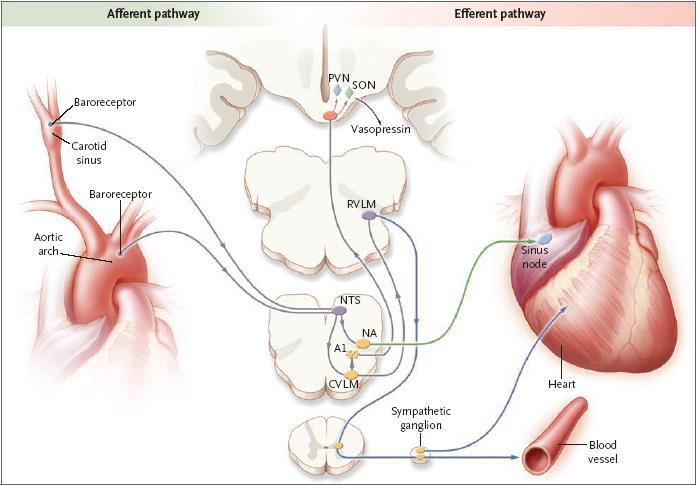
Role of Sympathetic Nervous System in Hypertension
|
|
|
- Cecily Thompson
- 6 years ago
- Views:
Transcription
1 Role of Sympathetic Nervous System in Hypertension
2 BP = CO x PVR SV HR
3 DEFENSE REACTION Suppressed vagal activity Increased sympathetic activity to heart, veins, kidneys, splachnic region, skin Skeletal muscle vasodilation Centralization of blood volume Rate dependent increase of C.O. Enhanced intestinal salt/water absorption Suppressed renal salt/water excretion Increased salt appetite
4 DEFENCE REACTION Long term Effects Renin-angiotensin-aldosterone release with positive feedback to sympathetic NS ACTH-glucocorticoid system ADH system Metabolic effects, trophic influences, modulating membrane ionic events

5 Pre-synaptically Receptors reinforce while the 2 receptor inhibits the release of nor-epinephrine into the synaptic cleft 1 receptor mediates vasoconstriction 2 also mediates vasoconstriction post-synaptically, but is part of a negative feedback loop presynaptically
6 SYMPATHETIC NERVE SYSTEM in HYPERTENSION In young people with a family history of Htn, or young people with hypertension, studies have found them to have a hyper-dynamic circulatory system that evolves over time
7 LONG TERM HEMODYNAMIC CHANGES Initial Hyperkinetic Circulatory State Beta- increases C.O. Alpha- level too active and does not allow for a reduction in PVR Normalized C.O. and Increased S.V.R. Reduced beta- tone with age Unopposed alpha tone leaves a high PVR
8 DOES STRESS LEAD TO HYPERTENSION? Long term studies are now reporting that people who tested as high in anxiety/stress many years ago, are now more likely to be hypertensive compared to those persons who tested low in anxiety, etc Domains such as demand and control in the workplace, coupled with certain lifestyle issues (alcohol) also predict who is more likely to become hypertensive
9 Effects of Age & Gender With age, especially after age 40 yrs, sympathetic nervous activity increases, especially in women For each increase of 10 bursts/min in MSNA, the mean increase in MAP for men is 2.7 mmhg and 6.1 mmhg for women

10 SNS Activity & MAP with Age
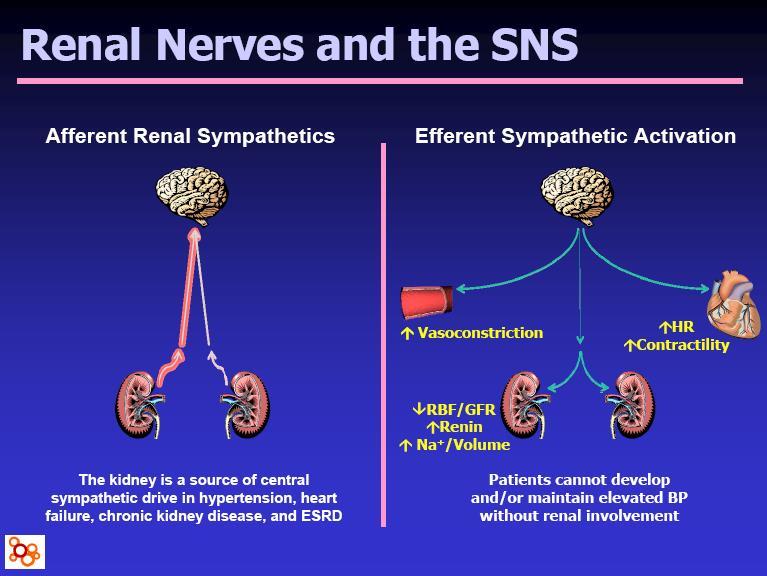
11 RENAL RESPONSE TO SYMPATHETIC NERVE STIMULATION Response increases with level of stimulation with: Increased renin secretion rate Decreased Na excretion with volume expansion Decreased GFR and RBF
12 HYPERINSULINEMIA in OBESITY and the SNS Hyperinsulinemia leads to increased SNS activity Increased cardiac output Increased systemic vascular resistance Increased BP Increased Na reabsorption
13 Questions??
14 What classes of anti-hypertensive drugs should be considered in stage 1 or stage 2 hypertension?
15 CHEP Guidelines: Systolic/Diastolic Hypertension Without Compelling Indications Target <140/90 mmhg Lifestyle modification Initial drug therapy Thiazide or thiazide-like diuretic ACEI ARB Long-acting CCB Beta-blocker* The combination of an ACEI + ARB should only be considered in selected and closely monitored people with advanced heart failure or proteinuric nephropathy Dual combination Triple or quadruple therapy CONSIDER Nonadherence Secondary HTN Interfering drugs or lifestyle White coat effect A combination of two first-line drugs may be considered as initial therapy if BP 20 mmhg systolic or 10 mmhg diastolic above target ACEI, ARB and direct renin inhibitors are contraindicated in pregnancy and caution is required in prescribing to women of child bearing potential *Not indicated as first line therapy over 60 years ACEI = Angiotensin-converting enzyme inhibitor; ARB = Angiotensin II receptor blocker; CCB = Calcium channel blocker; CHEP Guidelines. 19
16 Beta-Blocker Meta-analysis: Lindholm et al Compared with other antihypertensives, BBs were associated with: BUT 16% increase in stroke (p = 0.009) 3% increase in all-cause mortality (NS) Pooled end point was heterogeneous and largely driven by studies with mean age 60 years No differences in MI, death or heart failure between BBs and other antihypertensives 14 of 18 studies used atenolol as the BB (86% of patients) 4 trials used mixtures of atenolol, metoprolol, pindolol and/or propranolol (all 1st or 2nd generation BBs) BB = Beta-blockers; MI = Myocardial infarction; NS = Not statistically significant Lindholm LH, et al. Lancet 2005;366: Khan N and McAlister FA CMAJ 2006;174(12):
17 CHEP Position Statement on Beta-Blockers Beta-blockers are equally effective at reducing cardiovascular events as other BP-lowering classes in younger patients (< 60 years) Beta-blockers are strongly indicated in older hypertensive patients with angina, post-myocardial infarction or with congestive heart failure Beta-blockers reduce cerebrovascular events to a lesser extent than other BP-lowering drugs in older patients with uncomplicated hypertension Campbell N. 21
18 What are the key differences among the beta-blockers?
19 Evolution of Beta Blockers in Canada 1 st Generation 2 nd Generation 3 rd Generation Non-Selective Selective Vasodilating (alpha blockade) Non-Selective Vasodilating & Selective Propranolol Atenolol Metoprolol Bisoprolol Carvedilol* Labetalol Nebivolol *Not approved for Hypertension in Canada Poirier L, Lacourcière, Y. Can J Cardiol 2012; 28: BYSTOLIC (nebivolol tablets) Product Monograph, Forest Laboratories Canada Inc.,
20 Selectivity of Beta-Blockers Receptor Location Selected action Alpha 1 Most vascular arteries and veins Sphincters of the bladder and GI tract Penis Iris dilator Smooth muscle contraction Beta 1 Heart muscle Salivary glands Fat cells Beta 2 Bronchioles of lung Arterioles of skeletal muscles, brain and lungs Bladder wall GI tract Heart muscle contraction Smooth muscle relaxation GI = Gastrointestinal Hoffman BB, et al. In: Goodman and Gilman's: The Pharmacological Basis of Therapeutics. NY: McGraw-Hill, 2001:
21 1 / 2 selectivity Beta 1 Receptor Selectivity of Nebivolol (Human Myocardium) Bucindolol Propranolol Carvedilol * Metoprolol Bisoprolol Nebivolol *In Canada, carvedilol is indicated for heart failure only Beta 1 selectivity = K i ( 2 ) / K i ( 1 ). In extensive metabolizers and at doses less than or equal to 20 mg, nebivolol is preferentially beta 1 selective Bristow M. Am J Hypertens 2005;18(Part 2):51A-52A. 25
22 Pharmacologic Characteristics of Beta-Blockers beta1 / beta2 selectivity Nonselective beta-adrenergic antagonists Half-life (h) Lipophilicity Vasodilation Nadolol Low N/A Propranolol High N/A Selective beta-adrenergic antagonists Atenolol Low N/A Bisoprolol Moderate N/A Metoprolol High N/A Nebivolol High Alpha1-adrenergic and beta-adrenergic antagonists Labetalol Low Carvedilol* Moderate Endothelium-dependent, NO-mediated vasodilation 1 -adrenergic blocking activity; direct 2 vasodilatory activity 1 -adrenergic blocking activity, vasodilation *In Canada, carvedilol is indicated for heart failure only ISA = Intrinsic sympathomimetic activity, MSA = Membrane-stabilizing activity; N/A = Not applicable; NO = Nitric oxide Adapted from Mason RP, et al. J Cardiovasc Pharmacol 2009;54:
23 Adverse Events Commonly Associated with Beta-Blockers Bradycardia Dizziness Vertigo Fatigue Diarrhea Nausea Erectile dysfunction Cold extremeties Tenormin Product Monograph, Sept 2011 Inderal Product Monograph, Sept 2012 Rosen RC, et al. Arch Sex Behav 1988;17:


24 Hemodynamics of Non-vasodilating Beta-Blockers Beta-blockade: BP Reduction and Hemodynamic Change Peripheral resistance Stroke volume Cardiac output Heart rate The general direction of hemodynamic change described above is typical in patients receiving a beta-blocker without vasodilatory properties. The hemodynamic profile will vary based on betareceptor selectivity and patient-specific factors Lund-Johansen P, et al. Cardiovasc Drugs Ther 1991;5:
25 Percent change vs. baseline Beats per minute Hemodynamics of Nebivolol (5 mg) vs. Atenolol (100 mg) in Patients with Hypertension * 5.8 Peripheral resistance (dyne/cm -5 ) 20.6* 3.6 Stroke volume (ml) Nebivolol 5 mg qd (n = 12) Atenolol 100 mg qd (n = 13) * * Cardiac output -25 Heart rate (L/min) (bpm) The clinical significance of these changes is unknown *p < 0.05 nebivolol versus atenolol Systolic/diastolic BP reductions were -19/-12 mmhg for nebivolol and -16/-7 mmhg for atenolol Parameters measured at 2 weeks. Adapted from Kamp O, et al. Am J Cardiol 2003;92:
26 What new beta-blocker is available for the management of hypertension?
27 Nebivolol: A Novel 3rd Generation Beta-Blocker Indicated for the treatment of mild to moderate hypertension, to lower BP Cardioselective beta-blocker with vasodilating properties Effective as monotherapy, combination therapy, and in populations which do not typically respond to beta-blocker therapy Maintains cardiac output and exercise tolerance Associated with a low incidence of side effects Van de Water A, et al. J Cardiovasc Pharmacol 1988;11:552-63; Bystolic Product Monograph, January Saunders E et al. J Clin Hypertens. 2007;9: ; Germino FW Clin Ther 2009;31:
28 Mean change in blood pressure from baseline (mmhg) Nebivolol Monotherapy Pooled Data: Change in Blood Pressure n Baseline BP (mmhg) 152.2/ / / /99.2 Dose Placebo Nebivolol 5 mg Nebivolol 10 mg Nebivolol 20 mg * -10.8* -10.7* -10.5* SBP DBP *p < for all pairwise comparisons of active treatment vs. placebo DBP = Diastolic blood pressure; SBP = Systolic blood pressure Germino FW. Clin Ther 2009;31: * -11.1* 33
29 Nebivolol Monotherapy Pooled Data: Adverse Events The most common adverse events occurring in 2% of patients taking nebivolol monotherapy Adverse Events Placebo (n=205) % Nebivolol 5 mg (n=459) % Nebivolol 10 mg (n=461) % Nebivolol 20 mg (n=460) % Headache Fatigue Nasopharyngitis Dizziness Diarrhea Upper Respiratory Tract Infection Bystolic (nebivolol tablets) Product Monograph, Forest Laboratories Canada Inc., January 2013
30 Effect of Nebivolol vs. Metoprolol on Erectile Function: Study Design Nebivolol 5 mg qd Metoprolol 95 mg qd n = 48 Washout (2 weeks) Metoprolol 95 mg qd Washout (2 weeks) Nebivolol 5 mg qd Screening Baseline Assessment 12 weeks Cross-over Assessment 12 weeks Brixius K, et al. Clin Exper Pharmacol Phys 2007;34:
31 Change in score from baseline Effect of Nebivolol vs. Metoprolol on Erectile Function: IIEF Nebivolol 5 mg Metoprolol 100 mg * Erectile function Orgasmic function Sexual desire Intercourse satisfaction Overall satisfaction *p < 0.05 vs. baseline; p < 0.05 vs. metoprolol IIEF = International Index of Erectile Function Brixius K et al. Clin Exper Pharmacother 2007;34:
32 Sitting SBP (mmhg) Sitting DBP (mmhg) Nebivolol vs. Amlodipine: Change in BP Nebivolol mg/day (n = 81) Amlodipine 5-10 mg/day (n = 87) Weeks Weeks *p < 0.05 between the groups DBP = Diastolic blood pressure; SBP = Systolic blood pressure Mazza A, et al. Blood Press 2002;11:182-8 * * 37

33 Frequency of adverse events (n) Nebivolol vs. Amlodipine: Tolerability *p = vs. nebivolol Mazza A, et al. Blood Press 2002;11:
34 Nebivolol: Contraindications Severe bradycardia (generally < 50 bpm before start of therapy) Cardiogenic shock Decompensated heart failure Second or third degree atrioventricular block Sick sinus syndrome or sinoatrial block Severe hepatic impairment (Child-Pugh >B) Severe peripheral arterial circulatory disorders Hypersensitivity to any component of this product bpm = beats per minute Bystolic (nebivolol tablets) Product Monograph, Forest Laboratories Canada Inc., January
35 Summary: Beta-blockers in Hypertension Beta-blockers are equally effective at reducing CV events as other BP-lowering classes in younger patients (< 60 years) 1 Beta-blockers are recommended as a first-line option for patients (with uncomplicated hypertension <60 years of age), as add-on therapy, and for hypertensive patients with angina, post-mi or congestive HF (CHEP 2013) 2 Beta-blockers are a heterogeneous class 3 Outcomes seen in older clinical trials seem to be more of a drug effect than a class effect Newer vasodilatory beta-blockers such as nebivolol are promising 5 BP = Blood pressure; CV = Cardiovascular; HF = Heart failure; MI = Myocardial infarction 1. Khan N, McAlister FA. CMAJ 2006;174: CHEP Guidelines Mason RP, et al. J Cardiovasc Pharmacol 2009;54: Dhakam Z, et al. J Hypertens 2008;26:351-6; 5. Kuroedov A, et al. Cardiovas Drug Rev 2004;22:
36 NeuroModulation or Denervation for Hypertension Management

37 Breathing Control Device- RESPERATE





38 The CVRx Rheos System Programming System Baroreflex Activation Leads Implantable Pulse Generator 43
39


40 45 Ability to Personalize and Control the Therapy
41

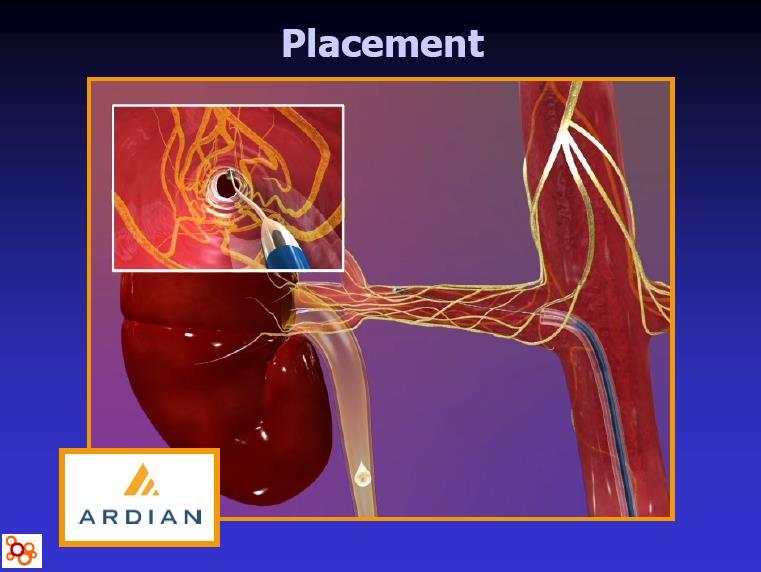
42 Renal Sympathetic Innervation
43
44

45 Ablation Catheter has electrodes on Multiple sites along Sides of the Catheter
46 Blood-pressure changes (mm Hg) in resistant hypertension patients with and without renal denervation Time mo Renal denervtn (n=45) Nontreated (n=5) 1-14/-10 +3/ /-10 +2/ / / / / / -17 Krum H et al. Lancet 2009
47 Conclusions The SNS plays an important role in the development and maintenance of htn Beta-blockers, particularly vasodilating beta-blockers, can be useful in lowering BP Medical devices for SNS denervation should be considered investigational until there is a better understanding of adverse effects.
48 Questions??
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Should beta blockers remain first-line drugs for hypertension?
 1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Beta blockers in primary hypertension. Dr. Md. Billal Alam Associate Professor of Medicine DMC
 Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
LESSON ASSIGNMENT Given the trade and/or generic name of an adrenergic blocking agent, classify that agent as either an alpha or beta blocker.
 LESSON ASSIGNMENT LESSON 8 Adrenergic Blocking Agents. TEXT ASSIGNMENT Paragraphs 8-1 through 8-5. LESSON OBJECTIVES 8-1. Given a group of statements, select the statement that best describes one of the
LESSON ASSIGNMENT LESSON 8 Adrenergic Blocking Agents. TEXT ASSIGNMENT Paragraphs 8-1 through 8-5. LESSON OBJECTIVES 8-1. Given a group of statements, select the statement that best describes one of the
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Structure and organization of blood vessels
 The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
The cardiovascular system Structure of the heart The cardiac cycle Structure and organization of blood vessels What is the cardiovascular system? The heart is a double pump heart arteries arterioles veins
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Angina pectoris due to coronary atherosclerosis : Atenolol is indicated for the long term management of patients with angina pectoris.
 Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Lonet Tablet Description Lonet contains Atenolol, a synthetic β1 selective (cardioselective) adrenoreceptor blocking agent without membrane stabilising or intrinsic sympathomimetic (partial agonist) activity.
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Adrenergic Receptor as part of ANS
 Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
- Dr Alia Shatnawi. 1 P a g e
 - 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
- 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
Chapter 10 Worksheet Blood Pressure and Antithrombotic Agents
 Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
Complete the following. 1. A layer of cells lines each vessel in the vascular system. This layer is a passive barrier that keeps cells and proteins from going into tissues; it also contains substances
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1
 Lecture 14 Cardiovascular control mechanisms p. 1") BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
First line treatment of primary hypertension
 First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Role of Minerals in Hypertension
 Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
Role of Minerals in Hypertension Lecture objectives By the end of the lecture students will be able to Define primary and secondary hypertention and their risk factors. Relate role of minerals with hypertention.
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center
 Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Blood Pressure. a change in any of these could cause a corresponding change in blood pressure
 Blood Pressure measured as mmhg Main factors affecting blood pressure: 1. cardiac output 2. peripheral resistance 3. blood volume a change in any of these could cause a corresponding change in blood pressure
Blood Pressure measured as mmhg Main factors affecting blood pressure: 1. cardiac output 2. peripheral resistance 3. blood volume a change in any of these could cause a corresponding change in blood pressure
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Nurse-sensitive factors in hypertension management
 Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Beta Blockade: Protection or Panacea
 Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
Beta Blockade: Protection or Panacea Jason Axt Jason s Recommendations Perioperative β Blockade (BB) If on BB stay on If Vascular Sx + documented ischemia - start. 2+ risk factors - start Use in isolated
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Combining Antihypertensives in People with Diabetes
 Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets
 METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25
METOTRUST XL-25/50 Metoprolol Succinate Extended-Release Tablets COMPOSITION Each film-coated tablet of Metotrust XL-25 contains: Metoprolol Succinate USP 23.75 mg equivalent to Metoprolol Tartrate 25