«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
|
|
|
- Clifton Foster
- 6 years ago
- Views:
Transcription
1 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
2 Post cardiac arrest First day of mechanical ventilation No patient received PEEP Mean V T 12mL/kg All patients received PEEP Mean V T 9 ml/kg Wongsurakiat, 2004, 126, 1281
3 END-INSPIRATORY LUNG VOLUME CRF spont + CRF PEEP + V T
4 IDEAL 2005 PEEP Good oxygenation (PaO 2, PaO 2 /FiO 2 ) Recruitment and prevention of derecruitment (homogenous ventilation) Absence of cyclic dynamic compression and reexpansion of peripheral airawys Limited end-inspiratory pressures and volumes Limited negative hemodynamic effects
5 PEEP STORY Suter (1975) Kirby (1975) Lamy (1976) Matamis (1984) CTScan (1993)
6 «Best» PEEP? «PEEP coinciding with the maximum oxygen transport» Peter M Suter, NEJM, 1975, 284
7 Peter M Suter, NEJM, 1975, 284
8 Best PEEP : maximum oxygen transport -maximum cardiac output -maximum total compliance Arterial blood gases do no identify the level of PEEP resulting in maximum oxygen transport. Total static compliance is a usefull means of finding the degree of lung distention that provides the best gas exchange with the least risk of alveolar overdistension and lung rupture.
9 SUPER-PEEP? For Q s /Q T < (Kirby), 1995 (DiRusso) Maximum PEEP mean = 27-32cm H 2 O true max = 57 cm H 2 O Fluid balance + 23 L Inotropes and vasopressors +++ Digoxin if PEEP > 20 cm H 2 O!!! Barotrauma 49% Mortality 30%
10 Lamy, ARRD, 1976, 114, 267 CONDENSATION FIBROSIS EDEMA ATELECTASIS TRUE SHUNT DIFFUSION V/Q Baseline PaO 2 47+/ / /-15 PEEP Effect (PaO 2,Q s /Q t ) effect 0 effect +, slow effect ++, fast Chronology early late early Mortality 82% 77% 52% VT 13 ml/kg, Ppeak 60
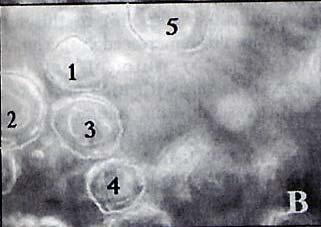
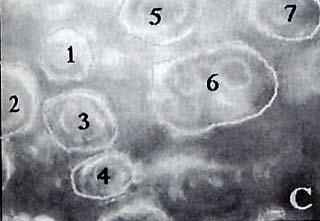
11 Matamis, Chest, 1984
12 Use of inflection point in the ascending limb of the static pressure-volume curve (indication of closing volume and reopening of alveoli and small airways) PREVENTION OF ALVEOLAR COLLAPSE
13 Use of inflection point in the ascending limb of the static pressure-volume curve (indication of closing volume and reopening of alveoli and small airways) PREVENTION OF ALVEOLAR COLLAPSE Argiras, BJA, 1987, 59, 1278 Sandhar, ICM, 1988, 14, 538 Oxygenation score Histological score EELV


14 EELV (ml) Low PEEP LIP PEEP Sandhar, ICM, 1988, 14, 538
15 4 3,5 Hyaline Membrane Score 3 2,5 2 1,5 1 0,5 0 Low PEEP LIP PEEP Sandhar, ICM, 1988, 14, 538
16 Tout cela était trop simple! On oubliait l hétérogénéité pulmonaire!
17 Lung heterogeneity concept Axial distribution -cephalocaudal -anteroposterior Anatomical distribution -diffuse 20% -focal lobar 40% patchy 40% Microscopic distribution

18 DIFFUSE JJR,CCM, 2003 Red Gray Black White Non Aerated Poorly Aerated Normally Aerated Overinflation

19 LOBAR JJR,CCM, 2003 Red Gray Black White Non Aerated Poorly Aerated Normally Aerated Overinflation

20 Schiller, CCM, 2003,31,1126
21 PEEP-induced increase in FRC -Alveolar recruitment: decrease in gas volume in poorly or non aerated area -Alveolar inflation (aeration): increase in volume of normally aerated area -Alveolar overinflation: increase in the volume of overinflated area Nieszkowska, CCM, 2004, 32, 1496

22 Treggiari, CCM, 2002, 30, 1747
23 Duration Duration Duration Dynam ic Crs of MV of EIP > 35 of FiO2 > 0.5 < 20 ml/cmh2o OV ERDIST ENSION ANTERIOR LUNG SEGMENT S ALVEOLAR AIR CYSTS (43%) BRONCHIAL BRONCHIECT ASIS (62%) Treggiari, CCM, 2002, 30, 1747


24 Red Gray Black White Non Aerated Poorly Aerated Normally Aerated Overinflation ZEEP PEEP 15
25
! Non dependent caudal regions!")
26 The «price» of PEEP Overinflation: anatomical and regional distribution?! In 50% of «focal» (vs 0% of diffuse)! Non dependent caudal regions! COPD Nieszkowska, CCM, 2004, 32, 1496


27 10 50
28 Lim, CCM, 2004, 32,2378

29 Potential for recruitment??? 0,35 0,3 0,25 Lung Recruitment 0,2 0,15 0,1 0,05 0-0, PEEP level (cmh2o) ARDS p ARDS extrap Gattinoni, AJRCCM, 1998,
30 Lim, CCM, 2004, 32,2378
31 Lim, CCM, 2004, 32,2378
32 FiO² PEEP 0,3 12 0,3 14 0,4 14 0,4 16 0,5 16 0,5 18 0,5-0,8 20 0,8 22 0, NIH, NEJM, 2004, 351

33 FiO² PEEP 0,3 12 0,3 14 0,4 14 0,4 16 0,5 16 0,5 18 0,5-0,8 20 0,8 22 0,
34 Best PEEP??? Balance -gas exchanges -mechanics -tissues oxygenation (CO, DO 2 ) Adapted for each patient -co-morbidity -origin of ARDS -morphology of ARDS -hemodynamic status -chronology
35 Best PEEP??? Method for choising optimal PEEP? (Ward, 2002, 30, 963) P flex or PEEP best? 68% P flex 86% P best 93% P flex or P best
36 Compliance maximale Compliance PEEP Infection abdominale Pneumonie
37 TIDAL VOLUME PEEP
38 52 Tidal Volume (ml)
39
40
41 Best PEEP??? Target? (Oxygenation, mechanics, O 2 transport) Morphologic basis? (focal, diffuse) Mecanichal basis (pulmonary versus extra-pulmonary ARDS) Chronological basis (early versus late ARDS) Hemodynamic basis (volhemia, compliance, cardiac function)
42 Best PEEP??? Predisposing factors to lung overinflation -focal distribution of the loss of aeration -presence of lung emphysema -degree of lung inflation at ZEEP (COPD) «There is no validated tool available at the bedside for detecting and quantifying lung overinflation» Nieszkowska, CCM, 2004, 32, 1496
43 Universal Best PEEP is a soft dream! Price of PEEP is a reality!
44 CONSOLIDATION COLLAPSE Primum Movens Alveolar epithel injury Endothelial Injury Pathology Inflamm alveolar flooding Interstitial edema Consequence Consolidation Compression Site of action Alveoli Small Airway Clinical situation Primary ARDS Secondary ARDS Morphology "Lobar" "Diffus" Potential for recruitment Low High Risk of hyperinflation High Low ECW/ETOT (Nl = 0.5) 0,2 0,8 Hemodynamic risk of Paw High Low
45 VALI in patients without ALI at the onset of mechanical ventilation Gajic, CCM, 2004, 32, 1817 Patients sans ALI/ARDS 25% développent ALI dans les 5 premiers jours Facteurs de risque Haut V T (OR 1,3 par ml au-dessus de 6 ml/kg) Femmes Petites tailles Transfusions (OR 2,97) Pneumopathies pré-existantes (OR 3,6)
46 Suter s PEEP or Amato s PEEP? The lowest value of RV outflow impedance is associated with the better value of Crs. Schmitt, AJRCCM, 2001,29,1154 ZEEP SUTER AMATO PEEP 0 6+/-3 13+/-4 PaO2 65+/ / /-40 Crs 30 +/-8 35+/-9 27+/-8 SVI 26+/ / /-0.8
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
PEEP nuove indicazioni, stesse problematiche
 PEEP nuove indicazioni, stesse problematiche Franco Valenza Department of Pathophysiology and Transplantation Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico Ossigenazione Clearance CO 2 Kats,
PEEP nuove indicazioni, stesse problematiche Franco Valenza Department of Pathophysiology and Transplantation Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico Ossigenazione Clearance CO 2 Kats,
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Lung CT Scan. Open Access. Paolo Pelosi *.1 and Marcelo Gama de Abreu 2. Gustav Carus, Dresden, Germany
 86 The Open Nuclear Medicine Journal, 2010, 2, 86-98 Lung CT Scan Paolo Pelosi *.1 and Marcelo Gama de Abreu 2 Open Access 1 Department of Ambient, Health and Safety, University of Insubria, Varese, Italy
86 The Open Nuclear Medicine Journal, 2010, 2, 86-98 Lung CT Scan Paolo Pelosi *.1 and Marcelo Gama de Abreu 2 Open Access 1 Department of Ambient, Health and Safety, University of Insubria, Varese, Italy
Chapter 21. Flail Chest. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Respiratory Mechanics
 Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness.
 Bibliography P/V curves This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Global and regional assessment
Bibliography P/V curves This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Global and regional assessment
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Respiratory failure requiring mechanical ventilation
 Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
PFT Interpretation and Reference Values
 PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
PFT Interpretation and Reference Values September 21, 2018 Eric Wong Objectives Understand the components of PFT Interpretation of PFT Clinical Patterns How to choose Reference Values 3 Components Spirometry
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management
:Evidence Based Management") Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Disclosures. Learning Objectives. Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach 3/10/2017
 Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
INTRODUCTION MATERIALS AND METHODS
 J Korean Med Sci 2003; 18: 349-54 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences This study was conducted to evaluate the effectiveness and safety of a practical protocol for titrating
J Korean Med Sci 2003; 18: 349-54 ISSN 1011-8934 Copyright The Korean Academy of Medical Sciences This study was conducted to evaluate the effectiveness and safety of a practical protocol for titrating
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
3/5/14. Disclosures. Background. None. No discussion of non FDA approved products
 Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
Management of Respiratory Disease in the Term Infant
 Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Ventilation in ARDS. 13 February C Evans CONTENTS. Definition Introduction Diagnostic Criteria for ARDS Pathogenesis...
 13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Applied Physiology of One Lung Ventilation
 Applied Physiology of One Lung Ventilation One Lung Ventilation Usual situation Thoracic surgery Lateral decubitus position GA, paralysis, PPV Non-dependant lung collapsed and non-ventilated Chest may
Applied Physiology of One Lung Ventilation One Lung Ventilation Usual situation Thoracic surgery Lateral decubitus position GA, paralysis, PPV Non-dependant lung collapsed and non-ventilated Chest may
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998