Current Reviews for Nurse Anesthetists
|
|
|
- Elwin Watkins
- 6 years ago
- Views:
Transcription
1

2 Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board Chuck Biddle, CRNA, PhD Richmond, Virginia Linda Callahan, CRNA, PhD Klamath Falls, Oregon Nancy Gaskey-Spears CRNA, PhD Gastonbury, Connecticut Joseph A. Joyce, CRNA, BS Winston-Salem, North Carolina Mary Jeanette Mannino, CRNA, JD Laguna Niguel, California Maria Garcia-Otero, CRNA, PhD Coral Gables, Florida Sandra Ouellette, CRNA, Med, FAAN Winston-Salem, North Carolina Charles Barton, MSN, MEd Akron, Ohio Carol G. Elliott, CRNA, MPA, PhD Kansas City, Kansas Linda J. Kovitch, CRNA, MSN Bedford, Massachusetts Frank T. Maziarski, CRNA Seattle, Washington Charles Moss, CRNA, MS Larkspur, Colorado Laura Wild-McIntosh, CRNA, MSN Hillsboro, New Jersey Monte Lichtiger, MD Coral Gables, Florida Associate Publishers Joan McNulty Elizabeth Moya, JD Assistant Editor Linda G. Williams Assistant Publishers Barbara McNulty Donna Scott Circulation Assistants Carrie Scott Tiffany Lazarich Myriam Montes Kimberly Gutierrez Sponsor Frank Moya Continuing Education Programs, LLC Subscription Office - Editorial Office Current Reviews Frank Moya, M.D S.E. First Avenue 1450 Madruga Ave Ft. Lauderdale, FL Suite 207 Coral Gables, FL Phone: (954) Fax: (800) Accreditation This program has been prior approved by the American Association of Nurse Anesthetists for 26 CE credits; Code Number 33802; Expiration Date May 31, Approved by Frank Moya Continuing Education Programs, LLC. Provider approved by the California Board of Registered Nursing, Provider Number CEP 1754, for 26 contact hours and Florida Board of Nursing, Provider Number FBN 2210 for 26 contact hours. In Accordance with AANA directives, you must get 80% of the answers correct to receive one credit for each lesson and if there is a failure, there is no retaking. Disclosure Policy Frank Moya Continuing Education Programs, LLC, in accordance with the Accreditation Council for the Continuing Medical Education s (ACCME) Standards for Commercial Support, will disclose the existence of any relevant financial relationship a faculty member, the sponsor or anyone else who may be in a position to control the content of this Activity has with any commercial interest. BEFORE STARTING, PLEASE SEE LAST PAGE OF LESSON TO READ WHETHER THERE ARE ANY RELEVANT RELATIONSHIPS TO DISCLOSE AND, IF SO, THE DETAILS OF THOSE RELATIONSHIPS. Current Reviews is intended to provide it s subscribers with information that is relevant to anesthesia providers. However, the information published herein reflects the opinions of it s authors and does not represent the views of Current Reviews in Clinical Anesthesia, Current Reviews for Nurse Anesthetists, or Frank Moya Continuing Education Programs, LLC. Anesthesia practitioners must utilize their knowledge, training and experience in their clinical practice of anesthesiology. No single publication should be relied upon as the proper way to care for patients. The information presented herein does not guarantee competency or proficiency in the performance of procedures discussed. Copyright 2015 by Current Reviews. Reproduction in whole or in part prohibited except by written permission. All rights reserved. Information has been obtained from sources believed to be reliable, but it s accuracy and completeness, and that of the opinions based therein are not guaranteed. Printed in U.S.A. Current Reviews is published biweekly by Current Reviews, 1828 S.E. First Avenue, Ft. Lauderdale, FL POSTMASTER: Send address changes to Current Reviews, 1828 S.E. First Avenue, Ft. Lauderdale, FL
3 Anesthesia and the Patient with Carotid Artery Disease Terrence L. Trentman, MD Associate Professor of Anesthesiology Mayo Clinic Arizona Phoenix, Arizona LESSON OBJECTIVES Upon completion of this lesson, the reader should be able to: 1. Discuss the epidemiology and pathophysiology of carotid artery disease. 2. List imaging options for patients with carotid artery disease. 3. List Class I guidelines for selection of patients for carotid revascularization. 4. Discuss the risks of shunt use during carotid endarterectomy (CEA) surgery. 5. Explain how carotid sinus manipulation may affect blood pressure. 6. Describe elements of the preoperative exam for patients undergoing carotid revascularization. 7. List and contrast neurologic monitoring options during CEA. 8. Discuss anesthetic goals during CEA surgery, including ventilation, blood pressure, glucose and temperature control. 9. Discuss the greatest long-term risk for CEA patients. 10. List common postoperative problems after CEA. Current Reviews for Nurse Anesthetists designates this lesson for 1 CE contact hour in pharmacology/therapeutics. Introduction Many patients with carotid artery disease will present for carotid endarterectomies (CEA) or other procedures, so it is vital that anesthesia providers understand the management of this challenging patient population. Nationally, stroke is the fourth most common cause of death after heart disease, cancer and respiratory conditions, with 15-20% of ischemic strokes due to carotid artery disease. Intracranial atherosclerosis is less common than extracranial atherosclerosis, which most commonly occurs at the bifurcation of the internal and external carotid arteries. Carotid artery disease is more frequently an embolic problem than one of complete occlusion of the artery. Emboli from the carotid artery cause amaurosis fugax (monocular blindness) or transient ischemic attacks (TIAs) manifested by paresthesia, clumsiness, or speech changes. Cerebral artery disease, including carotid artery stenosis, is about one-third as common as coronary artery disease in the United States. However, about 8.5% of patients will have both coronary and cerebral artery disease (Table 1). As discussed below, this combination of vascular disease creates management decision challenges for the anesthesia provider. This lesson will present an anatomic description of carotid artery disease, in addition to guidelines on management of patients with extracranial carotid stenosis. Based upon a review of current literature, discussion points in this lesson include: 1. When is CEA indicated vs. carotid artery stenting (CAS)? 