How did I decide on the topics?
|
|
|
- Hannah Shelton
- 6 years ago
- Views:
Transcription


1

2 Disclosures None

3 How did I decide on the topics? Important papers within 1 year vs topics of importance or innovation/aha moments Sepsis Atrial Fibrillation Pneumonia Procalcitonin
4 Objectives By the end of this lecture you should consider: What are the best screening criteria for sepsis (in my work area)? What should I consider regarding anticoagulation in the care of the patient with atrial fibrillation? What is new in the care of the pneumonia patient? Is procalcitonin helpful in making decisions on antibiotic choices?
5 What is the best screening for sepsis?
6 Case 1 67 yo man with hx ESRD and CAD presented 50 days prior to today with unremitting intestinal ischemia causing ileus, requiring TPN. He also was diagnosed with GNR bacteremia 4 days prior. He is on Cipro. This am, patient starts complaining of chest and abdominal pain. His rn reports his heart rate has increased to 124.
7 Case 1 His other vital signs are: T 37 RR 18 BP 120/57 100% on 2 liters What could be going on with this patient?
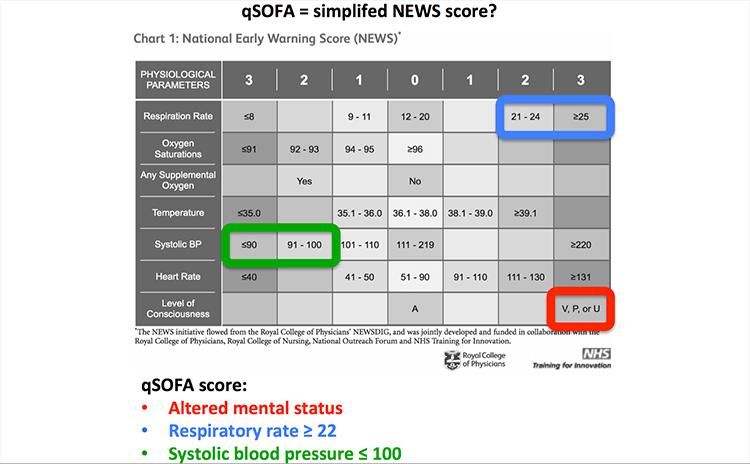
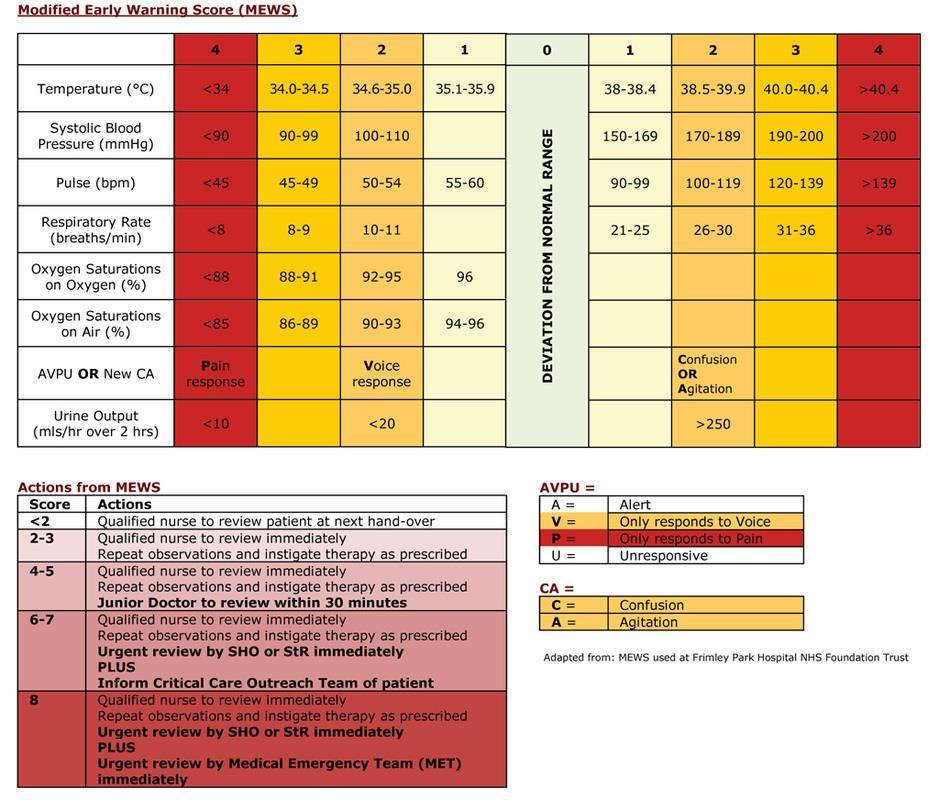
8 Case 1 Which criteria has the highest sensitivity for sepsis? SIRS qsofa NEWS MEWS
9
10
11 Case 1 Which criteria has the highest sensitivity for sepsis? SIRS qsofa NEWS MEWS

