Application of Appropriate Use Criteria in Clinical Care of CAD. Peter K. Smith, MD Professor and Chief Thoracic Surgery Duke University 4/29/2012
|
|
|
- Daniella Allen
- 6 years ago
- Views:
Transcription
1 Application of Appropriate Use Criteria in Clinical Care of CAD Peter K. Smith, MD Professor and Chief Thoracic Surgery Duke University 4/29/2012
2
3 Influence of Severity and Location of Stenosis on Cardiac Death Over a 7-Year Mean Follow-up in 29,082 Patients Catheterized for CAD at Duke Between and Treated Without Revascularization Group Severity and Location of Stenosis Relative Chance of Cardiac Death Number of Patients A B C D E F G H I J K L M N None 50% One 50 74% Two or Three 50 74% One 75% Two 75%; None 95% One 95% Prox. LAD or 50 74% LM Two 75%; At least one 95% Two 75% with 95% LAD or 25 49% LM or three 75% and < 95% Two 75% with either Prox. LAD or LM 50 74% Three 75% and two or three 95% Three 75% and either 75% Prox. LAD or 25 49% LM Three 75% and either 95% Prox. LAD or 50 74% LM 75% LM 95% LM
4 Revascularization vs Medical Therapy Revascularization Medical Therapy Low Severity CAD Survival Probability Years
5 Revascularization vs Medical Therapy Revascularization Medical Therapy Survival Probability Low Severity CAD Intermediate Severity CAD P< Years
6 Revascularization vs Medical Therapy Revascularization Medical Therapy 0.9 Low Severity CAD 0.8 Intermediate Severity CAD Survival Probability High Severity CAD P< P< Years
7
8 J Am Coll Cardiol Intv 2009;2:614-21


9
10
11 SYNTAX 4-year cumulative results Outcome CABG surgery, n=819 (%) PCI, n=879 (%) p MACCE <0.001 Death/stroke/MI All-cause mortality Cardiac death Stroke MI <0.001 Repeat revascularization <0.001 "CABG remains the standard of care for patients with complex disease and an intermediate or high SYNTAX score. However, PCI may be an acceptable alternative revascularization method to CABG when treating patients with less complex diseases (SYNTAX score <22), including left main." To put it another way, 75% of patients with left main or threevessel disease are still best treated with CABG, but for the remaining 25%, "PCI is an alternative to surgery, at least out to four years," Serruys commented.
12 MACCE to 3 Years by SYNTAX Score Tercile Low Scores (0-22) 40 CABG (N=104) TAXUS (N=118) Left Main CABG PCI P value > Death 6.0% 2.6% 0.21 Cumulative Event Ra ate (%) P= % 18.0% > CVA 4.1% 0.9% 0.12 MI 2.0% 4.3% 0.36 Death, CVA or MI < > 11.0% 6.9% Months Since Allocation 36 < Revasc. 13.4% 15.4% 0.69 Cumulative KM Event Rate ± 1.5 SE; log-rank P value Site-reported Data; ITT population
13 MACCE to 3 Years by SYNTAX Score Tercile Intermediate Scores (23-32) 40 CABG (N=92) TAXUS (N=103) Left Main CABG PCI P value > Death 12.4% 4.9% 0.06 Cumulative Event Ra ate (%) P= % 23.4% > CVA 2.3% 1.0% 0.46 MI 3.3% 5.0% 0.63 Death, CVA or MI < > 15.6% 10.8% Months Since Allocation 36 < Revasc. 14.0% 15.9% 0.75 Cumulative KM Event Rate ± 1.5 SE; log-rank P value Site-reported Data; ITT population
14 MACCE to 3 Years by SYNTAX Score Tercile High Scores (>32) Cumulative Event Ra ate (%) CABG (N=149) TAXUS (N=135) P= Months Since Allocation Left Main % 21.2% CABG PCI P value < Death 7.6% 13.4% 0.10 CVA 4.9% > 1.6% 0.13 MI 6.1% 10.9% 0.18 Death, CVA or MI < < 15.7% 20.1% 0.34 < Revasc. 9.2% 27.7% <0.001 Cumulative KM Event Rate ± 1.5 SE; log-rank P value Site-reported Data; ITT population
15 SYNTAX Randomized Patients 3 Vessel Disease Syntax Score CABG PCI Total% of Total % % >= % Total 1088 CABG Better 68% Left Main CAD Syntax Score CABG PCI Total % of Total Randomized % Randomized % Randomized >= % Total %
16 SYNTAX All Patients 3 Vessel Disease Syntax Score CABG PCI Total% of Total % % >= % Registry (Mean 38) % Total 1867 Left Main CAD Syntax Score CABG PCI Total % of Total Randomized % Randomized % Randomized >= % Registry (Mean 38) % Total 1187 CABG Better 81% 65%
17 The Usual Talking Points Increased stroke with CABG Revascularization drives the difference, and is not a major complication Neurocognitive Dysfunction with CABG The patient made me do it
18
19 Heart Team Approach to Revascularization Decisions I IIa IIb III A Heart Team approach to revascularization is recommended in patients with unprotected left main or complex CAD. I IIa IIb III Calculation of the STS and SYNTAX scores is reasonable in patients with unprotected left main and complex CAD.
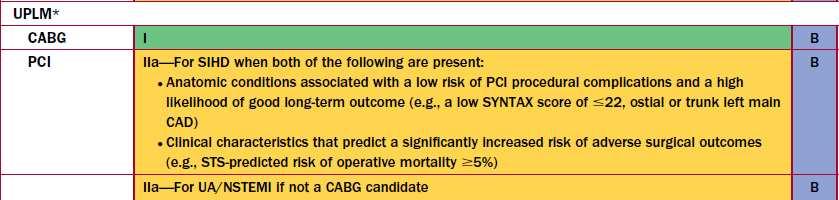
20 Revascularization to Improve Survival: Left Main CAD Revascularization I IIa IIb III CABG to improve survival is recommended for patients with significant ( 50% diameter stenosis) left main coronary artery stenosis. I IIa IIb III PCI to improve survival is reasonable as an alternative to CABG in selected stable patients with significant ( 50% diameter stenosis) unprotected left main CAD with: 1) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of a good long-term outcome (e.g., a low SYNTAX score [ 22], ostial or trunk left main CAD); and 2) clinical characteristics that predict a significantly increased risk of adverse surgical outcomes (e.g., STSpredicted risk of operative mortality 5%).
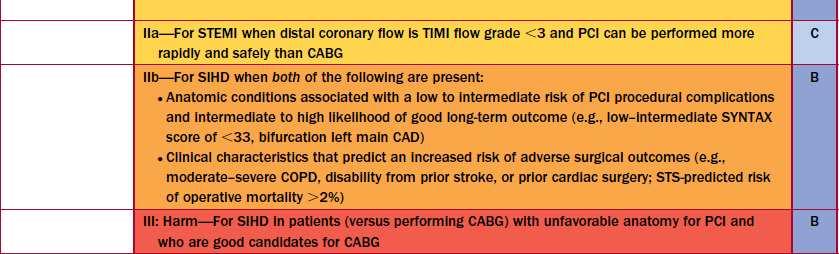
21 Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIa IIb III PCI to improve survival may be reasonable as an alternative to CABG in selected stable patients with significant ( 50% diameter stenosis) unprotected left main CAD with: 1) anatomic conditions associated with a low to intermediate risk of PCI procedural complications and an intermediate to high likelihood of good long-term outcome (e.g., low- intermediate SYNTAX score of <33, bifurcation left main CAD); and 2) clinical characteristics that predict an increased risk of adverse surgical outcomes (e.g., moderate-severe chronic obstructive pulmonary disease, disability from previous stroke, or previous cardiac surgery; STS-predicted risk of operative mortality >2%).
22 Revascularization to Improve Survival: Left Main CAD Revascularization (cont.) I IIa IIb III Harm PCI to improve survival should not be performed in stable patients with significant ( 50% diameter stenosis) unprotected left main CAD who have unfavorable anatomy for PCI and who are good candidates for CABG.
23 Revascularization to Improve Survival: Non- Left Main CAD Revascularization (cont.) I IIa IIb III I IIa IIb III CABG with a left internal mammary artery graft to improve survival is reasonable in patients with a significant ( 70% diameter) stenosis in the proximal LAD artery and evidence of extensive ischemia. It is reasonable to choose CABG over PCI to improve survival in patients with complex 3-vessel CAD (e.g., SYNTAX score >22) with or without involvement of the proximal LAD artery who are good candidates for CABG.
24 Revascularization to Improve Survival: Non- Left Main CAD Revascularization (cont.) I IIa IIb III CABG is probably recommended in preference to PCI to improve survival in patients with multivessel CAD and diabetes mellitus, particularly if a LIMA graft can be anastomosed to the LAD artery.

25 2012 Update Appropriateness Criteria
26
27 All the usual talking points, plus Unmeasured Confounders such as diffuse vs focal CAD, frailty, medical compliance and patient preference Industry conflict not explicitly declared
28 Crossroads Appropriate Use Criteria to be utilized to deny payment when criteria are not designated as appropriate unless: Specific documentation of exception for uncertain Second opinion from surgeon for inappropriate Dramatic shift in leadership in Cardiology away from Industry support.
29
30
31
32 ACCF-STS Database Collaboration on the Comparative Effectiveness of Revascularization Strategies (ASCERT) 86,244 CABG and 103,549 PCI with two- or threevessel disease, age >= 65 STS and NCDR clinical data matched CMS outcome and resource data Longitudinal 3-Year follow-up for mortality
33 Unnecessary stenting case in Tennessee grabs government attention June 10, 2011 Reed Miller Jackson, TN - The US Department of Justice is looking into charges of fraudulent billing leveled by a Tennessee cardiologist against another cardiologist and two hospitals. Dr Wood Deming (Regional Cardiology Consultants, Jackson, TN) is accusing Dr Elie Hage Korban (Heart and Vascular Center of West Tennessee, Jackson) of "blatant overutilization of cardiac medical services, including, but not limited to, cardiac sonography, scintigraphic stress imaging, angiography, angioplasty, and stenting" in order to defraud government insurance programs, according to documents filed with the US District Court for Western Tennessee. Deming also alleges that the executives of Jackson-Madison County General Hospital and the Regional Hospital of Jackson and radiologist Dr Joel Perchik (Advanced Radiology, Jackson, TN) condoned or assisted in Korban's fraud in addition to engaging in a bilateral kickback and self-referral scheme [1].
34 Special Thanks To Slide Set Editors L. David Hillis, MD, FACC, Chair and Peter K. Smith, MD, FACC, Vice-Chair CABG Guideline Writing Committee Members L. David Hillis, MD, FACC, Chair Peter K. Smith, MD, FACC, Vice-Chair Jeffrey L. Anderson, MD, FACC John A. Bittl, MD, FACC Charles R. Bridges, MD, ScD, FACC, FAHA John G. Byrne, MD, FACC Joaquin E. Cigarroa, MD, FACC Verdi J. DiSesa, MD, FACC Loren F. Hiratzka, MD, FACC Adolph M. Hutter, Jr., MD, MACC, FAHA Michael E. Jessen, MD, FACC Ellen C. Keeley, MD, MS Stephen J. Lahey, MD Richard A. Lange, MD, FACC Martin J. London, MD Michael J. Mack, MD, FACC Manesh R. Patel, MD, FACC John D. Puskas, MD, FACC Joseph F. Sabik, MD, FACC Ola Selnes, PhD David M. Shahian, MD, FACC, FAHA Jeffrey C. Trost, MD, FACC Michael D. Winniford, MD, FACC Developed in Collaboration with the American Association for Thoracic Surgery, Society of Cardiovascular Anesthesiologists, and Society for Thoracic Surgeons
35
36 UPLM PCI to Improve Survival (SIHD) Risk of PCI Complication Likelihood of Good Long-term Outcome CABG Mortality Risk Low Hi Hi Hi Low Low COR IIa For SIHD when low risk of PCI complications and high likelihood of good long-term outcome (e.g., SYNTAX score of 22, ostial or trunk left main CAD), and a signficantly increased CABG risk (e.g., STSpredicted risk of operative mortality 5%) IIb For SIHD when low to intermediate risk of PCI complications and intermediate to high likelihood of good long-term outcome (e.g., SYNTAX score of <33, bifurcation left main CAD) and increased CABG risk (e.g., moderate-severe COPD, disability from prior stroke, prior cardiac surgery, STS-predicted operative mortality >2%) III: Harm For SIHD in patients (versus performing CABG) with unfavorable anatomy for PCI and who are good candidates for CABG LOE B B B
37 Comprehensive Update 1264 References New Sections Cardiac Anesthesiology/TEE Hybrid Coronary Revascularization Anti-Platelet Therapy Cardiac Rehabilitation Revascularization harmonized with PCI Guidelines
38 Anesthetic Considerations I IIa IIb III Efforts are recommended to improve interdisciplinary communication and patient safety in the perioperative environment (e.g., formalized checklist-guided multidisciplinary communication). I IIa IIb III A fellowship-trained cardiac anesthesiologist (or experienced board-certified practitioner) credentialed in the use of perioperative TEE is recommended to provide or supervise anesthetic care of patients who are considered to be at high risk.
39 Intraoperative TEE I IIa IIb III Intraoperative TEE should be performed for evaluation of acute, persistent, and life-threatening hemodynamic disturbances that have not responded to treatment. I IIa IIb III I IIa IIb III Intraoperative TEE should be performed in patients undergoing concomitant valvular surgery. Intraoperative TEE is reasonable for monitoring of hemodynamic status, ventricular function, regional wall motion, and valvular function in patients undergoing CABG.
40 Bypass Graft Conduit I IIa IIb III When anatomically and clinically suitable, use of a second IMA to graft the left circumflex or right coronary artery (when critically stenosed and perfusing LV myocardium) is reasonable to improve the likelihood of survival and to decrease reintervention. I IIa IIb III Complete arterial revascularization may be reasonable in patients less than or equal to 60 years of age with few or no comorbidities.
41 Preoperative Antiplatelet Therapy I IIa IIb III In patients referred for elective CABG, clopidogrel and ticagrelor should be discontinued for at least 5 days before surgery and prasugrel for at least 7 days to limit blood transfusions. I IIa IIb III In patients referred for elective CABG, prasugrel should be discontinued for at least 7 days to limit blood transfusions.
42 Preoperative Antiplatelet Therapy (cont.) I IIa IIb III In patients referred for urgent CABG, clopidogrel and ticagrelor should be discontinued for at least 24 hours to reduce major bleeding complications. I IIa IIb III In patients referred for CABG, short-acting intravenous glycoprotein IIb/IIIa inhibitors (eptifibatide or tirofiban) should be discontinued for at least 2 to 4 hours before surgery and abciximab for at least 12 hours beforehand to limit blood loss and transfusions.
43 Preoperative Antiplatelet Therapy (cont.) I IIa IIb III In patients referred for urgent CABG, it may be reasonable to perform surgery less than 5 days after clopidogrel or ticagrelor has been discontinued and less than 7 days after prasugrel has been discontinued.
2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: Executive Summary
 Journal of the American College of Cardiology Vol. 58, No. 24, 2011 2011 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Journal of the American College of Cardiology Vol. 58, No. 24, 2011 2011 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Management of Patients Undergoing Coronary Artery Revascularization
 ACCF/AHA Pocket Guideline Management of Patients Undergoing Coronary Artery Revascularization November 2011 Adapted from the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the
ACCF/AHA Pocket Guideline Management of Patients Undergoing Coronary Artery Revascularization November 2011 Adapted from the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI
 Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
Guidelines/Appropriateness ARCH 2015 St Louis, Missouri April 9-11, 2015 Manish A. Parikh, MD, FACC,FSCAI Center for Interventional Vascular Therapy Columbia University Medical Center / New York Presbyterian
R&M Solutions
 PCI with DES versus CABG & syntax score Dr. Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology, Alexandria University, Egypt Head of Cardiology Department President of Egyptian Society of Cardiology
PCI with DES versus CABG & syntax score Dr. Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology, Alexandria University, Egypt Head of Cardiology Department President of Egyptian Society of Cardiology
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011
 Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Implications of the New ESC/EACTS Guidelines for Myocardial Revascularization in 2011 Prof. Dr. Volkmar Falk Klinik für Herz- und Gefäßchirurgie, Universitätsspital Zürich, Schweiz In 2004 headlines were
Le# Main Interven-on: When Is It Appropriate. Femi Philip, MD Assistant Professor Of Medicine UC Davis
 Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
Le# Main Interven-on: When Is It Appropriate Femi Philip, MD Assistant Professor Of Medicine UC Davis Nil Disclosures Outline What is the LMCA? Should we revascularize severe LMCA disease? What revascularizacon
COMMENT DEFINIR UN PLURITRONCULAIRE. Didier Carrié CHU Toulouse Rangueil
 COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
COMMENT DEFINIR UN PLURITRONCULAIRE VISION ANGIOGRAHIQUE DU PLURITRONCULAIRE Didier Carrié CHU Toulouse Rangueil Congrès GRCI 03 Décembre 2010 Pôle Cardiovasculaire et Métabolique Avec quel œil je regarde
Left Main Intervention: Will it become standard of care?
 Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Left Main Intervention: Will it become standard of care? David Cox, MD FSCAI, FACC Director, Interventional Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown,
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Maquet, Inc.,- unpaid consultant Cordis, Inc.,- unpaid consultant Boston Scientific, Inc.,- travel expenses paid for Syntax
Most Patients with Elective Left Main Disease. Farrel Hellig
 Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
Most Patients with Elective Left Main Disease Should be Treated with PCI! Farrel Hellig Sunnnghill and Sunward Park Hospitals Johannesburg South Africa Everything that can be invented has been invented
Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease
 Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Impact of Angiographic Complete Revascularization after Drug-Eluting Stent Implantation or Coronary Artery Bypass Surgery for Multivessel Coronary Disease Young-Hak Kim, Duk-Woo Park, Jong-Young Lee, Won-Jang
Left Main Intervention: Where are we in 2015?
 Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX
 Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
Michael Mack, M.D. Baylor Healthcare System Heart Hospital Baylor Plano Dallas, TX Boston Scientific, Inc.- Syntax Trial Steering Committee Member- travel expenses paid by trial sponsor Maquet, Inc.- unpaid
high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin Turin / Italy
 What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
What to do with patients with high SYNTAX Score? I Sheiban Division of Cardiology Interventional Card. University of Turin San Giovanni Battista Hospital Turin / Italy Who are the patients with high SYNTAX
Diagnostic, Technical and Medical
 Diagnostic, Technical and Medical Approaches to Reduce CABG Related Stroke Pieter Kappetein, Michael Mack, M.D. Dept Thoracic Surgery, Rotterdam, The Netherlands Baylor Healthcare System Dallas, TX Background
Diagnostic, Technical and Medical Approaches to Reduce CABG Related Stroke Pieter Kappetein, Michael Mack, M.D. Dept Thoracic Surgery, Rotterdam, The Netherlands Baylor Healthcare System Dallas, TX Background
PTCA 1979: : I
 The SYNTAX Message is Clear: CABG is Preferred in Complex MVD Angioplasty Summit TCTAP 2012 Seoul, Korea April 2012 David R. Holmes, MD Mayo Clinic Rochester, MN Presenter Disclosure Information David
The SYNTAX Message is Clear: CABG is Preferred in Complex MVD Angioplasty Summit TCTAP 2012 Seoul, Korea April 2012 David R. Holmes, MD Mayo Clinic Rochester, MN Presenter Disclosure Information David
The SYNTAX-LE MANS Study
 The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
The SYNTAX-LE MANS Study Synergy Between PCI with TAXUS Express and Cardiac Surgery: Late (15-month) Left Main Angiographic Substudy A. Pieter Kappetein, MD, PhD Erasmus MC, Rotterdam, NL SYNTAX-LE MANS
Assessing Myocardium at Risk: Applying SYNTAX
 Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
Assessing Myocardium at Risk: Applying SYNTAX Farouc Jaffer MD PhD FSCAI FACC FAHA Associate Professor of Medicine, Harvard Medical School Director, CAD Program and Chronic Total Occlusion PCI Program
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Important LM bifurcation studies update
 8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
8 th European Bifurcation Club 12-13 October 2012 - Barcelona Important LM bifurcation studies update I Sheiban E-mail: isheiban@yahoo.com Unprotected LM Percutaneous Revascularization What is important
Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)?
 or Coronary Artery Bypass Graft Surgery (CABG)?") Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
Cronicon OPEN ACCESS CARDIOLOGY Case Report Left Main Stenosis. Percutaneous Coronary Intervention (PCI) or Coronary Artery Bypass Graft Surgery (CABG)? Valentin Hristov* Department of Cardiology, Specialized
2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: Executive Summary
 Journal of the American College of Cardiology Vol. 58, No. 24, 2011 2011 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Journal of the American College of Cardiology Vol. 58, No. 24, 2011 2011 by the American College of Cardiology Foundation and the American Heart Association, Inc. ISSN 0735-1097/$36.00 Published by Elsevier
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Controversies in Cardiac Surgery
 Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Controversies in Cardiac Surgery 3 years after SYNTAX : Percutaneous Coronary Intervention for Multivessel / Left main stem Coronary artery disease Pro ESC Congress 2010, 28 August 1 September Stockholm
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Coronary Artery Disease: Revascularization (Teacher s Guide)
") Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Stephanie Chan, M.D. Updated 3/15/13 2008-2013, SCVMC (40 minutes) I. Objectives Coronary Artery Disease: Revascularization (Teacher s Guide) To review the evidence on whether percutaneous coronary intervention
Southern Thoracic Surgical Association CABG in 2012: Implications of the New ESC/EACTS Guidelines
 Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Southern Thoracic Surgical Association 2011 CABG in 2012: Implications of the New ESC/EACTS Guidelines David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford Conflicts of
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
PCI for Left Main Coronary Artery Stenosis. Jean Fajadet Clinique Pasteur, Toulouse, France
 PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
PCI for Left Main Coronary Artery Stenosis Jean Fajadet Clinique Pasteur, Toulouse, France Athens, October 19, 2018 Left Main Coronary Artery Disease Significant unprotected left main coronary artery disease
Improved CABG for Complex CAD: A Perspective of Coming Back
 Improved CABG for Complex CAD: A Perspective of Coming Back John D. Puskas, MD, MSc, FACS, FACC Professor of Cardiothoracic Surgery, Icahn School of Medicine at Mount Sinai Chairman, Department of Cardiac
Improved CABG for Complex CAD: A Perspective of Coming Back John D. Puskas, MD, MSc, FACS, FACC Professor of Cardiothoracic Surgery, Icahn School of Medicine at Mount Sinai Chairman, Department of Cardiac
8/28/2018. Pre-op Evaluation for non cardiac surgery. A quick review from 2007!! Disclosures. John Steuter, MD. None
 Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Pre-op Evaluation for non cardiac surgery John Steuter, MD Disclosures None A quick review from 2007!! Fliesheret al, ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and are for Noncardiac
Emergency surgery in acute coronary syndrome
 Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Emergency surgery in acute coronary syndrome Teerawoot Jantarawan Division of Cardiothoracic Surgery, Department of Surgery, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Update on STEMI Guidelines. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG vs PCI: What do the Guidelines Say?
 AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
AATS International Cardiovascular Symposium: Sao Paolo 2017 CABG vs PCI: What do the Guidelines Say? David P Taggart MD PhD FRCS FESC Professor of Cardiovascular Surgery, University of Oxford Conflicts
Adecade ago, many cardiac surgeons believed
 CABG for Multivessel CAD Recent studies show that CABG is still preferred over PCI for most patients. BY SUBHASIS CHATTERJEE, MD; JOHN C. ALEXANDER, MD; AND PAUL J. PEARSON, MD, PHD Adecade ago, many cardiac
CABG for Multivessel CAD Recent studies show that CABG is still preferred over PCI for most patients. BY SUBHASIS CHATTERJEE, MD; JOHN C. ALEXANDER, MD; AND PAUL J. PEARSON, MD, PHD Adecade ago, many cardiac
The MAIN-COMPARE Study
 Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
Long-Term Outcomes of Coronary Stent Implantation versus Bypass Surgery for the Treatment of Unprotected Left Main Coronary Artery Disease Revascularization for Unprotected Left MAIN Coronary Artery Stenosis:
The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study
 The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study Five-Year Results in the French Subset René Koning, MD On behalf of the SYNTAX investigators Three-year
The Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery: The SYNTAX Study Five-Year Results in the French Subset René Koning, MD On behalf of the SYNTAX investigators Three-year
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION
 TALK THAT NEEDS A LOT MORE ACTION") CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
CONTEMPORARY USE OF ARTERIAL GRAFTS DURING CORONARY ARTERY BYPASS SURGERY: PARADIGM SHIFT? OR A LITTLE (MORE) TALK THAT NEEDS A LOT MORE ACTION JAMES L ZELLNER MD I have no financial disclosures. 1897
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
PCI in Left Main Disease: Are We There Yet?
 PCI in Left Main Disease: Are We There Yet? Moderator Mark A. Turco, MD Director Center for Cardiac & Vascular Research Washington Adventist Hospital Takoma Park, Maryland Panelists David E. Kandzari,
PCI in Left Main Disease: Are We There Yet? Moderator Mark A. Turco, MD Director Center for Cardiac & Vascular Research Washington Adventist Hospital Takoma Park, Maryland Panelists David E. Kandzari,
Management of High-Risk Coronary Artery Disease
 Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
Management of High-Risk Coronary Artery Disease Jeffrey J. Popma, MD Director, Interventional Cardiology Clinical Services Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard Medical
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER
 When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
When should we indisputably perform CABG? Quand faut-il indiscutablement opérer? Dr Hakim BENAMER ICPS, Massy ICV-GVM La Roseraie, Aubervilliers Hôpital FOCH, Suresnes Disclosure Statement of Financial
Medical Rx vs PCI vs CABG
 Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Rationale for Percutaneous Revascularization ESC 2011
 Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Management of High-Risk CAD : Surgeons Perspective
 Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Management of High-Risk CAD : Surgeons Perspective Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Conflict : Cardiac Surgeon! High Risk CABG 77 year old with prior large anterior
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Unprotected Left Main Stenting: Patient Selection and Recent Experience. Alaide Chieffo. S. Raffaele Hospital, Milan, Italy
 Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
Unprotected Left Main Stenting: Patient Selection and Recent Experience Alaide Chieffo S. Raffaele Hospital, Milan, Italy Class IIa (Level B) AHA/ACC 2005 Guidelines Left Main CAD The use of PCI for pts
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Fractional Flow Reserve: Basics, FAME 1, FAME 2. William F. Fearon, MD Associate Professor Stanford University Medical Center
 Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Fractional Flow Reserve: Basics, FAME 1, FAME 2 William F. Fearon, MD Associate Professor Stanford University Medical Center Conflict of Interest Advisory Board for HeartFlow Research grant from St. Jude
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France
 Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Left Main Disease: what is left to surgery? Prof. Jacques Monségu CardioVascular Institute Grenoble, France Background on LM stenosis 5% of patients undergoing angiography Of the myocardium 80% Bifurcation
Appropriate Timing for Coronary Revascularization Post - MI. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Cardiac Catheterization & Stent Implantation
 Reducing Overutilization of Interventional ti Cardiology Procedures: Cardiac Catheterization & Stent Implantation David F. Kong, MD, AM Associate Professor of Medicine, Division of Cardiology Duke University
Reducing Overutilization of Interventional ti Cardiology Procedures: Cardiac Catheterization & Stent Implantation David F. Kong, MD, AM Associate Professor of Medicine, Division of Cardiology Duke University
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention
 Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Rationale for Left Ventricular Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Associate Professor, Division of Cardiology Director, Acute Circulatory Support Program
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille
 Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an
Lésions du tronc commun: Reste t il une place pour la chirugie? Pierre Deharo, CHU TIMONE, Marseille Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD
 Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Mise à Jour sur le traitement du Pluritronculaire Philippe Généreux, MD Columbia University Medical Center and The Cardiovascular Research Foundation, New York, USA Hôpital du Sacré-Coeur de Montréal,
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 89) is a regional and national referral center for percutaneous coronary intervention (PCI). A total of
PCI vs. CABG From BARI to Syntax, Is The Game Over?
 PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
PCI vs. CABG From BARI to Syntax, Is The Game Over? Seung-Jung Park, MD, PhD Professor of Medicine, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea PCI vs CABG Multi-Vessel Disease
Better CABGs vs Better PCI Devices
 CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
CABG vs PCI 2017 Multivessel Coronary Disease Better CABGs vs Better PCI Devices ACC New York, Dec 8, 2017 No Disclosures CABG vs PCI 2017 Stable Multivessel Coronary Disease 1. Are These The two Critical
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS?
 SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
SURGICAL MYOCARDIAL REVASCULARIZATION: ARTERIAL VS VENOUS GRAFTS, SINGLE VS MULTIPLE GRAFTS? Luigi Martinelli Chief, Dept. of Surgery Istituto Clinico Ligure di Alta Specialità RAPALLO During 1987 2006,
Percutaneous Coronary Interventions Without On-site Cardiac Surgery
 Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Percutaneous Coronary Interventions Without On-site Cardiac Surgery Hassan Al Zammar, MD,FESC Consultant & Interventional Cardiologist Head of Cardiology Department European Gaza Hospital Palestine European
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
SYNTAX score before decision making! Corrado Tamburino, MD, PhD
 SYNTAX score in left main - Tamburino TCT Asia Pacific Seoul, 27 April 2011 Slide 1 SYNTAX score before decision making! Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate
SYNTAX score in left main - Tamburino TCT Asia Pacific Seoul, 27 April 2011 Slide 1 SYNTAX score before decision making! Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate
Abbott Vascular. PROTOCOL EXCEL Clinical Trial
 Abbott Vascular PROTOCOL Clinical Trial Evaluation of XIENCE PRIME or XIENCE V versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization PCI (1 st gen DES) vs. CABG for Left
Abbott Vascular PROTOCOL Clinical Trial Evaluation of XIENCE PRIME or XIENCE V versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization PCI (1 st gen DES) vs. CABG for Left
Version 4.4. Institutional Outcomes Report 2014Q3. National Outcomes Report Aggregation Date: Jan 12, :59:59 PM
 Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Count Down to COMBAT
 Count Down to COMBAT Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor of
Count Down to COMBAT Randomized COMparison of Bypass Surgery versus AngioplasTy using Sirolimus-Eluting Stent in Patients with Left Main Coronary Artery Disease Roxana Mehran, MD Associate Professor of
LM stenting - Cypher
 LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
LM stenting - Cypher Left main stenting with BMS Since 1995 Issues in BMS era AMC Restenosis and TLR (%) 3 27 TLR P=.282 Restenosis P=.71 28 2 1 15 12 Ostium 5 4 Shaft Bifurcation Left main stenting with
Declaration of conflict of interest NONE
 Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Declaration of conflict of interest NONE Claudio Muneretto MD, PhD Director of Division of Cardiac Surgery University of Brescia Medical School Italy Hybrid Chymera Different features and potential advantages
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
CHAPTER 2. Heart Team: Concept and Utility MAIN BENEFITS BARRIERS. Praveen Chandra, Rashmi Xavier, Manoj Dhanger, Rohit Goel, Naresh Trehan
 CHAPTER 2 Praveen Chandra, Rashmi Xavier, Manoj Dhanger, Rohit Goel, Naresh Trehan Heart Team: Concept and Utility The concept of The Heart Team approach is gaining popularity in present-day cardiology
CHAPTER 2 Praveen Chandra, Rashmi Xavier, Manoj Dhanger, Rohit Goel, Naresh Trehan Heart Team: Concept and Utility The concept of The Heart Team approach is gaining popularity in present-day cardiology
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS
 CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS STENT, OPERATE, OR MEDICATE? DIFFERING PERSPECTIVES ON CORONARY REVASCULARIZATION JIM BAUCUM, MD FACC SCOTT JOHNSON, MD JANUARY 24, 2015
CARDIOLOGY SYMPOSIUM 2015 CAROLINA CARDIOLOGY CONSULTANTS OF GHS STENT, OPERATE, OR MEDICATE? DIFFERING PERSPECTIVES ON CORONARY REVASCULARIZATION JIM BAUCUM, MD FACC SCOTT JOHNSON, MD JANUARY 24, 2015
CORONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP OVERVIEW 2015 PQRS OPTIONS F MEASURES GROUPS: 2015 PQRS MEASURES IN CONARY ARTERY BYPASS GRAFT (CABG) MEASURES GROUP: #43 Coronary Artery Bypass Graft (CABG):
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease. Vladimir Ganyukov, MD, PhD
 HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease Vladimir Ganyukov, MD, PhD Nikita Kochergin MD, Aleksandr Shilov MD, PhD, Roman Tarasov, MD,
HREVS: A Randomized Trial of PCI vs CABG vs Hybrid Revascularization in Patients With Coronary Artery Disease Vladimir Ganyukov, MD, PhD Nikita Kochergin MD, Aleksandr Shilov MD, PhD, Roman Tarasov, MD,
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Upgrade of Recommendation
 Challenges in LM PCI Decision-making process for stenting Young-Hak Kim, MD, PhD, Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Upgrade of Recommendation for
Challenges in LM PCI Decision-making process for stenting Young-Hak Kim, MD, PhD, Heart Institute, University of Ulsan College of Medicine Asan Medical Center, Seoul, Korea Upgrade of Recommendation for
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention
 Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 08/01/2017 Last reviewed:
Clinical Appropriateness Guidelines: Percutaneous Coronary Intervention Appropriate Use Criteria Effective Date: January 2, 2018 Proprietary Date of Origin: 08/27/2015 Last revised: 08/01/2017 Last reviewed:
Advances in Cardiovascular Diagnosis and Therapy. No disclosure or conflicts. Outline
 Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?
Advances in Cardiovascular Diagnosis and Therapy Firas Zahr, MD Assistant Professor of Medicine Interventional Cardiology University Of Iowa No disclosure or conflicts Outline What is new with revascularization?