Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
|
|
|
- Stella Sullivan
- 6 years ago
- Views:
Transcription

1 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional Cardiology Zena and Michael a Weiner Professor of Medicine Mount Sinai Hospital, NY


2 Aortic Stenosis Aortic valve area: Ross J, Braunwald E. Circulation 1968; 38: Normal 3-4 cm 2 AS: - mild >1.5 cm 2 - moderate cm 2 - severe <1.0 cm 2 - critical <0.7 cm 2 Etiology: Congenital: unicuspid bicuspid tricuspid Acquired: 5% at 70 yrs 10% at 80 yrs 18% at 90 yrs rheumatic calcific cholesterolemia rheumatoid
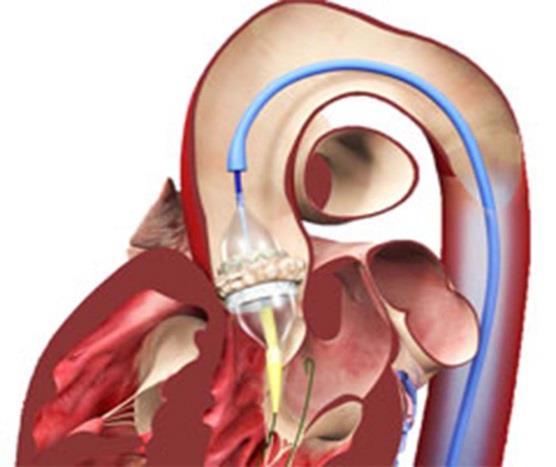
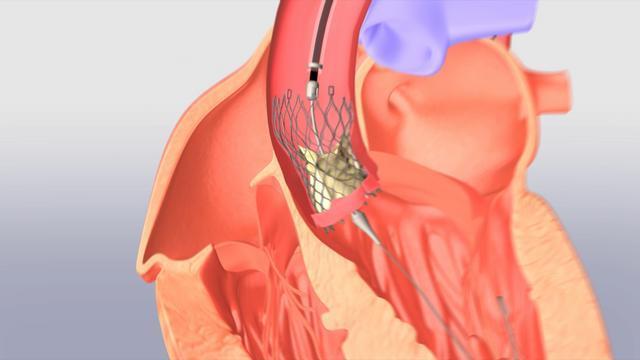
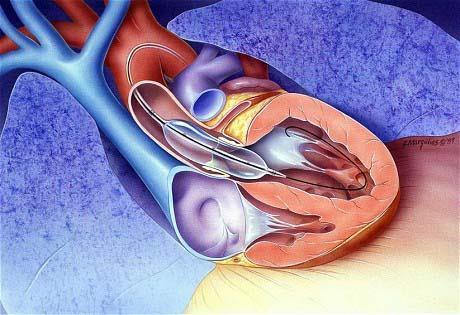
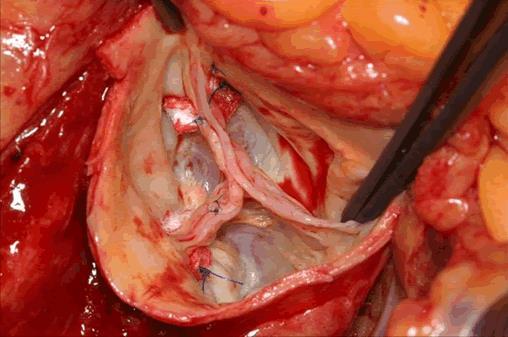
3 Interventional Choices for AS: SAVR TAVR BAV Sapien CoreValve
4
5 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
6 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
7 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
8 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
9 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1
10 Summary of Recommendations for AS: Choice of Surgical or Transcatheter Intervention BAV may provide palliative symptomatic benefit in these pts Nishimura et al., J Thorac Cardiovasc Surg 2014;148:e1







 Primary Endpoint: All")
 Primary Endpoint:")
11 Leon et al, NEJM 2010;363:1597 PARTNER US Trial: Study Design Symptomatic Severe Aortic Stenosis ASSESSMENT: High Risk AVR Candidate 3105 Total Patients Screened Total = 1058 patients n= 700 High-surgical risk Gp In-operable 2 Parallel Trials STS >10% Cohort A Gp Cohort B n=358 ASSESSMENT: Transfemoral Access ASSESSMENT: Transfemoral Access High Risk TF High Risk TA Yes No 1:1 Randomization 1:1 Randomization 1:1 Randomization Not In Study TAVR Trans Femoral VS Surgical AVR TAVI Trans Apical VS Surgical AVR TAVR Trans Femoral VS Standard Therapy (usually BAV) Primary Endpoint: All Cause Mortality (1 yr) (Non-inferiority) Primary Endpoint: All Cause Mortality over length of trial (Superiority)
12 PARTNER Trial Cohort B: Time-to-Event Analysis of Key Endpoints During 2 Years Follow-up Rate of Death From Any Cause 5yrs 94% Rate of Re-hospitalization 71% 20% Makkar et al., NEJM 2012;366:1696
13 PARTNER Trial Cohort A: Time-to-Event Curves for Primary Endpoints at 3-Yrs Death from Any Cause, Intention-to-Treat Population Death from Any Cause, As-Treated Population Kodali et al., NEJM 2012;366:1686
 High Risk Incremental STS mortality >15% Iliofemoral Access")

14 CoreValve Pivotal Trials Study Design CoreValve US Pivotal Trials Extreme Risk (Inoperable; STS mortality/morbidity >50%) High Risk Incremental STS mortality >15% Iliofemoral Access for 18 Fr Sheath Presented in TCT 2013 Yes No Randomization 1:1 N=790 Presented in ACC 2014 Versus CoreValve Iliofemoral CoreValve Non- Iliofemoral CoreValve SAVR N=487 N=147 N=392 N=388


15 CoreValve Extreme Risk Study: Primary Endpoints N= Year Mortality Major Stroke Popma et al, TCT 2013; JACC May 2014
 TAVR (N=")

16 All-cause Mortality (%) CoreValve High Risk Pivotal trial: Primary Endpoint-- 1 Year All-cause Mortality Surgical (N= 357) TAVR (N= 390) 19.1% 14.2% 4.5% P = 0.04 for superiority 3.3% Months Post-Procedure Adams et al., N Engl J Med 2014;370:1790

17 CoreValve High-risk Pivotal Trial: 1-Year Results SAVR (n=357) TAVR (n=390) p=<0.001 p=0.03 % p=0.10 p=<0.001 p=<0.001 p=0.59 p=0.004 Any stroke Major stroke AKI PPM Vasc MACCE Life-threatening/ compl disabling bleeding Adams et al., N Engl J Med 2014;370:1790
 N = 159 86 70 44 31 15 163 91 71")
18 Mean Gradient (mmhg) PARTNER Trial: Aortic Mean Gradient & Valve Area EOA Mean Gradient Error bars = ± 1 Std Dev Valve Area (cm²) N =


19 MEAN GRADIENT (mg) Mean Gradient Aortic Valve Area ± ± ± AVA (cm 2 ) ± ± ±5.7 Baseline Post TAVR 5 Year

20 Partner Trial Cohort B: TAVR for Inoperable Severe Aortic Stenosis; Impact of Co-morbidities Makkar et al., NEJM 2012;366:1696
21 What about Intermediate risk AS patients; (defined as STS mortality risk of 4 to 8-10%) Two Trials: PARTNER IIA (completed) SURTAVI Trial (ongoing)
22 CoreValve US Pivotal SURTAVI Trial: Design Severe AS Indication for AVR Separate randomization for AS+CAD Heart Team Discussion N = 1100 Europe: STS mortality risk score > 3% and < 8% US: STS mortality risk score > 4 and < 10% 1:1 Randomization Suitable for Randomization Non-randomization Registries TAVI AVR Control TAVI VS AVR VS Yes Primary Endpoint: All cause Mortality and Stroke at 2 yrs N = 220 No Medical Management N = 1760 N = 220 Endpoint: All-cause Mortality at 2 yrs

23 The PARTNER II Trial Study Design
24 Patient History Age (years): 90 Gender: M Height (ins): 72 Weight (Ibs): 160 The patient has the following: CARDIAC STATUS NYHA Class IV RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM Chronic Lung Disease/ COPD: Moderate FEV1: 1500cc %predicted: 55 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013 Creatinine (mg) /dl: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/ml): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe
 0.")
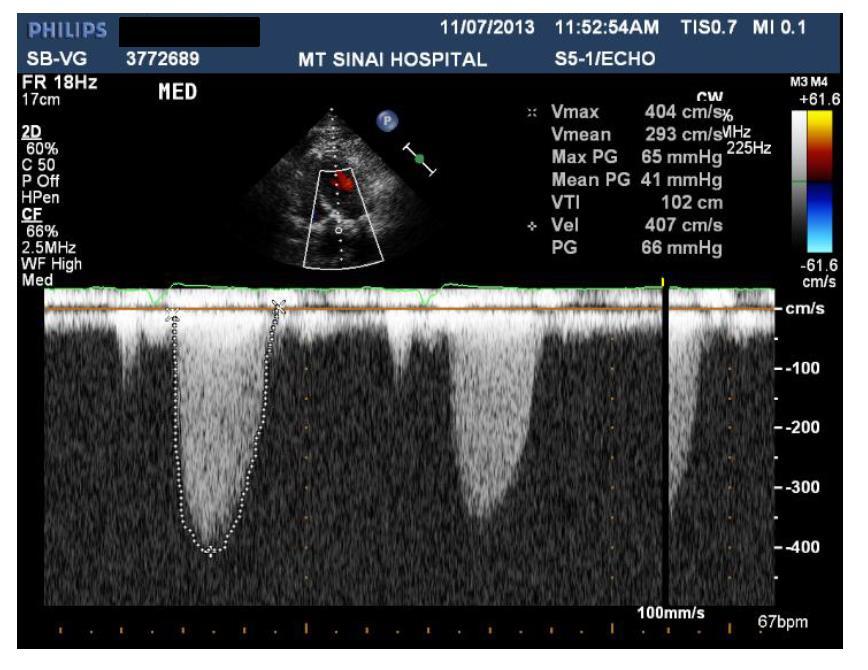
 48 Mean")
25 Echo Images: Annulus Measurement Echo Image 22 Aortic annular size (mm) 0.41 Aortic valve area (cm 2 ) Aortic valve area index (cm 2 /m 2 ) 48 Mean gradient (mmhg) 4.4 Peak velocity (m/sec) 52 LVEF (%)
 32.8 Max ascending Aorta diameter 35.8 39.3 Sinus of Valsalva diameter 23.5 30.5 Sinus of Valsalva height 29.5 30.9 Sinotubular Junction width (STJ) (all in mm)")
26 CT Images: Annulus Measurements CT Image Ao Annulus mean diameter: 28.0 mm 32.6 x 23.4 Major x Minor aortic annulus diam 89.2 Aortic Annulus perimeter (28.4 x 3.14) 32.8 Max ascending Aorta diameter Sinus of Valsalva diameter Sinus of Valsalva height Sinotubular Junction width (STJ) (all in mm)
27 CT 3D Reconstructions
28 Patient History Age (years): 90 Gender: M Height (ins): 72 Weight (Ibs): 160 Risk Summary: STS Score: 12% mortality 39% morbidity/mortality The patient has the following: CARDIAC STATUS NYHA Class IV RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM Chronic Lung Disease/ COPD: Moderate FEV1: 1500cc %predicted: 55 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013 Creatinine (mg) /dl: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/ml): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe
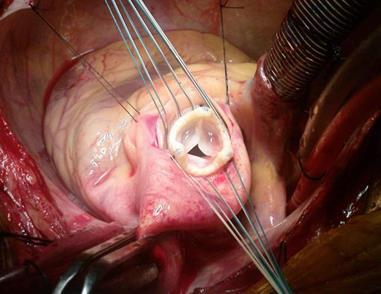
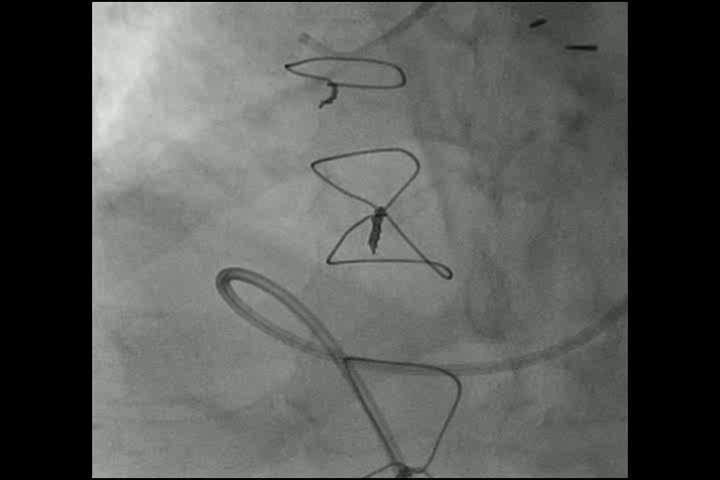
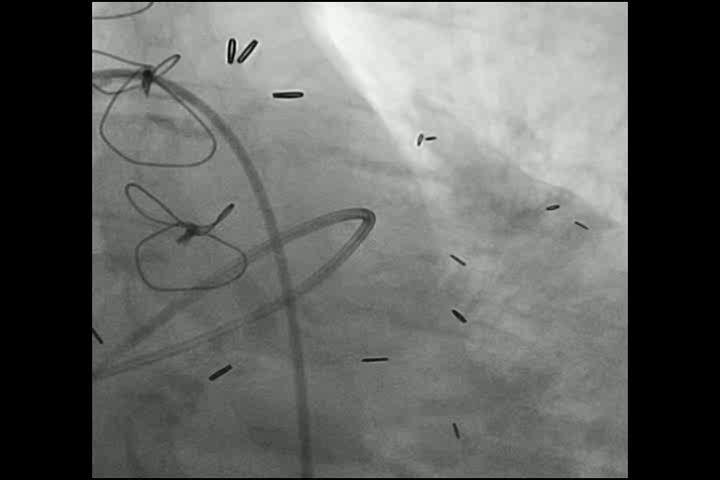
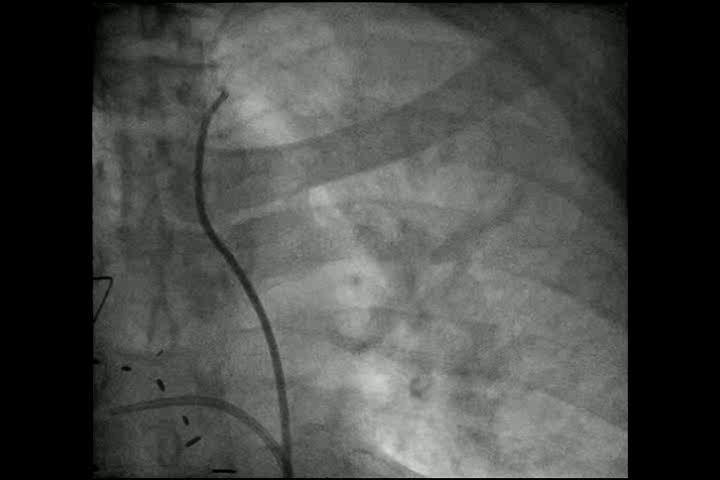
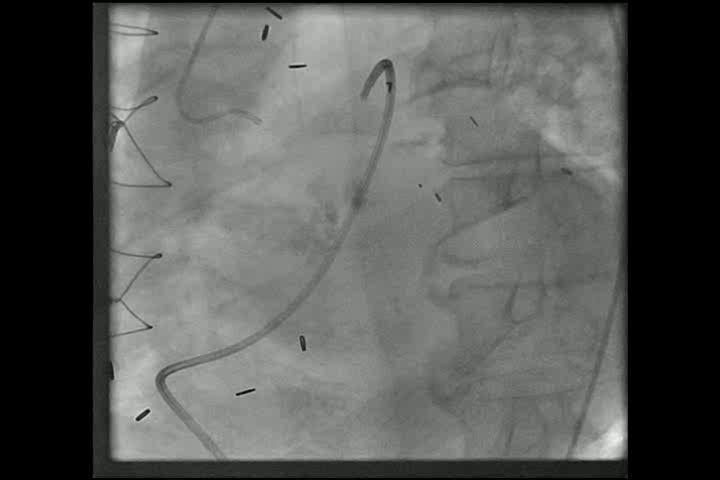
29 Treatment of Choice in this 90 Yr old AS pt?re-bav?savr?tavr TAVR because - 12% STS risk score making him high risk for conventional SAVR Pt underwent 31mm CoreValve via RFA percutaneous approach (using 2 perclose sutures) under conscious sedation.
30
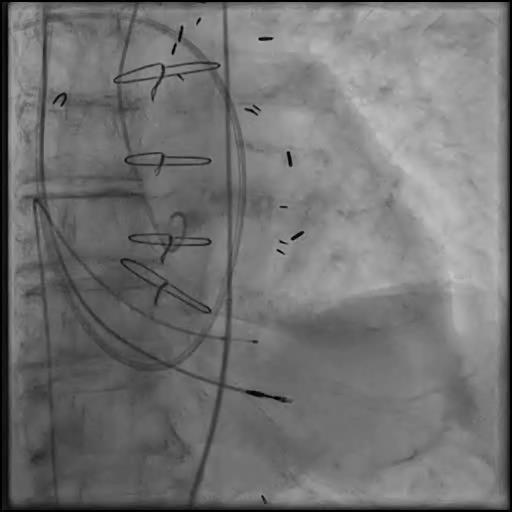
31

32

33

34

35
36 Treatment of Choice in this 90 Yr old AS pt?re-bav?savr?tavr TAVR because - 12% STS risk score making him high risk for conventional SAVR Pt underwent 31mm CoreValve via RFA percutaneous approach (using 2 perclose sutures) under conscious sedation. No complications, out of CCU next day and discharged on post TAVR day 5.
37 Patient History Age (years): 90 Gender: M Height (ins): 72 Weight (Ibs): 160 Risk Summary: STS Score: 32% mortality 69% morbidity/mortality The patient has the following: CARDIAC STATUS NYHA Class IV RISK FACTORS AND COMORBIDITIES History of CVA, previous CABG x4, chronic persistent A-Fib, s/p PPM Chronic Lung Disease/ COPD: Severe FEV1: 500cc %predicted: 25 Other: Frail, history of multiple GI bleeds, hyponatremia PREVIOUS CARDIAC INTERVENTIONS: CABG x4 in 1991, PCI x3 in remote and BAV in July 2013 Creatinine (mg) /dl: 1.03 Creatinine clearance (cc/min) : 60 BNP (pg/ml): 717 Coronary Art Disease: 3 Patent grafts Aortic Calcification: Severe
38 Treatment of Choice in this 90 Yr old AS pt?re-bav?savr?tavr Re-BAV because - This pt with high comorbidity (FEV1 <500 cc) has extremely poor 1 year survival and TAVR is unlikely to improve the long-term survival - BAV will provide palliative symptomatic relief in these pts
39 Patient History Age (years): 71 Gender: M Height (ins): 66 Weight (Ibs): 170 The patient has the following: NYHA Class: III RISK FACTORS AND COMORBIDITIES previous CABG x4 in 2005, PAD Chronic Lung Disease/ COPD: Mild FEV1: 1900cc %predicted: 65 Other: No frailty PREVIOUS CARDIAC INTERVENTIONS PCI x2 last in 2/2013, recent cath showed patent all 3 grafts and patent PCI sites Creatinine (mg) /dl) 1.9 Creatinine clearance (cc/min) 30 BNP (pg/ml) 117 LVEF: 55% Aortic Calcification: Severe

40 Echo Images: Annulus Measurement

41 CT Images: Annulus Measurements
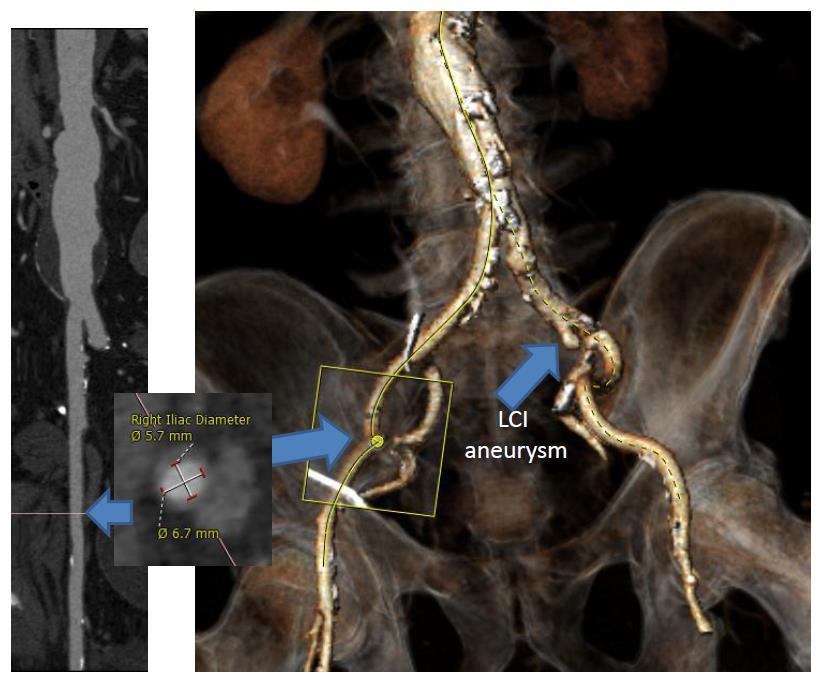
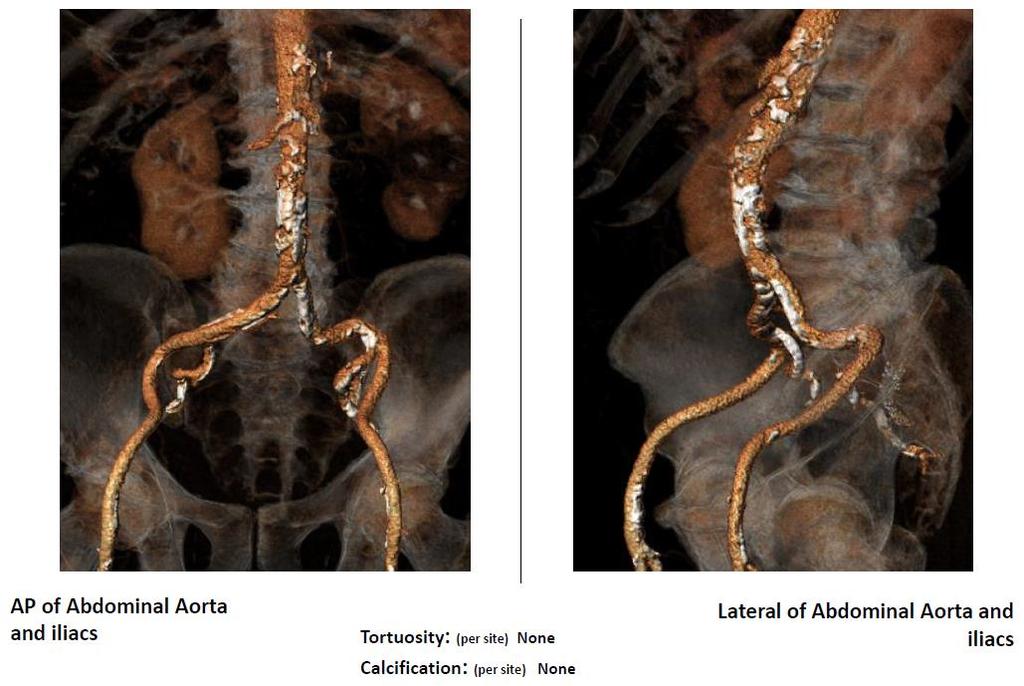
42 Iliofemorals
43 Patient History Age (years): 71 Gender: M Height (ins): 66 Weight (Ibs): 170 Risk Summary: STS Score: 4.5% mortality 8.2% morbidity/mortality The patient has the following: NYHA Class: III RISK FACTORS AND COMORBIDITIES previous CABG x4 in 2005, PAD Chronic Lung Disease/ COPD: Mild FEV1: 1900cc %predicted: 55 Other: No frailty PREVIOUS CARDIAC INTERVENTIONS PCI x2 last in 2/2013, recent cath showed patent all 3 grafts and patent PCI sites Creatinine (mg) /dl) 1.9 Creatinine clearance (cc/min) 30 BNP (pg/ml) 117 LVEF: 55% Aortic Calcification: Severe
44 Treatment of Choice in this 71 Yr old AS pt?bav?savr?tavr Pt was Randomized in the ongoing Intermediate risk TAVR trial (SURTAVI) because - 4.5% STS risk score makes him ideal for evaluation of TAVR vs. SAVR in these intermediate risk AS pts Pt was randomized to SAVR and underwent 21mm Pericardial valve without complications.
45 Patient History Age (years): 78 Gender: M Height (ins): 68 Weight (Ibs): 162 The patient has the following in 8/2013: NYHA Class: IV and CCS class III angina on presentation to OSH with TnI 1.2U and transferred for treatment RISK FACTORS AND COMORBIDITIES previous CABG x4 in 1999 Chronic Lung Disease/ COPD: None FEV1: 2250cc %predicted: 95 Other: No frality PREVIOUS CARDIAC INTERVENTIONS Recent cath showed patent all 4 grafts with 80% stenosis of SVG to OM, LVEF 55% Creatinine (mg) /dl) 0.9 Creatinine clearance (cc/min) 70 BNP (pg/ml) 57 LVEF: 55% Aortic Calcification: Severe
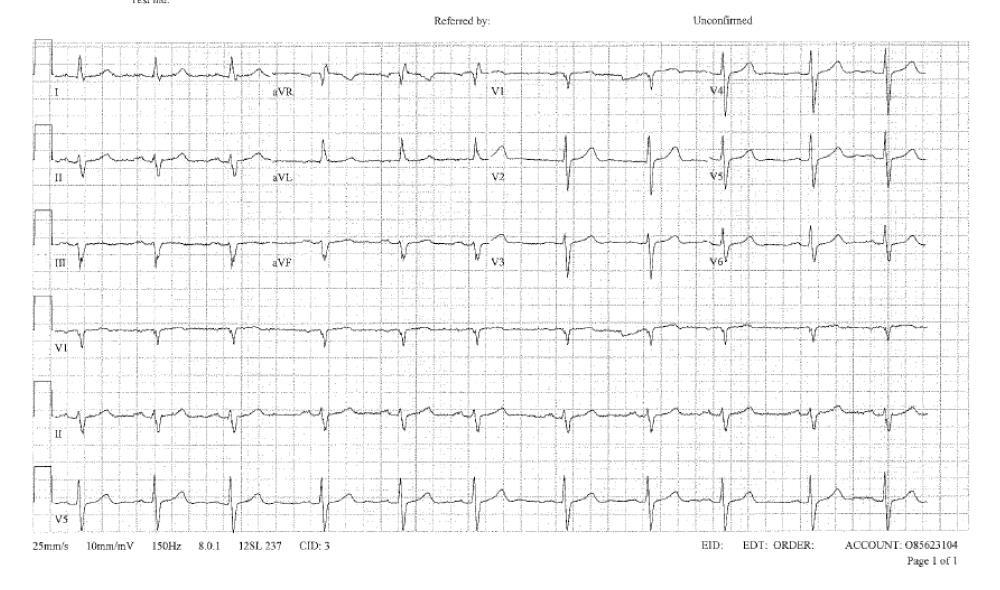
46 ECG
 ---_ Aortic valve area index (cm 2 /m 2 ) 42.0_ Mean gradient (mmhg) _4.")
47 Echo Images: Annulus Measurement Site Images of AV annulus _23_ Aortic annular size (mm) _0.6_ Aortic valve area (cm 2 ) ---_ Aortic valve area index (cm 2 /m 2 ) 42.0_ Mean gradient (mmhg) _4.2_ Peak velocity (m/sec) 60_ LVEF (%)

 31.4 28.")
48 CT Images: Annulus Measurements Clinical Analyst s Image Ao Annulus mean diameter 26.1 mm 30.3 X 21.8_ Major x Minor aortic annulus diameter 82.9_ Aortic Annulus perimeter (26.4 x 3.14) 33.5 Max Ascending Aorta diameter Sinus of Valsalva width Sinus of Valsalva height (all in mm) Sinotubular Junction width (STJ)
49 Hemodynamics: Baseline
50
51
52
53
54
55 Patient History Age (years): 78 Gender: M Height (ins): 68 Weight (Ibs): 162 Risk Summary: STS Score: 2.8% mortality 4.2% morbidity/mortality The patient has the following in 8/2013: NYHA Class: IV and CCS class III angina on presentation to OSH and transferred for treatment RISK FACTORS AND COMORBIDITIES previous CABG x4 in 1999 Chronic Lung Disease/ COPD: None FEV1: 2250cc %predicted: 95 Other: No frality PREVIOUS CARDIAC INTERVENTIONS Recent cath showed patent all 4 grafts with 80% stenosis of SVG to OM Creatinine (mg) /dl) 0.9 Creatinine clearance (cc/min) 70 BNP (pg/ml) 57 LVEF: 55% Aortic Calcification: Severe
56 Treatment of Choice in this 78 Yr old AS pt Presenting with CHF and NSTEMI/UA?BAV+ PCI to SVG to OM?SAVR+ CABG to OM?TAVR+ PCI to SVG to OM Pt was in CHF class IV and NSTEMI/unstable angina. Had Heart Team discussion with CT surgeon and recommended percutaneous approach to stabilize the pt s condition.
57
58
59
60
61 Treatment of Choice in this 78 Yr old AS pt Presenting with CHF and NSTEMI/UA?BAV+ PCI to SVG to OM?SAVR+ CABG to OM?TAVR+ PCI to SVG to OM Pt was in CHF class IV and NSTEMI/unstable angina. Had Heart Team discussion with CT surgeon and recommended percutaneous approach to stabilize the pt s condition. Pt then underwent BAV and BMS PCI to SVG to OM. Did well and discharged home next day.
62 Treatment of Choice in this 78 Yr old AS pt 5 mths later for CHF Class III symptom recurrence Risk Summary: STS Score: 1.8% mortality 3.2% morbidity/mortality?re-bav?savr?tavr Pt had low STS risk (<4) score and hence underwent conventional SAVR using 23mm Pericardial valve without any complications. No CABG needed as BMS to SVG to OM was patent.
63 Algorithm for Management of Severe AS: SAVR vs TAVR Severe AS AS Symptoms No Yes LVEF <50% No Physically active No Yes Exercise Test Symptoms ressure below or fall baseline blood pressure below baseline No Presence of risk factors and Presence of risk factors and low/intermediate individual surgical low/intermediate individual surgical risk risk No Yes Re-evaluate in 6 months Yes Yes SAVR No High risk for AVR Contraindication for AVR Yes Short life expectancy Serious Comorbidity STS >50% No Yes No Yes TAVR or SAVR TAVR Med Rx? BAV

64 Emerging TAVR Devices Involving Improved Technologies, Potentially Minimizing PVL/AR after TAVR
65 TAVR in Evolution (2014+) Future Clinical Indications Valve-in-valve for bio-prosthetic aortic valve failure Intermediate (moderate) risk AS patients Asymptomatic severe AS Low flow-low gradient AS impedance mismatch Aortic insufficiency; difficult with current generation which is dependent on calcified native AV to anchor the prosthesis
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative
 Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Severe Aortic Valve Disease: TAVR in Four Ages and Four Etiologies Age 25 y/o Congenital, 50 y/o Bicuspid, 75 y/o Rheumatic, 100 y/o Degenerative Samin K. Sharma, MD, FACC, FSCAI Director Clinical & Interventional
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute
 Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
Neal Kleiman, MD Houston Methodist DeBakey Heart and Vascular Institute Despite a 33 fold growth in the first five years, there is still tremendous variability among penetration in different countries
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Aortic Stenosis: Open vs TAVR vs Nothing
 Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
The Role of TAVI in high-risk and normal-risk Patients
 The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update
 Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Aortic Stenosis Background and Breakthroughs in Treatment: TAVR Update Howard J Broder MD Interventional Cardiology DaVita Medical Group/ Healthcare Partners Cardiology Disclosures for Howard J Broder
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients:
 Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Trans Catheter Aortic Valve Replacement
 Trans Catheter Aortic Valve Replacement Satish K Surabhi, MD,FACC,FSCAI Medical Director, Cardiac Cath Labs AnMed Health Heart and Vascular Care No financial conflict of interest related to this talk Will
Trans Catheter Aortic Valve Replacement Satish K Surabhi, MD,FACC,FSCAI Medical Director, Cardiac Cath Labs AnMed Health Heart and Vascular Care No financial conflict of interest related to this talk Will
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI
 Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Debate: SAVR for Low-Risk Patients in 2017 is Obsolete AVR vs TAVI Joseph E. Bavaria, MD Roberts-Measey Professor of Surgery Vice Chair, Division of Cardiovascular Surgery University of Pennsylvania Immediate
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR)
") Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Structural Heart Disease Transcatheter Aortic Valve Replacement (TAVR) Kathleen Harper DO FACC FACP 87 Chief, Cardiology Section VA Maine Healthcare Kathleen.Harper@va.gov Prevalence of Aortic Stenosis
Disclosures 4/16/2018. What s New in Valvularand Structural Heart Disease. None relevant to the presentation
 What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
What s New in Valvularand Structural Heart Disease Ryan C. Shelstad, MD Surgical Enthusiast, Valvular and Structural Heart Disease Bryan Heart Cardiothoracic Surgery Disclosures None relevant to the presentation
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON
 THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
THE PERCUTANEOUS MANAGEMENT OF VALVULAR HEART DISEASE DR JOHN RAWLINS CONSULTANT INTERVENTIONAL CARDIOLOGIST UNIVERSITY HOSPITAL SOUTHAMPTON INTRODUCTION History of heart valve intervention Current indications
TAVI After PARTNER-2 : The Hamilton Approach
 TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
TAVI After PARTNER-2 : The Hamilton Approach James L. Velianou MD FRCPC Interventional Cardiology Hamilton General Hospital St Catharines General Hospital Associate Professor of Medicine McMaster University
LOW RISK TAVR. WHAT THE FUTURE HOLDS
 LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
LOW RISK TAVR. WHAT THE FUTURE HOLDS Michael J. Reardon, M.D. Professor of Cardiothoracic Surgery Allison Family Distinguish Chair of Cardiovascular Research Houston Methodist DeBakey Heart & Vascular
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia
 Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
TAVR: Review of the Robust Data from Randomized Trials
 TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
TAVR: Review of the Robust Data from Randomized Trials Nicholas J. Ruggiero II, MD,FACP, FACC, FSCAI, FSVM, FCPP Director, Structural Heart Disease and Non-Coronary Interventions Director, Jefferson Heart
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Evolving and Expanding Indications for TAVR
 Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Evolving and Expanding Indications for TAVR Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients
 Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Is TAVR Now Indicated in Even Low Risk Aortic Valve Disease Patients Saibal Kar, MD, FACC, FAHA, FSCAI Director of Interventional Cardiac Research Cedars Sinai Heart Institute, Los Angeles, CA Potential
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
TAVR in 2020: What is Next!!!!
 TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
TAVR in 2020: What is Next!!!! Vinod H. Thourani, MD Professor of Surgery Chairman, Department of Cardiac Surgery Medstar Heart and Vascular Institute Washington Hospital Center Washington, DC Disclosures
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Strokes After TAVR Reasons for Declining Frequency
 Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Strokes After TAVR Reasons for Declining Frequency Samir Kapadia, MD Professor of Medicine Director, Cardiac Catheterization Laboratory Cleveland Clinic Disclosure NONE Second Generation Valves Newer
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee
 - 5 important lessons learnt from HK experiences Michael KY Lee") Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the FORWARD Study
 30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
30-Day Outcomes Following Implantation of a Repositionable Self-Expanding Aortic Bioprosthesis: First Report From the Study Stephan Windecker Department of Cardiology Bern University Hospital - INSELSPITAL
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Ian T. Meredith AM. MBBS, PhD, FRACP, FCSANZ, FACC, FAPSIC. Monash HEART, Monash Health & Monash University Melbourne, Australia
 Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland
 Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Andrzej Ochala, MD Medical University of Silesia, Katowice, Poland Bicuspid aortic valve o Most common congenital heart disease in adults (1% - 2%) o AS is the most common complication of BAV o Patophysiology
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Disclosures. LGH TAVR: Presentation Outline 2/2/2016. Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience
 and the LGH Experience") Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Updates in Transcatheter Aortic Valve Replacement (TAVR) and the LGH Experience The LGH TAVR Program James E. Harvey, MD, MSc Medical Director, Structural Heart Intervention The Heart Group of Lancaster
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients
 O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
O P E N A C C E S S Department of Cardiology, Aswan Heart Centre *Email: ahmed.elguindy@aswanheartcentre.com Lessons from the trials PARTNER 2A & SAPIEN 3: TAVI for intermediate risk patients Ahmed ElGuindy*
The Future of Medicine. Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy
 The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
The Future of Medicine Who to TAVR? Azeem Latib MD EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy FIRST PATIENT TO UNDERGO PTCA FIRST PATIENT TO UNDERGO TAVI Grüntzig
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE
 CVI SYMPOSIUM 2012 VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE Luis F. Tami, MD Cardiac Cath Lab Director Memorial Regional Hospital 86 yr old CABG 1995. LIMA to LAD and SVG to OM. Presented
CVI SYMPOSIUM 2012 VALVULAR HEART DISEASE AORTIC VALVE STENOSIS TAVR PROCEDURE Luis F. Tami, MD Cardiac Cath Lab Director Memorial Regional Hospital 86 yr old CABG 1995. LIMA to LAD and SVG to OM. Presented
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
TAVI limitations for low risk patients
 TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TAVI limitations for low risk patients Dr. T. Modine / P. Lancellotti MD, PhD, MBA CHRU de Lille, France Potential conflicts of interest Speaker's name: Thomas Modine I have the following potential conflicts
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization
 Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
L evoluzione nel management della valvulopatia aortica
 L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
L evoluzione nel management della valvulopatia aortica Giuseppe Tarantini, MD, PhD, FESC Director of Interventional Cardiology University of Padua GISE president TAVI: BIG BANG 2002 TAVI - EVOLUTIONs Commitment
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis
 Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
Percutaneous aortic valve replacement should NOT be preferred therapy for aortic stenosis James Bartholomew McClurken, MD FACC, FCCP, FACS, FESC Professor & Vice-Chair of Surgery, Temple University Hosp.,
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
State of the Art and Future perspective
 State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
State of the Art and Future perspective Giuseppe Tarantini, MD, PhD, FESC Associate professor University of Padua Director Interventional Cardiology Dpt of Cardiac Thoracic and Vascular Sciences, Padua
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Tissue vs Mechanical What s the Data??
 Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Biological (Tissue) Valve in a 60 year old patient: Debate Tissue vs Mechanical What s the Data?? Joseph E. Bavaria, MD Immediate-Past President - Society of Thoracic Surgeons (STS) Brooke Roberts-William
Neuroprotection During TAVR
 Neuroprotection During TAVR Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac Catheterization Laboratories Cleveland Clinic Cleveland Clinic Disclosure Co
Neuroprotection During TAVR Samir Kapadia, MD Professor of Medicine Section head, Interventional Cardiology Director, Cardiac Catheterization Laboratories Cleveland Clinic Cleveland Clinic Disclosure Co
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK
 Overview for Wales. Dr Richard Anderson University Hospital of Wales, Cardiff, UK") Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
Transcatheter Aortic Valve Implantation (TAVI) Overview for Wales Dr Richard Anderson University Hospital of Wales, Cardiff, UK Aortic stenosis is a disease of old age Age demographics in Wales % Wales
TAVR: What Have Cardiologists Have Learned from the Cardiac Surgeons?
 TAVR: What Have Cardiologists Have Learned from the Cardiac Surgeons? Jeffrey J. Popma, MD Professor of Medicine Harvard Medical School Director, Interventional Cardiology Clinical Services Beth Israel
TAVR: What Have Cardiologists Have Learned from the Cardiac Surgeons? Jeffrey J. Popma, MD Professor of Medicine Harvard Medical School Director, Interventional Cardiology Clinical Services Beth Israel
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
3 years after introduction of TAVI in QEH. Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong
 3 years after introduction of TAVI in QEH Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong HA Convention 2014 Introduction Aortic Stenosis most common valvular heart disease
3 years after introduction of TAVI in QEH Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong HA Convention 2014 Introduction Aortic Stenosis most common valvular heart disease
TAVR in 2017 What we know? What to expect?
 Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Journal of Geriatric Cardiology (2018) 15: 55 60 2018 JGC All rights reserved; www.jgc301.com Perspective Open Access TAVR in 2017 What we know? What to expect? Panagiota Kourkoveli 1,*, Konstantinos Spargias
Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel
 TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?
TAVI CON Extension to medium and low risk patients? Friedrich Eckstein University Hospital Basel Extension to medium and low risk patients? In octogenerians already reality in most of the swiss clinics!?