ARDS: MANAGEMENT UPDATE
|
|
|
- Oswin Williams
- 6 years ago
- Views:
Transcription


1 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine
2 The AECC Definition Timing Acute onset, within hours Oxygenation ALI PaO2/FiO2<300 (regardless of positive end expiratory pressure level) ARDS PaO2/FiO2<200 (regardless of positive end expiratory pressure level) Chest radiograph Bilateral infiltration seen on frontal chest radiograph Pulmonary artery occlusion pressure <18mmHg when measure or no clinical evidence of left atrial hypertension Bernard GR, et al. Report of the American European consensus conference on ARDS:definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee. Intensive Care Med 1994;20:
3 Berlin Definition of ARDS Timing Within 1 week of a known clinical insult or new or worsening respiratory symptoms Chest imaging Bilateral opacities-not fully explained by effusions, lobar/lung collapse, or nodules Origin of edema Respiratory failure not fully explained by cardiac failure or fluid overload Need objective assesment (eg, echocardiography) to exclude hydrostatic edema if no risk factor present Oxygenetion Mild 200mmHg<PaO2/FiO2 300 with PEEP or CPAP 5cmH2O Moderate 100mmHg<PaO2/FiO2 200 with PEEP or CPAP 5cmH2O Severe PaO2/FiO2 100 with PEEP or CPAP 5cmH2O JAMA 2012;307:

4 Acta Paediatr 2010;99: In China, 26 PICUs, within 1 year period, multicenter prospective study, PICU patients Incidence: ALI in 4%, ARDS in 2.7% Etiology: Pneumonia in 75%, Sepsis in 14.7% of ARDS patients Mortality rate: 44% in children with ARDS Total mortality rate is 15% Mortality rate is significant high especially in children with pneumonia and sepsis.

5
6 TRATMENTS in ARDS Mechanical Ventilation managements Supportive treatments Pharmacologic treatments

7 Mechanical Ventilation Treatments Conventional MV - Pressure Control - Volume Control New Methods - APRV - HFOV
8 Treatment Mains Reduction to O2 consumption Decreased to respiratory work O2 delivery as sufficient and non-toxic concentration Open to atelectatic areas in lung Continious open-lung strategy with ideal PEEP
9 Protective Lung Methods in MV Low TV High TVs is harmful for lung (10-15 cmh2!!! O PIP< ml/kg) High PEEP ~ cmh2o Permissive hypercapnia (ph>7.25, pco2 :60-80mmHg) Permissive hypoxia (po2>50mmhg, so2>%85)
10 Conventional and lung protective MV Tobin MJ. Advances in mechanical ventilation. N Eng J Med 2001;344:
11
12 Positive end-expiratory pressure: PEEP Maximizes alveolar recruitment Evaluate to compliance and set to Increase to compliance ideal PEEP at level of the best of Open to collapsed alveoles and lung compliance. Augmented to ventilation perfusion ratio Decrease to intrapulmonary shunt Decrease the need for oxygene Ideal PEEP is over 2 cmh2o than lower iflection point. The most important effect of PEEP is open lung effect.
13 PEEP and Lower inflection point PEEP= 5 cm H2O PEEP= 12 cm H2O Volume Volume Pressure 5 pressure 12 Lower inflection point
14 The Pressure-Volume relation during MV treatment in patients with ALI Pinhu L, et al. Ventilator-associated lung injury. Lancet 2003;361:
15 Ideal PEEP Technically, the definition of ideal PEEP is not easy. Our main way is one side increase to PEEP and other side decrease to FiO2 FiO2 < PEEP

16 Kenneth P. et al. N Engl J Med 2006
17 Permissive Hypercapnia Well accepted consequence of lung protective strategies of venilatory support. Low tidal volume and together high PEEP cause to increased dead space and caused to hypercapnia (ph>7.25, pco2 :65-85mmHg) For decrease to excessive CO2 produce; - Restrict to excessive carbonhydrate intake - Control to fever - Decrease to muscle activity with sedative and paralytic drugs Contraindications for permissive hypercapnia; Increased intracranial pressure, Sickle cell disease, Pulmonary HT Severe cardiac dysfunction
18 Prone Positioning Another way to recruit atelectatic dependent zones of the lung. Several mechanism have been proposed to account for this effect, Better Ventilation/perfusion matching Increase to end-expiratory lung volume Improve overall oxygenetion But there is not clearly effect on mortality and duration of MV in meta-analyses. Priya Prabhakaran. ARDS.. Indian Pediatr 2010;47.

19
20 High Frequency Oscillatory Ventilation (HFOV) With HFOV treatment in ARDS, There is possible to provide open alveoles and prevent to excessive strenght of lung tissue with low TV (1ml/kg) There is additional advantage that CO2 removel by high respiratory rate (900/min) in HFOV.
x100] If OI > 13-15; HFOV")
21 HFOV Oxygenetion Index= OI OI= [(MAPx FiO2/PaO2)x100] If OI > 13-15; HFOV indication
22 HFOV Advantages Improve oxygenetion in shorter time Decrease to risk of barotrauma than conventional MV methods Demonstrated to decreased changes of chronic lung diseases ARDS in Children. Pediatric Critical Care, 3rd Edition, Brandley Fuhrrman,Jerry Zimmerman, 2011; Arnold J, Crit Care Med 1994
 patients survived Indian J Pediatr")
23 Turkey In 20 children with severe ARDS, Conventional MV was switched to HFOV because of insuffiency 13/20 (65%) patients survived Indian J Pediatr 2009
24 APRV: Airway Pressure Release Ventilation More easier to exhalation with very low PEEP and high and long PIP Possible Effects: Improve to ventilation/perfusion match Decrease to barotrauma and hemodynamic adverse events of mechanical ventilation
 7 children with ARDS, Conventional MV is insuffiency and switched to APRV 4/7 survived.")

25 3 children with ARDS Switcthed to APRV because of severe hypoxemia contineued under conventional MV All patients survived. Indian J Pediatr 2010;77: ) 7 children with ARDS, Conventional MV is insuffiency and switched to APRV 4/7 survived. Pediatr Pulmonol 2010;42: In adults, Randomized-controlled study for compare to conventional MV (SIMV+PS) and APRV mode. -There isn t any significant duration of MV and mortality between two modes. Varpula T, et al. Acta Aneasthesiol Scand 2004;48: There isn t any randomized-controlled study about the APRV mode effects in children with the ARDS.



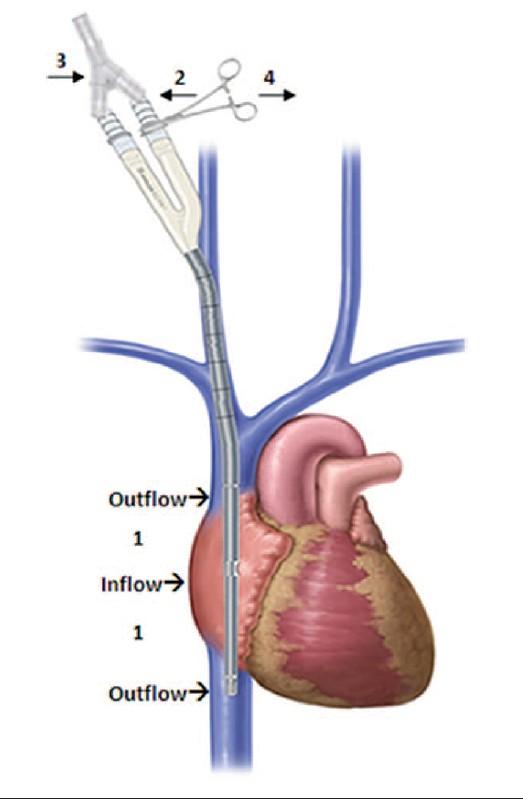
26 ECMO (Extracorpereal Membran Oxygenetion)
27 Extracorpereal Life Support Provides both gas exhange and circulatory support for children with life-threatening ALI and ARDS. Allows the lung the rest from mechanical ventilation. ELCS can be provided by venoarterial or venovenous bypass techniques
 Duration time of ECMO: 10 (7-15) days Mortality")
28 15 adult ICUs, ECMO performed when conventional MV was insufficient, 68 patients with ARDS due to pandemic influenza At the beginning of the ECMO; PO2 /FiO2 : 56 (48-63) Duration time of ECMO: 10 (7-15) days Mortality rate: 29%
29
30 Supportive Tretments 1) Hemodynamic Support - Fluid restriction? (Avoid to volume overload!!!!) - Determine to intravascular volume(cvp follow!!!!) - Albumin infusion? - Inotropic support (Dobutamin?) 2) Feeding - Prefer enteral feeding - Low carbonhydrate, and high lipid involved parenteral feeding. ARDS in Children, Pediatric Critical Care, Third Edition, Brandley Fuhrrman,Jerry Zimmerman, chapter 46, page:

31 Pharmacologic Therapies Surfactant Steroid İnhaler nitric oxide Other agents
32 SURFACTANT Main effect ; prevent to alveol collapse Basic trouble in ARDS; surfactant making and functional trouble ELEŞTİRİ: But there is contraversial opinion about this study; There are more immunsupressed children in non-surfactant group(22 patient in surfactant group vs 30 children in non-surfactant group) Unclear surfactant doses and type Very expensive treatment
33 Pulmonary Pharmacol & Therapeutics 2003;16: Turkey, 36 children with ARDS 12 children treated with surfactant, The most frequent cause is Sepsis (42%) Within 24-hour after surfactant treatment; improved oxygenetion Mortatlity rate is 42% in surfactant treated group vs 63% in non-surfactant treated group (p>0.05)

34 Crit Care studies, 314 children with ARDS, -Surfactant can decrease to mortality -Increase to without mechanical ventilation days, -There isn t important adverse effect Crit Care 2007 There are unresponsive a lot of questions about surfactant, Unclear treatment doses and time In surfactant treatment; we should decide, individually

35 STEROID -In adult studies, steroid may beneficial if steroid treatment is started in late period (>7day). -There isn t randomized-controlled study about streoid treatment in children with ARDS. -It is beneficial in anectodal cases. -Steroid treatmen in ARDS; increase to neuromuscular weakness and sepsis.
36 N Engl J Med 2006;354; adult patients wit ARDS longer than 7 days, Randomized-controlled study, 91 patients received placebo, 89 patients received methyl prednisolon (2mg/kg) There isn t significant difference mortality rates at 60th day (28,6% and 29.2%) between 2 groups. In steroid treated group; oxygenetion, without ventilator days and blood pressure are better It isn t effect on infection risk. Increased to neuromuscular weakness.
37 ino ino selective pulmonary vasodilatator and minimal systemic effect Improve oxygenetion but can not be decreased mortality rate. If OI>25 must be consider ino treatment. Its effects can be increased together with HFOV. DobynsEL, et al. Multicenter randomized controlled trial of inhaled nitric oxide therapy on gas exchange in children with acute hypoxic respiratory failure. J Pediatr 1999;4:
38 IMMUNODEFIENCY/ ARDS / MORTALITY ARDS developed in 43 children after BMT, BMT indications: Solid tumors (30%), leukemia (44%), Primary immunodefincies (19%), and aplastic anemia (7%). The most frequent cause of ARDS: pneumonia (43%) Mortality rate is 88% Bojko T, et al. Acute hypoxemic respiratory failure in children following bone marrow transplantation: An outcome and pathologic study. Crit Care Med 1995;23: MV indications after BMT in children -Mortality rate is 81% Keenan Ht, et al. Outcome of childre who required mechanically ventilatory support after bone marrow tranplantation. Crit Care Med 2000;28; In 5 children with SCID and ARDS developed at follow; mortality rate is 100%. Kendirli T, Doğu F, İkincioğulları A, Aytekin C, Yıldıran A, Yüksek M, İnce E. Fatal acute respiratory distress syndrome in children with combined immunedeficiencies. Asthma Allergy Immunol 2009;7:
39 PROGNOSIS Mortality rate is decreasing in ALI and ARDS. Mortality rate is 20-30% The causes of Mortality: - Severe respiratory failure (especially hypoxemia) - Multiorgan failure The most frequent cause of mortality in Nosocomial infections children with ARDS; Sepsis and MODS Primary/secondary infections - Neurologic deficit - Prolongation of mechanical ventilation - Critical illness polymyoneuropathy - Pneumothorax, pneumomediastinum
40
41
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
ECMO FOR PEDIATRIC RESPIRATORY FAILURE. Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta
 ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
ECMO FOR PEDIATRIC RESPIRATORY FAILURE Novik Budiwardhana * PCICU Harapan Kita National Cardiovascular Center Jakarta Introduction Case D 8 month old baby with severe ARDS with fungal sepsis. He was on
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
SWISS SOCIETY OF NEONATOLOGY. Supercarbia in an infant with meconium aspiration syndrome
 SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Literature List APRV 2016
 Literature List APRV 2016 APRV Literature List INDEX Writer Subject Publication Page Li JQ. et Yoshihisa Morimoto et Clinical research about airway pressure release ventilation for moderate to severe acute
Literature List APRV 2016 APRV Literature List INDEX Writer Subject Publication Page Li JQ. et Yoshihisa Morimoto et Clinical research about airway pressure release ventilation for moderate to severe acute
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
QuickLung Breather Patient Settings
 The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
Ventilation in ARDS. 13 February C Evans CONTENTS. Definition Introduction Diagnostic Criteria for ARDS Pathogenesis...
 13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Airway Pressure Release Ventilation: A Pediatric Case Series
 Pediatric Pulmonology 42:83 88 (2007) Case Reports Airway Pressure Release Ventilation: A Pediatric Case Series Jambunathan Krishnan, MD 1 * and Wynne Morrison, MD 2 Summary. Airway pressure release ventilation
Pediatric Pulmonology 42:83 88 (2007) Case Reports Airway Pressure Release Ventilation: A Pediatric Case Series Jambunathan Krishnan, MD 1 * and Wynne Morrison, MD 2 Summary. Airway pressure release ventilation
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza
 was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza") PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
PANEL DISCUSSION The 1918 flu pandemic (January 1918 December 1920) was an unusually deadly influenza pandemic, the first of the two pandemics involvingh1n1 influenza virus. [1] It infected 500 million
Management of Respiratory Disease in the Term Infant
 Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
HFOV IN THE NON-RECRUITABLE LUNG
 HFOV IN THE NON-RECRUITABLE LUNG HFOV IN THE NON-RECRUITABLE LUNG PPHN Pulmonary hypoplasia after PPROM Congenital diaphragmatic hernia Pulmonary interstitial emphysema / cystic lung disease 1 30 Mean
HFOV IN THE NON-RECRUITABLE LUNG HFOV IN THE NON-RECRUITABLE LUNG PPHN Pulmonary hypoplasia after PPROM Congenital diaphragmatic hernia Pulmonary interstitial emphysema / cystic lung disease 1 30 Mean
Key words: ARDS; high-frequency oscillation; high-frequency ventilation; mechanical ventilation; respiratory failure
 High-Frequency Oscillatory Ventilation in Adults* The Toronto Experience Sangeeta Mehta, MD; John Granton, MD, FCCP; Rod J. MacDonald, RRCP; Dennis Bowman, BSc; Andrea Matte-Martyn, RRT; Thomas Bachman,
High-Frequency Oscillatory Ventilation in Adults* The Toronto Experience Sangeeta Mehta, MD; John Granton, MD, FCCP; Rod J. MacDonald, RRCP; Dennis Bowman, BSc; Andrea Matte-Martyn, RRT; Thomas Bachman,
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
VENTILATING CHILDREN- a quick recap. Dr Despina Demopoulos Paediatric Intensivist
 VENTILATING CHILDREN- a quick recap Dr Despina Demopoulos Paediatric Intensivist Introduction Six Tricks Case Scenarios Goals of ventilation Modes of ventilation Different diseases Conclusion OVERVIEW
VENTILATING CHILDREN- a quick recap Dr Despina Demopoulos Paediatric Intensivist Introduction Six Tricks Case Scenarios Goals of ventilation Modes of ventilation Different diseases Conclusion OVERVIEW