12 Am J Respir Crit Care Med Vol 195, Iss 7, pp , Apr 1, 2017
13 University of Chicago, Chicago, Ill All admitted patients who met the criteria for suspicion of infection from 11/08-1/16 (30,677) Observational study Compared for predicting death and composite outcome of death and ICU transfer
14 Scoring system Sens for death+icu Spec for death+icu Main criticism >/= 2 SIRS Id s too many patients >/= 2 qsofa Id s pt s too late >/=8 NEWS Complicated >/=5 MEWS Complicated
15 ..less than one in five patients who later go on to die or be transferred to the ICU will have met >2 qsofa criteria by the time of infection suspicion Furthermore, most patients who experienced the composite outcome met >2 SIRS criteria more than 17 hours before the composite outcome compared with only 5 hours for >2 qsofa, with almost one-half of patients still not meeting >2 qsofa criteria at the time of the outcome. They advocated for not using qsofa
16 Case 1 Which criteria has the highest sensitivity for sepsis? SIRS qsofa NEWS MEWS
17 Case 1 Which criteria should we use to screen for sepsis in this patient? SIRS qsofa NEWS MEWS
18 Which criteria do we use at UNM? SIRS

19 Our Sepsis leader
20 Surviving Sepsis Assuming that the reduction in mortality seen to date can be sustained and 10,000 hospitals comply with the Campaign recommendations, we could save 400,000 lives if we treat only half of the eligible patients with the Surviving Sepsis Campaign Bundles.
21 Case 1 Which of these is not an initial sepsis bundle element? 30ml/kg crystalloid fluid bolus. Draw blood cultures and cultures of other areas of suspected infection. Draw a lactate or lactic acid level. Administer a broad spectrum antibiotic Draw a follow up lactate after fluid

22
23 Caveats / Limitations of ProCESS, ARISE & Promise The overall management of sepsis has changed In all three studies patients had early antibiotics, 30ml/kg of intravenous fluid prior to randomization. We need therefore to be very careful about over interpreting the results in areas where this paradgim is not valid.
24 The River s work was useful. As it provided us a construct on how to understand resuscitation: Start early- (give antibiotics) Correct hypovolaemia Restore perfusion pressure And in some cases a little more may be required..! These concepts are as important today as they ever were.
25 Sepsis bundle C C A L 30ml/kg crystalloid fluid bolus for suspected hypovolemia and/or tissue hypo-perfusion (especially for lactate>4 SBP<90 or MAP<65). Draw blood cultures and cultures of other areas of suspected infection. (Do not delay antibiotics greater than 30 minutes, if unable to draw cultures). Administer a broad spectrum antibiotic. Draw a lactate or lactic acid level.
26 Case 1 Which of these is not an intial sepsis bundle element? 30ml/kg crystalloid fluid bolus. Draw blood cultures and cultures of other areas of suspected infection. Draw a lactate or lactic acid level. Administer a broad spectrum antibiotic Draw a follow up lactate after fluid

27 Case wrapup Patient developed fever however remained hemodynamically stable He was cultured and his antibiotics were broadened to Vancomycin/Zosyn. He did not received fluids due to his ESRD. He had a cardiac arrest 1-2 hours later and died in the ICU 1 day later
28 Bottom line Which sepsis screening criteria you use depends on your setting. However qsofa may be too insensitive Don t forget about the initial sepsis bundle: fluids, cultures, antibiotics and lactate
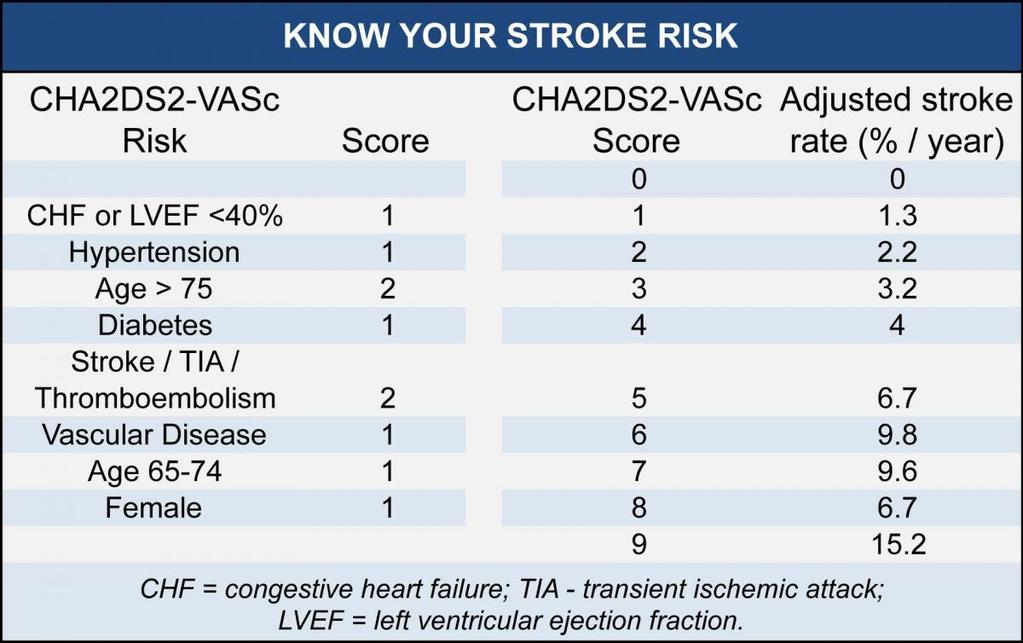
29 What is new in anticoagulation in the care of the patient with afib?
30 Case 2 67 yo man with hx htn and ICH admitted for syncopal episode and found to be in asymptomatic atrial fibrillation.
31 Case 2. Which of these would not help us make a decision on whether to anticoagulate this man? ECHO of the heart Current blood pressure of 120/80 with medication Hx of aortic stenosis Hx of liver cirrhosis
32

33 JAMA. 2015;313(19):
34
35


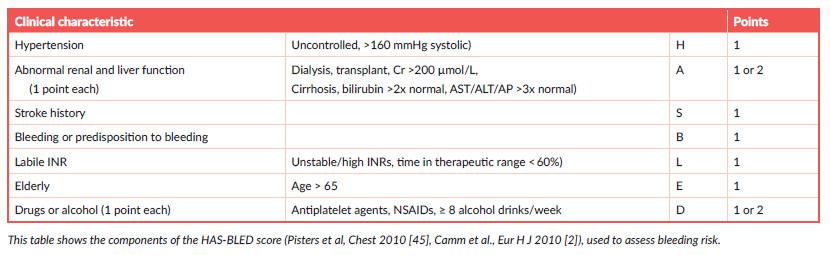
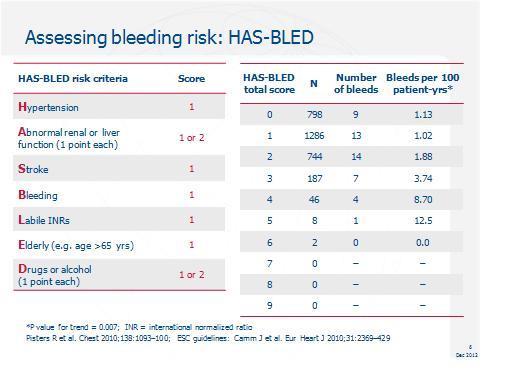
36 Net clinical benefit CVA risk Bleeding risk CHADS2VASC HASBLED Multiplied By 1.5
37 Case 2. Which of these would not help us make a decision on whether to anticoagulate this man? ECHO of the heart Current blood pressure of 120/80 with medication Hx of aortic stenosis Hx of liver cirrhosis
38 Case wrap up CHADS 2 VASC HTN-1 CVA-2 Age-1 HAS BLED CVA-1 Bleeding-1 Elderly-1 4% 3.75% X 1.5=5.6

39
40 Case wrapup Pt was seen by anticoag service Discussion held with pt neurologist Pt had MRI brain multiple prior intracranial hemorrhages, as could be seen with either amyloid angiopathy or severe chronic hypertension. With discussion of all patient started on apixiban
41 Bottom line Use CHADS2VASC and HASBLED when making decisions on anticoagulation

42 mitral stenosis or artificial heart valves Arch CV Dis 10/2015)
43 Case 2. If this patient had a CHADS2 VASC score of 1 what would not be appropriate in terms of anticoagulation for afib? None ASA Warfarin DOAC

44 Part time hospitalist Full time viking

45 Ann Intern Med. 2007;146:
46 29 RCT that tested >12 weeks use of antithrombotic agents in nonvalvular afib Outcomes: All CVA Ischemic ICH Mortality Major bleeding outside head
47 Adjusted dose warfarin vs placebo or control 2900 patients Primary prevention CVA NNT 37 Secondary prevention CVA NNT 12
48 Adjusted dose warfarin vs placebo or control
49 Asa compared with placebo or no treatment 4876 patients Primary prevention CVA NNT 125 Secondary prevention CVA NNT 40
50 Asa compared with placebo or no treatment
51 Case 2. If this patient had a CHADS2 VASC score of 1 what would not be appropriate in terms of anticoagulation for afib? None ASA Warfarin DOAC
52 Guidelines? European Society of Cards still endorse but oac preferred ACC/AHA still endorse ASA level of evid C
53 Bottom line There does not appear to be antithrombotic benefit of ASA in Atrial fibrillation
54 What is new in the care of the pneumonia patient?
55 Case 3 57 yo male with 5 day hospitalization for congestive heart failure within the last month presents with cough productive of green sputum. His T is 39, his HR is 110 and his RR is 26. His CXR shows a dense infiltrate.
56 Case 3. What antibiotics might you put this patient on? Oral amoxicillin/clavulinic acid ceftriaxone iv and azithromycin po vancomycin and piperacillin/tazobactam iv fluconazole iv
57
58 Clinical Infectious Diseases 2014;58(3):330 9
59 Metaanalysis Outcomes: Frequency Resistant Organisms Mortality 24 studies, patients --15 retrospective --12 Asian studies -- high risk of bias --mod-poor quality studies --heterogeneity

60 Table 3. Discrimination of the Healthcare-Associated Pneumonia Concept for Identifying Potentially Resistant Microorganisms Across All Included Studies
61 Conclusions Our meta-analysis raises serious questions about the validity of the HCAP concept by demonstrating that it is poorly predictive of resistant pathogens No difference in mortality
62 Case 3. What antibiotics might you put this patient on? Oral amoxicillin/clavulinic acid ceftriaxone iv and azithromycin po vancomycin and piperacillin/tazobactam iv fluconazole iv
63 Case 4 A 27 yo male with a history of persistent vegetative state due traumatic brain injury with trach, PEG lives in a NH. He presents to ED with increased work of breathing and purulent sputum per the trach. On PE his T is 38.2 and his HR is 130. He has green mucus coming from his trach and coarse breath sounds bilaterally. CXR shows dense pneumonia. You do not know his hx of MDRO.
64 Case 4. What antibiotics might you put this patient on? Oral amoxicillin/clavulinic acid ceftriaxone iv and azithromycin through the PEG vancomycin and piperacillin/tazobactam fluconazole iv
65 Case 4. What antibiotics might you put this patient on? Oral amoxicillin/clavulinic acid ceftriaxone iv and azithromycin through the PEG vancomycin and piperacillin/tazobactam fluconazole iv
66 Bottom line HCAP, in it s current definition, does not select for patients with resistant organiisms. That does not mean that some of those populations which we considered in the HCAP category do not have resistant organisms
67 Is procalcitonin helpful in making decisions on antibiotic choices?
68 Case 5 45 yo male smoker presents to ed with malaise, sob and vomiting/diarrhea. He is found to have diffusely coarse breath sounds on exam. His CXR shows atelectasis vs. infiltrate on the right. He is started on treatment for CAP/aspiration pneumonia. Eventually his diarrheal stool comes back positive for Cdiff and his nasal swab is positive for rhinovirus. His procalcitonin is 2.3.

69 Case 5 Antibiotic stewardship calls and asks that you stop the antibiotics as his procalcitonin of 2.3 is likely due to the Cdiff infection. His respiratory status is not improving after 2-3 days of hospitalization. He requires 4-5 liters of O2 Do you stop the antibiotics?

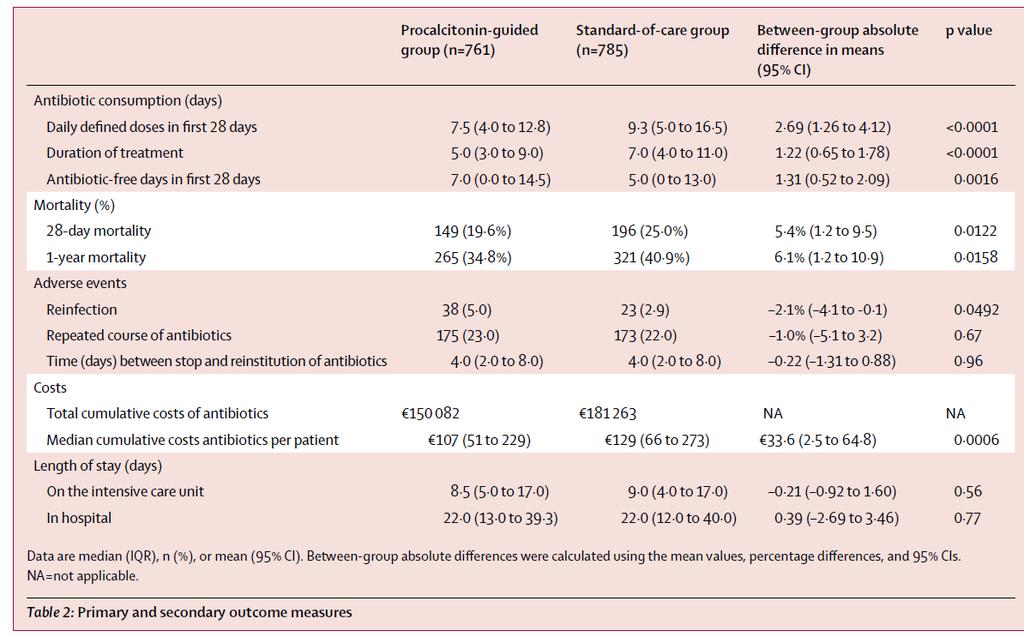
70 Vol 16 July 2016
71 Prospective, multicenter, randomized, controlled open-label intervention Netherlands Sept 2009-July adult ICU patients --80% sepsis or severe sepsis --20% septic shock --65% pulmonary infection, 14% intraabdominal Intervention: Daily measurement of procalcitonin in intervention group. Advice given to discontinue antibiotics if: --Procalcitonin decreased by 80% or to less than.5ug.l Note: Clinicians did not have to follow advice
72
73
74 Case 5 wrapup We continued the respiratory antibiotics for 5 days However once we started treating him for a COPD exacerbation his respiratory status improved substantially. We treated his Cdiff for 10 days after stopping the respiratory antibiotics
75 Bottom line Procalcitonin can help to make decisions about stopping antibiotics but does not supplant clinical reasoning.
76 Thank you. Questions?
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Atrial Fibrillation is Common. The (S)Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation
Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation") The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Medical Apps for Cardiology Uses. There s an App for That!
 Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
Medical Apps for Cardiology Uses There s an App for That! Audience Participation Question #1 1. ASCVD Risk App What is the predicted 10 year CV event rate for a 57 y/o black male patient with treated
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC NPSS Asheville, NC
 Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Documenting in the World of ICD-10 Capturing all your CCs and MCCs Crystal Coen, RN, MSN, FNP-BC 2017 NPSS Asheville, NC Objectives Understand the importance of documenting to the highest specificity Understand
Physician's Core Measure Pocket Guide AMI
 Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Physician's Core Measure Pocket Guide Core Measure Hotline: Ext. 4448 http://centegramedsource.com Indicator: AMI AMI VER. 9/2018 MUST document WHY no ASA unless there is documentation of contraindication
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Update in the Literature 2012
 Update in the Literature 2012 Mel L. Anderson, MD, FACP Chief, Hospital Medicine Section Associate Chief, Medical Service Denver VA Medical Center Associate Professor of Medicine University of Colorado
Update in the Literature 2012 Mel L. Anderson, MD, FACP Chief, Hospital Medicine Section Associate Chief, Medical Service Denver VA Medical Center Associate Professor of Medicine University of Colorado
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
CLAIRE NOWLAN & SAM SEARLE. Pneumonia in the nursing home
 CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
CLAIRE NOWLAN & SAM SEARLE Pneumonia in the nursing home No disclosures or conflicts of interest PMHX: A. FIB. GERD MIXED DEMENTIA MMSE 16/30 HTN Mr. Hack 86 years old RAMIPRIL 4 MG OD PARIET 20MG OD DONEPEZIL
ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE
 ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE 2016 17 Melissa (Moe) Hagman, MD, FACP Associate Professor, Internal Medicine/Palliative Medicine mhagman@uw.edu SYNCOPE 72 year old otherwise
ARTICLES THAT HAVE CHANGED MY INPATIENT PRACTICE OF MEDICINE 2016 17 Melissa (Moe) Hagman, MD, FACP Associate Professor, Internal Medicine/Palliative Medicine mhagman@uw.edu SYNCOPE 72 year old otherwise
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part III: Measure updates and Abstraction Guidance Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital
 Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
Prospective audit and feedback of piperacillin-tazobactam use in a 1115 bed acute care hospital Final Results Nathan Beahm, BSP, PharmD(student) September 10, 2016 Objectives Review background information
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Atrial Fibrillation in the Elderly: Causes, Symptoms, and Treatment
 Atrial Fibrillation in the Elderly: Causes, Symptoms, and Treatment Asa Oxner, MD Assistant Professor of Medicine Division of General Internal Medicine University of South Florida Co-Investigator: Geriatric
Atrial Fibrillation in the Elderly: Causes, Symptoms, and Treatment Asa Oxner, MD Assistant Professor of Medicine Division of General Internal Medicine University of South Florida Co-Investigator: Geriatric
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
A Diagnostic Dilemma saved by sound
 A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
A Diagnostic Dilemma saved by sound Dr Syam Ravindranath MBBS DNB, Dr Ash Mukherjee FCEM FACEM We p r e s e n t a d i a g n o s t i c a l l y c h a l l e n g i n g s c e n a r i o in a 59 y e a r old f
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Chris Fox, MD Professor and Interim Chair Department of Emergency
 Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
Close Calls with the Executioner: Where POCUS Avoided Misdiagnosis Chris Fox, MD Professor and Interim Chair Department of Emergency Medicine En route with 22 year old female Asthma attack witnessed by
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Effectively Managing Sepsis Denials
 Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
Effectively Managing Sepsis Denials Krysten Brooks, RN, BSN, MBA Senior Inpatient Consultant 3M Health Information Systems This is the Full Title of a Session Atlanta, GA 1 Learning Objectives At the completion
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship
 New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship Mia A. Taormina, DO, FACOI Chair, Department of Infectious Disease, DuPage Medical Group Disclosures While product trade
New Antimicrobials and Rapid Diagnostics: Implications for Antibiotic Stewardship Mia A. Taormina, DO, FACOI Chair, Department of Infectious Disease, DuPage Medical Group Disclosures While product trade
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Objectives. Falling Down on Warfarin Therapy. CHADS 2 Score. CHADS 2 & CHA 2 DS 2 -VASc Score. HAS-BLED Score 04/08/2014. Real World Application
 Falling Down on Warfarin Therapy David Andrew Jacob, PharmD Pharmacy Resident 2013-2014 Dayton VA Medical Center Dayton, Ohio Objectives Describe CHADS 2 score and the decision to anticoagulate patients
Falling Down on Warfarin Therapy David Andrew Jacob, PharmD Pharmacy Resident 2013-2014 Dayton VA Medical Center Dayton, Ohio Objectives Describe CHADS 2 score and the decision to anticoagulate patients
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Inpatient Quality Reporting (IQR) Program
 Program") Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
Hypotension Inpatient Quality Reporting (IQR) Program SEP-1 Early Management Bundle, Severe Sepsis/ Septic Shock: v5.1 Measure Updates Questions and Answers Moderator: Candace Jackson, RN Project Lead,
A BRIEF HISTORY OF SEPSIS. Euan Mackay
 A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
Inpatient Internal Medicine Update A Patient-Centered Review of the Literature
 Inpatient Internal Medicine Update A Patient-Centered Review of the Literature A. Scott Keller October 28, 2016 2010 MFMER slide-1 Disclosures Certain images and/or photos are the copyrighted property
Inpatient Internal Medicine Update A Patient-Centered Review of the Literature A. Scott Keller October 28, 2016 2010 MFMER slide-1 Disclosures Certain images and/or photos are the copyrighted property
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Atrial Fibrillation is Common. ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat. Incidence of Atrial Fibrillation by Age
 ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
10/27/13. Update in Hospital Medicine Update in Hospital Medicine Update in Hospital Medicine 2013
 2013 Brad Sharpe, MD, SFHM, FACP UCSF Division of Hospital Medicine Michelle Mourad, MD, SFHM, FACP UCSF Division of Hospital Medicine 2013 Updated literature March 2012 March 2013 Process: CME collaborative
2013 Brad Sharpe, MD, SFHM, FACP UCSF Division of Hospital Medicine Michelle Mourad, MD, SFHM, FACP UCSF Division of Hospital Medicine 2013 Updated literature March 2012 March 2013 Process: CME collaborative
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Urinary Tract Infections in Hospitalized Patients
 Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Urinary Tract Infections in Hospitalized Patients Puerto Rico Chapter Annual Meeting Daniel C. DeSimone, MD March 9, 2019 2017 MFMER slide-1 Disclosures for speaker: Date of presentation: 3/9/2019 No relevant
Management of Atrial Fibrillation. Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018
 Management of Atrial Fibrillation Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018 Disclosures Speaker: St. Jude Medical, Biotronik Consultant: St. Jude Medical, World Care Clinical Objectives Recognize
Management of Atrial Fibrillation Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018 Disclosures Speaker: St. Jude Medical, Biotronik Consultant: St. Jude Medical, World Care Clinical Objectives Recognize
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
NEWLY DETECTED ATRIAL FIBRILLATION. Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology
 NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
NEWLY DETECTED ATRIAL FIBRILLATION Edgar S. Carell, M.D. Director, Vascular Medicine Clinic West Suburban Cardiology 68 y/o woman complains of - generalized fatigue - mild DOE - never eats but keeps gaining
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Sepsis as Seen by the CMO. Randy C. Roth, MD Chief Medical Officer
 Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Sepsis as Seen by the CMO Randy C. Roth, MD Chief Medical Officer 1 Challenges of Sepsis Sepsis, like many disease processes, is much more than a clinical challenge. For Hospitalists, we are treating the
Update in Outpatient Medicine ACP Scientific Session November 12, 2016
 Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
How do we define pneumonia?
 Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Robert L. Keith MD FCCP Associate Professor of Medicine Division of Pulmonary Sciences & Critical Care Medicine Denver VA Medical Center University of Colorado Denver How do we define pneumonia? Fever
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc
 Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures