Diagnosis and Treatment of Pulmonary Embolism. Farzin Ghiasi, MD Pulmonologist August, 2016
|
|
|
- Veronica Gilmore
- 6 years ago
- Views:
Transcription

1

2 Diagnosis and Treatment of Pulmonary Embolism Farzin Ghiasi, MD Pulmonologist August, 2016
3 DVT & PE Hypercoagulable state is characteristic of pregnancy, and DVT occurs in about 1 in 500 pregnancies. In pregnant most unilateral DVTs occur in the left leg because the left ilaic vein is compressed by the right iliac artery and the uterus compresses the IVC.
4






5 VTE: A strong relationship between DVT and PE About 50% of patients with proximal DVT of the leg have asymptomatic PE 1 Migration Embolus DVT (mainly asymptomatic) is found in around 80% of patients with PE 2 Thrombus
6
7
8 VENOUS THROMBOEMBOLISM Deep vein thrombosis and pulmonary embolism Identical pathophysiology Similar risk factors Identical therapeutic goals Similar treatment strategies
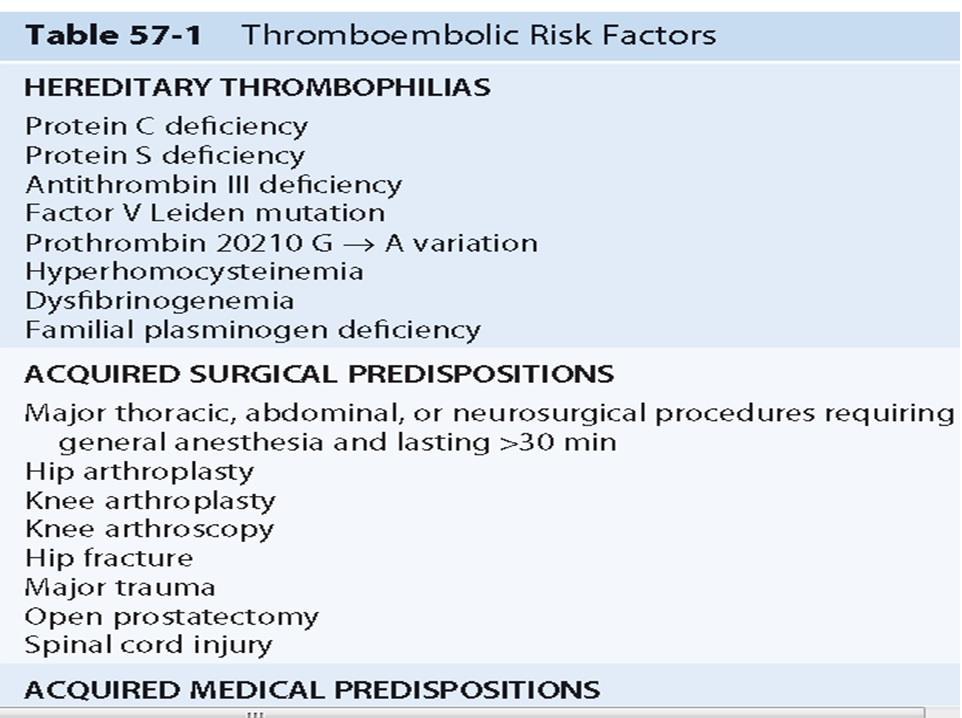
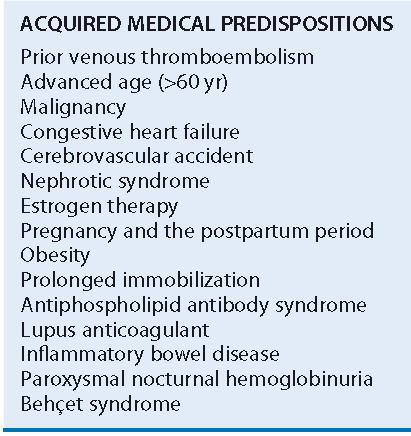
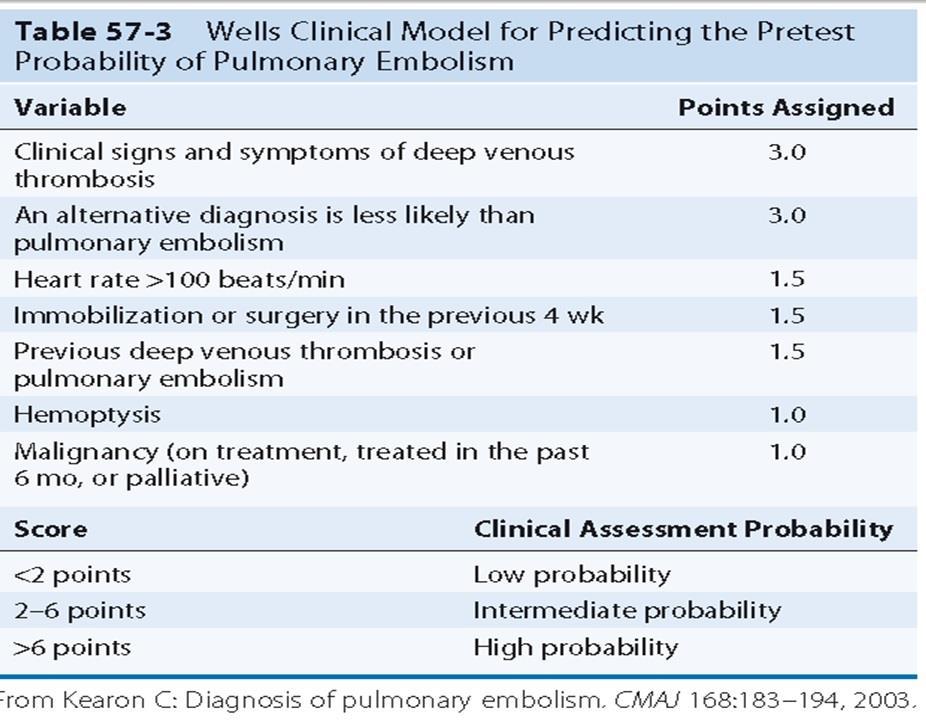
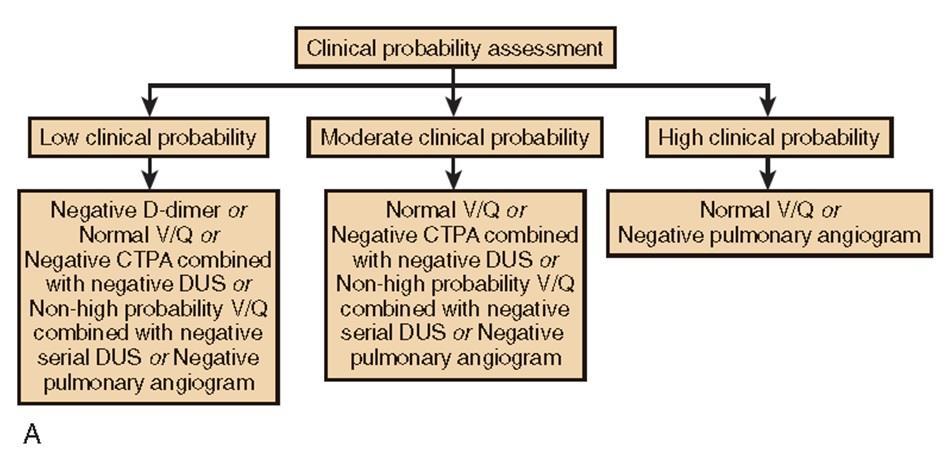
9 DX of PE Clinical history and physical exam. PE cannot be diagnosed or excluded on clinical grounds as symptoms and signs are often nonspecific CXR ECG ABG Perfusion scan D-Dimer Spiral CT scan MRI angiography Echocardiography Pulmonary angiography Cardiac troponin and brain natriuretic peptide. Cardiac enzymes troponin I and T (right ventricular dysfunction). BNP (left ventricular dysfunction, and acute right ventricular overload)
10 Diagnosis of Pulmonary Embolism PE should always be considered whenever unexplained dyspnea is present. Dyspnea, pleuritic chest pain, and hemoptysis are common in PE but, again, are nonspecific. Tachypnea and tachycardia are the most common signs of PE but are also nonspecific.
 due to thrombus in the popliteal and distal")
11 Figure 57-1 Venography for DVT. Contrast venogram shows a large filling defect (arrows) due to thrombus in the popliteal and distal superficial femoral veins. Such thrombi pose substantial embolic risk.

12 Figure 57-2 Compression ultrasonography for DVT. A, Rest and B, compression duplex ultrasonography demonstrates a noncompressible distal superficial femoral vein containing an echogenic mass (arrows), consistent with venous thrombosis.

13 Figure 57-3 Chest radiographs in a patient with pulmonary embolism. A, Opacities caused by atelectasis with edema in the right lower lobe and in the retrocardiac area in a patient with angiographically confirmed pulmonary embolus. B, Two weeks later, the opacities have cleared. (Courtesy Michael Gotway, MD.)

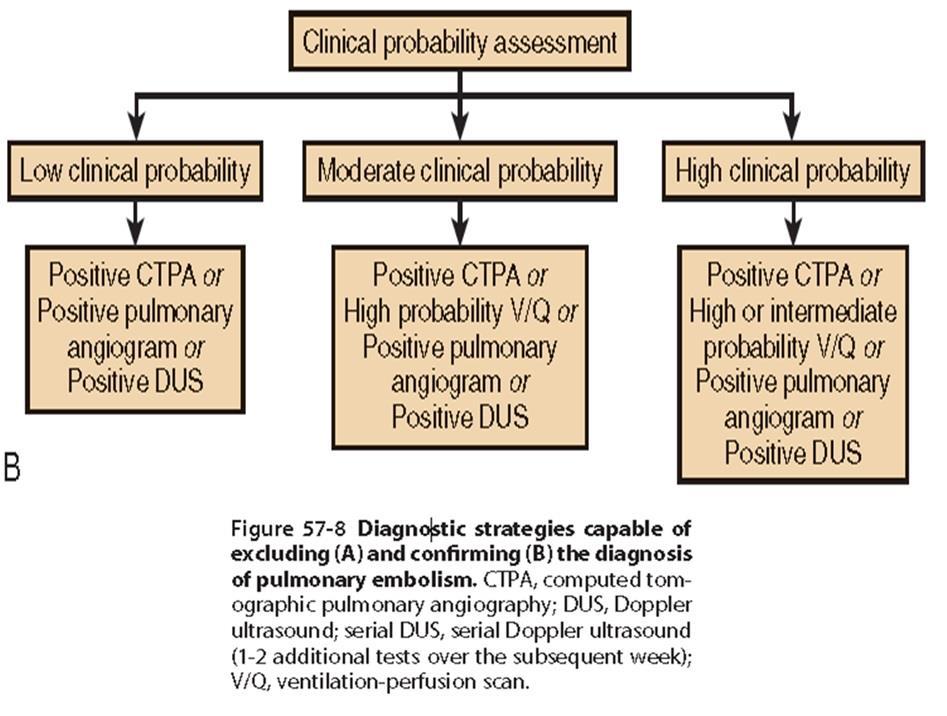
14 Figure 57-4 Normal six-view lung perfusion scan. This finding is capable of excluding the diagnosis of embolism.
 and chest radiograph were normal.")
15 Figure 57-5 Lung perfusion (Q) scan shows major segmental and lobar defects bilaterally. The ventilation scan (not shown) and chest radiograph were normal. This pattern is strongly associated with the presence of embolism.
; right upper lobe emboli (white")
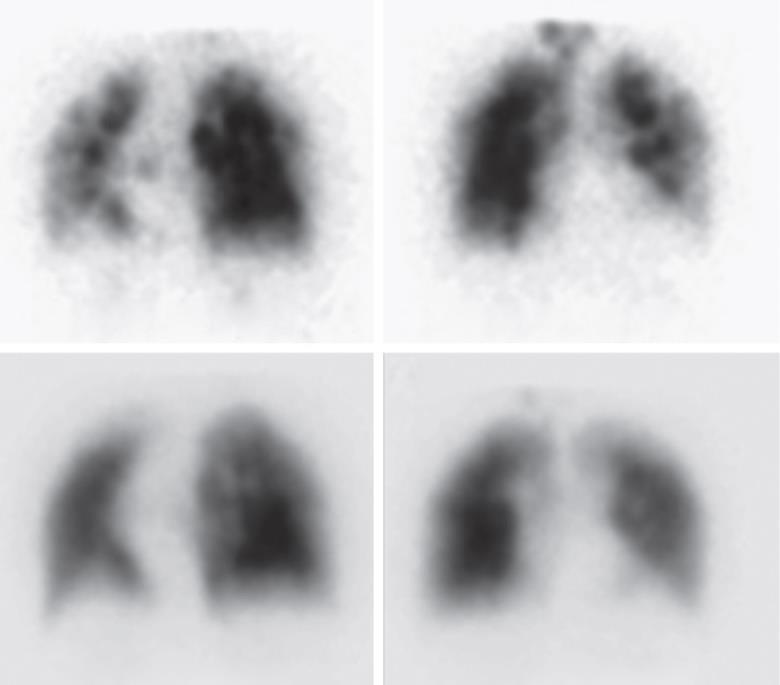
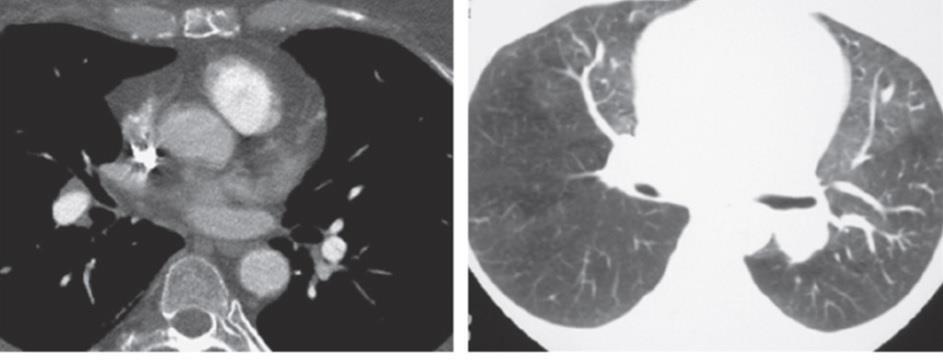
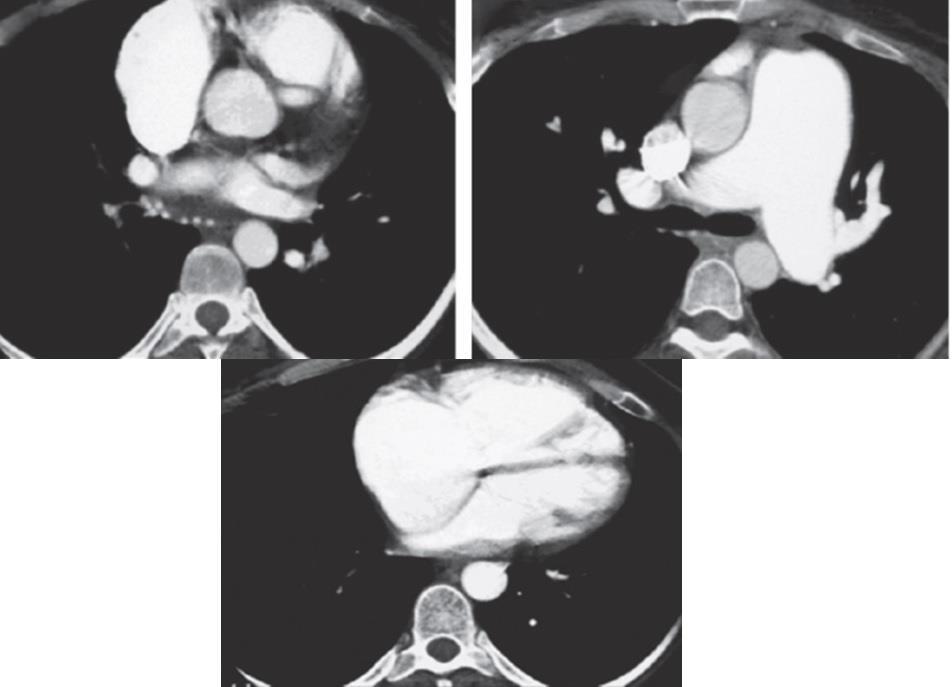
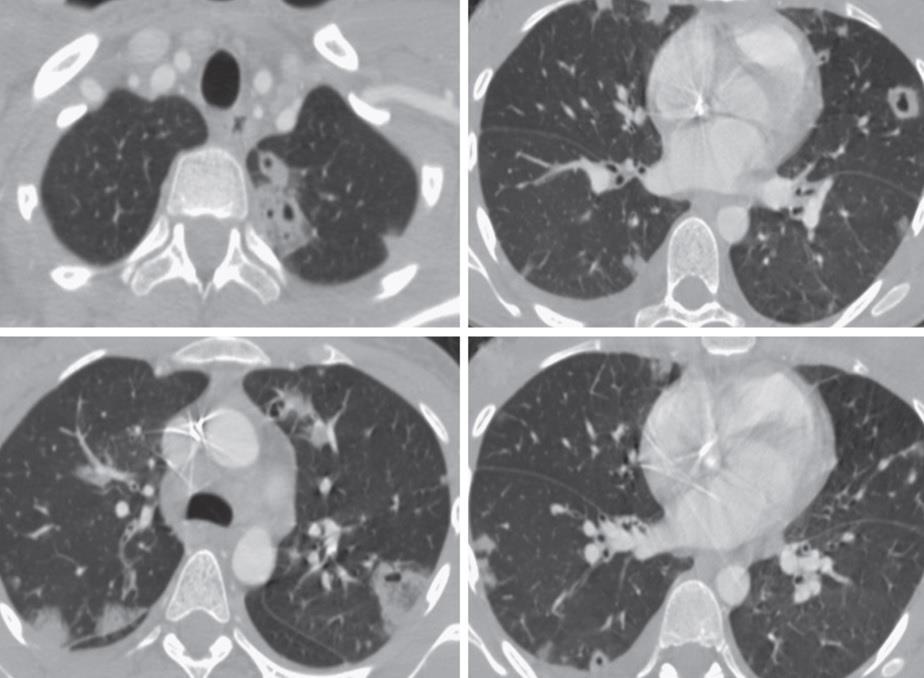
16 Figure 57-6 CT pulmonary angiography of pulmonary embolism. A D, Chest CT pulmonary angiography shows bilateral pulmonary emboli, including a saddle embolism (black arrowheads, B and C); right upper lobe emboli (white arrowheads, A and C), and interlobar emboli (arrows, B D). For a video clip of the full CT study, see Video 57-3.
 and the upper lobe, lingula,")
17 Figure 57-7 Pulmonary angiography for pulmonary embolism. Left-sided pulmonary angiogram shows extensive filling defects within the left pulmonary artery (arrow) and the upper lobe, lingula, and lower lobe arteries, consistent with the diagnosis of pulmonary embolism.
18
19
20

21 Figure Chest radiograph in a patient with chronic thromboembolic pulmonary hypertension. A, Note asymmetry of central pulmonary arteries, absence of descending left pulmonary artery, left lower lobe oligemia, and peripheral opacity representing prior infarct. B, Angiogram in the same patient demonstrates complete proximal occlusion of the descending left pulmonary artery.

22 Figure Rightsided pulmonary angiogram in a patient with chronic thromboembolic pulmonary hypertension.

23 Figure Specimen obtained at the time of pulmonary thromboendarterectomy.

24 Before Thromboendarterectomy Soon After Thromboendarterectomy Figure Perfusion scans show pulmonary artery steal.

25 Figure Chest radiograph shows postoperative reperfusion pulmonary edema.

26 Figure Pulmonary angiography before and after thromboendarterectomy. A, Preoperative pulmonary angiogram shows thromboembolic obstruction involving the right upper, middle, and lower lobe arteries. B, Postoperative angiogram shows nearnormalization of flow. This angiographic improvement was accompanied by a corresponding hemodynamic improvement.

27 efigure 57-1 Ultrasound image of DVT. Longitudinal ultrasound image shows mixed echogenicity material within the popliteal vein, consistent with acute deep venous thrombosis.
 is present with the superficial femoral vein, entering the common femoral vein; thrombus can be seen filling the saphenous vein")
28 efigure 57-2 Color Doppler ultrasound of the lower extremity. A, Normal color Doppler examination of the lower extremity venous and arterial systems. B, Echogenic material representing deep venous thrombosis (arrowheads) is present with the superficial femoral vein, entering the common femoral vein; thrombus can be seen filling the saphenous vein anteriorly at the junction of the superficial and common femoral veins. Note the displacement of color Doppler flow to the periphery of the thrombosed superficial femoral vein.

29 efigure 57-3 Acute deep venous thrombosis presenting as nearly completely anechoic material filling the venous lumen. Note peripheral displacement of color Doppler signal, marking the remaining patent lateral portions of the common femoral vein. Some echogenic thrombus is seen peripherally both anteriorly and posteriorly as well.

30 efigure 57-4 Indirect contrast venography. Axial contrast-enhanced image through the pelvis performed in the course of indirect contrast venography shows a lowattenuation filling defect within the right external iliac vein (arrow), consistent with deep venous thrombosis.

31 efigure 57-5 Indirect contrast venography. Axial contrast-enhanced image through the lower abdomen performed in the course of indirect contrast venography shows a low-attenuation filling defect within the inferior vena cava (arrow), consistent with deep venous thrombosis.
 shown to represent pulmonary infarction.")
32 efigure 57-6 Acute pulmonary embolism. A, Frontal chest radiograph in a patient with acute pulmonary embolism shows a rounded opacity in the peripheral right upper lung (arrow) shown to represent pulmonary infarction. B D, Chest CT pulmonary angiography shows pulmonary emboli in the right upper and interlobar arteries (arrowheads) as well as subpleural, wedgeshaped opacity representing pulmonary infarction (arrows).

33 efigure 57-7 The Westermark sign of pulmonary embolism.

34 efigure 57-8 Acute pulmonary embolism.

35 efigure 57-9 Fleischner and Westermark signs of pulmonary embolism.
 and right ventricle (RV).")
36 efigure Right ventricular enlargement with pulmonary embolism. A, Four-chamber echocardiographic image shows enlargement of the right atrium (RA) and right ventricle (RV). B, Chest CT pulmonary angiography shows bilateral pulmonary emboli (arrows), indicating the cause of the right heart chamber enlargement.
37
 show inhomogeneous ventilation")
38 efigure Chronic thromboembolic disease. A D, Ventilation-perfusion scintigraphy (A and B, ventilation images performed with 133Xenon; C and D, perfusion images performed with 99Tc-macroaggregated albumin) show inhomogeneous ventilation bilaterally, but perfusion images show relatively uniform tracer distribution. The study is consistent with a low probability for pulmonary embolism. E and F, Chest CT pulmonary angiography shows eccentric low-attenuation material (arrows) within the central pulmonary arteries consistent with chronic thromboembolic disease.
; B, Eccentric low-attenuation material along the wall of the affected vessel (arrow); C, Intravascular web")
39 efigure Chronic thromboembolic disease. Chest CT pulmonary angiographic findings of chronic thromboembolic disease. A, Recanalized arterial lumen, showing peripheral hypoattenuating material (arrows); B, Eccentric low-attenuation material along the wall of the affected vessel (arrow); C, Intravascular web (arrowhead); D, Inhomogeneous lung opacity representing areas of oligemia (the areas of decreased attenuation); E, Bronchial artery collateral vessels (arrowheads); F, Main pulmonary artery (MPA) enlargement, consistent with pulmonary hypertension; and G, Enlargement of the right atrium (RA) and right ventricle (RV), consistent with pulmonary hypertension. Note straightening of the interventricular septum, also consistent with elevated right heart pressures.
40
41

42 efigure Pulmonary artery air embolism. A, Frontal and B, lateral chest radiography performed for acute-onset chest pain following manipulation of a central venous catheter shows a gas and fluid level (arrowheads) in the main pulmonary artery. This finding resolved without sequelae.
,")
 shows progression in size of the nodular opacities (arrows).")
43 efigure Septic embolization. A, Frontal chest radiography performed in an intravenous drug user with fever shows multiple, bilateral, poorly defined nodular opacities (arrows), one of which is cavitary (arrowhead). B, Frontal chest radiography performed 2 years earlier, for comparison, appears normal. C, Frontal chest radiography performed one day following (A) shows progression in size of the nodular opacities (arrows). D-G, Axial-enhanced chest CT confirms the presence of multiple, bilateral, peripherally distributed nodules (arrows), many of which are cavitary (arrowheads).
44
 with small foci of methyl")
45 efigure Methyl methacrylate pulmonary emboli following vertebroplasty. Oblique frontal image of the chest shows thoracic spine vertebroplasty material (arrows) with small foci of methyl methacrylate emboli in the right upper lobe (arrowheads).

46 Methyl methacrylate pulmonary emboli following vertebroplasty.
47 A, Frontal chest radiograph shows thoracic spine vertebroplasty material (arrows) with a small curvilinear focus of methyl methacrylate in the right interlobar pulmonary artery (arrowhead).

48 C, Axial unenhanced chest CT confirms high attenuation in the right interlobar pulmonary artery (arrows), representing a methyl methacrylate embolism. Methyl methacrylate is also present in the azygos vein (arrowheads).
49
50
51
52
53 MANAGEMENT OF VENOUS THROMBOEMBOLISM
54 UNFRACTIONATED HEPARIN AND LOWMOLECULAR-WEIGHT HEPARIN Heparin, both unfractionated and LMWH, remains the mainstay of therapy for venous thrombosis and for PE not associated with hemodynamic compromise. With a strong suspicion of embolism based on clinical findings and laboratory tests, heparin therapy should be instituted immediately, without awaiting diagnostic confirmation unless anticoagulation places the patient at significant risk.
55 Data suggest that physician practices in the administration of unfractionated heparin often result in levels of anticoagulation that fall below those currently recommended in the literature. To overcome these problems, standardized protocols for heparin administration and monitoring have been recommended.
56 A number of different intravenous heparin dosing schemes have been published, all of which have demonstrated the potential to reach a therapeutic threshold more rapidly than a nonstandardized approach. The most widely utilized of these is a weightbased system that includes an 80 unit/kg intravenous bolus of heparin followed by an 18 unit/kg/hr infusion.
57 Whatever regimen is used, an activated partial thromboplastin time (a PTT) is generally obtained 6 hours after the bolus dose, 6 hours after each prescribed dose adjustment, and then on a daily basis for the duration of therapy.
58 Because maintenance of the a PTT within a rigidly defined range does not appear to increase the efficacy or safety of the drug, frequent dosage adjustments are not necessary once the dose has been stabilized within a therapeutic range. This therapeutic range of a PTT, which corresponds to heparin levels of 0.2 to 0.4 unit/ml by protamine sulfate titration or 0.3 to 0.7 unit/ml by anti-factor Xa assay, may vary substantially depending on the sensitivity of the reagent utilized and among coagulation analyzers.
59 Given the variance in a PTT values possible with different reagents and analyzers, individual institutional validation should be performed to define a therapeutic a PTT value. It also should be recognized that heparin requirements tend to decrease during the course of therapy, resulting in an increase in the level of the a PTT.
60 For patients with heparin resistance (defined as the need for >40,000 units/day), monitoring heparin with an antifactor Xa assay appears safe and effective and results in less escalation of the heparin dose than monitoring with the a PTT.
61 Interestingly, supratherapeutic a PTT values are not associated with an increased risk of clinically important bleeding complications. There is no direct evidence that the absolute dose of heparin or the level of the a PTT can predict the likelihood of bleeding. Instead, bleeding during heparin therapy appears to be related to the presence of concurrent illness such as renal disease, a history of heavy alcohol consumption, aspirin use, and prior surgical procedures or peptic ulcer disease.
62 Thus these data encourage adequate use of heparin doses. In fact, failure to treat patients early with sufficient heparin doses appears to have longterm and short-term implications for thromboembolic recurrence. It is somewhat controversial, however, whether the a PTT level itself, independent of the heparin dose, is associated with higher recurrence rates or whether it is strictly a matter of insufficient dosing itself.
63 Subcutaneous LMWHs are widely used for the treatment of VTE because of their high bioavailability and longer halflife, which allows the strategy of dosing once or twice daily, with adjustment for weight but without the need for adjustment by a PTT monitoring. Indeed, the same strategy is appropriate for subcutaneous (unfractionated) heparin as well, administered in high doses.
64 An approach utilizing a fixed dose of subcutaneous unfractionated heparin, administered as an initial dose of 333 U/kg followed by a dose of 250 U/kg every 12 hours, has been demonstrated to be as safe and effective as LMWH in patients presenting with venous thrombosis and PE. Clinicians must recognize that the administration of LMWH may not be preferable under certain clinical circumstances.
65 Standardized dosing can be a problem in patients at the extremes of body weight; Because the drug is renally cleared, dose adjustments and monitoring with anti-factor Xa levels are necessary in patients with renal insufficiency; The anticoagulant effect of the drug cannot be monitored easily; populations exist (e.g., patients at high bleeding risk) in which a longer drug halflife is not a desirable effect; The ability of protamine sulfate to reverse the anticoagulant effect remains uncertain; Drug costs are substantially higher than with unfractionated heparin.
66 Clinical trials have demonstrated that the safety and efficacy of LMWH preparations are comparable with those of unfractionated heparin in patients with venous thrombosis. In selected patients, fixed-dose subcutaneous LMWH appears to be safer and more effective than intravenous adjusted-dose unfractionated heparin. However, fixeddose subcutaneous LMWH appears to be comparable with subcutaneous unfractionated heparin, either in adjusted doses or fixed doses.
67 Trials have also demonstrated that most patients with acute venous thrombosis can be treated safely on an outpatient basis with LMWH and that outpatient therapy can reduce total medical expenditure. However, not all patients with venous thrombosis can or should be treated in an outpatient setting. Approximately 50% of patients are ineligible for outpatient therapy owing to such factors as major bleeding risk, compliance problems, renal failure, significant comorbid disease, inadequate cardiopulmonary reserve, and inaccessibility for follow-up.
68 Furthermore, embolism can happen during the early aspects of therapy in patients treated with both unfractionated and LMWH preparations. Although this circumstance would not be diminished in an inpatient setting, the potential consequences of recurrence, especially in patients with preexisting cardiopulmonary disease, might be more promptly detected and managed in this setting.
69 The Hestia Study demonstrated the feasibility of outpatient therapy for acute PE patients who are hemodynamically stable (without perceived need for thrombolysis or embolectomy), At low risk for bleeding, Not hypoxemic, Free of severe liver or kidney dysfunction, Without severe pain or other reason for hospital admission Who did not develop PE while on anticoagulants or while pregnant.
70 About one quarter of the patients who met these criteria were briefly admitted for evaluation and discharged in less than 24 hours. The Hestia criteria for outpatient therapy appear to be useful even in patients with CTPA evidence of enlarged right ventricular dimensions, provided they are otherwise hemodynamically stable. Even in patients who require initial inpatient management, the duration of hospitalization can be decreased considerably by a quick transition to outpatient therapy as their conditions stabilize.
71 In terms of duration of heparin/lmwh therapy, studies have shown that utilizing a 5-day course of therapy in patients with proximal venous thrombosis is associated with a recurrence rate identical to that of a 10-day course. This assumes, of course, that warfarin is started early and is in a therapeutic range for 2 consecutive days before heparin is discontinued, a target often difficult to achieve. It is likely that a short course of heparin therapy would be similarly effective in patients with uncomplicated PE.
72 However, a longer course of therapy is advisable in patients with major PE or extensive iliofemoral venous thrombosis. The major complications of unfractionated heparin and LMWH are bleeding and the development of thrombocytopenia.
73 There are no predisposing factors to heparin associated thrombocytopenia other than a history of a previous exposure, and it develops at the same frequency with either (unfractionated) heparin or LMWH.
74 Two types of thrombocytopenia are associated with heparin administration: An early-onset (1-5 days), non immunemediated reduction in platelet count (type I) believed to be secondary to a direct agglutinating effect of heparin on platelets A late-onset ( 4 days), immune-mediated thrombocytopenia (type II) that may be associated with venous and arterial thrombosis.
75 Immune-mediated thrombocytopenia can also arise within a day of initiating therapy in patients who have been exposed to the drug within the prior 100 days. The incidence of thrombosis with heparinassociated thrombocytopenia appears to be low, but when it happens, it is associated with considerable morbidity and mortality.
76 Therefore heparin should be immediately withdrawn if this diagnosis is suspected. If heparin-associated thrombocytopenia type II is confirmed by either a functional assay or an immunoassay, withdrawal of heparin alone may be associated with an adverse outcome. A number of therapeutic alternatives exist, including direct thrombin inhibitors (lepirudin or argatroban), which do not react with heparin antibodies, or danaparoid, which appears to have a low rate of in vivo cross reactivity with heparin. Cross reactivity between unfractionated heparin and LMWH is relatively common, and these drugs should be avoided.
77 FONDAPARINUX Fondaparinux is effective and safe for the initial treatment of PE and of DVT. The dosing regimen used in these trials was straightforward: 7.5 mg subcutaneously once daily in patients who weighed from 50 to 100 kg (85% of cases). The dose was decreased to 5 mg in patients weighing less than 50 kg and increased to 10 mg in those weighing more than 100 kg. As is the case for unfractionated heparin and LMWH, the treatment was continued for at least 5 days, during which time warfarin was administered.
78 After 5 days and once warfarin was therapeutic, treatment with fondaparinux was stopped. In a doubleblinded randomized trial for the treatment of acute proximal lower extremity DVT, this regimen was as effective in preventing recurrent symptomatic VTE as enoxaparin, 1 mg/kg body weight twice per day. A randomized, open-label clinical trial compared the same fondaparinux treatment regimen with intravenous unfractionated heparin (using standard a PTTdriven dosage adjustments) for the treatment of pulmonary embolism.
79 The outcomes of the two treatments appeared identical: the fondaparinux and standard therapy groups did not significantly differ with respect to the incidence of recurrent VTE, bleeding, overall mortality, or mortality due to PE. It is noteworthy that fondaparinux may accumulate to dangerous levels in patients with renal insufficiency because of its near total renal clearance.
80 DIRECT INHIBITORS OF FACTOR Xa AND OF THROMBIN Rivaroxaban is a synthetic inhibitor of Xa that can be used in the acute phase of VTE treatment. It differs from the parenteral agents (unfractionated, LMWH, and fondaparinux) in that it is a direct inhibitor. For this reason, it does not depend on the body s antithrombin in order to inactivate thrombosis.
81 Another important difference is that it is well absorbed when given orally. Rivaroxaban is safe and effective for the treatment of the acute phase, as well as the 3-month follow-up phase of treatment for PE and for DVT. However, the acute phase of VTE treatment with rivaroxaban lasts for 3 weeks, as opposed to the shorter acute phase used with parenteral agents.
82 The high bioavailability and pharmacokinetic predictability of once- or twice-daily oral rivaroxaban, as well as the safety of using it without the need for adjustment by INR values, is advantageous. Rivaroxaban is cleared by both renal and hepatic routes, including cytochrome P450- mediated metabolism. In the trials listed earlier, patients with severe renal or hepatic dysfunction were excluded. There are also potential drug interactions with agents that inhibit cytochrome P4503A4, such as azole compounds or HIV-protease inhibitors.
83
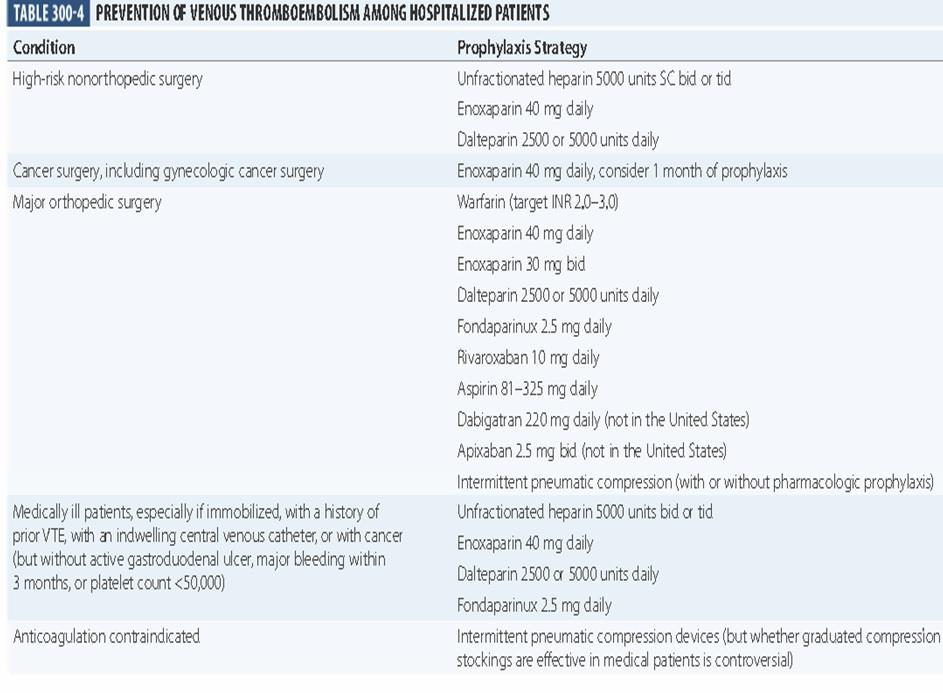
84 INFERIOR VENA CAVA FILTERS Scientific evidence supporting the use of inferior vena cava filters is limited. Established indications for filter placement in the therapy of VTE include 1) protection against PE in patients with acute VTE in whom conventional anticoagulation is contraindicated (recent surgery, hemorrhagic cerebrovascular accident, active bleeding, heparin-associated thrombocytopenia, etc.); 2) protection against PE in patients with acute VTE in whom conventional anticoagulation has proved ineffective;
85 3) protection of an already compromised pulmonary vascular bed from further thromboembolic risk (massive PE, chronic thromboembolic pulmonary hypertension). In support of the third indication is the recent review of a national inpatient database that disclosed that unstable PE patients who received inferior vena cava (IVC) filters had higher survival rates than those who did not receive them.
86 Mortality from filter placement appears to be quite low regardless of what filter is used. Nonfatal complications of IVCs include 1) complications relating to the insertion process, 2) venous thrombosis at the site of insertion, 3) filter migration, 4) filter erosion through the inferior vena cava wall, 5) inferior vena cava obstruction. The majority of clinically important complications appear to involve venous thrombosis at the insertion site and inferior vena cava obstruction.
87 Filter placement should not be considered as the sole therapy for VTE unless an absolute contraindication to anticoagulation exists. Although protecting the pulmonary vascular bed, filter placement does not inhibit the extension of existing venous thrombi or diminish the systemic prothrombotic state.
88 Small thrombi can pass through patent filters or through collaterals around obstructed filters; furthermore, thrombus can extend through the filter itself. One study demonstrated that placement of a vena cava filter was capable of diminishing the incidence of early PE. The benefit was somewhat offset by an increased risk of recurrent DVT within 2 years, although an 8-year follow-up did not disclose an increased risk of recurrence or postthrombotic syndrome.
89 The development of retrievable filters suggests that the intervention will no longer be irreversible, although extensive randomized clinical trials have not yet been performed to establish the safety and efficacy of this strategy. Given these considerations, long-term anticoagulation should be placement if no contraindications exist or as soon as any utilized following filter existing bleeding risk resolves.

90
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT)
") HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) OBJECTIVE: To assist clinicians with the investigation and management of suspected and documented heparin-induced thrombocytopenia (HIT). BACKGROUND: HIT is a transient,
DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS
 TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
TOKUDA HOSPITAL SOFIA DOPPLER ULTRASOUND OF DEEP VENOUS THROMBOSIS MILENA STANEVA, MD, PhD Department of vascular surgery and angiology Venous thromboembolic disease continues to cause significant morbidity
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Clinical Guide - Suspected PE (Reviewed 2006)
") Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
REVIEW ON PULMONARY EMBOLISM
 REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous Thromboembolism National Hospital Inpatient Quality Measures
 Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Venous Thromboembolism National Hospital Inpatient Quality Measures Presentation Overview Review venous thromboembolism as a new mandatory measure set Outline measures with exclusions and documentation
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Diagnosis and management of pulmonary embolism
 Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
A A U
 PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
University Journal of Medicine and Medical Specialities
 University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
Supplementary Online Content
 Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Supplementary Online Content Mismetti P, Laporte S, Pellerin O, Ennezat P-V, Couturaud F, Elias A, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone
Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C
 Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C ABSTRACT Acute pulmonary embolism is a life-threatening diagnosis that can present with a multitude of nonspecific symptoms.
Diagnosis and management of acute pulmonary embolism Bobbie Morici, MSPAS, PA-C ABSTRACT Acute pulmonary embolism is a life-threatening diagnosis that can present with a multitude of nonspecific symptoms.
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Jordan M. Garrison, MD FACS, FASMBS
 Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Jordan M. Garrison, MD FACS, FASMBS Peripheral Arterial Disease (PAD) Near or Complete obstruction of > 1 Peripheral Artery Peripheral Venous reflux Disease Varicose Veins Chronic Venous Stasis Ulcer Disease
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range
 Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range") Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Deep Vein Thrombosis
 Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
Deep Vein Thrombosis from NHS (UK) guidelines Introduction Deep vein thrombosis (DVT) is a blood clot in one of the deep veins in the body. Blood clots that develop in a vein are also known as venous thrombosis.
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Pulmonary embolism - the great masquerader
 Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Anticoagulant Therapy During Pregnancy
 Anticoagulant Therapy During Pregnancy AIM - June 2007 Russell K. Laros, Jr., MD Thromboembolism and Pregnancy Leading Non-Obstetrical Cause of Maternal Mortality Early recognition and proper treatment
Anticoagulant Therapy During Pregnancy AIM - June 2007 Russell K. Laros, Jr., MD Thromboembolism and Pregnancy Leading Non-Obstetrical Cause of Maternal Mortality Early recognition and proper treatment
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Venous Thromboembolism (VTE)
") Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
Venous Thromboembolism (VTE) Nursing A guide for patients and carers Contents Why do blood clots form in veins?... 1 How common is a deep vein thrombosis (DVT) or pulmonary embolus (PE)?... 2 How are DVTs/
Radiation Exposure in Pregnancy. John R. Mayo UNIVERSITY OF BRITISH COLUMBIA
 Radiation Exposure in Pregnancy John R. Mayo UNIVERSITY OF BRITISH COLUMBIA Illustrative Clinical Scenario 32 year old female 34 weeks pregnant with recent onset shortness of breath and central chest pain
Radiation Exposure in Pregnancy John R. Mayo UNIVERSITY OF BRITISH COLUMBIA Illustrative Clinical Scenario 32 year old female 34 weeks pregnant with recent onset shortness of breath and central chest pain
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension. Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA
 Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Surgical Management in Chronic Thromboembolic Pulmonary Hypertension Michael Bates, MD, FACS Ochsner Health System, New Orleans, LA Disclosures No industry conflicts I am a surgeon and always disclose
Diagnosis of Venous Thromboembolism
 Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Diagnosis of Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD MScCH, University of
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Hemodynamic Disorders, Thrombosis, and Shock. Richard A. McPherson, M.D.
 Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Hemodynamic Disorders, Thrombosis, and Shock Richard A. McPherson, M.D. Edema The accumulation of abnormal amounts of fluid in intercellular spaces of body cavities. Inflammation and release of mediators
Pulmonary embolism. Paweł Balsam MD, PhD
 Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel)
") New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
New Antithrombotic and Antiplatelet Drugs in CAD : (Factor Xa inhibitors, Direct Thrombin inhibitors and Prasugrel) Limitations and Advantages of UFH and LMWH Biological limitations of UFH : 1. immune-mediated
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Pulmonary Embolism..Diagnostic Approach and Algorithm. Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD
 Pulmonary Embolism..Diagnostic Approach and Algorithm Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD Epidemiology of Pulmonary Embolism Pulmonary Embolus (PE): Thrombus originating
Pulmonary Embolism..Diagnostic Approach and Algorithm Tolulope Adesiyun Harvard Medical School, Year III Gillian Lieberman, MD Epidemiology of Pulmonary Embolism Pulmonary Embolus (PE): Thrombus originating
What You Should Know
 1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
1 New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know New 2018 ASH Clinical Practice Guidelines on Venous Thromboembolism: What You Should Know The American Society
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Clinical Policy: Dalteparin (Fragmin) Reference Number: ERX.SPA.207 Effective Date:
 Reference Number: ERX.SPA.207 Effective Date:") Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Fragmin) Reference Number: ERX.SPA.207 Effective Date: 01.11.17 Last Review Date: 02.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
ED Diagnosis of DVT or tools to rule out DVT in your ED
 ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
ED Diagnosis of DVT or tools to rule out DVT in your ED Ralph Wang UCSF Department of Emergency Medicine 53 yo f c/o left leg swelling recent cholecystectomy its midnight how do you manage this patient?
Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT)
") ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
ASH CLINICAL PRACTICE GUIDELINES VENOUS THROMBOEMBOLISM (VTE) POCKET GUIDE Diagnosis and Management of Heparin-Induced Thrombocytopenia (HIT) A POCKET GUIDE FOR THE CLINICIAN DECEMBER 08 Allyson M. Pishko,
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION
 IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
IVC FILTERS: A CASE REPORT REVIEWING THE INDICATIONS FOR PLACEMENT, RETRIEVAL AND ANTICOAGULATION Resident(s): George Athanasatos Attending(s): Daniel Golwyn Program/Dept: Interventional Radiology CHIEF
MDCT and Pulmonary Embolism. Heber MacMahon The University of Chicago Department of Radiology
 MDCT and Pulmonary Embolism Heber MacMahon The University of Chicago Department of Radiology https://tinyurl.com/hmpe2018 Disclosures Consultant for Riverain Medical Minor stockholder in Hologic, Inc.
MDCT and Pulmonary Embolism Heber MacMahon The University of Chicago Department of Radiology https://tinyurl.com/hmpe2018 Disclosures Consultant for Riverain Medical Minor stockholder in Hologic, Inc.
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015
 Clinical Practice Guideline August 2015") Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Outpatient Treatment of Deep Vein Thrombosis with Low Molecular Weight Heparin (LMWH) Clinical Practice Guideline August 2015 General Principles: There is compelling data in the medical literature to support
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Radiologic Features of The Pulmonary Embolus
 January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
Heparin-Induced Thrombocytopenia. Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital
 Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
Pulmonary embolism. Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan
 Pulmonary embolism Objectives: Epidemiology Pathophysiology Diagnosis Massive PE Treatment Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan Team Leader: Nawaf Alkhudhayri
Pulmonary embolism Objectives: Epidemiology Pathophysiology Diagnosis Massive PE Treatment Team Members: Fatima AlTassan, Jawaher abanumy, Abdulrahman thekry, khalid aleidan Team Leader: Nawaf Alkhudhayri
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Diagnosis & Management of Heparin-Induced Thrombocytopenia
 Diagnosis & Management of Heparin-Induced Thrombocytopenia An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng
Diagnosis & Management of Heparin-Induced Thrombocytopenia An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng
Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient
 ...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein
...PRESENTATIONS... Deep Vein Thrombosis and Pulmonary Embolism in the Perioperative Patient Based on a presentation by James E. Muntz, MD Presentation Summary Approximately 500,000 cases of deep vein
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Difficulties of timely diagnosis of the Pulmonary Embolism of patients with chronic obstructive lung disease: possibility MSCT.
 Difficulties of timely diagnosis of the Pulmonary Embolism of patients with chronic obstructive lung disease: possibility MSCT. Poster No.: C-2618 Congress: ECR 2012 Type: Scientific Exhibit Authors: I.
Difficulties of timely diagnosis of the Pulmonary Embolism of patients with chronic obstructive lung disease: possibility MSCT. Poster No.: C-2618 Congress: ECR 2012 Type: Scientific Exhibit Authors: I.
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital
 Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Is it safe to manage pulmonary embolism in Primary Care? Roopen Arya King s College Hospital A few definitions Safe Avoid death, recurrent thrombosis, bleeding Manage Diagnosis + treatment Pulmonary embolism
Severe pulmonary embolism: surgical aspects. Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland
 Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Severe pulmonary embolism: surgical aspects Oliver Reuthebuch Clinic for Cardiac Surgery University Hospital Basel Switzerland Severe pulmonary embolism Acute pulmonary embolism Chronic pulmonary thromboembolism
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
8/16/2012. Pulmonary Embolism
 Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
DENOMINATOR: All surgical patients aged 18 years and older undergoing procedures for which VTE prophylaxis is indicated in all patients
 Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
Measure #23 (NQF 0239): Perioperative Care: Venous Thromboembolism (VTE) Prophylaxis (When Indicated in ALL Patients) National Quality Strategy Domain: Patient Safety 2017 OPTIONS FOR INDIVIDUAL MEASURES:
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL
 PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
PULMONARY EMBOLISM/VTE CARE PROCESS MODEL IMCP FALL CONFERENCE 2017 Scott Stevens, MD Co-Director, Thrombosis Clinic & Thrombosis Research Group Intermountain Medical Center Professor of Clinical Medicine
Treatment of Pediatric Venous Thromboembolism
 Treatment of Pediatric Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD, MScCH, University
Treatment of Pediatric Venous Thromboembolism An Educational Slide Set American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism Slide set authors: Eric Tseng MD, MScCH, University
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Real life management of CTEPH: patient case
 2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
2 nd International Congress on cardiovascular imaging in clinical practice k Real life management of CTEPH: patient case Anastasia Anthi Pulmonary Hypertension Clinic, Attikon University Hospital, Athens
Venous Thromboembolism: Deep Venous Thrombosis and Pulmonary Embolism
 Venous Thromboembolism: Deep Venous Thrombosis and Pulmonary Embolism MD Cardiovascular Interventions Orlando Objectives Recognize common presentations of deep venous thrombosis (DVT) and pulmonary embolus
Venous Thromboembolism: Deep Venous Thrombosis and Pulmonary Embolism MD Cardiovascular Interventions Orlando Objectives Recognize common presentations of deep venous thrombosis (DVT) and pulmonary embolus
PULMONARY EMBOLISM MANAGEMENT GUIDELINES
 PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia