Renal Artery Stenting
|
|
|
- Cory Tyler
- 6 years ago
- Views:
Transcription

1 Renal Artery Stenting We are unable to predict patients who will benefit from RAS MEET 2008 Thomas Ischinger MD FACC FESC Heart Center Bogenhausen Munich, Germany
2 Disclosure Statement of Financial Interest I DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation. MEET 2008
3 Effects of renal artery stenosis on blood pressure and the heart: Pathophysiology 1. Renin-Angiotensin-Aldosteron-System Hormonal System regulates: Fluid volume, blood pressure, cardiovascular function Angiotensinogen Angiotensin I Renin Angiotensin Converting Enzyme Stenosis Negative Feedback Angiotensin II Aldosteron Vasoconstriction Sodium/Water- Retention Bloodpressure Elevation
4 Association of renal artery stenosis and heart failure acute heart failure, pulmonary edema, cardiac arrhythmia, angina pectoris Risk factors: hypertension, nicotin, diabetes, FA, HLP, age, genter Atherosclerosis, renal artery stenosis chronic heart failure, chronic renal insufficiency hypertension, increased LV-mass, syst. and diast. dysfunction activated RAAS, renal dysfunction

5 G.Zie, female, 55y Post reocclusion after 1.RAS of right renal artery.silent at szinti. Medication: Nebivolol 5mg, Ramipiril 30mg, Valsartan 240mg, HCT 20mg, Lercarnidipin 20mg, Moxonidin 0.3mg, Torasemid 20mg Therapy: recanalization + 2.stenting of renal artery
6 Renal artery stenting, illustrative case Malignant hypertension in 54 year old female with Angina as initially leading symptom stenting of right renal ostial stenosis Reocclusion Recanalization & restenting Reocclusion Further therapies & medications isch05

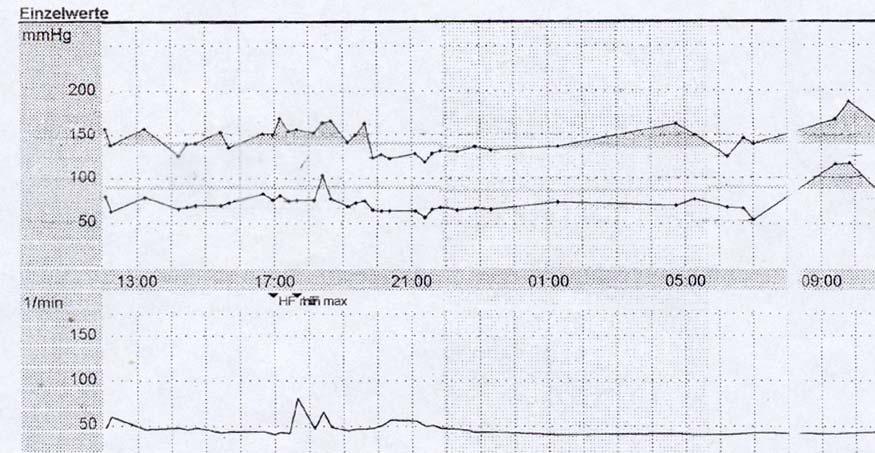
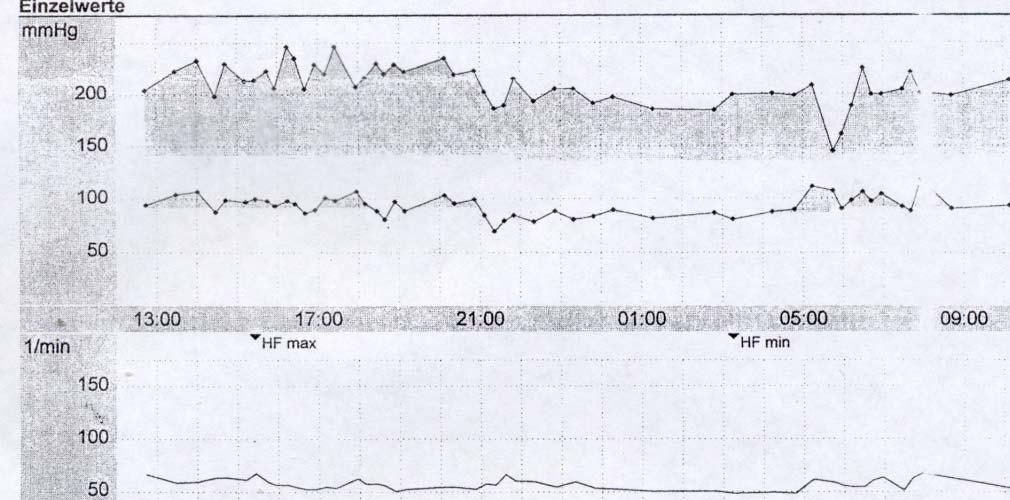


7 24 h RR RAS, illustrative case RAS occluded angiographies RAS recan / restented RAS reoccluded isch05
8 Reoccluded renal stent


.")
9 Complex management for complex vascular pts:, Cardiac destabilization and hypertension with RAS History: H.S. 61 J / S/P bypass Surgery, multiple PTCA+stent, ACS with bei hypertensive crisis, pulm. edema, CCU, acute coronary angio.no coronary restenosis, high grade prox. RAS right (Angio + Duplex). Left 50%. Tx: PTA right RAS, cutting bal., stent. 1 year FU: no antihypertensive medication (110/90) Isch 08
10 Renal artery stenting: Background & Facts Atherosclerotic disease of renal arteries is common - > 7% over age 65, > 10% with chr renal disease, >30% of older pts with CHF - in cardiac cath pts a >70% RAS was present in : 7% of pts w severe atherosclerosis, in 9% w hypertension, in 16% with renal dysfunction, in 22% w pulmonary edema RAS > 50% is independ. predictor of all cause mortality (30-50%!) RAS may lead to renovasc.hypertx & and loss of renal function RAS is considered an avoidable cause of renal failure RAS >60% DS progress to occlusion in 5% of pts/year RA stenting is Tx of choice, yet is associated with hazards Selection of pts who may (predictably?) benefit is warranted Buller JACC 2004, White Circ 2006
11 What are the benefits we wish to expect from RA stenting? Long term patency of the RA...and thereby...sustained improvement in BP control Improvement in renal functional parameters Slowing of deterioration of renal funtion (delay of end stage renal failure) Decrease of cardiac destabilisation syndromes Decrease of all cause mortality (cardiac, cerebrovascular events)
12 Renal artery stenting:outcome reporting I Definition of failure & benefit (benefit = cure or improvement) Anatomic success: < 30% DS by QCA, MLD > 2mm Hemodynamic success: translesional P gradient < 20mmHg, PSV < 180cm/s, RAR (renal/aortic ratio) < 3 Clinical success: -cardiovascular events (MI, stroke, UA, flash pulm. edema) -hypertension > 120 days post tx (cure: dp<90,sp<140 w/o drugs, improvement: on drugs, failure: no change) -renal function: absolute value of creatinine ( binary outcome ) & slope of functional decline (5xCrea pre during 3 mos / 5x Crea post Tx for 3mos, starting 1 week post tx) AHA Guidelines for Reporting Renal Artery Revascularization, Circulation 2002; 106:1572
13 Breakpoint analysis of GFR Benefit = improvement or stabilization of slope alpha2 post intervention Rundback, J. H. et al. Circulation 2002;106:
14 Renal artery stenting: Outcome reporting II Patency or restenosis (>50%DS): primary or assisted primary patency, secondary patency(after reocclusion) 3-6 mos..?) Complications: (within 30 days) -Major Clinical Adverse Events (MaCE), systemic and local: additional procedure, prolonged LOS, transfusion, surgical revision, death, MI, stroke, renal failure -Minor Clinical Adverse Events (MiCE): no prolonged LOS, hematoma, transient rise in Crea AHA Guidelines for Reporting Renal Artery Revascularization, Circulation 2002; 106:1572
15 Is there any evidence that RAS works? Author year n study endpoint Plouin 1998 n=58 R med vs bal BP ns Webster 1998 n=55 R med vs bal BP/RF ns Jaarsveld 2000 n=106 R med vs bal BP/RF ns Nordmann 2003 n= 219 med vs bal meta BP red sign. De Ven 1999 n=84 R stent vs bal Patency x 4,no BP/renF Soulez 2003 n=74 NR BP red in 50% Zeller 2003 n=215 NR BP red in76% crea red in 52% ASTRAL 2008 n=806 R med vs stent BP/RF/events ns CORAL 2008 R med vs stent+med ongoing BP=blood pressure, RF=renal function, red=reduction, ns=non significant, NR = non randomized Isch meet 2008
16 The ASTRAL study (Angioplasty and STenting for Renal Artery Lesions) Pts: n=806, with > 60% renal stenosis, average crea 2.0, 33% diabetes, 50% CAD Randomization: stenting vs medical tx Successful stenting in 88% Complications in 3% 1 year: no differences between tx: -rise of crea in both groups by 0.2 -similar event rates, renal and cardio/cerebrovascular -arterial pressure reduction similar in both groups ACC i2 summit, Chicago, April 2008 Isch meet 2008
17 Unexpected deterioration of renal function by RA stenting : RESIST study N=100 Zur Anzeige wird der QuickTime Dekompressor TIFF (Unkomprimiert) benötigt.
18 Complications Renal Complications (total 6-10%): -Deterioration of renal function (1-10%) (embolism, contrast induced nephropathy) -renal artery dissection (< 2-3%) -aortic dissection (<1%) -renal artery perforation (< 1%) -dislocation/embolization of stent (<1%) Access complications (3-4%): -bleeding, transfusion, surgical revision, false aneurysm (compression) Isch meet 2008
19 Renal stenting: Have expectations come true? current knowledge and guesses Anatomical success (stenosis reduction): almost always Improvement of BP? Probably in some patients, but durable? Improvement in renal function? Sometimes Slowing of renal functional loss? Probably sometimes Delay of end stage renal failure? Unknown Saving lives by preventing cardiovascular events? Unknown Isch meet 2008
20 Selection of patients who have may benefit from RAS - clinical parameters High prevalence in : atherosclerotic vascular disease in multiple vasc territories > 60% DS (CAD, supraaortic, PAD), Heart F Proven renal hypertension (more likely: absence of fam hx, resistant Hytx, reduction of renal function post ACE, > 1.5cm diff in kidney size, younger age) Bilateral stenoses (significant) Single kidney Resistant Hypertension Elevated Serum-Crea Pulm. flash edema Kidney length > 90 mm Przewlocki 2007, Bates 2008 Isch Meet 2008
21 Evidence for no/low predictability? Even after most stringent patient selection for significant renal artery stenosis = DS > 70%, hypertension and/or Crea elevation: Some improvement in hypertension in 50%-75% (8% cure, 42% improved No/some improvement in Crea clearance (0-52%) No clinical parameters to reliably predict successful outcome (-high Crea, low LV predict RF, -female, high BP, preserved parenchym predict BP) No angiographic predictor with current selction criteria (clinical, functional & anatomic criteria): clinical success in < 2/3 of pts Soulez AJR 2003, Zeller Circ 2003) Isch meet 2008
22 Why is there no predictable cure of hypertension by stenting of significant Atheromatous Renal Artery Stenosis (ARAS)? Because ARAS is not the (target)disease to treat? Because ARAS is not so much the cause of hypertension but rather the consequence of the atheromatous process for which hypertension is the major contributor.....and patients with ARAS tend to have generalized atherosclerotic disease in coronary, cerebral and peripheral circulation Beevers, J Human Hypertension 2007 Isch meet 2008
23 But:BP improvement by Stenting despite RI>0.8 = severe nephrosclerosis* From Zeller Circ 2003 *improvement in renal function (Crea) with RI > 0.7
24 Is lack of predictability of therapeutic benefit the nail in the coffin of RA stenting? No, because measureable benefit in > 50% of selected pts may outweigh useless procedures - yet: complications must be avoided/minimized (is likely with experience / selection) No, because there is evidence, that refined (functional) selection criteria or criteria that reflect function, improve likelihood of clinical benefit No, because restenosis / low patency rates may interfere with longer term improvement, thus concealing benefit.. Yes, if intense medical treatment is equally effective in avoiding renal failure, cardiovascular events and decreasing hypertension as a patent renal artery...
25 Can we better identify predictors for benefit or predictors for failure? Definitely NOT, if we rely on angiography as gold (and only) standard for assessing hemodynamic significance of RAS May be some, if we use improved functional criteria... Therefore next step: improved selection process..?
26 Poor correlation between renal angiography and hemodynamic parameters Subramanian 2005
27 Excellent correlation between renal FFR & baseline PG Subramanian, Catheter Cardiovasc Interv 2005
28 Next step: Avoid Overestimation of stenosis significance by degree & parameter function = avoid wrong Tx targets Current / revised value Diagnostic accuracy RAR > 3.5 > % 15% EDV(cm/s) > 90 > 75 77% 11% MLD (mm) < 2 < % 15% DS (%) > 50 > 65% 60% 38% PSV(cm/s) > 180 > % 55% Pd/Pa < 90 accepted RI bi/unilat 0.75(0.65) Evaluation of 66% / 60% Kidney Length > 90 mm 70% False positive stenosis & tissue Drieghe EHJ 2008, De Bruyne JACC 2006, Rundback Circ 2002,Soulez AJR 2003 Isch meet 2008
29 But: Lack of Correlation Between Renal Translesional Pressure Gradients and Treatment Response After Renal Artery Stent Placement 40 Peak, mm Hg Mean, mm Hg Hyperemic, mm Hg Responders 28.6 ± ± ±17.9 Nonresponders 30.7 ± ± ±10.9 P White Circ 2006 Isch meet 2008
30 We only need to reliably answer 2 questions...: 1.- Is degree of stenosis significant enough to trigger RENIN release and cause renal hypertension? 2.- Does cure of stenosis cure kidney... and decrease RENIN?
31 Is that possible by identifying predictors for benefit or predictors for failure? Definitely NOT, if we rely on angiography as gold (and only) standard for assessing hemodynamic significance of RAS Yes, some, if we use improved functional criteria (in combination with few clinical criteria), but still not reliably Complications, albeit rare, can not predictably be avoided, therefore must also influence pt selection by risk/benefit assessment Prediction of failure is certainly not reliable enough to deny renal artery stenting to patients who may progress to loss of kidney and worse cardiovascular event prognosis
32
33 Incidence of RAS at cardiac catheterization Study Authors Patients, n Any RAS, % RAS 50%, % Bilateral, % Aqel et al NR Weber-Mzell et al Rihal et al Vetrovec et al Harding et al Jean et al NR Mean±SD ±3.6 19±6 17.4±14.2 RAS indicates renal artery stenosis; NR, not reported. White, Circ 2006
34 Causes of Increased Prevalence of Renal Artery Stenosis Onset of hypertension 30 years or 55 years Malignant, accelerated, or resistant hypertension Unexplained renal dysfunction Development of azotemia with an ACE inhibitor or ARB medication Unexplained size discrepancy of 1.5 cm between kidneys Cardiac disturbance syndrome (flash pulmonary edema) Peripheral arterial disease (abdominal aortic aneurysm or ABI <0.9) Multivessel ( 2) coronary artery disease ACE indicates angiotensin-converting enzyme; ARB, angiotensin-receptor blocker; and ABI, ankle brachial index. White, Circ 2006
35 Renal Artery Stenting: Complications Study Authors Patients, n Death, % Dialysis, % Major Complications,% Rocha-Singh et al Tuttle et al White et al Burket et al Dorros et al Total 795 <1% <1% 2.0% Major complications include death, myocardial infarction, emergency surgery, need for dialysis, or blood transfusion. White Circ 2006
36 RAS facts and uncertainty Facts: High prevalence of renal artery stenosis in vascular patients RAS marker of CV risk Renovascular HTN present in 5% Questions: Does PTRA or stenting improve BP? Is renal function preserved after RA stenting? Does RA stenting lower CV events?
37 ACC/AHA Guidelines 2006 INDICATIONS FOR RENAL REVASCULARIZATION Hypertension Class IIa (Level of evidence: B) Preservation of Renal Function Class IIa (Level of evidence: B) RAS and CKD with b/l RAS or RAS to a solitary functioning kidney. Class IIb (Level of evidence: C) RAS and CRI and u/l RAS CHF and Unstable Angina Class I (Level of evidence: B) unexplained pulmonary edema Class IIa (Level of evidence: B) RAS and unstable angina NO LEVEL 1/A DATA multiple RCT s or meta-analyses to support any renal intervention
38 Renal Trials to date Evaluating Stenting: Van de Ven RCT, restenosis: stenting 14%, PTRA 48% ASPIRE 2 salvage stenting better than OPC GREAT Trial Renal DES RENAISSANCE Trial Evaluating BP response: Webster PTRA only beneficial for bilateral disease EMMA PTRA no better than medical therapy DRASTIC PTRA no better than medical therapy
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Renal Artery Stenting
 Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
PCI for Renal Artery stenosis
 PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10
Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10
CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective
 CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective Michael R. Jaff, DO Massachusetts General Hospital Boston, Massachusetts, USA Michael R. Jaff, DO Conflicts of Interest
CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective Michael R. Jaff, DO Massachusetts General Hospital Boston, Massachusetts, USA Michael R. Jaff, DO Conflicts of Interest
Renal Artery Stenosis: Insights from the CORAL Trial
 Renal Artery Stenosis: Insights from the CORAL Trial Christopher J. Cooper, M.D., FACC, FACP Dean and Senior Vice President University of Toledo, College of Medicine President, Ohio Chapter ACC State of
Renal Artery Stenosis: Insights from the CORAL Trial Christopher J. Cooper, M.D., FACC, FACP Dean and Senior Vice President University of Toledo, College of Medicine President, Ohio Chapter ACC State of
Renal Intervention. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
RENAL ARTERY PTA. JH PEREGRIN IKEM, Prague
 RENAL ARTERY PTA JH PEREGRIN IKEM, Prague PTRA/Stenting PTRA technical success rate > 90 % In some patients helps control hypertension In some patients can improve kidney function Serious complications
RENAL ARTERY PTA JH PEREGRIN IKEM, Prague PTRA/Stenting PTRA technical success rate > 90 % In some patients helps control hypertension In some patients can improve kidney function Serious complications
Masahiko Fujihara, MD
 Verify the efficacy of renal artery stenting to define the predictive factors by physiological assessment with pressure wire gradient VERDICT study Masahiko Fujihara, MD Kishiwada Tokushukai Hospital Osaka,
Verify the efficacy of renal artery stenting to define the predictive factors by physiological assessment with pressure wire gradient VERDICT study Masahiko Fujihara, MD Kishiwada Tokushukai Hospital Osaka,
Effective Health Care
 Number 5 Effective Health Care Comparative Effectiveness of Management Strategies for Renal Artery Stenosis Executive Summary Background Renal artery stenosis (RAS) is defined as the narrowing of the lumen
Number 5 Effective Health Care Comparative Effectiveness of Management Strategies for Renal Artery Stenosis Executive Summary Background Renal artery stenosis (RAS) is defined as the narrowing of the lumen
Appropriate Patient Identification For Renal Artery Intervention Remains Challenging
 Renal Intervention Herbert D. Aronow, MD, MPH, FACC, FSCAI, FSVM Director, Interventional Cardiology, Cardiovascular Institute Director, Cardiac Cath Labs, Rhode Island &The Miriam Hospitals None Disclosures
Renal Intervention Herbert D. Aronow, MD, MPH, FACC, FSCAI, FSVM Director, Interventional Cardiology, Cardiovascular Institute Director, Cardiac Cath Labs, Rhode Island &The Miriam Hospitals None Disclosures
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
How to assess the hemodynamic importance of a renal artery stenosis. Felix Mahfoud, MD Saarland University Hospital Homburg/Saar, Germany
 How to assess the hemodynamic importance of a renal artery stenosis Felix Mahfoud, MD Saarland University Hospital Homburg/Saar, Germany How to assess renal artery stenosis severity 1. Non-invasive assessments
How to assess the hemodynamic importance of a renal artery stenosis Felix Mahfoud, MD Saarland University Hospital Homburg/Saar, Germany How to assess renal artery stenosis severity 1. Non-invasive assessments
MEET /06/2013 SESSION : RENAL AND VISCERAL
 MEET 2003 11/06/2013 SESSION : RENAL AND VISCERAL AFTER 35 YEARS, WHAT ARE THE INDICATIONS AND RESULTS OF PTRA IN PATIENTS WITH RI OR RVH? THOMAS SOS, MD NYPH CORNELL New York, NY THOMAS SOS, MD NYPH CORNELL
MEET 2003 11/06/2013 SESSION : RENAL AND VISCERAL AFTER 35 YEARS, WHAT ARE THE INDICATIONS AND RESULTS OF PTRA IN PATIENTS WITH RI OR RVH? THOMAS SOS, MD NYPH CORNELL New York, NY THOMAS SOS, MD NYPH CORNELL
Renal Artery Disease. None > 65,000,000. Learning objectives: Renal Artery Disease
 Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Diagnosis and management of atherosclerotic renal artery stenosis: improving patient selection and outcomes
 Diagnosis and management of atherosclerotic renal artery stenosis: improving patient selection and outcomes Christopher J White* and Jeffrey W Olin SuMMarY Renal artery stenosis (RAS) is common among patients
Diagnosis and management of atherosclerotic renal artery stenosis: improving patient selection and outcomes Christopher J White* and Jeffrey W Olin SuMMarY Renal artery stenosis (RAS) is common among patients
Renal Artery FFR. Woo-Young Chung. Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center
 Renal Artery FFR Woo-Young Chung Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center Why renal FFR? Renal artery angioplasty (PTRA) Indication of Renal artery angioplasty
Renal Artery FFR Woo-Young Chung Seoul National University, College of Medicine Boramae Medical Center Cardiovascular Center Why renal FFR? Renal artery angioplasty (PTRA) Indication of Renal artery angioplasty
Endovascular treatment
 210..217 NEPHROLOGY 2010; 15, S210 S217 doi:10.1111/j.1440-1797.2009.01243.x Endovascular treatment Date written: February 2009nep_1243 Final submission: August 2009 Authors: Robert MacGinley, Subramanian
210..217 NEPHROLOGY 2010; 15, S210 S217 doi:10.1111/j.1440-1797.2009.01243.x Endovascular treatment Date written: February 2009nep_1243 Final submission: August 2009 Authors: Robert MacGinley, Subramanian
Cindy L. Grines MD FACC FSCAI
 Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Cindy L. Grines MD FACC FSCAI Hofstra Northwell School of Medicine Chair, Cardiology Academic Chief of Cardiology, Northwell Health North Shore University Hospital, Manhasset NY Multivessel Disease in
Case yr old lady; type 2 Diabetes 10 yrs; PVD; hypertension
 Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
RENAL ARTERY STENOSIS. Grand Rounds 10/11/2011
 RENAL ARTERY STENOSIS Grand Rounds 10/11/2011 ARAS Prevalence- 0.5% overall population, 5.5% in ckd pts No correlation between ischemic nephropathy and severity of stenosis Increased risk of vascular events-
RENAL ARTERY STENOSIS Grand Rounds 10/11/2011 ARAS Prevalence- 0.5% overall population, 5.5% in ckd pts No correlation between ischemic nephropathy and severity of stenosis Increased risk of vascular events-
Renal artery stenosis
 Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
The role of percutaneous revascularization for renal artery stenosis
 The role of percutaneous revascularization for renal artery stenosis Gregory J Dubel and Timothy P Murphy Abstract: Renal artery stenosis (RAS) is usually caused by atherosclerosis or fibromuscular dysplasia.
The role of percutaneous revascularization for renal artery stenosis Gregory J Dubel and Timothy P Murphy Abstract: Renal artery stenosis (RAS) is usually caused by atherosclerosis or fibromuscular dysplasia.
NOT FOR PUBLICATION, QUOTATION, OR CITATION RESOLUTION NO. 22
 BE IT RESOLVED, Sponsored By: RESOLUTION NO. 22 that the American College of Radiology adopt the ACR SIR Practice Parameter for the Performance of Angiography, Angioplasty, and Stenting for the Diagnosis
BE IT RESOLVED, Sponsored By: RESOLUTION NO. 22 that the American College of Radiology adopt the ACR SIR Practice Parameter for the Performance of Angiography, Angioplasty, and Stenting for the Diagnosis
Disclosure of Potential Conflicts. Renal Artery Stenosis. RAS Epidemiology. Road Map. Background. ASDIN 7th Annual Scientific Meeting
 Renal Artery Stenosis Disclosure of Potential Conflicts Cytopherx, Inc. R4 Vascular, Inc. Bard Peripheral Vascular Spectranetics, Inc. Alexander S. Yevzlin, MD Associate Professor of Medicine (CHS) ASDIN
Renal Artery Stenosis Disclosure of Potential Conflicts Cytopherx, Inc. R4 Vascular, Inc. Bard Peripheral Vascular Spectranetics, Inc. Alexander S. Yevzlin, MD Associate Professor of Medicine (CHS) ASDIN
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium
 FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
FFR and CABG Emanuele Barbato, MD, PhD, FESC Cardiovascular Center Aalst, Belgium Conflict of Interest Institutional research grants and speaker s fee from St. Jude Medical and Boston Scientic to Cardiovascular
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
A Closer Look: Renal Artery Stenosis. Renal artery stenosis (RAS) is defined as a TOPICS FROM CHEP. Shawn s stenosis
 is defined as a TOPICS FROM CHEP. Shawn s stenosis") TOPICS FROM CHEP A Closer Look: Renal Artery Stenosis On behalf of the Canadian Hypertension Education Program (CHEP), Dr. Tobe gives an overview of renal artery stenosis, including the prevalence, screening
TOPICS FROM CHEP A Closer Look: Renal Artery Stenosis On behalf of the Canadian Hypertension Education Program (CHEP), Dr. Tobe gives an overview of renal artery stenosis, including the prevalence, screening
Interventional Cardiology
 nal Review Interventional Cardiology Selecting patients likely to benefit from renal artery stenting Patients with refractory hypertension, progressive ischemic nephropathy and cardiac destabilization
nal Review Interventional Cardiology Selecting patients likely to benefit from renal artery stenting Patients with refractory hypertension, progressive ischemic nephropathy and cardiac destabilization
Incidence and Prevalence of Atherosclerotic Renal Artery Stenosis (RAS) in Patients with Coronary Artery Disease (CAD)
 in Patients with Coronary Artery Disease (CAD)") Incidence and Prevalence of Atherosclerotic Renal Artery Stenosis (RAS) in Patients with Coronary Artery Disease (CAD) AHMW Islam, S Munwar, S Talukder, AQM Reza Dept. of Invasive & Interventional Cardiology,
Incidence and Prevalence of Atherosclerotic Renal Artery Stenosis (RAS) in Patients with Coronary Artery Disease (CAD) AHMW Islam, S Munwar, S Talukder, AQM Reza Dept. of Invasive & Interventional Cardiology,
Coronary stenting: the appropriate use of FFR
 Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Coronary stenting: the appropriate use of FFR Morton J. Kern, MD Professor of Medicine Chief of Cardiology LBVA Associate Chief Cardiology University California Irvine Orange, California To treat or not
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Clinical Considerations for CTO Revascularization
 Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
Clinical Considerations for CTO Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD, FACC, FSCAI Chief Medical Officer Cordis Cardiology Johnson & Johnson
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018
 11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
11 TH ANNUAL VASCULAR NONINVASIVE TESTING SYMPOSIUM NOVEMBER 10, 2018 RENAL ARTERY DISEASE AND RENOVASCULAR HYPERTENSION 1 WHAT IS RENOVASCULAR HYPERTENSION? https://my.clevelandclinic.org/health/diseases/16459-renovascular-hypertension
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Renal fractional flow reserve and hypertension response after renal artery stenting
 Renal fractional flow reserve and hypertension response after renal artery stenting Jacek Kadziela,Adam Witkowski, Andrzej Januszewicz, Aleksander Prejbisz, Ilona Michałowska, Krzysztof Cedro, Magdalena
Renal fractional flow reserve and hypertension response after renal artery stenting Jacek Kadziela,Adam Witkowski, Andrzej Januszewicz, Aleksander Prejbisz, Ilona Michałowska, Krzysztof Cedro, Magdalena
FFR in Multivessel Disease
 FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
FFR in Multivessel Disease April, 26 2013 Coronary Physiology in the Catheterization Laboratory Location: European Heart House, Nice, France Pim A.L. Tonino, MD, PhD Hartcentrum, Eindhoven, the Netherlands
Hypothesis: When compared to conventional balloon angioplasty, cryoplasty post-dilation decreases the risk of SFA nses in-stent restenosis
 Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!!
 FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FRACTIONAL FLOW RESERVE USE IN THE CATH LAB BECAUSE ANGIOGRAPHY ALONE IS NOT ENOUGH!!!!!!!! Juan Antonio Pastor-Cervantes,M.D FSCAI, FACC Cardiovascular Institute Memorial Regional Hospital Hollywood Florida
FFR-Guided PCI. 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea. Stanford
 4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
4 th Imaging and Physiology Summit October 29 th, 2010 Seoul, Korea FFR-Guided PCI William F. Fearon, M.D. Associate Professor Division of Cardiovascular Medicine University Medical Center Disclosure Statement
Ultrasound of the Renal Arteries
 Ultrasound of the Renal Arteries Greg Curry Vascular Ultrasound Workshop Aug 2017 The Examination Technique Pathophysiology Role of US then and now Background Live Scanning Ultrasound Population: 20% Hypertensive
Ultrasound of the Renal Arteries Greg Curry Vascular Ultrasound Workshop Aug 2017 The Examination Technique Pathophysiology Role of US then and now Background Live Scanning Ultrasound Population: 20% Hypertensive
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
A Polymer-Free Dual Drug-Eluting Stent in Patients with Coronary Artery Disease: Randomized Trial Versus Polymer-Based DES.
 A Polymer-Free Dual Drug-Eluting Stent in Patients with Coronary Artery Disease: Randomized Trial Versus Polymer-Based DES ISAR-TEST 2 Trial Robert A. Byrne, MB MRCPI Deutsches Herzzentrum and 1. Med.
A Polymer-Free Dual Drug-Eluting Stent in Patients with Coronary Artery Disease: Randomized Trial Versus Polymer-Based DES ISAR-TEST 2 Trial Robert A. Byrne, MB MRCPI Deutsches Herzzentrum and 1. Med.
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Clinical Considerations for CTO
 38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
38 RCTs Clinical Considerations for CTO 18,000 pts Revascularization Whom to treat, Who derives benefit and What can we achieve? David E. Kandzari, MD FACC, FSCAI Director, Interventional Cardiology Research
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Predictors of restenosis and cardiovascular events in patients undergoing percutaneous angioplasty for subclavian/innominate artery stenosis
 Predictors of restenosis and cardiovascular events in patients undergoing percutaneous angioplasty for subclavian/innominate artery stenosis Tadeusz Przewlocki, Anna Kablak Ziembicka, Piotr Pieniazek,
Predictors of restenosis and cardiovascular events in patients undergoing percutaneous angioplasty for subclavian/innominate artery stenosis Tadeusz Przewlocki, Anna Kablak Ziembicka, Piotr Pieniazek,
Renal Artery Stenting With Embolic Protection
 Renal Artery Stenting With Embolic Protection Embolic protection during renal stenting may be beneficial, but new device designs are necessary. BY RAJESH M. DAVE, MD Renal artery stenosis (RAS) is the
Renal Artery Stenting With Embolic Protection Embolic protection during renal stenting may be beneficial, but new device designs are necessary. BY RAJESH M. DAVE, MD Renal artery stenosis (RAS) is the
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
TCT mdbuyline.com Clinical Trial Results Summary
 TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
Management of ST-elevation myocardial infarction Update 2009 Late comers: which options?
 European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
European Society of Cardiology Annual Session 2009 Management of ST-elevation myocardial infarction Update 2009 Late comers: which options? Antonio Abbate, MD Assistant Professor of Medicine Virginia Commonwealth
Renal PEI: critical appraisal
 Renal PEI: critical appraisal On Topaz M.D., F.A.C.C.,F.S.V.M. Professor of Medicine & Pathology Director, Interventional Cardiology McGuire Veterans Medical Center Virginia Commonwealth University Richmond,
Renal PEI: critical appraisal On Topaz M.D., F.A.C.C.,F.S.V.M. Professor of Medicine & Pathology Director, Interventional Cardiology McGuire Veterans Medical Center Virginia Commonwealth University Richmond,
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period
 Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Fractional Flow Reserve and the Results of the FAME Study
 Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Imaging and Physiology Summit Seoul, Korea November 21 st, 2009 Fractional Flow Reserve and the Results of the FAME Study William F. Fearon, M.D. Assistant Professor Division of Cardiovascular Medicine
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI
 Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Peter A. Soukas, M.D., FACC, FSVM, FSCAI, RPVI Director, Peripheral Vascular Interventional Laboratory Director, Vascular & Endovascular Medicine Fellowship Program Assistant Professor of Medicine The
Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
 Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 8:87-91, 2010 doi: 10.5049/EBP.2010.8.2.87 Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 8:87-91, 2010 doi: 10.5049/EBP.2010.8.2.87 Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
Evaluation of the Safety and Effectiveness of Renal Artery Stenting After Unsuccessful Balloon Angioplasty The ASPIRE-2 Study
 Journal of the American College of Cardiology Vol. 46, No. 5, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.11.073
Journal of the American College of Cardiology Vol. 46, No. 5, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.11.073
PCI for Chronic Total Occlusions
 PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
PCI for Chronic Total Occlusions Chronic Total Occlusions Why not Medical Treatment? Medical Treatment CTO in 891 pts over 24 years High 10% Mortality Low 2 % 1 year 10 years Puma JA, et al. JACC 1994;23:390A
Catheter Based Denervation for Heart Failure
 Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Catheter Based Denervation for Heart Failure David E. Kandzari, MD, FACC, FSCAI Chief Scientific Officer Director, Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia david.kandzari@piedmont.org
Benefit of Performing PCI Based on FFR
 Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
Benefit of Performing PCI Based on FFR William F. Fearon, MD Associate Professor Director, Interventional Cardiology Stanford University Medical Center Benefit of FFR-Guided PCI FFR-Guided PCI vs. Angiography-Guided
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis
 Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis Chee Yang CHIN, MBChB, MRCP(UK) C.W.L. Chin, P.T.L. Chiam, R.S. Tan National Heart Centre Singapore 26
Simultaneous Acute ST Elevation Myocardial Infarction And Acute Left Subclavian Artery Thrombosis Chee Yang CHIN, MBChB, MRCP(UK) C.W.L. Chin, P.T.L. Chiam, R.S. Tan National Heart Centre Singapore 26
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial
 Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Controversies in Coronary Revascularization. Atlanta CCU April 15, 2016
 Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Controversies in Coronary Revascularization Atlanta CCU April 15, 2016 Habib Samady MD FACC FSCAI Professor of Medicine Director, Interventional Cardiology, Emory University Director, Cardiac Catheterization
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
RAS Epidemiology. Renal Artery Stenosis. Pathophysiology of RAS. Disclosure of Potential Conflicts. Background Pathophysiology of RAS.
 Renal Artery Stenosis RAS Epidemiology Common Disease Incidence General Population 0.1% Hypertensive Population 4% HTN & Suspected CAD 10-20% Malignant HTN 20-30% Malignant HTN and CKD 30-40% Alexander
Renal Artery Stenosis RAS Epidemiology Common Disease Incidence General Population 0.1% Hypertensive Population 4% HTN & Suspected CAD 10-20% Malignant HTN 20-30% Malignant HTN and CKD 30-40% Alexander
CTO Re vascularization in 2013
 CTO Re vascularization in 2013 Is it safe to use/stent the sub intimal space? Dimitri Karmpaliotis, MD, FACC, FSCAI Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia Dimitri.karmpaliotis@piedmont.org
CTO Re vascularization in 2013 Is it safe to use/stent the sub intimal space? Dimitri Karmpaliotis, MD, FACC, FSCAI Interventional Cardiology Piedmont Heart Institute Atlanta, Georgia Dimitri.karmpaliotis@piedmont.org
Renovascular hypertension in children and adolescents
 Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
FRACTIONAL FLOW RESERVE: STANDARD OF CARE
 FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
FRACTIONAL FLOW RESERVE: FROM INVESTIGATIONAL TOOL TO STANDARD OF CARE TCT ASIA Seoul, Korea, april 26 th, 2012 Nico H. J. Pijls, MD, PhD Catharina Hospital, Eindhoven, The Netherlands FRACTIONAL FLOW
Final Clinical and Angiographic Results From a Nationwide Registry of FIREBIRD Sirolimus- Eluting Stent: Firebird In China (FIC) Registry (PI R. Gao)
 Registry (PI R. Gao)") The Microport FIREBIRD Polymer-based Sirolimus- Eluting Stent Clinical Trial Program Update: The FIC and FIREMAN Registries Junbo Ge, MD, FACC, FESC, FSCAI On behalf of Runlin Gao (FIC PI) and Haichang
The Microport FIREBIRD Polymer-based Sirolimus- Eluting Stent Clinical Trial Program Update: The FIC and FIREMAN Registries Junbo Ge, MD, FACC, FESC, FSCAI On behalf of Runlin Gao (FIC PI) and Haichang
Renal artery stenosis (RAS) is a relatively common
 is a relatively common") The Importance of Appropriate Renal Artery Stenting Considerations for diagnosis and treatment of patients with renal artery stenosis. By Massoud A. Leesar, MD, FACC, FSCAI Renal artery stenosis (RAS)
The Importance of Appropriate Renal Artery Stenting Considerations for diagnosis and treatment of patients with renal artery stenosis. By Massoud A. Leesar, MD, FACC, FSCAI Renal artery stenosis (RAS)
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Technical Considerations for Renal Artery Stenting
 CLINICAL REVIEW Technical Considerations for Renal Artery Stenting Jeffrey A. Goldstein, MD, Raghu Kolluri, MS, MD, Krishna Rocha-Singh, MD Abstract Renal artery stenosis (RAS) is the most common secondary
CLINICAL REVIEW Technical Considerations for Renal Artery Stenting Jeffrey A. Goldstein, MD, Raghu Kolluri, MS, MD, Krishna Rocha-Singh, MD Abstract Renal artery stenosis (RAS) is the most common secondary
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Fractional Flow Reserve: Review of the latest data
 Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
Fractional Flow Reserve: Review of the latest data Michalis Hamilos, MD, PhD, FESC University Hospital of Heraklion Fractional Flow Reserve (FFR) Coronary angiography does not always tell the truth Most
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Left Main Intervention: Where are we in 2015?
 Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Left Main Intervention: Where are we in 2015? David A. Cox, MD FSCAI Director, Cardiology Research Associate Director, Cardiac Cath Lab Lehigh Valley Health Network Allentown, PA Fall Fellows Course Laa
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
Instantaneous Wave-Free Ratio
 Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Instantaneous Wave-Free Ratio Alejandro Aquino MD Interventional Cardiology Fellow Washington University in St. Louis Barnes-Jewish Hospital Instantaneous Wave-Free Ratio Alejandro Aquino MD Disclosure
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Why I try to avoid side branch dilatation
 Why I try to avoid side branch dilatation Hyeon-Cheol Gwon Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Why I don t kiss? I kiss! I prefer to discuss SB ballooning rather
Why I try to avoid side branch dilatation Hyeon-Cheol Gwon Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Why I don t kiss? I kiss! I prefer to discuss SB ballooning rather
Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease
 2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
2012 대한춘계심장학회 Perioperative Cardiology Consultations for Noncardiac Surgery Ischemic Heart Disease 울산의대울산대학병원심장내과이상곤 ECG CLASS IIb 1. Preoperative resting 12-lead ECG may be reasonable in patients with
Protection of side branch is essential in treating bifurcation lesions: overview
 Angioplasty Summit TCT Asia Pacific Seoul, April 26-28, 2006 Protection of side branch is essential in treating bifurcation lesions: overview Alfredo R Galassi, MD, FACC, FSCAI, FESC Head of the Catetherization
Angioplasty Summit TCT Asia Pacific Seoul, April 26-28, 2006 Protection of side branch is essential in treating bifurcation lesions: overview Alfredo R Galassi, MD, FACC, FSCAI, FESC Head of the Catetherization
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To