2. How is a CEA performed as opposed to CAS? 3. What is the greatest risk to patients undergoing a CEA? 4. What neurologic monitoring options are available during CEA procedures? 5. What are the hemodynamic goals during and after cross clamping the carotid artery? 6. Is regional anesthesia better than general anesthesia for CEA? Curr Rev Nurs Anesth 38(7):81-92,
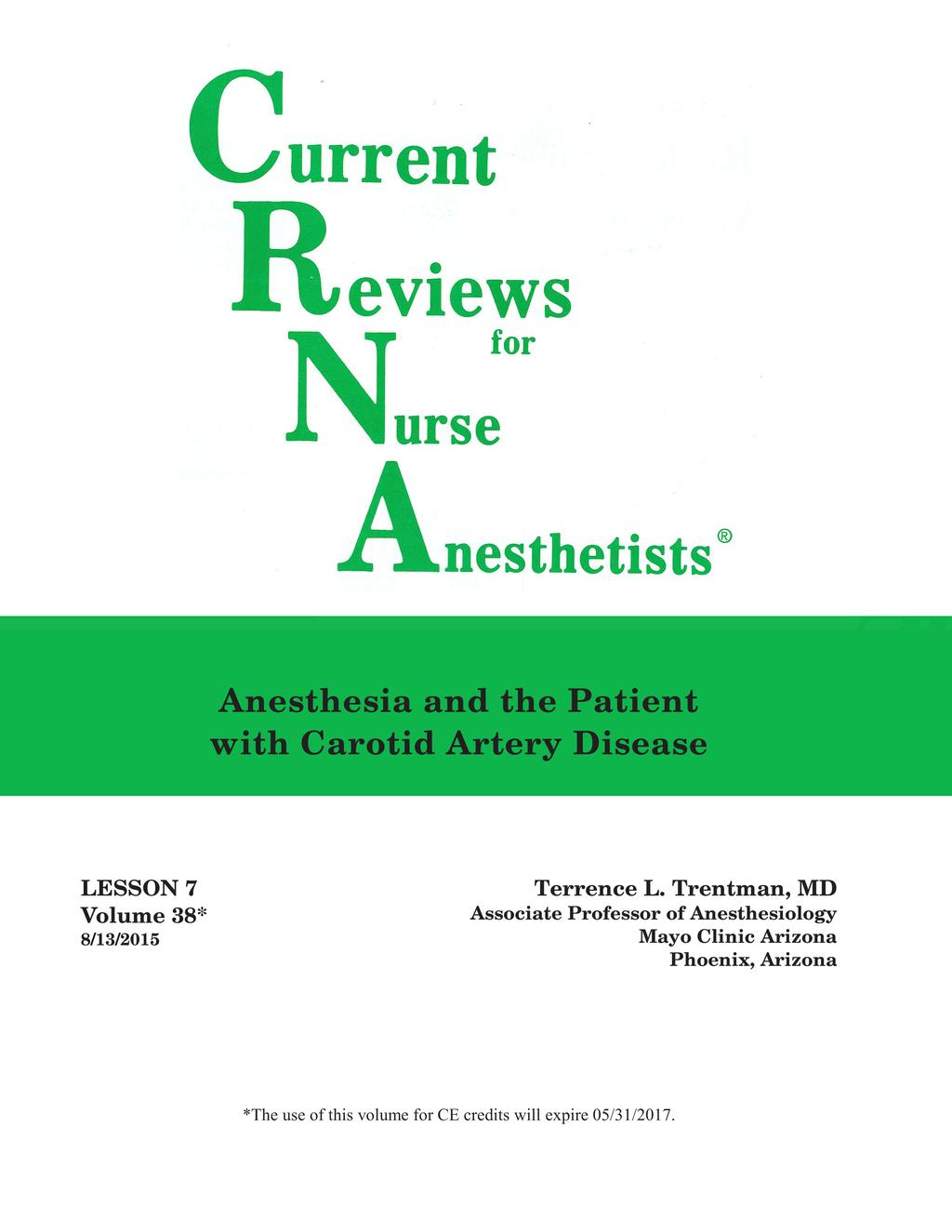
4 Diagnosing Carotid Artery Disease A diagnosis of carotid artery disease is based upon symptoms of a transient ischemic attack, or results of screening patients with risk factors, including advanced age, smoking, hypertension and hyperlipidemia. A carotid bruit may be heard over the neck; however, cardiac valvular noise can be transmitted to the carotids, so this is not a particularly sensitive test. For those suspected of having carotid disease, the most common test is the duplex ultrasound, which has a sensitivity of 94% and a specificity of 92% for carotid artery stenosis greater than 60% (the gold standard is digital subtraction angiography). A positive carotid ultrasound is usually followed by CT angiography or magnetic resonance angiography (Figure 1). Management Guidelines In 2011, the American College of Cardiology Foundation and the American Heart Association published their guidelines on the management of patients with extracranial carotid artery disease. The recommendations were classified as follows: 1. Class I recommendation means that the benefit far outweighs the risk of the treatment, and the treatment should be performed. 2. Class IIa means the benefit outweighs the risk, but additional studies are needed. It is reasonable to perform the treatment. 3. Class IIb means the benefit outweighs or is equal to the risk, and more studies are needed; therefore, the treatment may be considered. 4. Class III means there is no benefit or even harm, and the treatment should not be performed. All patients should undergo medical management, including smoking cessation, use of aspirin, a statin and blood pressure management. Class I recommendations for carotid revascularization include patients who have had a nondisabling stroke or TIA within six months who are at average to low surgical risk. These patients should undergo a CEA, assuming that they have greater than 70% of stenosis of the internal carotid artery by ultrasound or greater than 50% stenosis by angiography. Carotid artery stenting (CAS) is an alternative to CEA in this patient population (Table 2). Class IIa recommendations include performing CEA in asymptomatic patients with greater than 70% stenosis if their perioperative risk is low. CAS can be chosen instead of CEA in this patient population if the anatomy is unfavorable for CEA. Class IIb guidelines include prophylactic CAS in asymptomatic patients who have significant stenosis (70% by ultrasound or 60% by angiography). However, the benefit of intervention in this asymptomatic patient population (vs medical therapy) is not well established. Class III guidelines include patients where carotid revascularization is not recommended. This includes patients with less than 50% stenosis, chronic total occlusion of the artery, or patients with severe disability caused by a cerebral infarct. A number of factors should be considered in evaluating these patients; most importantly, their greatest long-term risk is myocardial ischemia. As the reader can surmise, some controversy surrounds the management of patients with asymptomatic carotid artery disease. It is reasonable to screen asymptomatic patients for carotid stenosis when they have known or strongly suspected coronary artery disease. Also, patients who have a bruit or known carotid stenosis greater than 50%, known vascular disease or > 2 risk factors (e.g., age, smoking and dyslipidemia) can be screened with an ultrasound. In addition, patients who are scheduled for a CABG should undergo screening if they have at least one risk factor such as left main coronary disease, peripheral vascular disease, smoking, age > 65 years, carotid bruit or prior TIA or stroke. Particularly challenging are those patients with symptomatic carotid artery disease AND coronary Table 1 Epidemiology and Pathophysiology of Carotid Artery Disease # Stroke is the 4 most common cause th of death # Among patients who have coronary disease, 8.5% will also have carotid disease # Of ischemic strokes, 15-20% are caused by carotid disease # Extracranial is more common than intracranial atherosclerosis # Carotid disease is usually an embolic rather than an occlusive problem # Transient ischemic attack (TIA) presents as paresthesias, clumsiness, speech changes and/or weakness # Amaurosis fugax is monocular blindness 84 Current Reviews for Nurse Anesthetists
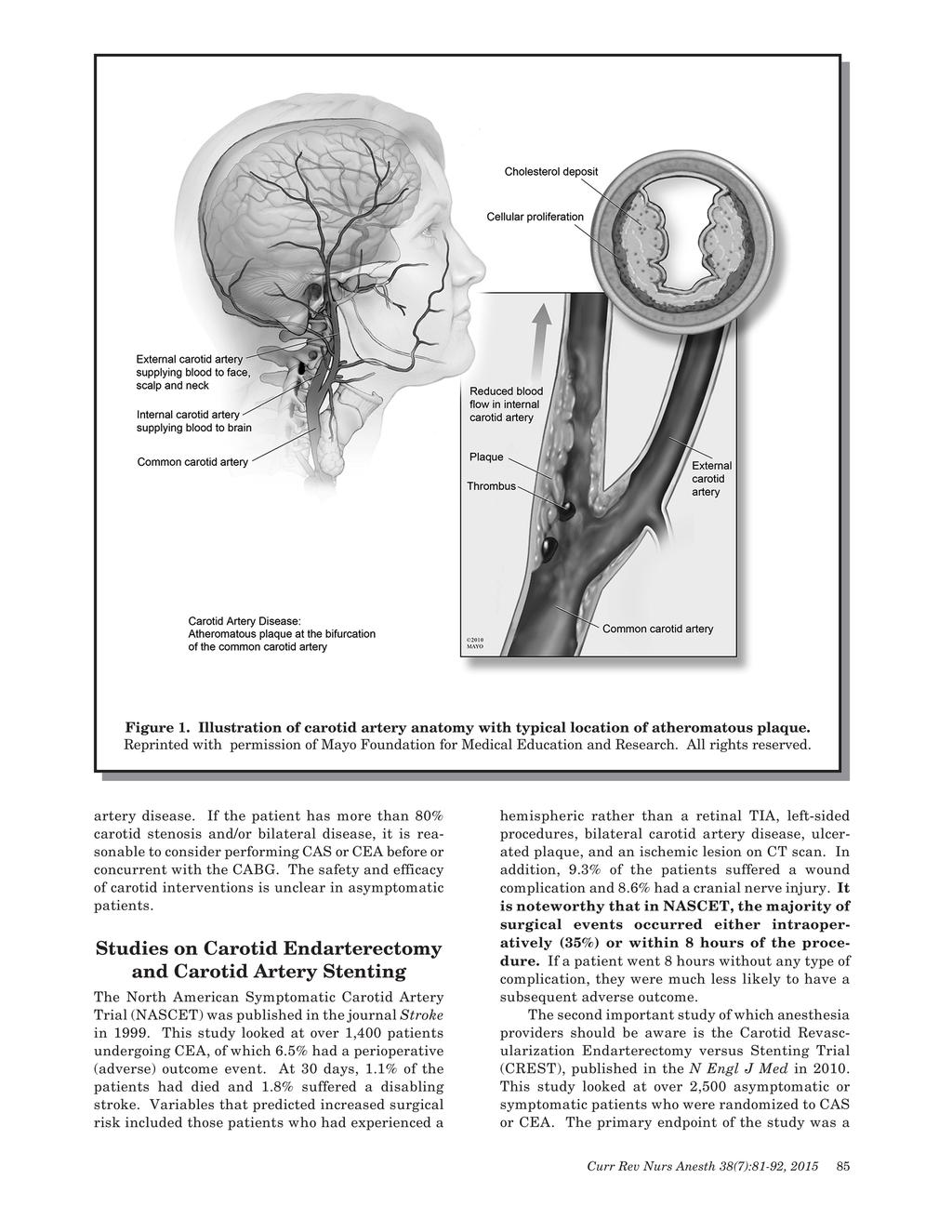
5
6
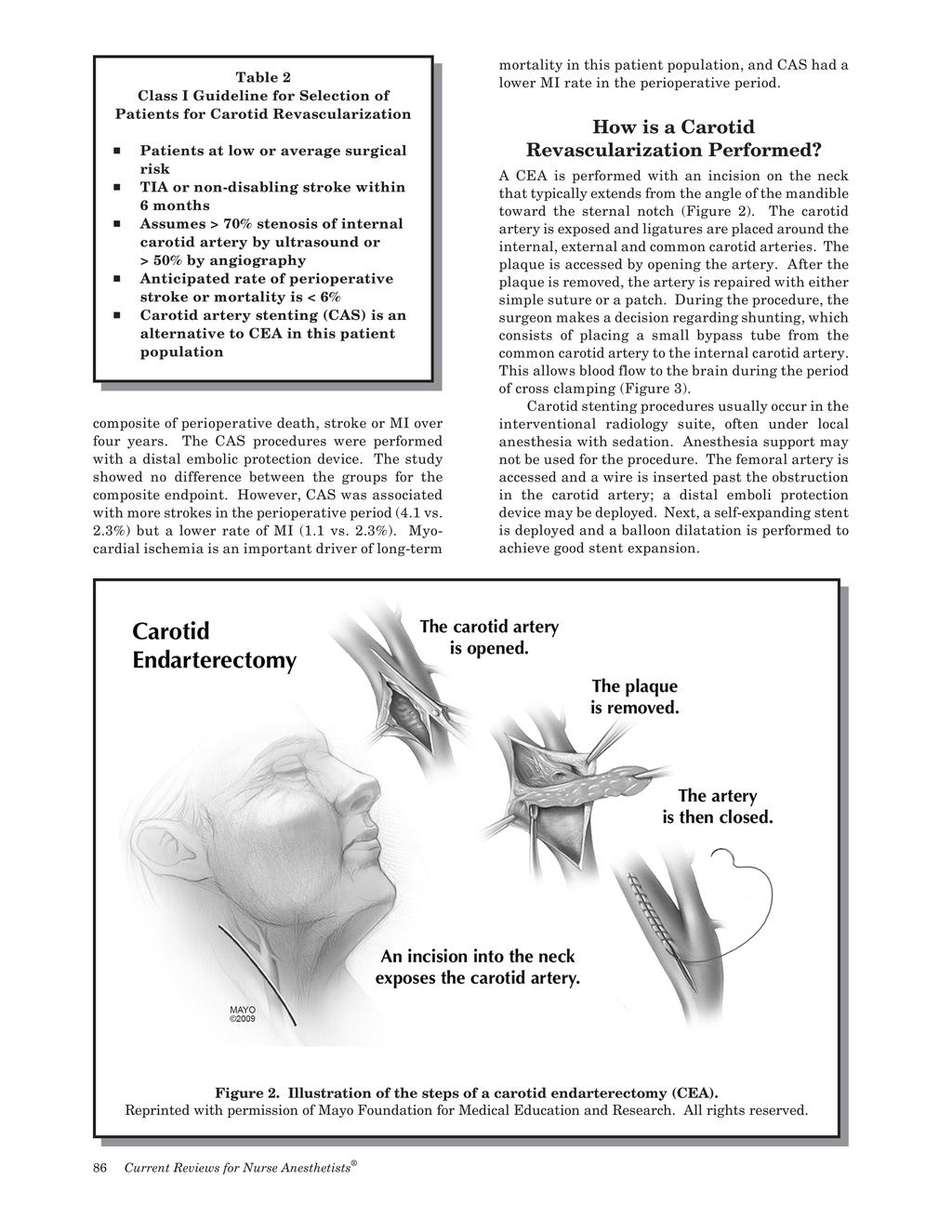
7
8 This is vital because ischemic or under-perfused regions of the brain may have lost their normal autoregulation. However, the most common cause of stroke is embolism, not hypoperfusion. Nonetheless, during the cross clamp phase of a CEA, anesthesia providers commonly use fluids and vasopressors (e.g., phenylephrine) to maintain blood pressure at normal to approximately 20% above the patient s baseline (unless contraindicated). Unfortunately, augmenting blood pressure can increase the risk of myocardial ischemia. Most important during the cross clamp phase of a CEA is to avoid hypotension, particularly if no shunt is used. What follows is a description of various neurologic monitoring options during CEA (Table 4). The Awake Patient. Having the patient awake and communicating during a CEA is the gold standard of neurologic monitoring. The patient and surgeon must be comfortable with this approach, and frequent communication with the patient is required. Verbal and strength testing is carried out during the procedure every 2 to 5 minutes, usually with a handgrip (squeeze toy) and patient responses to questions. The procedure may be carried out under regional anesthesia with local anesthetic augmentation as needed. This approach is difficult if the patient is claustrophobic, anxious, unable to lay flat or coughing. If a complication develops, airway access may be difficult. Carotid Stump Pressure. In this approach, the surgeon places a needle or balloon catheter in the distal carotid artery to measure the pressure. A pressure of at least 40 mmhg may be equally reliable and as cost effective as EEG. If there is adequate stump pressure, the surgeon may decide not to shunt. However, stump pressure may not correlate with cerebral perfusion pressure. The ischemic threshold for brain tissue may vary from patient to patient; therefore, it is difficult to know how much stump pressure is needed in a patient. Electrocephalogram (EEG). This is carried out with scalp electrodes. EEG deterioration begins below a cerebral blood flow of 15 ml/ min/100 grams of brain tissue. Ipsilateral EEG attenuation, slowing or both are seen in ischemia. If evidence of ischemia is seen, the surgeon can place a shunt and the anesthesia provider can increase blood pressure. However, the EEG is sensitive to changes in anesthetic depth and drugs such as propofol and barbiturates. If the anesthetic depth is adjusted during EEG monitoring, the technician should be advised. Bilateral EEG changes should result from changes in anesthetic depth (ischemia is unilateral). It is noteworthy that the EEG is more effective at monitoring cortical rather than deep brain structures. Also, many patients have baseline EEG abnormalities, making the evaluation of EEG changes difficult. Somatosensory Evoked Potentials (SSEP). This form of monitoring evaluates cortical potentials after stimulation of a peripheral nerve. It is more effective at evaluating deep brain structures than EEG. A 50% decrease in amplitude or a 10% increase in latency is considered significant. A constant, light level of anesthesia is required during SSEP monitoring. Overall, EEG and SSEP have similar sensitivity and specificity for cerebral ischemia. Transcranial Doppler (TCD). TCD measures middle cerebral artery flow velocity through the thin petrous bone, and it can also detect embolic signals. TCD predictors of stroke after a CEA include emboli during wound closure, > 90% decrease in systolic velocity at cross clamp placement, and/or > 100% increase in the pulsatility index at cross clamp release. TCD is operator dependant and 10-15% of patients cannot be monitored due to a poor temporal region window. Cerebral Oximetry (Near Infrared Spectroscopy, NIRS). Cerebral oximetry monitors cerebral oxygen saturation of the frontal lobe. NIRS is easy to apply and non-invasive. With awake monitoring as the gold standard, a > 10% drop in cerebral oxygen saturation has been shown to have high sensitivity and specificity for cerebral ischemia. Other Perioperative Management Considerations Ventilation management during CEA is important. Hypercarbia can be detrimental due to dilatation of normal vessels and potential steal from hypoperfused areas. Conversely, hypocarbia may result in cerebral vasoconstriction. Therefore, normocarbia should be maintained during CEA surgery. Table 4 Neurologic Monitoring Options During Carotid Endarterectomy # Assess the awake patient (verbal response, contralateral hand grip) # Carotid stump pressure (40-50 mm Hg?) # Electroencephalogram (EEG) # Somatosensory evoked potentials (SSEP) # Transcranial Doppler (TCD) # Cerebral oximetry = Near infrared spectroscopy (NIRS) 88 Current Reviews for Nurse Anesthetists
9 Hyperglycemia is associated with worse neurologic outcomes after cerebral ischemia. Therefore, blood glucose should be monitored throughout the perioperative period and maintained within reasonable levels. For example, at the author s institution, blood glucose levels between mg/dl is acceptable. This is particularly important as many patients with cerebral vascular disease will also be diabetic. In terms of volatile agents, isoflurane, sevoflurane and desflurane all reduce the cerebral metabolic rate of oxygen (CMRO 2). There may be advantages to less soluble agents like sevoflurane and desflurane in terms of rapid wake-up. There are reports of administration of barbiturates during CEA surgery, as these drugs may provide cerebral protection during periods of ischemia. Thiopental decreases CMRO 2 by 50%. While a barbiturate bolus could be given before cross clamping of the carotid artery, there is no evidence of better outcomes with this technique and delayed emergence is likely. Hypothermia can also depress neuronal activity and decrease CMRO 2. A 2-3 degree temperature decrease will reduce ischemic damage. However, there is no evidence of benefit of hypothermia during CEA and the logistics of cooling are considerable. Also, shivering increases myocardial oxygen demand. In terms of monitoring, arterial lines are commonly used. Transesophageal echocardiogram (TEE) monitoring is an option but logistically difficult to insert and use during this particular procedure. Intravenous access must be adequate to support the use of infusions (both a vasopressor and vasodilator). New neurologic deficits need to be investigated, including evaluating for patency of the newly repaired carotid artery and CT scanning of the brain. Minimal premedication is ideal, because the goal is an awake patient ready for neurological evaluation at the end of surgery. The preoperative blood pressure range and pulse information should be obtained before the surgery begins. Minimizing long-acting opiates is also desirable to reduce sedation at the end of the procedure (Table 5). If regional anesthesia is selected, a superficial cervical plexus block can be performed by infiltrating local anesthetic just behind the posterior border of the sternocleidomastoid muscle. The surgical field covers the C2-4 dermatomes. Deep cervical plexus blocks do not contribute to patient comfort and have been associated with complications. The GALA trial, published in Lancet in 2008, showed no difference in outcome for general versus local anesthesia in over 3,500 patients. Similarly, a Cochrane review from 2013 looked at over 4,500 operations and showed no statistically significant difference in 30-day death or stroke for those patients undergoing local versus regional anesthesia for CEA. Table 5 Anesthetic Considerations During CEA # Routine arterial line plus ability to titrate infusions to increase or decrease blood pressure # While carotid artery is cross clamped, maintain blood pressure ~ 20% above baseline # Maintain normocarbia # Avoid hyperglycemia (worsens neurologic outcome) # Barbiturate bolus before cross clamping may decrease CMRO 2, but no evidence of better outcomes, and slower wake-up # Cooling patient is logistically difficult and is not associated with benefit # Carotid sinus stimulation can cause hypotension and bradycardia # Goal: rapid wake-up and early neurologic assessment Post Procedure Management In the postoperative period, a number of management challenges may develop (Table 6). Although hypotension is possible, hypertension is more common. Less frequent are cranial nerve injuries including vagus, hypoglossal, mandibular and posterior auricular nerve injuries. In NASCET, 101/1,415 patients developed a wound hematoma, 4 of which were severe enough to cause death or permanent disability. The hyperperfusion syndrome consists of headache and hypertension. This occurs in 6-11% of patients because of loss of brain autoregulation and increased brain perfusion after removal of the carotid plaque. The carotid sinus controls baroreceptor reflexes and responds to increased arterial pressure with bradycardia and vasodilation. This reflex can be triggered during surgery as the surgeon manipulates the carotid bifurcation. The surgeon can infiltrate the area with local anesthetic to blunt this response. However, after removal of the plaque, the sinus may detect increased blood pressure leading to hypotension. More common is postoperative hypertension due to denervation of the baroreceptor fibers in the artery. The denervated carotid sinus receives less stimulation and responds as if the blood pressure is low. Therefore, careful hemodynamic monitoring should continue in the immediate postoperative period. In the author s practice, patients are monitored at least overnight in the step-down unit. Curr Rev Nurs Anesth 38(7):81-92,
10 Table 6 Post-Carotid Endarterectomy Concerns # New neurologic deficits, requiring imaging and/or neck exploration # Hemodynamic instability (hypertension more common than hypotension) # Cranial nerve injury # Neck hematoma # Hyperperfusion syndrome (headache, hypertension, cerebral edema, seizures) # Myocardial ischemia Poor preoperative blood pressure control predicts postoperative hypertension. Hypertension and tachycardia are associated with myocardial ischemia, the greatest risk to patients after CEA. Hypertension can be associated with cerebral edema, hemorrhage and seizures. Post-CEA hypertension is associated with adverse outcomes; whereas, hypotension and bradycardia are not. In the immediate postoperative period, a blood pressure greater than 140/90 should be treated and continuous ECG monitoring should be carried out, knowing that myocardial ischemia will occur in up to 15% of CEA patients. If the patient is hypotensive, residual anesthetic is a possible cause, as well as too much antihypertensive medication or possible resetting of the baroreceptors. If patients have multiple risk factors, including a history of stroke, congestive heart failure, renal failure, hypertension, dysrhythmia and/or MI, they should be considered for the ICU postoperatively. As noted above, most patients in NASCET who suffered an adverse outcome were identified within 8 hours of surgery. Summary Carotid artery disease is common and associated with coronary artery disease. The greatest perioperative risk remains myocardial ischemia. It is important for the anesthesia provider to discuss with the surgeon the plan for neurologic monitoring and shunting. Since there is no benefit to regional over general anesthesia, this decision can be based upon provider preference and patient factors including anxiety and ability to lie flat. Cerebral perfusion pressure is a key to the successful outcome of CEA. Blood pressure should be maintained at normal to approximately 20% above baseline during the cross clamp period with normocarbia and an anesthetic technique tailored for a rapid wake up. Postoperative blood pressure control, stroke, and myocardial ischemia remain important considerations. Terrence L. Trentman, MD, Department of Anesthesiology, Mayo Clinic Arizona, Phoenix, Arizona. trentman.terrence@mayo.edu References Augoustides J. Advances in the management of carotid artery disease: focus on recent evidence and guidelines. Journal of Cardiothoracic and Vascular Anesthesia 26: , Brott T. et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis (CREST). N Eng J Med 363:11-23, Ferguson G. et al. The North American symptomatic carotid endarterectomy trial (NASCET). Stroke 30: , Lewis S. et al. General anaesthesia versus local anaesthesia for carotid surgery (GALA): a multicentre, randomized controlled trial. Lancet 372: , Roffi M. et al. Carotid artery stenting vs. endarterectomy. European Heart Journal 30: , (Good review of CAS vs. CEA) Unic-Stojanovic D. et al. General versus regional anesthesia for carotid endarterectomy. Journal of Cardiothoracic and Vascular Anesthesia 27: , Vaniyapong T. et al. Local versus general anaesthesia for carotid endarterectomy. Cochrane Database of Systematic Reviews Dec Terrence L. Trentman, MD. Dr. Trentman graduated from Tulane University School of Medicine and completed an internship, anesthesiology residency and pain fellowship at Mayo Clinic, Rochester, Minnesota. He now practices at Mayo Clinic in Arizona and is a member of the liver transplant team. He divides his time between the general operating room including ultrasound guided regional anesthesia, and the chronic pain clinic. 90 Current Reviews for Nurse Anesthetists
11 Tips for your Clinical Practice: Key Points # Stroke is the fourth leading cause of mortality in the United States, and carotid arterial disease is responsible for 15-20% of ischemic strokes; approximately 8.5 % of patients have both cerebral and coronary artery disease. # Recommendations for carotid revascularization range from Class I (> 70% occlusion; benefit far outweighs risk; non-disabling stroke or TIA within six months; average to low surgical risk) to Class III (< 50% occlusion; no benefit or even harm; chronic total occlusion or severe disability; carotid revascularization not recommended). # For patients with symptomatic carotid artery and coronary artery disease and > 80% carotid stenosis, CAS or CEA may be considered prior to or concurrently with CABG. # In preparation for anesthesia and surgery patients should continue statins, aspirin and antihypertensive drugs (particularly beta-blockers). Baseline blood work and blood chemistries should be checked, and a cardiac evaluation should be obtained. # The circle of Willis is complete in < 50% of patients; cross clamping of the carotid artery may precipitate additional neurologic deficits and/or a permanent stroke. # Neurological monitoring and shunt insertion do not change the risk of stroke. # Although debated for many decades, hyper- and hypocarbia should be avoided during CEA. Blood glucose should be maintained at mg/dl. # Hypothermia and thiopental administration decrease CMRO 2, but better outcomes have not been demonstrated for either intervention. # Postoperative hypotension may reflect residual anesthetic or excessive administration of antihypertensive drugs. Robert R. Kirby, M.D. Professor Emeritus of Anesthesiology University of Florida, College of Medicine FRANK MOYA CONTINUING EDUCATION PROGRAMS, INC. & FACULTY DISCLOSURE THIS AUTHOR S AND FMCEP S SPECIFIC DISCLOSURES: The author / faculty has indicated that there is no relevant financial interest or relationship with any commercial interest. The author / faculty has indicated that, as appropriate, he/she has disclosed that a product is not labeled for the use under discussion, or is still under investigation. As a matter of policy, FMCEP does not have any relevant financial interest or relationship with any commercial interest. In addition, all members of the staff, Governing Board, Editorial Board and CME Committee who may have a role in planning this activity have indicated that there is no relevant financial interest or relationship with any commercial interest. Current Reviews is intended to provide its subscribers with information that is relevant to anesthesia providers. However, the information published herein reflects the opinions of its authors. Anesthesia practitioners must utilize their knowledge, training and experience in their clinical practice of anesthesiology. No single publication should be relied upon as the proper way to care for patients. DESIGNATON OF SPECIFIC CONTENT AREAS: Current Reviews for Nurse Anesthetists (CRNA) is designed to meet the standards and criteria of the American Association of Nurse Anesthetists (AANA) for the prior-approved continuing medical education activity, Provider-Directed Independent Study, also known as home study. CRNA is an approved program provider. CRNA has designated the lessons which meet specific content areas such as pharmacology, HIV/AIDS, etc. However, only the Board of Nursing of an individual State is the final authority in the determination of whether or not these lessons meet the State s licensure requirements. Curr Rev Nurs Anesth 38(7):81-92,
12 MARK ONLY THE ONE BEST ANSWER PER QUESTION ON YOUR ANSWER CARD. MARK THIS PAGE AND KEEP FOR YOUR RECORDS. 7 In accordance with AANA directives, you must get 80% of the answers correct to receive one credit for each lesson, and if there is a failure, there is no retaking. POST-STUDY QUESTIONS 1. Amaurosis fugax can be caused by carotid artery emboli and is defined as: G A. Transient clumsiness. G B. Monocular blindness. G C. Arm or leg weakness that lasts less than 24 hours. G D. Speech changes. 2. A carotid bruit: G A. Almost always emanates from the cardiac valves. G B. Is used to diagnose coronary artery disease. G C. Is highly sensitive for carotid stenosis > 70%. G D. Is an abnormal sound auscultated over the carotid artery. 3. Class I recommendations for carotid revascularization include which of the following: G A. Less than 50% stenosis in symptomatic patients. G B. TIA within 6 months with low surgical risk. G C. Total occlusion of the artery. G D. Severe disability caused by a cerebral infarct. 4. In NASCET, the majority of surgical adverse events occurred: G A. Intraoperatively or within 8 hours after surgery. G B. 30 days or more postop. G C. 90 days or more postop. G D. 7 days or more postop. 5. In CREST: G A. Carotid stent (CAS) patients had a higher rate of MI. G B. CAS patients had fewer strokes than endarterectomy (CEA) patients. G C. No difference was found in the composite endpoint, CAS vs. CEA. G D. Overall, CEA patients had the best long-term results. 6. During CEA surgery, shunting: G A. Is considered standard of care. G B. Is the only reasonable response to electroencephalogram (EEG) changes. G C. Lowers the risk of stroke. G D. Can cause air emboli. 7. The most common cause of stroke during CEA surgery is: G A. Embolism. G B. Hypotension. G C. Shunt use. G D. Hypertensive hemorrhage. 8. The gold standard of neurologic monitoring during CEA surgery is: G A. Carotid stump pressure. G B. Electroencephalogram (EEG). G C. The awake patient. G D. Transcranial Doppler (TCD). 9. Ventilation during CEA surgery should be managed to achieve: G A. Hypercarbia to dilate cerebral blood vessels. G B. Hypocarbia to constrict normal cerebral vessels and drive blood toward stenotic areas. G C. A mild to moderate respiratory alkalosis. G D. Normocarbia. 10. Carotid sinus fibers in the artery wall can be damaged during CEA surgery, most commonly resulting in postoperative: G A. Hypotension. G B. Hypertension. G C. Tachycardia. G D. New neurologic deficits. Moving? Please notify us at least six weeks before you move to your new address, so you won t miss any issues of your subscription. The post office will not forward your subscription to Current Reviews for Nurse Anesthetists. Phone: (954) Fax: (954) or (800)
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY
 GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
GUIDELINE FOR RECOVERY ROOM MANAGEMENT OF PATIENTS AFTER CAROTID ENDARTERECTOMY Full Title of Guideline: Author (include email and role): Guideline for Recovery Room Management of Patients after Carotid
Current Reviews for Nurse Anesthetists
 Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board Chuck Biddle, CRNA, PhD Richmond, Virginia Linda Callahan, CRNA,
Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board Chuck Biddle, CRNA, PhD Richmond, Virginia Linda Callahan, CRNA,
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Controversies in Carotid Endarterectomy
 Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Carotid endarterectomy
 British Journal of Anaesthesia 99 (1): 119 31 (2007) doi:10.1093/bja/aem137 Advance Access publication June 6, 2007 Carotid endarterectomy S. J. Howell* Academic Unit of Anaesthesia, The General Infirmary
British Journal of Anaesthesia 99 (1): 119 31 (2007) doi:10.1093/bja/aem137 Advance Access publication June 6, 2007 Carotid endarterectomy S. J. Howell* Academic Unit of Anaesthesia, The General Infirmary
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Carotid Artery Stenting (CAS) Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA
 Pathophysiology. Technical Considerations. Plaque characteristics: relevant concepts. CAS and CEA") Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Carotid Artery Stenting (CAS) Carotid Artery Stenting for Stroke Risk Reduction Matthew A. Corriere MD, MS, RPVI Assistant Professor of Surgery Department of Vascular and Endovascular Surgery Rationale:
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Surgical Treatment of Carotid Disease
 Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Surgical Treatment of Carotid Disease The Old, the New, and the Future
Disclosures. State of the Art Management of Carotid Stenosis. NIH funding for clinical trials Consultant for Scientia Vascular and Medtronic
 State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
State of the Art Management of Carotid Stenosis Mark R. Harrigan, MD UAB Stroke Center Professor of Neurosurgery, Neurology, and Radiology University of Alabama, Birmingham Disclosures NIH funding for
Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie?
 XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
XXV. kongres České společnosti anesteziologie, resuscitace a intenzivní medicíny, Praha 3.-5.10. 2018 Co chce/čeká neurochirug od anesteziologa během karotické endarterektomie? Hejčl A., Orlický M., Sameš
Carotid Stenosis 1/24/2019. Review of Primary Studies. NASCET- Moderate stenosis. ACAS (Asymptomatic Carotid Atherosclerosis Study) NASCET
 NASCET") Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Review of Primary Studies Carotid Stenosis NINDS National Institute of Neurological Disorders and Stroke 2 large studies to determine who would benefit from surgery NASCET North American Symptomatic Carotid
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA
 Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Management of Carotid Disease CHRISTOPHER LAU PGY-3 BROOKLYN VA SUNY DOWNSTATE MEDICAL CENTER Case 61 year old male referred to Vascular Surgery for left internal carotid stenosis Presented with transient
Anesthesia for Cardiac Patients for Non Cardiac Surgery. Kimberly Westra DNP, MSN, CRNA
 Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Anesthesia for Cardiac Patients for Non Cardiac Surgery Kimberly Westra DNP, MSN, CRNA Anesthesia for Cardiac Patients for Non Cardiac Surgery Heart Disease is a significant problem in the United States:
Current Reviews for Nurse Anesthetists
 Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board JOHN AKER, CRNA, DNAP Iowa City, Iowa MONTE LICHTIGER, MD Coral
Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board JOHN AKER, CRNA, DNAP Iowa City, Iowa MONTE LICHTIGER, MD Coral
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE?
 UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
UPMC HAMOT CAROTID ARTERY DISEASE WHERE DO WE GO FROM HERE? Richard W. Petrella M.D. FACP,FACC,FASCI DEPARTMENT CHAIRMAN CVM&S UPMC HAMOT MEDICAL CENTER 1 LEARNING OBJECTIVES REVIEW THE RISK FACTORS FOR
Contemporary Management of Carotid Disease What We Know So Far
 Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Contemporary Management of Carotid Disease What We Know So Far Ammar Safar, MD, FSCAI, FACC, FACP, RPVI Interventional Cardiology & Endovascular Medicine Disclosers NONE Epidemiology 80 % of stroke are
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Carotid artery disease: stenting vs endarterectomy
 British Journal of Anaesthesia 105 (S1): i34 i49 (2010) doi:10.1093/bja/aeq319 NEUROSCIENCES AND NEUROANAESTHESIA Carotid artery disease: stenting vs endarterectomy K. M. Erickson* and D. J. Cole Mayo
British Journal of Anaesthesia 105 (S1): i34 i49 (2010) doi:10.1093/bja/aeq319 NEUROSCIENCES AND NEUROANAESTHESIA Carotid artery disease: stenting vs endarterectomy K. M. Erickson* and D. J. Cole Mayo
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough
 Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Todd W GenslerMD April 28, 2018 CAROTID DEBATE High-Grade Asymptomatic Disease Should Be Repaired Selectively; Medical Management is NOT Enough DISCLOSURES I have no financial disclosures Presenter name
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cardiothoracic Fellow Expectations Division of Cardiac Anesthesia, Beth Israel Deaconess Medical Center
 The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
The fellowship in Cardiothoracic Anesthesia at the Beth Israel Deaconess Medical Center is intended to provide the foundation for a career as either an academic cardiothoracic anesthesiologist or clinical
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Cerebral hyperperfusion syndrome after carotid angioplasty
 case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
case report Cerebral hyperperfusion syndrome after carotid angioplasty Zoran Miloševič 1, Bojana Žvan 2, Marjan Zaletel 2, Miloš Šurlan 1 1 Institute of Radiology, 2 University Neurology Clinic, University
Carotid endarterectomy as complex intraoperative monitoring
 Carotid endarterectomy as complex intraoperative monitoring Dr. Cristina Tudor 1, Dr. Ramona Jemna 1, Dr. Horia Muresian 2, Conf. Dr. Elena Copaciu 1 1 Clinica Anestezie-Terapie Intensiva, Spitalul Universitar
Carotid endarterectomy as complex intraoperative monitoring Dr. Cristina Tudor 1, Dr. Ramona Jemna 1, Dr. Horia Muresian 2, Conf. Dr. Elena Copaciu 1 1 Clinica Anestezie-Terapie Intensiva, Spitalul Universitar
Implanting a baroreceptor stimulation device for resistant hypertension
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Implanting a baroreceptor stimulation device for resistant hypertension Hypertension (or high blood pressure)
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Implanting a baroreceptor stimulation device for resistant hypertension Hypertension (or high blood pressure)
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases
 Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Carotid Stenosis (carotid artery disease)
") 1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
Fast-track CEA: a 3-year experience
 Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
Fast-track CEA: a 3-year experience Giorgio L. Poletto, MD Milano, Italy 6th ACST-2 Collaborators Meeting, Palau de Congresos, Valencia. 24th and 25th September 2018. Stroke prevention Primary prevention:
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH
 ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
ESC Congress 2011 SIMULTANEOUS HYBRID REVASCULARIZATION OF CAROTID AND CORONARY DISEASE IN PATIENTS WITH ACUTE CORONARY SYNDROME: INITIAL RESULTS OF A NEW THERAPEUTIC APPROACH AUTHORS: Marta Ponte 1, RICARDO
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
IOM at University of. Training for physicians. art of IOM. neurologic. injury during surgery. surgery on by IOM. that rate is.
 Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
Topics covered: Overview of science and art of IOM IOM at University of Michigan Hospital and Health Systems What is the purpose of Intraoperative monitoring? Training for physicians Overview of science
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions. No Disclosures. Prevalence >70% Asymptomatic ICA Stenosis*
 How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
How Duplex Ultrasound Screening Can Lead to Overuse of Carotid Interventions Gregory L. Moneta, M.D. Chief, Division of Vascular Surgery Department of Surgery Knight Cardiovascular Institute Oregon Health
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Transcatheter Aortic Valve Implantation Procedure (TAVI)
") Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Page 1 of 5 Procedure (TAVI) Introduction Aortic stenosis (AS) is a common heart valve problem associated with heart failure and death. Surgical valve repair or replacement is recommended if AS patients
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk
 Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk Amy B. Reed, MD, a Peter Gaccione, MA, b Michael Belkin, MD, b Magruder C. Donaldson, MD, b John A. Mannick, MD,
Preoperative risk factors for carotid endarterectomy: Defining the patient at high risk Amy B. Reed, MD, a Peter Gaccione, MA, b Michael Belkin, MD, b Magruder C. Donaldson, MD, b John A. Mannick, MD,
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION
 FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION CPT/HCPCS Codes 93875 Non-invasive physiologic studies of extracranial arteries, complete bilateral study (eg, periorbital
FIRST COAST SERVICE OPTIONS FLORIDA MEDICARE PART B LOCAL COVERAGE DETERMINATION CPT/HCPCS Codes 93875 Non-invasive physiologic studies of extracranial arteries, complete bilateral study (eg, periorbital
Current Reviews for Nurse Anesthetists
 Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board CHUCK BIDDLE, CRNA Ph.D Richmond, Virginia MONTE LICHTIGER, MD Coral
Current Reviews for Nurse Anesthetists Publisher And Editor-in-Chief FRANK MOYA, MD Coral Gables, Florida Editorial Board Advisory Board CHUCK BIDDLE, CRNA Ph.D Richmond, Virginia MONTE LICHTIGER, MD Coral
Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
 Case Reports in Vascular Medicine Volume 2013, Article ID 207602, 4 pages http://dx.doi.org/10.1155/2013/207602 Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
Case Reports in Vascular Medicine Volume 2013, Article ID 207602, 4 pages http://dx.doi.org/10.1155/2013/207602 Case Report Cerebral Hyperperfusion Syndrome following Protected Carotid Artery Stenting
Preoperative assessment of a patient for carotid endarterectomy
 Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Vascular Carotid endarterectomy Preoperative assessment of a patient for carotid endarterectomy Abdominal aortic aneuysm Thoracic aortic aneurysms Vascular 3.D.2.1 James Mitchell (December 24, 2003) Carotid
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Goals and Objectives of the Educational Program
 Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
Goals and Objectives of the Educational Program Neurosurgical Fellowship Definition: This fellowship is designed to give concise and formal training in neurosurgical anesthesia at LAC+USC Medical Center
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Any vascular studies performed should be as a result of, or to complement, a thorough patient evaluation and neurological examination.
 National Imaging Associates, Inc. Clinical guidelines NON-INVASIVE CEREBROVASCULAR ARTERIALS TUDIES Original Date: October 2015 Page 1 of 8 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes: Please refer to page
National Imaging Associates, Inc. Clinical guidelines NON-INVASIVE CEREBROVASCULAR ARTERIALS TUDIES Original Date: October 2015 Page 1 of 8 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes: Please refer to page
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Corporate Medical Policy
 Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
Corporate Medical Policy Endovascular Therapies for Extracranial Vertebral Artery Disease File Name: Origination: Last CAP Review: Next CAP Review: Last Review: endovascular_therapies_for_extracranial_vertebral_artery_disease
This quiz is being published on behalf of the Education Committee of the SNACC.
 Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Section Editor Scott E Kasner, MD
 1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33361-33369, 33200-37186, 37195-37785, 92950-93272,
The contribution of the external carotid artery to cerebral perfusion in carotid disease
 The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
The contribution of the external carotid artery to cerebral perfusion in carotid disease Shirley J. Fearn, PhD, FRCS, Andrew J. Picton, BSc, Andrew J. Mortimer, MD, FRCA, Andrew D. Parry, MBChB, FRCS,
Extracranial Carotid Artery Stenting With or Without Distal Protection Device
 Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
Extracranial Carotid Artery Stenting With or Without Distal Protection Device Eak-Kyun Shin MD. Professor of Medicine Division of Cardiology, Heart Center, Gil Medical Center Gacheon Medical School Incheon,
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Outcome
 Measure #344: Rate of Carotid Artery Stenting (CAS) for Asymptomatic Patients, Without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Effective Clinical
Measure #344: Rate of Carotid Artery Stenting (CAS) for Asymptomatic Patients, Without Major Complications (Discharged to Home by Post-Operative Day #2) National Quality Strategy Domain: Effective Clinical
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2): Oxford University Press
: Oxford University Press") Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Posted: 11/27/2011 on Medscape; Published Br J Anaesth. 2011;107(2):209-217. 2011 Oxford University Press Effect of Phenylephrine and Ephedrine Bolus Treatment on Cerebral Oxygenation in Anaesthetized
Feasibility and Safety of Simultaneous Carotid Endarterectomy and Carotid Stenting for Bilateral Carotid Stenosis
 Feasibility and Safety of Simultaneous Carotid Endarterectomy and Carotid Stenting for Bilateral Carotid Stenosis Zhidong Ye, Jianbing Zhang, Peng Liu et al. Dept. of Cardiovascular Surgery China-Japan
Feasibility and Safety of Simultaneous Carotid Endarterectomy and Carotid Stenting for Bilateral Carotid Stenosis Zhidong Ye, Jianbing Zhang, Peng Liu et al. Dept. of Cardiovascular Surgery China-Japan