Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
|
|
|
- Martina Cox
- 6 years ago
- Views:
Transcription




1 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth University Division of Cardiology Department of Internal Medicine Richmond, VA, USA
2 Conflict of interests NO POTENTIAL CONFLICTS OF INTERESTS TO BE DISCLOSED
3 Definition Late comers : The current reperfusion paradigm in STEMI is that prompt reperfusion should be attempted within 12 hours of symptoms onset* hence late comers are patients presenting >12 hours after symptom onset * Exceptions include stuttering chest pain, or shock.
4 Who are the Late Comers? Timing h vs >72 h Hemodynamics stable vs unstable Symptoms Reperfusion angina/heart failure/none complete/incomplete/none IRA obstruction 100% vs 70-99%






5 Mortality Who are the Late Comers? A heterogenous group No reperfusion /Occluded IRA Shock -Arrhythmia Heart failure Stenotic IRA Angina Depressed LVEF Patent IRA Asymptomatic Preserved LVEF High risk Low risk
6 High risk STEMI Cardiogenic shock Case #1: 45 yo F presenting with hypotension, requiring vasopressor/inotropes, chest discomfort ongoing for hours, ECG shows ST elevation V1-V4 Question: Should this patient be offered emergent angiogram and PCI/CABG?
7 High risk STEMI Cardiogenic shock The SHOCK trial (Hochman et al. NEJM 1999) included patients with STEMI and shock within 54 hours of presentation (median 11.5 hours) Hochman et al. NEJM 1999 Reynold and Hochman. Circulation 2008
8 High risk STEMI Cardiogenic shock Case #1: 45 yo F presenting with hypotension, requiring vasopressor/inotropes, chest discomfort ongoing for hours, ECG shows ST elevation V1-V4 Question: Should this patient be offered emergent angiogram and PCI/CABG? Definitely yes
9 The not so late late-comers 12 to 72 hours Case #2: 65 yo M presenting with chest pain ongoing for 16 hours, ST elevation V1-V4 Options: Fibrinolysis?
10 Fibrinolysis 12 to 24 hours Fibrinolysis? not a viable option Data from >2 RCT and a meta-analysis (FTT collaborative review Lancet 1994) suggest that the benefit of fibrinolysis for pts presenting between hours is minimal (35-day mortality 10.0% vs 10.5%, p=ns)
11 The not so late late-comers 12 to 72 hours Case #2: 65 yo M presenting with chest pain ongoing for 16 hours, ST elevation V1-V4 Options: Fibrinolysis? NO Mechanical reperfusion?
12 Mechanical reperfusion 12 to 72 hours PCI? conflicting results The BRAVE-2 study (Schoemig et al. JAMA 2005) pts (57% TIMI 0/1 flow, 23% TIMI 2 flow) h (median 23 hours) - invasive (PCI 95%) vs conservative strategy 6.8% mean reduction in infarct size 45% RRR for 4-year mortality (11 vs 20%) (Ndrepepa et al. JAMA 2009)
13 Mechanical reperfusion 12 to 72 hours PCI? conflicting results A substudy of the OAT study (Menon et al. EHJ 2009) pts (approx 15% of all OAT pts) h (median 66 hours) - PCI of occluded IRA vs conservative strategy (approx 20% had failed thrombolysis) No difference in the Kaplan-Meyer 4-year mortality (8 vs 8%)
14 Mechanical reperfusion 12 to 72 hours BRAVE-2 23 hours (12-48 hours) OAT substudy 66 hours (24-72 hours) 10% 11% vs 20%, p= year mortality 8% vs 8%, p= % TIMI 0/1 flow 99%
15 Mechanical reperfusion 12 to 72 hours Which is the time frame for infarct salvage? Busk et al (Eur Heart J 2009) looked at 247 pts with total occlusion undergoing PCI within 72 hours
16 The not so late late-comers 12 to 72 hours Case #2: 65 yo M presenting with chest pain ongoing for 16 hours, ST elevation V1-V4 Options: Fibrinolysis? NO Mechanical reperfusion? Possibly Within 24 hours Yes hours Yes/No
17 The very late late-comers >72 hours Case #3: 55 yo M on day 7 after non-reperfused anterior STEMI, asymptomatic (at rest) Question: Should he be offered a coronary angiogram and late revascularization?
18 mortality (%) The very late late-comers >72 hours GUSTO I angiographic substudy Modified from Puma et al. Am J Cardiol P<0.001 Occluded IRA Open IRA 8 P< P<0.001 * * Independent of infarct size and ejection fraction 1 year days 1-30 days
19 The very late late-comers >72 hours TOSCA-2 trial - OAT substudy (Dzavik et al. Circulation 2006) - paired angiograms at baseline and 12 months Irrespective of randomization arm, -54% had a patent IRA and 46% did not patients with a patent IRA at follow-up had a greater increase in LVEF than those with an occluded artery (absolute difference of 3.0%; p=0.003). supporting Braunwald s Open Artery Hypothesis
20 The very late late-comers >72 hours ALKK study (Zeymer et al. Circulation 2003) patients days after STEMI (median 23 days) - 1-vessel CAD (30% had total occlusion) 34% RRR in the composite endpoint (p=0.020) SWISSI II study (Erne et al. JAMA 2007) patients days after STEMI (median 32 days) - all with silent ischemia (30% had total occlusion) 80% RRR in mortality at 10 years (p<0.001)
21 The very late late-comers >72 hours DECOPI study (Steg et al. Eur Heart J 2004) patients - >48 hours after STEMI (median 5 days) - all with total (100%) IRA occlusion No differences in outcome (but > LVEF increase with PCI) OAT study (Hochman et al. N Engl J Med 2006) - 2,166 patients days after STEMI (median 8 days) - all with total (100%) IRA occlusion (88% collaterals) No differences in outcome (but angina with PCI and a trend in more favorable remodeling [TOSCA-2 substudy])
22 The very late late-comers >72 hours Case #3: 55 yo M on day 7 after non-reperfused anterior STEMI, asymptomatic (at rest). Question: Should he be offered a coronary angiogram and late revascularization? CONFLICTING DATA FROM RCT
23 The very late late-comers >72 hours Better late than never? Modified from Abbate et al. J Am Coll Cardiol 2008 A meta-analysis of 10 studies 3,560 patients late PCI of the infarct-related artery >12h of AMI median 12 days (range 1-26 days) after AMI 10 studies over more than 15 years variable inclusion and exclusion criteria variable interventional and non-interventional tx
24 The very late late-comers >72 hours Death Study Better late than never? Modified from Abbate et al. J Am Coll Cardiol 2008 OR (random) 95% CI ALKK BRAVE-2 DECOPI Horie et al OAT Silva et al SWISSI II TOAT TOMIIS TOPS Total (95% CI) P= % vs 8.4% 3 studies showed a mortality benefit 0.51 [0.29, 0.91] Favours PCI Favours medical Rx Median F/U 2.8 years
25 The very late late-comers >72 hours Better late than never? Modified from Abbate et al. J Am Coll Cardiol 2008 Late PCI lead also to: -A greater increase in LVEF (+4.4%, p=0.009) -A smaller increase in EDVi (-7.0 ml/m2, p=0.008) -A smaller increase in ESVi (-7.5 ml/m2, p=0.004) Even if analyzing the study with 100% IRA occlusion alone (Appleton et al. Cath Cardiovasc Int 2008): LVEF (+3.0%, p<0.001), EDVi (-5.1 ml/m2, p=0.02), ESVi (-5.2 ml/m2, p<0.001)
26 The very late late-comers >72 hours Better late than never? Modified from Abbate et al. J Am Coll Cardiol 2008 A meta-regression analysis showed: - Greater length of follow up predicted survival benefit and change in LVEF with PCI -Studies enrolling also IRA 70-99% obstruction (representing 4 of the 10 studies, 16% of patients) more likely to be positive -Studies that did not exclude patient with > moderate ischemia were also more likely to be positive
27 The very late late-comers >72 hours Case #3: 55 yo M on day 7 after non-reperfused anterior STEMI, asymptomatic (at rest). Question: Should he be offered a coronary angiogram and late revascularization? If the IRA 70-99% stenosed Yes If angina/ischemia present Yes If no angina/ira 100% Yes/No
28 What do the ACC/AHA guidelines recommend? Beyond 24 hours NO REPERFUSION + Cardiogenic shock (class IIa) Decomp CHF (class IIa) Ventr arrhythmias (class IIa) selected patients NO REPERFUSION + Without HIGH RISK FEATURES Late PCI >24h after AMI is not indicated Class III for totally occluded artery Class IIb for 70-99% stenosis Angiography Focused update: Antman et al. J Am Coll Cardiol 2008 Conservative Management
29 What do the ESC guidelines recommend? Beyond 12 hours hours Persistent pain (class IIa) Asymptomatic (class IIb) selected patients >24 hours Stable patient Late PCI >24h after AMI is not indicated Class III for totally occluded artery No mention of IRA 70-99% stenosis Angiography Van der Werf et al. Eur Heart J 2008 Conservative Management
30 Conclusions 1) STEMI late comers represents a heterogeneous group of patients 2) The benefits of late reperfusion are largely variable 3) A patient-tailored approach is preferable weighing risk/benefits, patients preference, and physician judgment 4) To date <4,000 pts have been studied calling for more RCT to address these questions
31 My approach * Late comer Hemodynamically unstable 12-48h Hemodynamically stable >48h 12-72h >72h Selected Patients Coronary angiogram Revascularization 12-24h 24-48h IRA 70-99% stenosis Selected Patients Selected Patients Angina / ischemia Coronary angiogram IRA 100% stenosis Asymptomatic Selected Patients Conservative Management * This proposed approach may be in disagreement with current AHA/ACC or ESC guidelines
32 For further slides on these topics please feel free to visit the metcardio.org website:
33 THE END
34 Who are the Late Comers? hours >72 hours Total IRA occlusion No Reperfusion Reperfusion Partial Reperfusion Critical IRA Stenosis (>70%)
35 The very late late-comers >72 hours What about the risk of recurrent AMI Modified from Abbate et al. J Am Coll Cardiol 2008 Review: Late percutaneous coronary intervention for infarct-related artery occlusion Comparison: Late percutaneous coronary intervention vs best medical therapy for infarct-related artery occlusion Outcome: Non-fatal Myocardial infarction Study PCI Medical Rx OR (random) OR (random) or sub-category n/n n/n 95% CI 95% CI ALKK 3/149 7/ [0.11, 1.67] BRAVE-2 5/182 4/ [0.33, 4.78] DECOPI 3/109 2/ [0.23, 8.73] Horie et al 3/44 7/ [0.08, 1.40] OAT 59/ / [0.91, 2.03] Silva et al 0/18 0/18 Not estimable SWISSI II 11/96 40/ [0.10, 0.44] TOAT 3/32 1/ [0.34, 34.65] TOMIIS 0/25 0/19 Not estimable TOPS 5/42 0/ [0.71, ] Total (95% CI) [0.38, 1.95] Total events: 92 (PCI), 105 (Medical Rx) Test for heterogeneity: Chi² = 26.96, df = 7 (P = ), I² = 74.0% Test for overall effect: Z = 0.36 (P = 0.72) Favours PCI Favours medical Rx
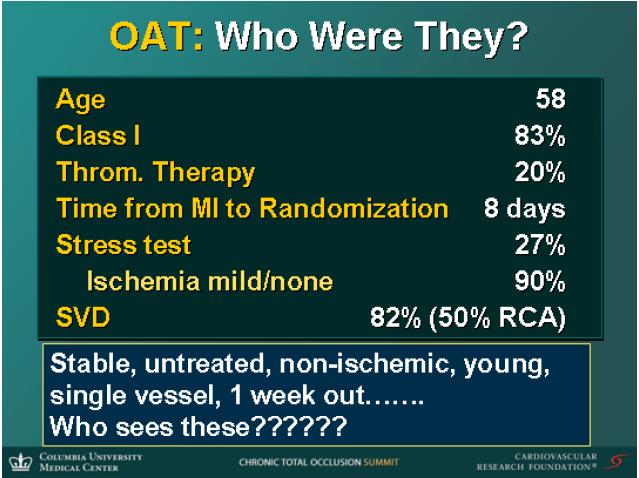
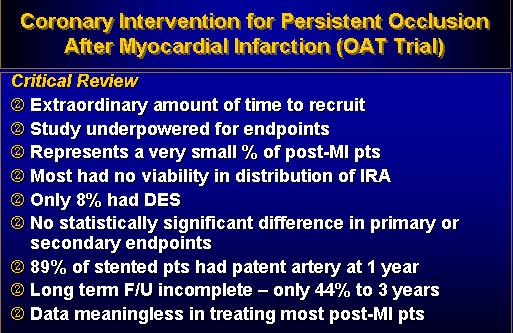
36 The OAT in perspective
37
38
39 Mechanical reperfusion 12 to 72 hours PCI? clinical benefit? BRAVE-2 study 90-day mortality 4-year mortality 4% vs 6%, p= % vs 20%, p=0.04 Schoemig et al. JAMA 2005 Ndrepepa et al. JAMA 2009 Median time to randomization 23 hours (absolute range hours)
40 Mechanical reperfusion 12 to 72 hours PCI? clinical benefit? OAT substudy year Kaplan-Meyer survival curve 8% vs 8%, p=0.88 Mean time 66 hours (range 24-72) Menon et al. Eur Heart J 2009
41 Mechanical reperfusion 12 to 72 hours Is there a Role for an Early Viability Study? The VIAMI study (abstract presentation Gruberg ) pts (approx 50% post-lytics) - Low-dose dobutamine h after MI viability randomized to PCI or cons tx no viability registry In viable pts, PCI lead to a reduction in events (D/MI/UA) (16% vs 7%, p=0.04) The non-viable pts had lowest rate (5%)
42 4-year 4-year 4-year 4-year Variable risk / variable benefit ALKK 10% 10% SWISSI 2 DECOPI 10% OAT 10%
43 The very late late-comers >72 hours The ALKK study (Zeymer et al. Circulation 2003) randomized patients with 1-vessel CAD, 8-42 days after STEMI, to PCI vs conserv ther >4-year F/U Event rates 38% vs 25%, p=0.02 favoring PCI Of note: >70% pts had IRA stenosis <100%, Pts with 100% IRA occlusion had less benefit
44 The very late late-comers >72 hours The SWISSI-2 study (Erne et al. JAMA 2007) randomized patients with 3-58 days after STEMI to PCI vs conservative therapy Death rate 3% vs 21%, p=0.01 favoring PCI >10-year F/U Of note: >70% pts had IRA stenosis <100%, All pts had inducible silent ischemia
45 The very late late-comers >72 hours A substudy of the SWISSI-2 study (Schoenenberger et al. Am J Cardiol 2009) looked at sudden death in PCI vs conservative therapy Sudden Death 1% vs 11%, p=0.002 favoring PCI >10-year F/U Of note: >70% pts had IRA stenosis <100%, All pts had silent ischemia The risk of sudden death was related to LVEF decline
46 The very late late-comers >72 hours The DECOPI study (Steg et al. Eur Heart J 2004) randomized patients with >48 hours after STEMI to PCI vs conservative therapy No differences in outcome >4-year F/U Of note: All pts had 100% IRA stenosis PCI was associated with greater LVEF increase
47 The very late late-comers >72 hours The OAT study (Hochman et al. N Engl J Med 2006) is the largest (>2,000 pts) randomized trial of late PCI vs conservative therapy No differences in outcome Of note: All pts had 100% IRA stenosis Median follow up <3 yrs
48 The very late late-comers >72 hours The OAT study (Hochman et al. N Engl J Med 2006) is the largest (>2,000 pts) randomized trial of late PCI vs conservative therapy Fewer patients had angina w/ PCI up to 24 months
49 The very late late-comers >72 hours The TOSCA-2 trial is a substudy of the OAT (Dzavik et al. Circulation 2006) in which patients had paired angiograms at baseline and 12 months. Patients in the PCI group tended to have a more favorable remodeling 17% of PCI group had late IRA occlusion 25% of MED had late IRA patency
50 The very late late-comers >72 hours Better late than never? Modified from Abbate et al. J Am Coll Cardiol 2008 Study PCI Medical Rx OR (random) OR (random) or sub-category n/n n/n 95% CI 95% CI ALKK 6/149 17/ [0.13, 0.86] BRAVE-2 4/18 8/ [0.15, 1.66] DECOPI 8/109 9/ [0.31, 2.23] Horie et al 1/44 5/ [0.02, 1.42] OAT 87/ / [0.76, 1.42] Silva et al 0/1 2/ [0.01, 3.99] SWISSI II 3/ 22/ [0.04, 0.42] TOAT 2/32 1/ [0.19, 25.52] TOMIIS 1/2 1/ [0.04, 12.82] TOPS 0/42 0/45 Not estimable Total (95% CI) Total events: 112 (PCI), 149 (Medical Rx) Test for heterogeneity: Chi² = 19.36, df = 8 (P = 0.01), I² = 58.7% Test for overall effect: Z = 2.15 (P = 0.03) Outcome: Death Favours PCI Favours medical Rx 0.49 [0.26, 0.94]
51 Study or sub-category Late presentation / No reperfusion Better late than 95% CI never? Or is it better? Modified by Abbate et al. J Am Coll Cardiol 2008 Meta-analysis of 3,560 patients from OAT 10 different RCTs PCI n/n OR (random) Medical Rx n/n OR (random) 95% CI OR (random) 95% CI ALKK 6/149 17/ [0.13, 0.86] BRAVE-2 4/18 8/ [0.15, 1.66] DECOPI 8/109 9/ [0.31, 2.23] Horie et al 1/44 O5/ [0.02, 1.42] OAT 87/ / [0.76, 1.42] Silva et al 0/1 2/ [0.01, 3.99] SWISSI II 3/ 22/ [0.04, 0.42] TOAT 2/32 1/ [0.19, 25.52] TOMIIS 1/2 1/ [0.04, 12.82] TOPS 0/42 0/45 Not estimable [0.26, 0.94] Total (95% CI) [0.26, 0.94] Total events: 112 (PCI), 149 (Medical Outcome: Rx) Death (NNT 48) Test for heterogeneity: Chi² = 19.36, df = 8 (P = 0.01), I² = 58.7% Outcome: Death Test for overall effect: Z = 2.15 (P = 0.03) Favours PCI Favours medical Rx Favours PCI Favours medical Rx
52 Why such a difference in outcome? OR (random) Longer follow up greater 95% CI benefit Review: Late percutaneous coronary intervention for infarct-related artery occlusion Comparison: Late percutaneous coronary intervention vs best medical therapy for infarct-related artery occlusion Outcome: Death Study PCI Medical PCI Rx OR Medical (random) Rx OR (random) or sub-category n/n n/n n/n 95% n/n CI 95% CI ALKK 6/149 17/151 6/149 17/ [0.13, 0.86] BRAVE-2 4/18 8/183 4/18 8/ [0.15, 1.66] DECOPI 8/109 9/103 8/109 9/ [0.31, 2.23] Horie et al 1/44 5/39 1/44 O5/ [0.02, 1.42] OAT 87/1 84/ / / [0.76, 1.42] Silva et al 0/1 2/18 0/1 2/ [0.01, 3.99] SWISSI II 3/ 22/105 3/ 22/ [0.04, 0.42] TOAT 2/32 1/34 2/32 1/ [0.19, 25.52] TOMIIS 1/2 1/19 1/2 1/ [0.04, 12.82] TOPS 0/42 0/45 0/42 0/45 Not estimable [0.26, 0.94] Total (95% CI) [0.26, 0.94] Total events: 112 (PCI), 149 (Medical Rx) Outcome: Death (NNT 48) Test for heterogeneity: Chi² = 19.36, df = 8 (P = 0.01), I² = 58.7% Test for overall effect: Z = 2.15 (P = 0.03) Favours PCI Favours medical Rx Favours PCI Favours medical Rx Data from the recent BRAVE-2 publication not included OAT
53 Why such a difference in outcome? OR (random) Presence of ischemia 95% CI and/or suboccluded IRA greater benefit OAT Review: Late percutaneous coronary intervention for infarct-related artery occlusion Comparison: Late percutaneous coronary intervention vs best medical therapy for infarct-related artery occlusion Outcome: Death PCI Medical Rx Study PCI Medical n/nrx OR n/n(random) OR (random) or sub-category n/n n/n 95% CI 95% CI 6/149 17/151 ALKK 6/149 17/151 4/18 8/ [0.13, 0.86] BRAVE-2 4/18 8/183 8/109 9/ [0.15, 1.66] DECOPI 8/109 9/103 1/44 O5/ [0.31, 2.23] Horie et al 1/44 5/39 87/ / [0.02, 1.42] OAT 87/1 84/1084 0/1 2/ [0.76, 1.42] Silva et al 0/1 2/183/ 22/ [0.01, 3.99] SWISSI II 3/ 22/105 2/32 1/ [0.04, 0.42] TOAT 2/32 1/341/2 1/ [0.19, 25.52] TOMIIS 1/2 1/ /42 0/ [0.04, 12.82] TOPS 0/42 0/45 [0.26, 0.94] Not estimable Total (95% CI) 1779 Outcome: 1781 Death (NNT 48) 0.49 [0.26, 0.94] Total events: 112 (PCI), 149 (Medical Rx) Test for heterogeneity: Chi² = 19.36, df = 8 (P = 0.01), I² = 58.7% Test for overall effect: Z = 2.15 (P = 0.03) Favours PCI Favours medical Rx Favours PCI Favours medical Rx
54 Horie et al. Circulation 1998
55 Mechanical reperfusion 12 to 72 hours Is there a Role for an Early Viability Study? The VIAMI study (abstract presentation Gruberg ) pts (approx 50% post-lytics) h after MI - Low-dose dobutamine viability randomized to PCI or cons tx no viability registry In viable pts, PCI lead to a reduction in events (D/MI/UA) (16% vs 7%, p=0.04) The non-viable pts had lowest event rate
presenters 2010 Sameh Sabet Ain Shams University
 Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
Guidelines for PCI in late STEMI presenters 2010 Sameh Sabet Assistant Professor of Cardiology Ain Shams University 29% of MI patients have STEMI. NRMI 4 (Fourth National Registry of Myocardial Infarction),
Benefits of coronary revascularization in stable patients in the short and long term after acute myocardial infarction
 REVIEW Benefits of coronary revascularization in stable patients in the short and long term after acute myocardial infarction The benefit of coronary revascularization in stable patients with acute myocardial
REVIEW Benefits of coronary revascularization in stable patients in the short and long term after acute myocardial infarction The benefit of coronary revascularization in stable patients with acute myocardial
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Approach to Multi Vessel disease with STEMI
 Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
Approach to Multi Vessel disease with STEMI MANAGEMENT OF ST-ELEVATION MYOCARDIAL INFARCTION Dr. Thomas Alexander, M.D; D.M; F.A.C.C. Senior Consultant and Interventional Cardiologist Kovai Medical Centre
What do the guidelines say?
 Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Percutaneous coronary intervention in 3-vessel disease and main stem What do the guidelines say? Nothing to disclose Dariusz Dudek Institute of Cardiology, Jagiellonian University Krakow, Poland The European
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
Management of cardiovascular disease - coronary interventions -
 Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Master Classes in Preventive Cardiology I Management of diabetes in patients with CVD European Heart House Management of cardiovascular disease - coronary interventions - Francesco Cosentino MD, PhD, FESC
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Assist Devices in STEMI- Intra-aortic Balloon Pump
 Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Assist Devices in STEMI- Intra-aortic Balloon Pump Ioannis Iakovou, MD, PhD Onassis Cardiac Surgery Center Athens, Greece Cardiogenic shock 5-10% of pts after a heart attack 60000-70000 pts in Europe/year
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Clinical Considerations for CTO
 38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
A Future for the IABP in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany
 University of Lübeck, Germany") A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
A Future for the in Cardiogenic Shock? Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University of Lübeck, Germany Disclosures Funding: German Research Foundation German Heart Research
FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators
 FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Republic of
FFR-guided Complete vs. Culprit Only Revascularization in AMI Patients Ki Hong Choi, MD On Behalf of FRAME-AMI Investigators Heart Vascular Stroke Institute, Samsung Medical Center, Seoul, Republic of
CORONARY CHRONIC TOTAL OCCLUSIONS IN THE SETTING OF ACUTE MYOCARDIAL INFARCTION
 CORONARY CHRONIC TOTAL OCCLUSIONS IN THE SETTING OF ACUTE MYOCARDIAL INFARCTION *Bimmer Claessen, Loes Hoebers, José Henriques Department of Cardiology, Academic Medical Center, University of Amsterdam,
CORONARY CHRONIC TOTAL OCCLUSIONS IN THE SETTING OF ACUTE MYOCARDIAL INFARCTION *Bimmer Claessen, Loes Hoebers, José Henriques Department of Cardiology, Academic Medical Center, University of Amsterdam,
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend )
") Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Intraaortic Balloon Counterpulsation- Supportive Data for a Role in Cardiogenic Shock ( Be Still My Friend ) Stephen G. Ellis, MD Section Head, Interventional Cardiology Professor of Medicine Cleveland
Clinical Considerations for CTO Revascularization
 Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function?
 Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
Should All Patients Be Treated with Ace-inh /ARB after STEMI with Preserved LV Function? Avi Shimony, MD, FESC Cardiology Division Soroka University Medical Center Ben-Gurion University, Beer-Sheva Disclosure
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
DECLARATION OF CONFLICT OF INTEREST Multivessel disease and cardiogenic shock: CABG is the optimal revascularization therapy. Contra Prof. Christian JM Vrints Cardiogenic Shock Spiral Acute Myocardial
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor
 Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Medical Rx vs PCI vs CABG
 Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Medical Rx vs PCI vs CABG S. Hinan Ahmed, MD Associate Professor: Cardiology and Cardiothoracic Surgery Program Director: Interventional Fellowship Program Assoc Editor: Cath and Cardiovasc Intervention
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
PCIs on Intermediate Lesions NCDR Cath-PCI Registry
 Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Practical Application Of Coronary Physiology in The Cath Lab Talal T Attar, MD, MBA, FACC PCIs on Intermediate Lesions NCDR Cath-PCI Registry Fraction of stenoses 50-70% treated with PCI without further
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY
 ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
ACUTE CORONARY SYNDROME PCI IN THE ELDERLY G.KARABELA MD.PhD ATHENS NAVAL HOSPITAL INTERVENTIONAL CARDIOLOGY DEPARTMENT NO CONFLICT OF INTEREST TO DECLAIRE Risk stratification in Αcute Coronary Syndrome.
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Transfer in D2B. Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland. The Problem
 Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
Transfer in D2B Scott D Friedman, MD FACC Medical Director, Cardiology Services Shore Health System of Maryland The Problem NRMI-5: North Carolina, July 2003- June 2004 NC Nation Guidelines N 2,738 79,927
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017
 Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017 Holger Thiele Cardiogenic Shock STEMI Guidelines Steg et al. Eur Heart J.2012;33:2569-2619 Cardiogenic Shock CHF Guidelines
Why we need a consensus document on cardiogenic shock? ACCA Masterclass 2017 Holger Thiele Cardiogenic Shock STEMI Guidelines Steg et al. Eur Heart J.2012;33:2569-2619 Cardiogenic Shock CHF Guidelines
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Evaluating Clinical Risk and Guiding management with SPECT Imaging
 Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Evaluating Clinical Risk and Guiding management with SPECT Imaging Raffaele Giubbini Chair and Nuclear Medicine Unit University & Spedali Civili Brescia- Italy U.S. Congressional Budget Office. Technological
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Intervention: How and to which extent is technology helping us?
 Cardiological Society of India Congress 12th February 2016 Chennai, India Intervention: How and to which extent is technology helping us? SIMONE BISCAGLIA MD CARDIOVASCULAR INSTITUTE, FERRARA, ITALY Introduction
Cardiological Society of India Congress 12th February 2016 Chennai, India Intervention: How and to which extent is technology helping us? SIMONE BISCAGLIA MD CARDIOVASCULAR INSTITUTE, FERRARA, ITALY Introduction
Management of Cardiogenic shock. Prof. Christian JM Vrints
 Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
Management of Cardiogenic shock Prof. Christian JM Vrints none conflicts Management of Cardiogenic Shock Incidence and trends Importance of early revascularization Multivessel disease Left main disease
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Coronary Revascularization for Severe LV Dysfunction Is s. Is the concept of viability testing still viable?
 Coronary Revascularization for Severe LV Dysfunction Is s Is the concept of viability testing still viable? Banff 2017 2015 MFMER 3492638-7 Prognosis of Patients With LV Dysfunction and CAD Major determinants
Coronary Revascularization for Severe LV Dysfunction Is s Is the concept of viability testing still viable? Banff 2017 2015 MFMER 3492638-7 Prognosis of Patients With LV Dysfunction and CAD Major determinants
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
original article Department of Interventional Cardiology and Angiology, Institute of Cardiology, Warsaw, Poland
 original article Cardiology Journal 2013, Vol. 20, No. 5, pp. 552 559 DOI: 10.5603/CJ.2013.0141 Copyright 2013 Via Medica ISSN 1897 5593 Late percutaneous coronary intervention for an occluded infarct-related
original article Cardiology Journal 2013, Vol. 20, No. 5, pp. 552 559 DOI: 10.5603/CJ.2013.0141 Copyright 2013 Via Medica ISSN 1897 5593 Late percutaneous coronary intervention for an occluded infarct-related
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Thrombus Aspiration before PCI: Routine Mandatory. Professor Clinical Cardiology Academic Medical Center University of Amsterdam
 Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
The Case for Multivessel Revascularization in Shock
 The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
The Case for Multivessel Revascularization in Shock Emmanouil S. Brilakis, MD, PhD Minneapolis Heart Institute 9.37 9.49 am Disclosures Consulting/speaker honoraria: Abbott Vascular, American Heart Association
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Timing of angiography for high- risk ACS
 Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
Timing of angiography for high- risk ACS Christian Spaulding, MD, PhD, FESC, FACC Cardiology Department Cochin Hospital, Inserm U 970 Paris Descartes University Paris, France A very old story. The Interventional
COURAGE to Leave Diseased Arteries Alone
 COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
COURAGE to Leave Diseased Arteries Alone Spencer King MD MACC, FSCAI St. Joseph s s Heart and Vascular Institute Professor of Medicine Emeritus Emory Univ. Atlanta, USA Conflict: I am an Interventionalist
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Ventricular tachycardia and ischemia. Martin Jan Schalij Department of Cardiology Leiden University Medical Center
 Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Ventricular tachycardia and ischemia Martin Jan Schalij Department of Cardiology Leiden University Medical Center Disclosure: Research grants from: Boston Scientific Medtronic Biotronik Sudden Cardiac
Rationale for Prophylactic Support During Percutaneous Coronary Intervention
 Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Rationale for Prophylactic Support During Percutaneous Coronary Intervention Navin K. Kapur, MD, FACC, FSCAI Assistant Director, Interventional Cardiology Director, Interventional Research Laboratories
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why.
 Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
Implementing the pharmacoinvasive strategy in STEMI The Need for Rescue PCI after Failed Fibrinolysis: Who, When and Why. 7:20-7:40 Robert C. Welsh, MD, FRCPC, FESC, FAHA, FACC Professor of Medicine Director,
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
How to do Primary Angioplasty. - Patients with Cardiogenic Shock
 How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
How to do Primary Angioplasty - Patients with Cardiogenic Shock Advanced Cardiovascular Intervention 2011 Dan Blackman Leeds General Infirmary MY CONFLICTS OF INTEREST ARE: Research Grants Medicines Company
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Primary Percutaneous Coronary Intervention
 STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
Σεμινάριο Ομάδων Εργασίας Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική
 Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική") ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
ΕΛΛΗΝΙΚΗΚΑΡΔΙΟΛΟΓΙΚΗΕΤΑΙΡΕΙΑ Σεμινάριο Ομάδων Εργασίας 2011 Fractional Flow Reserve (FFR) Σε ποιούς ασθενείς; ΔΗΜΗΤΡΗΣ ΑΥΖΩΤΗΣ Επιστ. υπεύθυνος Αιμοδυναμικού Τμήματος, Βιοκλινική GUIDELINES ON MYOCARDIAL
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
New Insights on Reperfusion Choices Implications of STREAM. Paul W Armstrong MD
 New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
New Insights on Reperfusion Choices Implications of STREAM ESC STEMI Satellite Symposium August 31 2014 Aligning Optimal Care to Time Place and Person Paul W Armstrong MD Disclosure Statement Paul W. Armstrong
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia.
 STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
STEMI Stents What next? Arshad Khan - HNE Clinical Research Fellow. Supervisors: Prof Boyle and Attia. PART 1 Systems of care for STEMI. STEMI Management Coronary angiogram +/- stenting. Prehospital thrombolysis
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Treatment Options for Angina
 Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
Treatment Options for Angina Interventional Cardiology Perspective Michael A. Robertson, M.D. 10/30/10 Prevalence of CAD in USA 15 million Americans with CAD 2 million diagnostic catheterizations 1 million
12/18/2009 Resting and Maxi Resting and Max mal Coronary Blood Flow 2
 Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Cardiogenic Shock. Dr. JPS Henriques. Academic Medical Center University of Amsterdam The Netherlands
 Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Cardiogenic Shock Dr. JPS Henriques Academic Medical Center University of Amsterdam The Netherlands Conflict of interest disclosure Research grant Abbott Vascular Research grant Abiomed Inc. Global Impella
Stable Ischemic Heart Disease. Ivan Anderson, MD RIHVH Cardiology
 Stable Ischemic Heart Disease Ivan Anderson, MD RIHVH Cardiology Outline Review of the vascular biology of atherosclerosis Why not just cath everyone with angina? Medical management of ischemic cardiomyopathy
Stable Ischemic Heart Disease Ivan Anderson, MD RIHVH Cardiology Outline Review of the vascular biology of atherosclerosis Why not just cath everyone with angina? Medical management of ischemic cardiomyopathy
Primary Percutaneous Coronary Intervention
 The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
The big 5 in PCI Primary Percutaneous Coronary Intervention W. Wijns (Aalst, BE) Disclosures Consulting Fees: on my behalf go to the Cardiovascular Research Center Aalst Contracted Research between the
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Coronary Interventions Indications, Treatment Options and Outcomes
 Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies
 Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Severe Left Ventricular Dysfunction: Evolving Revascularization Strategies Robert O. Bonow, MD, MS, MACC Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability
 Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
Revascularization for Patients with HFrEF: CABG and PCI and the Concept of Myocardial Viability 22nd Annual Heart Failure 2018: an Update on Therapy April 2018 Eric J. Velazquez, MD, FACP, FACC, FASE,
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE
 CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
CLINCIAL APPLICATION OF GUIDELINES IN HEART FAILURE SSC Journée d Automne 25 novembre 2010 Dr. Charles Seydoux, spéc. FMH en médecine interne et en cardiologie, Lausanne Dr. Claudia Bösch, Oberärztin Herzinsuffizienz
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
The role of pre hospital thrombolysis. Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel
 The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
The role of pre hospital thrombolysis Aaron Frimerman Hillel Yaffe Medical Center Hadera Israel Is thrombolysis still valid? Disclosure I am an Interventional Cardiologist STEMI is mainly a thrombotic
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
STEMI Linee guida ESC Maddalena Lettino, Italy
 STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta
 Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo