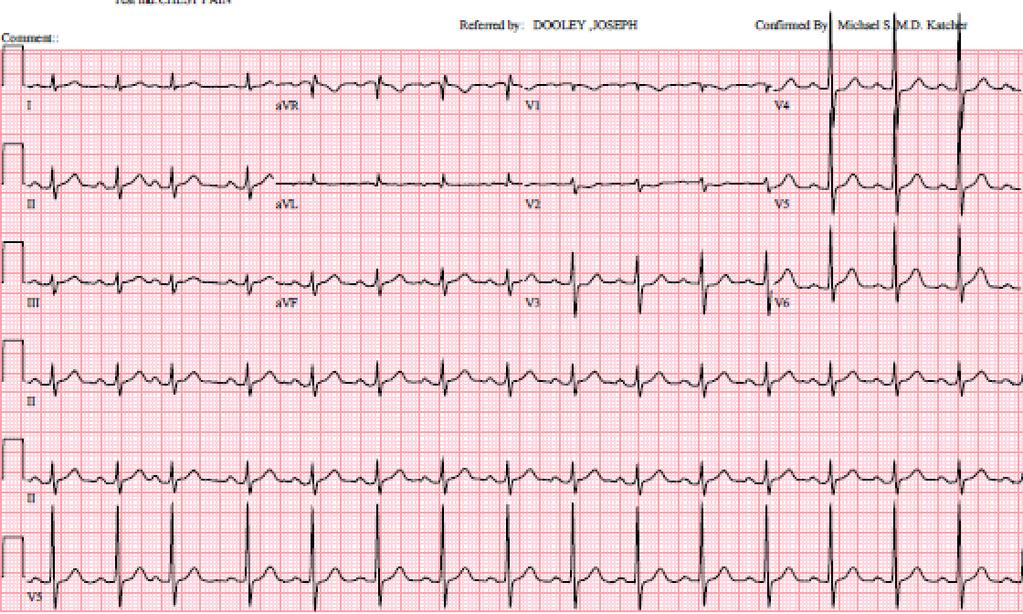
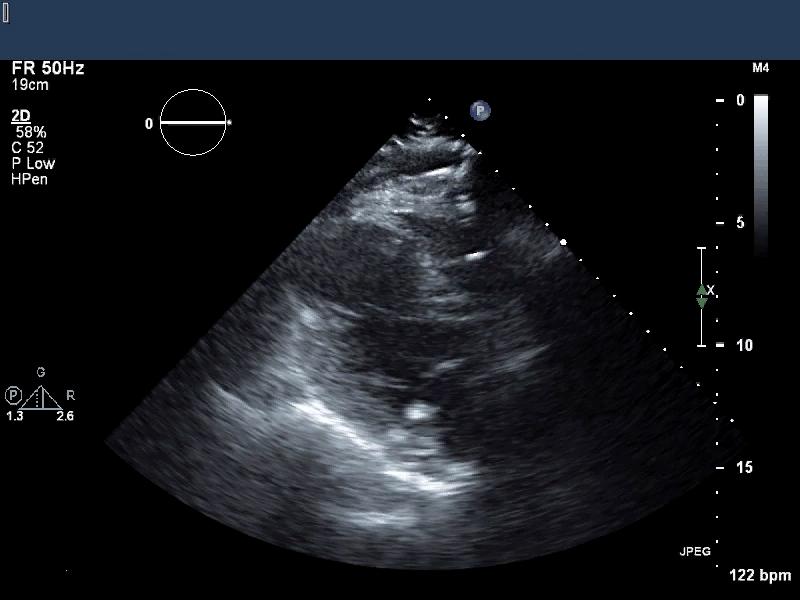
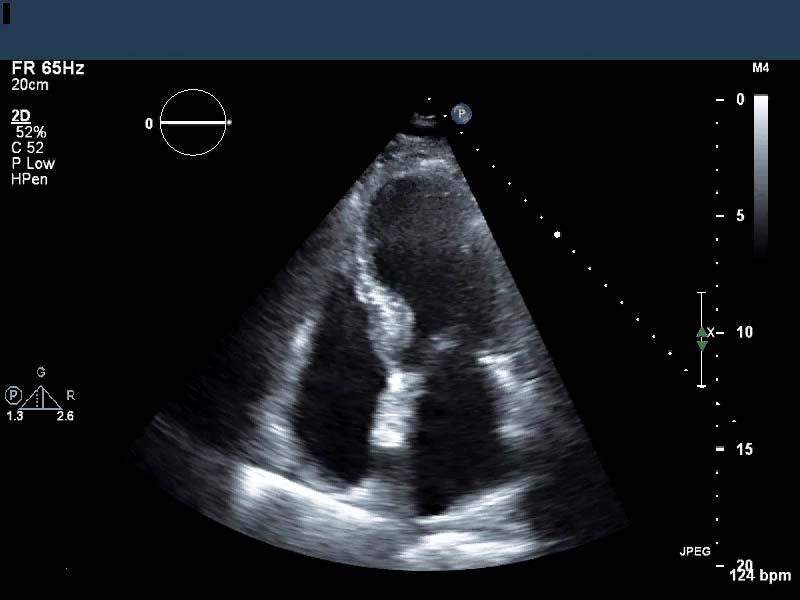
6 BASED UPON THIS ECHOCARDIOGRAM WHAT IS THE MOST LIKELY ETIOLOGY OF THE PATIENT S SYMPTOMS? 6
")
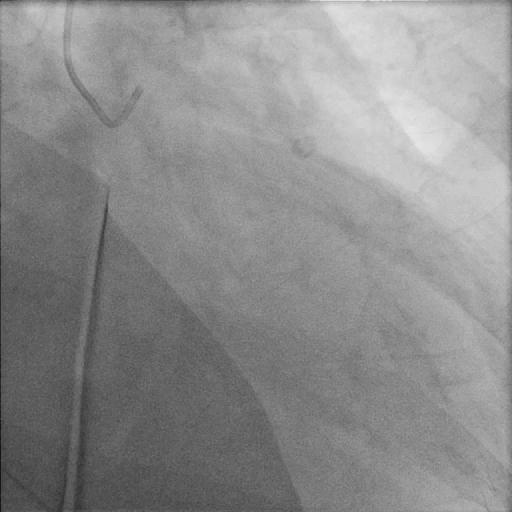
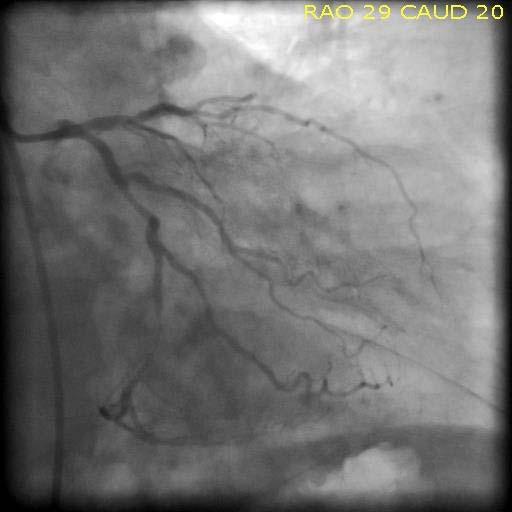
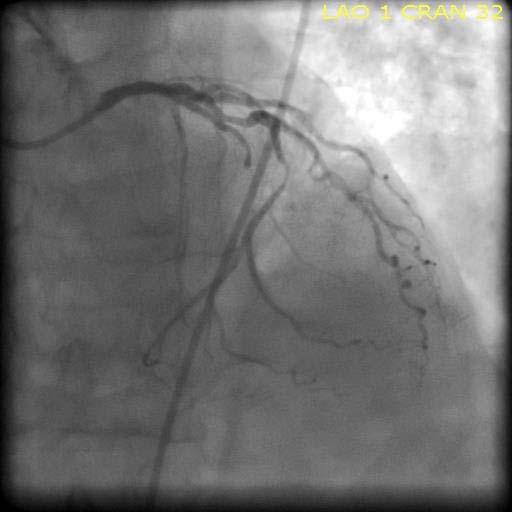
7 PRESENTATION The patient was sent for a right heart catheterization and coronary angiogram RHC 02 Sat: SVC: 46.3% IVC: 54.4% High RA: 47% Low RA: 56% RV: 85% PA: 79% Hemodynamics: RA: 18, RV: 62/17, PA: 62/24/26, PCWP: 23 (with V waves to 60) 7

8 A BLOCKAGE IN WHICH CORONARY ARTERY IS MOST LIKELY RESPONSIBLE FOR THIS PATIENT S VENTRICULAR SEPTAL DEFECT? 8
 and 50% occur with inferior MIs (VSD located in the basal inferior septum) Risk factors: single vessel disease, first myocardial")
9 VENTRICULAR SEPTAL DEFECTS Epidemiology and Natural History: With increased coronary reperfusion, incidence has declined to 0.2% 50% occur with anterior MIs (VSD located in the apical septum) and 50% occur with inferior MIs (VSD located in the basal inferior septum) Risk factors: single vessel disease, first myocardial infarction (due to lack of collaterals), and extensive myocardial damage Increased mortality with inferobasal VSDs compared with anterior apical VSDs. 9
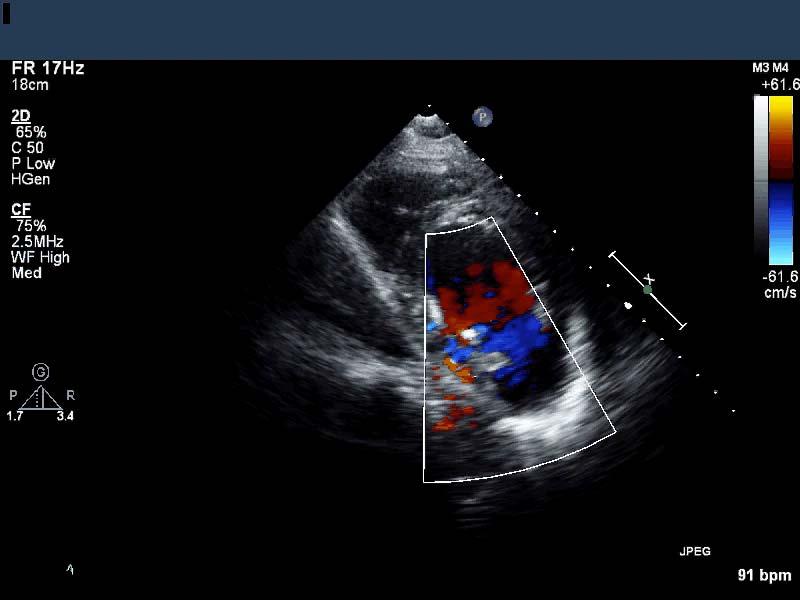
10 VENTRICULAR SEPTAL DEFECTS Clinical Manifestations: Chest pain Shortness of breath without frank pulmonary congestion Tachycardia and hypotension Signs of right-sided heart failure including elevated jugular venous pressure, right-sided S3, and/or RV lift New, harsh holosystolic murmur with widespread radiation Thrill (50% of patients) VENTRICULAR SEPTAL DEFECTS Diagnosis: Two-dimensional echocardiography alone only has a sensitivity of 40% The sensitivity of two-dimensional echocardiography is increased with the addition of Doppler color flow mapping Turbulent Doppler color flow may be the only clue to a VSD as some VSDs are narrow, irregular, and serpiginous (especially in the basal inferior septum) Confirmation can be made through a RHC with shunt run which shows a step-up at the ventricular level as well as giant pulmonary capillary pressure V waves because of volume overload in the setting of reduced LA compliance. 10
11 VENTRICULAR SEPTAL DEFECTS Treatment: Medical: vasodilators, diuretics, IABP Surgical**: patch repair +/- coronary artery bypass grafting Percutaneous closure** (** in the absence of cardiogenic shock the optimal timing for repair is still controversial) CLINICAL COURSE The patient underwent a surgical repair of the VSD with coronary artery bypass grafting (LIMA- LAD, SVG-RCA) The patient did well post-operatively and was ultimately discharged home 11
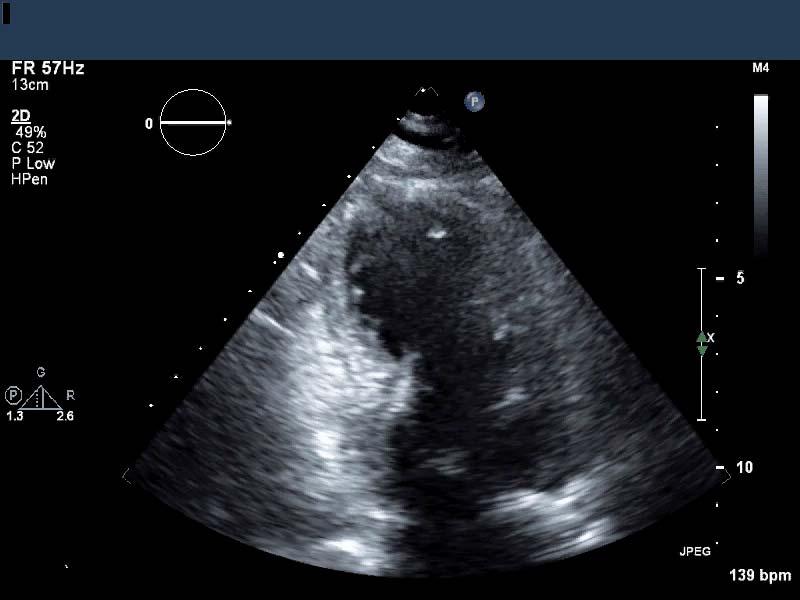
12 CASE 2 PRESENTATION 67 yo female with a past medical history of hypertension, hyperlipidemia, and tobacco use presented with acute onset shortness of breath 4-5 days prior to admission the patient developed flu-like symptoms with fatigue, myalgias, back and shoulder pain, and shortness of breath On the morning of admission the patient developed acute worsening of her shortness of breath so she presented to the emergency department 12

13 PRESENTATION The patient s vital signs upon arrival to the emergency department were notable for a systolic blood pressure of 90 mmhg and an oxygenation saturation of 70% on RA Physical exam was notable for a III/VI holosystolic murmur heard over the apex, coarse rhonchi R>L, and mottled cold extremities Initial lab work was notable for a lactate of 14.8 mmol/l, central venous 02 Sat 85.8%, troponin T of 3.53 ng/ml, and a WBC of K/uL 13

14 PRESENTATION The patient was diagnosed with septic shock from a right lower lobe pneumonia and started on ceftriaxone and azithromycin Over the next 6 hours the patient developed worsening hypoxemic respiratory failure and hypotension She was sent for a PE protocol CT scan of the chest which showed: no evidence of pulmonary embolism or aortic dissection and extensive groundglass opacities, worst at the right lower lobe, consistent with multifocal pneumonia A TTE was requested to evaluate cardiac function 14
15 15
16 16
17 17
18 WHAT WOULD YOU RECOMMEND AS THE NEXT STEP IN THE MANAGEMENT OF THIS PATIENT? 18
19 19
20 20
21 21

22 PAPILLARY MUSCLE RUPTURE Epidemiology and Natural History: Accounts for approximately 5% of all deaths after myocardial infarction Most often occurs 2-7 days after myocardial infarction Posteromedial papillary muscle is affected 6-12x more often than the anterolateral papillary muscle secondary to differences in blood supply (posteromedial papillary muscle is supplied by the PDA, anterolateral papillary muscle is supplied by the LAD/LCx) 50% of patients have single-vessel disease and for most patients it occurs with their first myocardial infarction 22
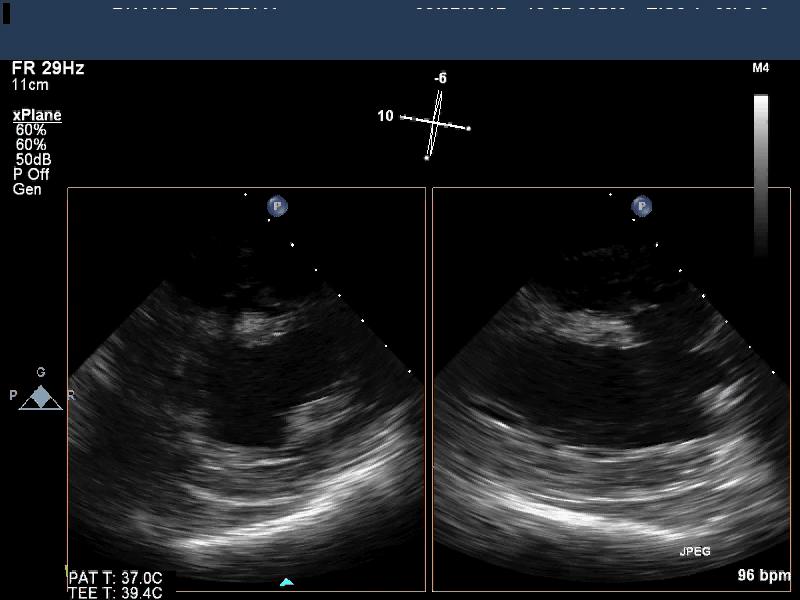
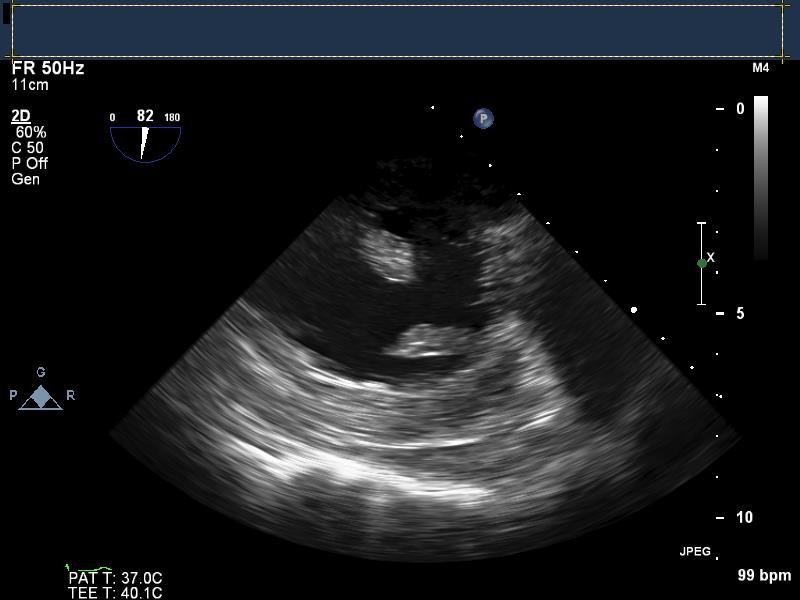
23 PAPILLARY MUSCLE RUPTURE Clinical Manifestations: Chest pain and/or shortness of breath Tachycardia, hypotension and hypoxemic respiratory failure with an inability to lie flat Asymmetric pulmonary edema New, mid/late/holosystolic murmur with widespread radiation End-organ malperfusion (renal failure, shock liver, mottled cold extremities) PAPILLARY MUSCLE RUPTURE Diagnosis: Suspected on TTE based on the presence of a hyperdynamic left ventricle, flail mitral valve, eccentric severe mitral regurgitation, and freely mobile chordae or papillary muscle in the left ventricle Ruptured papillary muscle can often be best visualized by TEE 23
 CLINICAL COURSE Approximately 24 hours after presentation the patient was taken to the operating room for mitral valve replacement and coronary artery bypass grafting")
24 PAPILLARY MUSCLE RUPTURE Treatment: Medical: vasodilators, diuretics, IABP (75% mortality at 24 hours, 95% mortality at 2 weeks) Surgical: mitral valve repair/replacement +/- coronary artery bypass grafting (50% mortality) CLINICAL COURSE Approximately 24 hours after presentation the patient was taken to the operating room for mitral valve replacement and coronary artery bypass grafting (SVG-RCA) 24
25 CLINICAL COURSE Despite surgical intervention the patient continued to have multi-organ failure including cardiogenic shock requiring multiple inotropes After extensive discussions with the patient s family, the decision was made to withdrawal support and the patient passed away CASE 3 25
26 PRESENTATION 71 yo male with a past medical history of hypertension and tobacco use presented with substernal chest pain One day prior to presentation the patient developed substernal chest pain that radiated to the back After the symptoms had not resolved by the next morning, the patient presented to the emergency room for evaluation PRESENTATION The patient s vital signs and physical exam on presentation were within normal limits The patient s initial troponin T was negative 26
27 27

28 28
29 29
30 30

31 THIS PATIENT S ECHOCARDIOGRAPHY FINDING IS MOST LIKELY TO BE CAUSED BY AN OCCLUSION IN WHICH CORONARY ARTERY? 31
32 PRESENTATION The patient was sent for a cardiac catheterization which showed: diffuse nonobstructive disease in the RCA, 50% proximal and 60% distal LAD stenoses, 100% occlusion of OM1, and patent OM2 and OM3 PSEUDOANEURYSM Epidemiology and Natural History: Ventricular free wall rupture that is contained by localized pericardium, adhesions, and/or thrombus (does not contain endocardium or myocardium) Most commonly seen in the inferior or inferolateral wall after myocardial infarction 30%-45% risk of rupture without surgical repair 32
33 PSEUDOANEURYSM Clinical Manifestations: Chest pain and/or shortness of breath Sudden cardiac death (3% of patients) Asymptomatic (12% of patients) New to-and-fro murmur representing flow into and out of the pseudoaneurysm during systole and diastole, respectively Systemic embolization New mass on CXR EKG changes with nonspecific TWI being the most common (95% of patients) PSEUDOANEURYSM Diagnosis: Transthoracic echocardiography only has a sensitivity of 26% Transesophageal echocardiography has a sensitivity of 75% Cineventriculography, cardiac CT, and cardiac MRI all have a high sensitivity and are the imaging tests of choice to confirm the diagnosis Typically has a narrow neck appearance on cardiac imaging (neck diameter <40% of the maximal aneurysm diameter) 33
34 PSEUDOANEURYSM Treatment: Surgical repair or patch closure (<10% perioperative mortality) CLINICAL COURSE The patient was taken to the operating room where he underwent a pseudoaneurysm patch repair and coronary artery bypass grafting with SVG-LAD The patient has done well post-operatively 34
35 CASE 4 PRESENTATION 82 yo male with a past medical history of peripheral arterial disease, hypertension, hyperlipidemia, type II diabetes, tobacco use and atrial fibrillation presented with chest pain 1 day prior to presentation the patient developed an achy pain in his chest that radiated down both of his arms When the patient s symptoms persisted the next day, he presented to the emergency department for evaluation 35


36 PRESENTATION The patient s vital signs upon arrival to the emergency department were: T: 98.8, HR: 134, BP: 145/69, RR: 38, Sp02: 93% on 2L NC The patient s physical exam was notable for an irregularly irregular rhythm and diminished lower extremity pulses Initial lab work was notable for an elevated troponin T of 2.35 ng/ml 36
37 37

38 PRESENTATION Attempts at revascularization of the LAD were unsuccessful and the patient was admitted to the cardiac intensive care unit for further monitoring and medical management The patient remained asymptomatic and had a repeat EKG on hospital day 3 38

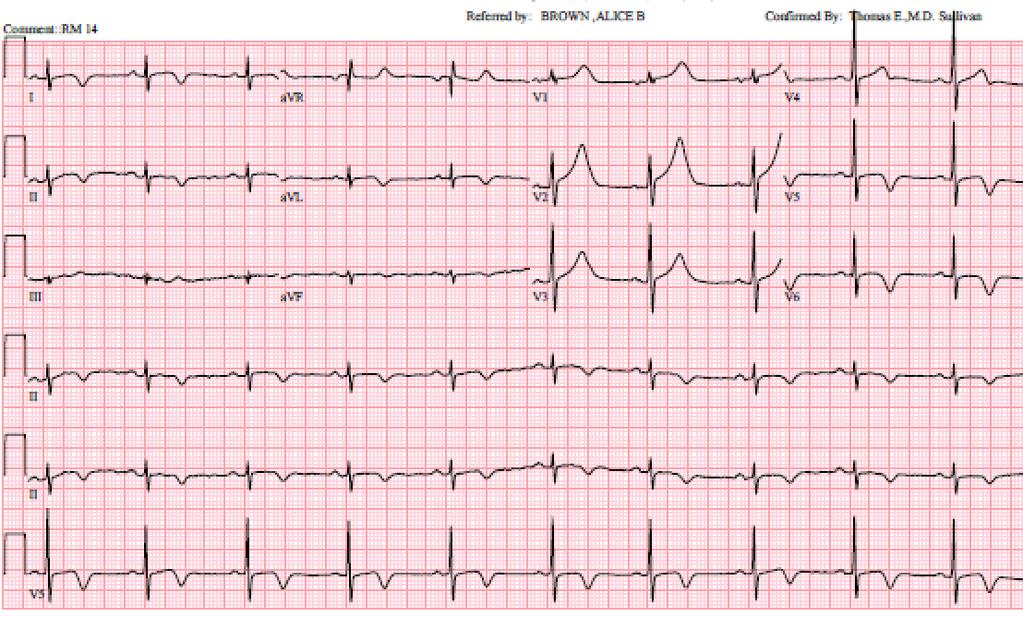
39 WHAT ECHOCARDIOGRAPHIC ABNORMALITY WOULD YOU EXPECT TO FIND BASED ON THE PATIENT S EKG? 39
40 40
41 41
42 LV THROMBUS Epidemiology and Natural History: Occurs in 4%-8% of myocardial infarctions Occurs because of stasis and the procoagulant effects of fibrotic/necrotic myocardium Most thrombi form within the first two weeks following myocardial infarction Highest risk of embolization in the first 3-4 months following myocardial infarction Most common in the anteroapical location following large anterior STEMIs Risk factors: LAD occlusion, EF<30%, long delay between symptom onset and reperfusion LV THROMBUS Clinical Manifestations: Most are asymptomatic and diagnosed on screening transthoracic echocardiogram following myocardial infarction Systemic embolization 42
43 LV THROMBUS Diagnosis: Transthoracic echocardiography is the initial test of choice though thrombi can be difficult to visualize because they may have a similar acoustic appearance to normal myocardium and/or the apex may be obscured by near field artifact The sensitivity of transthoracic echocardiography is increased to 64% with the use of contrast Increased mobility and protrusion into the LV cavity on transthoracic echocardiogram have been associated with an increased risk of embolization Gold standard is cardiac MRI LV THROMBUS Treatment: No treatment: 10-15% risk of embolization Medical: anticoagulation with warfarin, usually for 3-4 months following myocardial infarction (86% reduction in the risk of embolization) 43
44 CLINICAL COURSE The patient was medically managed with aspirin, ticagrelor, warfarin, atorvastatin, and metoprolol On hospital day 4 the patient had an abrupt episode of hypotension with systolic blood pressure in the 70s that resolved with IV fluids 6 hours later the patient suffered a PEA arrest. CPR was performed for 35 minutes without return of spontaneous circulation and the patient was pronounced dead BASED ON THE PATIENT S PRESENTATION, WHAT IS THE MOST LIKELY CAUSE OF DEATH? 44
45 THANK YOU Dr. Noreen Kelly Dr. Michael Picard Dr. Danita Sanborn Dr. Rory Weiner Dr. David Dudzinski 45
NOT ANOTHER TALK ABOUT A - FIB
 NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
NOT ANOTHER TALK ABOUT A - FIB CASES KUDOS AND A CHALLENGE Case 1 67 y/o female s/p R mastectomy 3 months earlier Second course of adjuvant chemotherapy Muga scan E.F. 35% What do we do next? Case 1 Cardiology
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Complications of Myocardial Infarction
 Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
What is Your Diagnosis?
 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One
 Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI).
 Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI).") 1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI). 5- cardiogenic shock (massive MIs >40% of the left ventricle)
1) Severe, crushing substernal chest pain 2) radiate to the neck, jaw, epigastrium, or left arm. 3- rapid and weak pulse 4- nausea (posterior MI). 5- cardiogenic shock (massive MIs >40% of the left ventricle)
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United
 Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Heart disease remains the leading cause of morbidity and mortality in industrialized nations. It accounts for nearly 40% of all deaths in the United States, totaling about 750,000 individuals annually
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
2. Case Report. 1. Introduction
 Case Reports in Cardiology Volume 2016, Article ID 3251032, 5 pages http://dx.doi.org/10.1155/2016/3251032 Case Report Ventricular Septal Perforation after Biventricular Takotsubo Cardiomyopathy Successfully
Case Reports in Cardiology Volume 2016, Article ID 3251032, 5 pages http://dx.doi.org/10.1155/2016/3251032 Case Report Ventricular Septal Perforation after Biventricular Takotsubo Cardiomyopathy Successfully
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
CCRN Review Cardiovascular
 CCRN Review Cardiovascular Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Angina Definition discomfort that occurs when oxygen demand
CCRN Review Cardiovascular Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Angina Definition discomfort that occurs when oxygen demand
You Won t Believe What I Saw on. Disclosures. Goals. Dimensions 2013 October 18 th Michael Pfeiffer, MD. No Financial Disclosures
 You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
Myocardial Infarction
 Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
Myocardial Infarction MI = heart attack Defined as necrosis of heart muscle resulting from ischemia. A very significant cause of death worldwide. of these deaths, 33% -50% die before they can reach the
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome
 Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Acute heart failure in a patient with lower urinary tract infection Case report of an infection-induced Reverse Takotsubo syndrome N.Μoschos, A.Dimitra, E.Tsakiri, D.Stavrianakis, A.Nouli CARDIOLOGY DEPARTMENT
Ischemic Heart Diseases. Dr. Nabila Hamdi MD, PhD
 Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
Ischemic Heart Diseases Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast the different types of angina regarding their pathogenesis, clinical manifestations and evolution. Discuss myocardial infarct,
12 th Annual West Virginia ACC Meeting April 8, 2017
 12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Pulmonary-Vascular Disease. Howard J. Sachs, MD.
 Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Pulmonary-Vascular Disease Howard J. Sachs, MD www.12daysinmarch.com Dyspnea Cardiac Pulmonary CAD Pump Failure Chest Wall Airways Valve Disease Pericardial Disease Alveoli Interstitium Rhythm Disturbance
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
Complications of Acute Myocardial Infarction
 Acute Myocardial Infarction Complications of Acute Myocardial Infarction Diagnosis and Treatment JMAJ 45(4): 149 154, 2002 Hiroshi NONOGI Director, Division of Cardiology and Emergency Medicine, National
Acute Myocardial Infarction Complications of Acute Myocardial Infarction Diagnosis and Treatment JMAJ 45(4): 149 154, 2002 Hiroshi NONOGI Director, Division of Cardiology and Emergency Medicine, National
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS POST MYOCARDIAL INFARCTION
 Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie Vol. XIV Nr. 2 2015 UPDATES ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS
Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie Vol. XIV Nr. 2 2015 UPDATES ANATOMICAL IMAGING USING 3D ECHOCARDIOGRAPHY IN PATIENTS WITH MECHANICAL COMPLICATIONS
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
SUPPLEMENTAL MATERIAL
 SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
SUPPLEMENTAL MATERIAL Table S1: Number and percentage of patients by age category Distribution of age Age
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Coronary arteriography in complicated acute myocardial infarction; clinical and angiographic correlates
 Coronary arteriography in complicated acute myocardial ; clinical and angiographic correlates Luis M. de la Fuente, M.D. Buenos Aires, Argentina From January 1979 to June 30, 1979, we performed coronary
Coronary arteriography in complicated acute myocardial ; clinical and angiographic correlates Luis M. de la Fuente, M.D. Buenos Aires, Argentina From January 1979 to June 30, 1979, we performed coronary
UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R COLEMAN MD, SILVIA E General
 UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R 784945341 COLEMAN MD, SILVIA E General Medicine 72 years 10/2/1945 Female 0210384908200 AROMATORIO Patient is admitted with acute anterior MI, DES stent LAD. Ejection
UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R 784945341 COLEMAN MD, SILVIA E General Medicine 72 years 10/2/1945 Female 0210384908200 AROMATORIO Patient is admitted with acute anterior MI, DES stent LAD. Ejection
Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg
 Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year
![Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year](/thumbs/76/74263761.jpg "Protocol Identifier Subject Identifier Visit Description. [Y] Yes [N] No. [Y] Yes [N] N. If Yes, admission date and time: Day Month Year") PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
PAST MEDICAL HISTORY Has the subject had a prior episode of heart failure? o Does the subject have a prior history of exposure to cardiotoxins, such as anthracyclines? URGENT HEART FAILURE VISIT Did heart
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Radiology of the respiratory/cardiac diseases (part 2)
") Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
Cardiology Cycle - Lecture 6 436 Teams Radiology of the respiratory/cardiac diseases (part 2) Objectives Done By Team Leaders: Khalid Alshehri Hanin Bashaikh Team Members: Leena Alwakeel Aroob Alhuthail
Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm
 CASE REPORT Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm Mariana M. Floria 1, 4, Carmen Elena Pleșoianu 2, 4, Michel Buche 3, Baudouin Marchandise 4, Erwin
CASE REPORT Left ventricle pseudoaneurysm as late postoperative complication of a large apical aneurysm Mariana M. Floria 1, 4, Carmen Elena Pleșoianu 2, 4, Michel Buche 3, Baudouin Marchandise 4, Erwin
Patient Management Conference. John M. Lasala MD PhD Professor of Medicine and Surgery Washington University
 Patient Management Conference John M. Lasala MD PhD Professor of Medicine and Surgery Washington University Disclosures None Case Patient SK 63 y/o man with history of: Atrial fibrillation with RVR, on
Patient Management Conference John M. Lasala MD PhD Professor of Medicine and Surgery Washington University Disclosures None Case Patient SK 63 y/o man with history of: Atrial fibrillation with RVR, on
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult: A Diagnostic Imaging Challenge
 Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
Case Reports in Medicine Volume 2015, Article ID 128462, 4 pages http://dx.doi.org/10.1155/2015/128462 Case Report Sinus Venosus Atrial Septal Defect as a Cause of Palpitations and Dyspnea in an Adult:
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Echo Emergencies. Outline. Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures
 Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
(For items 1-12, each question specifies mark one or mark all that apply.)
") Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Form 121 - Report of Cardiovascular Outcome Ver. 9.2 COMMENTS -Affix label here- Member ID: - - To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: - Central Case No.:
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia
 Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
Marshall University Marshall Digital Scholar Internal Medicine Faculty Research Spring 5-2004 Diversion of the inferior vena cava following repair of atrial septal defect causing hypoxemia Ellen A. Thompson
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since.
 1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
1 2 3 4 5 Chapter 14 Cardiovascular Emergencies Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD)
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Medical Management of Acute Heart Failure
 Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Critical Care Medicine and Trauma Medical Management of Acute Heart Failure Mary O. Gray, MD, FAHA Associate Professor of Medicine University of California, San Francisco Staff Cardiologist and Training
Cardiovascular System
 Cardiovascular System angio BELLWORK Day One: Define using technology hemo/hema cardio Medical Therapeutics Standards 11) Outline the gross normal structure and function of all body systems and summarize
Cardiovascular System angio BELLWORK Day One: Define using technology hemo/hema cardio Medical Therapeutics Standards 11) Outline the gross normal structure and function of all body systems and summarize
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
Can be felt where an artery passes near the skin surface and over a
 1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
1 Chapter 14 Cardiovascular Emergencies 2 Cardiovascular Emergencies Cardiovascular disease has been leading killer of Americans since. Accounts for 1 of every 2.8 deaths Cardiovascular disease (CVD) claimed
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση. Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας
 Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
Οξύ στεφανιαίο σύνδρομο και καρδιογενής καταπληξία. Επεμβατική προσέγγιση Σωτήριος Πατσιλινάκος Κωνσταντοπούλειο Γ.Ν. Ν. Ιωνίας ACUTE HEART FAILURE AND CAD: ACS / LV ischaemic dysfunction Mechanical complications
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Cardiac Mass in a 15-Year-Old Boy
 Cardiac Mass in a 15-Year-Old Boy Echocardiographic Case Report Hortensia Vuçini Department of Cardiology and Cardiac Surgery UHC Mother Theresa Tirana, Albania October 20, 2007 Case Presentation 15 year-old
Cardiac Mass in a 15-Year-Old Boy Echocardiographic Case Report Hortensia Vuçini Department of Cardiology and Cardiac Surgery UHC Mother Theresa Tirana, Albania October 20, 2007 Case Presentation 15 year-old
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic