BASIC CRITICAL CARE OF THE PATIENT. Hannelisa Callisen PA C February 2017
|
|
|
- Clarence Walton
- 6 years ago
- Views:
Transcription
1 BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017
2 Disclosures Industry: None ECMO is off label
3 Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO Monitoring on ECMO Bedside management of the ECMO patient Complications 2 ICU patients
4 FIRST.. WHAT IS ECMO? Image credit: S. Conrad

5 42F to ED w/ SOB PMH: Obesity, Pre diabetes Admitted last night for acute hypoxic respiratory failure Intubated, paralyzed On low dose pressors BAL: +H1N1 PIP 40 Vt 210 PEEP 14 RR 32 ABG ph 7.15 paco2 66 pao2 52 SaO2 76 HCO3 19
6 To Cannulate? CURRENT SITUATION: ARDS w/ significant hypercapnia & hypoxia affecting DO2 and end organ function, on maximal vent settings Does she meet criteria? When is the right time to cannulate? What is the likelihood of recovery? PIP 40 Vt 210 PEEP 12 RR 32 ABG ph 7.15 paco2 66 pao2 52 SaO2 76 HCO3 19
7 To Cannulate? SELECTION CRITERIA
8 To Cannulate? SELECTION CRITERIA? Are these specific gas exchange parameters useful?why 7 days of aggressive ventilation?how definite are these contraindications Brodie NEJM 2011
9 To Cannulate? INDICATIONS? Are these specific gas exchange parameters useful GENERAL CRITERIA: Reversible (or transplantable) disease Refractory to maximal conventional therapy High risk of mortality


10 To Cannulate? TIMING TO ECMO?Why 7 days of aggressive ventilation Timing to cannulation / transfer is difficult to discern Trajectory of illness is most important factor Ferguson ND ICM 2012 Rescue therapies for ARDS Moerer. Curr Opin 2016
11 To Cannulate? TIMING TO ECMO?Why 7 days of aggressive ventilation Domico M, Ped Crit Care Med 2012 Nance, J of Ped Surg 2009

12 To Cannulate? CONTRAINDICATIONS?How definite are these contraindications ECMO IS A BRIDGE THERAPY Goal: Buy time for disease process to resolve Avoid injury from other therapies Consider end point & ability to recover and overcome potential complications of ECMO therapy (early) ELSO Guidelines for acute resp failure
13 To Cannulate? PRE ECMO PREDICTORS RESP Score ECMOnet Score Pre ECMO SOFA Score?helpful
14 Rationale for VV ECMO ARDS continues to have high mortality VILI may develop and worsen lung disease ECMO: Puts less dependence on ventilator, reduces transpulmonary pressures Allows DO2 and VO2 to be better controlled and manipulated (even if SaO2 NOT improved) May improve hemodynamics & CO
15 RATIONALE FOR ECMO Improve Cellular Oxygenation DO2 normally 4 5 times that of VO2 Resting VO2: 3 5mL/kg/min for adults DO2 (ml/min) = CO (L/min) x CaO2 (ml O2 / L blood) [1.34 Hgb SaO2] + [0.003 PaO2] OER = VO2 / DO2 [Normal~25%] CO (L/min) x CaO2 CvO2 (ml O2 / L blood) = VO2 (ml/min) Cells determined by tissue metabolic rate
16 RATIONALE FOR ECMO Improve Cellular Oxygenation DO2 normally 4 5 times that of VO2 Resting VO2: 3 5mL/kg/min for adults OER = VO2 / DO2 [Normal~25%] If DO2:VO2 is < 2:1 Anaerobic Metabolism ILLNESS SvO2 < 50 60% DO2crit ~4mL/kg/min Monitoring DO2 in the crit ill Huang. Chest 2005 O2 delivery and consumption, macrocirc perpective Nichols. Crit Care Clin 2010

17 VV ECMO NO cardiac support NO in pulmonary blood flow Configura on Usually PARTIAL pulmonary support Based on ECBF : CO Ratio ECMO flow Venous Admixture Outlet / Return Native Lung Function Recirculation Patient Cardiac Output VV perfusate mixes with mixed venous blood return, bypassed by ECMO Venous Admixture Inlet / Drainage Venous Return mixed Cells Bypassed Venous Flow

18 VV ECMO Cannulation SINGLE SITE CANNULATION DUAL SITE CANNULATION ECMO in CP disease in adults Abrams. JACC 2014



19 ECMO CIRCUIT Cannula Biggest, shortest cannula = least resistance to flow Appropriate cannula selection is critical! ECMO for adult resp failure Turner. Resp Care 2013
20 ECMO CIRCUIT Tubing PVC TUBING Neonates: 1/4 inch Peds: 3/8 inch Adults: 3/8 1/2 inch TUBING SIZE SV (ml/rpm) PRIME VOLUME MAX ART FLOW MAX VEN FLOW 1/4 inch 13ml 9.65ml/ft 3 LPM 1.3 LPM 3/8 inch 27ml 21.71ml/ft 8 LPM 4 :PM Biocompatible surface coating
 Flow RPM Impeller design Magnetically coupled to motor NO Direct relationship between RPM and Flow Flowmeter is")
21 ECMO CIRCUIT Pump CENTRIFUGAL PUMP Non occlusive pump Pre load sensitive Afterload dependent (must overcome positive resistance) Flow RPM Impeller design Magnetically coupled to motor NO Direct relationship between RPM and Flow Flowmeter is necessary


22 ECMO CIRCUIT Oxygenator MICROPOUROUS HOLLOW FIBER Polymethylpentene Gas inside fibers, blood on outside Low pressure drop across membrane Very small nano pore size Rare plasma leakage High gas permeability Rated flow Maquet.com
23 ECMO CIRCUIT Heat Exchanger Integrated in hollow fiber membrane lungs External water bath warms blood Bath temp usually set C above 37 C
 Connects to 30 70PSI inlet Air Gas flow = Sweep 2 dials 0 10")
24 ECMO CIRCUIT Gas Blender Connected to oxygenator Mixes air and oxygen O2 Dial for FiO2 (0 100%) Connects to 30 70PSI inlet Air Gas flow = Sweep 2 dials 0 10 LPM

25 Cannulated for VV ECMO using fem fem approach Sedated, paralyzed 42F w/ ARDS on VV ECMO ABG BP: 78/50 (60) on Norepinephrine HR: 100 CVP: 16 SWEEP FiO2 ph 7.29 paco2 42 pao2 59 SaO2 88 HCO3 17 Lactate 4.1 FLOW: RPM:
26 42F w/ ARDS on VV ECMO What is most concerning? What are we missing here? What do we address first? vent?? ABG BP: 78/50 (60) on Norepinephrine HR: 100 CVP: 16 SWEEP FiO2 ph 7.29 paco2 42 pao2 58 SaO2 87 HCO3 17 Lactate 4.1 FLOW: RPM:

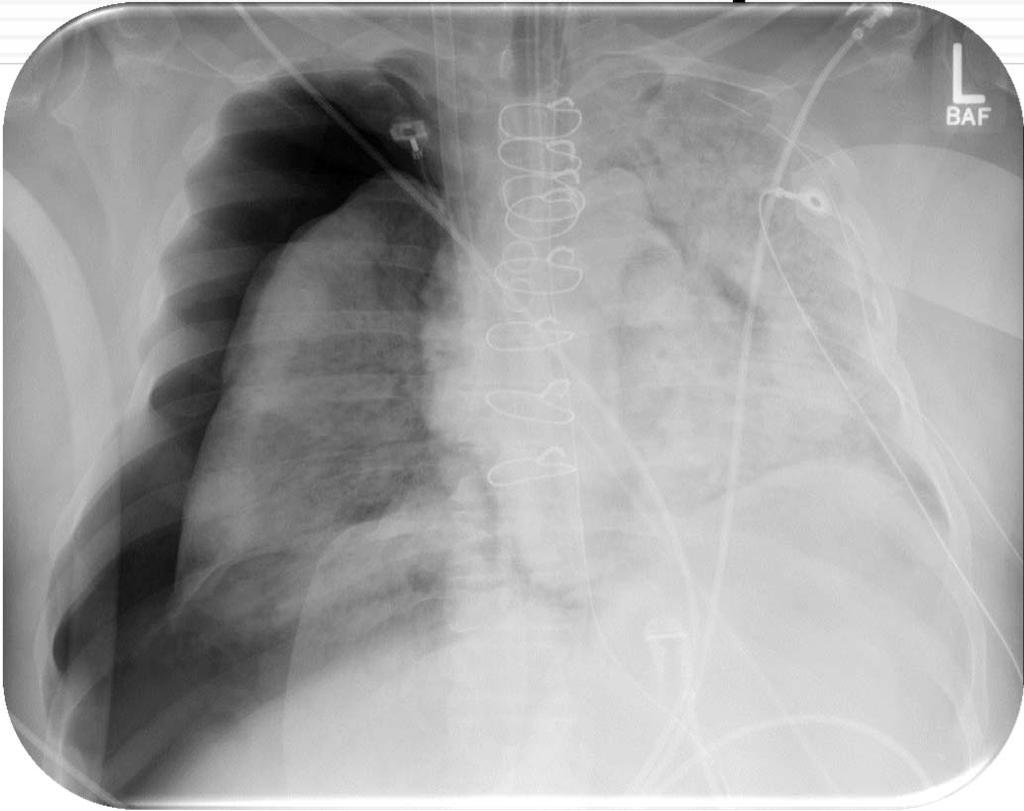
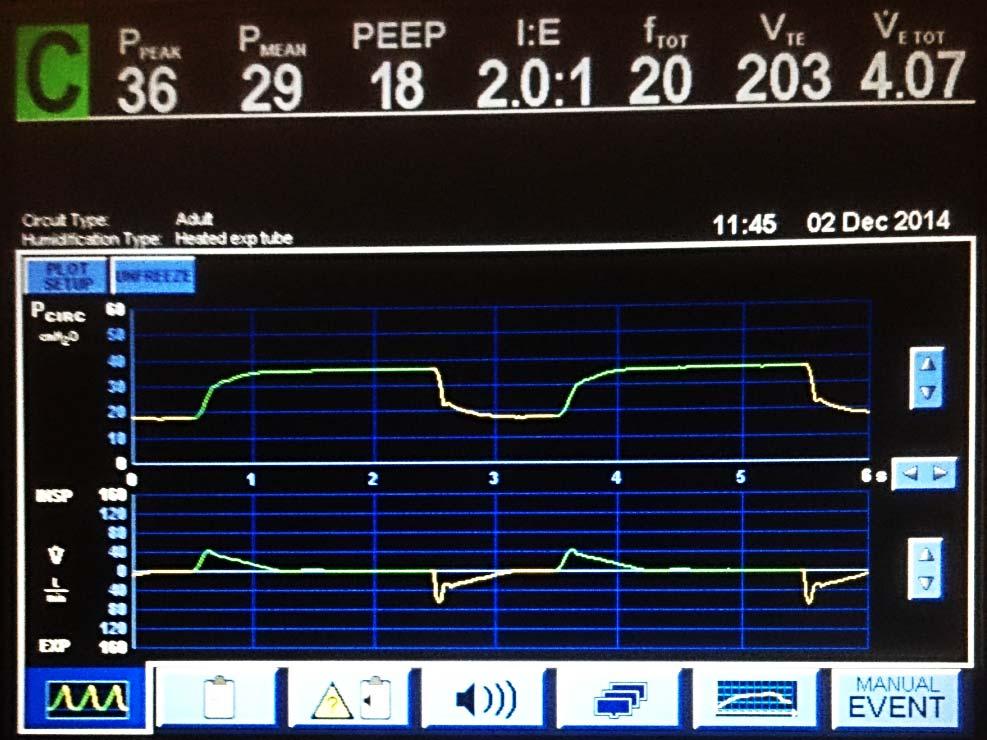
27 42F w/ ARDS on VV ECMO
28 PATIENT A B C Vitals / Pressures / Waveforms SpO2 RR HR BP CVP Physical Exam IMAGING MEDS LABS CO VO2 CANNULAS TUBING FLOWS PRESSURES OXYGEN ATOR PUMP CaO2 ECMO VENTILATOR INTERACTION GAS EXCHANGE FiO 2 PEEP RR V T PIP

29 Oxygen Delivery ON VV ECMO DO2 = CaO2 CO native cardiac function



30 VV Air/O2 Blender MO V A Motor Pump S inlet O2 MO FiO2 MO Dynamics Blood Flow Rate membrane oxygenated blood For Best Ratio: Effec ve ECBF Recircula on CO true S V O2 Lung Function Ventilator Settings lung oxygenated blood
31 Blood Viscosity Blender / O2 Blood Flow : CO Ratio?OK OK MO Dynamics Membrane thickness Membrane Surface Area Diffusion capacity OK OK Lung Function MINIMAL, but that is OK! True SvO2 LOW: due to shock, VO2 Recirculation Fraction HIGH: Due to PTX Cells Oxygen Delivery Adequate CO NO: Obstructive shock due to PTX & high PIP Hemoglobin?OK NEEDS CHEST TUBE!
32 Mechanical Ventilation ON VV ECMO

33 38M w/ NIMCP Code Blue PEA ARREST Admitted 1 day ago w/ decompensated HF Hx of dilated CMP (non ischemic, previous viral) CPR ROSC Ends up on high dose inotropes Hypoxic & Acidemic ABG ph 7.20 paco2 36 pao2 50 SaO2 86 HCO3 12 Lactate 11? VA ECMO
34 38M w/ NIMCP Code Blue? VA ECMO INDICATIONS CONTRAINDICATIONS CONSIDERATIONS

35 38M w/ NIMCP Code Blue ECMO in CP disease in adults Abrams. JACC 2014
36 Outcomes FOR VA ECMO
 Mixture of ECLS perfusate and natively oxygenated blood in aorta Venous Return mixed Mixing Cloud")
37 VA ECMO Configura on Inlet / Drainage in pulmonary blood flow ECMO flow Outlet / Return Cardiac bypass support (partial to sub total) Total CO = Native CO + ECBF Native Lung Function Native Cardiac Output Arterial oxygenation: Dependent on sample location (in relation to mixing cloud) Mixture of ECLS perfusate and natively oxygenated blood in aorta Venous Return mixed Mixing Cloud Cells

38 VA ECMO Peripheral Cannulation ECMO in CP disease in adults Abrams. JACC 2014



39 DO2 = C Nat O2 CO Nat + C ECMO O2 ECBF VA V A S V O2 Lung Function Ventilator Settings lung oxygenated blood Ratio Native CO : ECBF membrane oxygenated blood S V O2 MO FiO2 MO Dynamics Native CO + ECBF
40 38M w/ Card Shock on VA ECMO What to do with inotropes? How to approach hypoxia? What is an acceptable SaO2? How to manage ventilator?

41 38M w/ Card Shock on VA ECMO With most inotropes off:
42 LV Distention ON PERIPHERAL VA ECMO Risk of LV thrombosis Pulmonary Edema LV Failure
43 CHEST TUBE now in place 42F w/ ARDS on VV ECMO BP: 110/50(70) HR: 120 CVP: 11 SaO2: 83% What SaO2 is acceptable? If DO2 inadequate, how can it be improved?


44 Lung Function Oxygen Delivery Adequate CO Blood Flow : CO Ratio Hemoglobin Blood Viscosity Blender / O2 MO Dynamics Membrane thickness Membrane Surface Area Diffusion capacity True SvO2 Recirculation Fraction Cells
45 VV ECBF DETERMINANTS AND LIMITATIONS Effective

46 Recirculation CAUSES 1. RPM 2. Cannula Positioning 3. Venous Chamber Compliance 4. Low CO
47 38M w/ Card Shock on VA ECMO Inotropes increased to arterial pulsatility (native CO) Ventilator Settings decreased (FiO2 50%, PEEP 5) BP: 72/60 (64) SaO2: 80%

48 Differential Hypoxia ON PERIPHERAL VA ECMO C. Lotz Circulation 2014



49 VV & VA side by side IN SERIES Cells Cells IN PARALLEL
50 Complications, Considerations Bleeding, Hemolysis, Thrombosis Renal Failure Pharmacy Neurocognitive Limb perfusion Nursing care Team Cost
51 Complications, Considerations Lim ECLS physiological concepts and clinical outcomes. J of Card Failure 2016
52 Final Thoughts ECMO: Physiology is complex! Needs meticulous consideration of risks, potential for recovery (or transplant), & co morbidities Is resource intensive & costly Best practiced at experienced, high volume centers w/ well trained team members (that means everyone involved)



53 PATIENT A B C Vitals / Pressures / Waveforms SpO2 RR HR BP CVP Physical Exam IMAGING MEDS LABS CO VO2 CANNULAS TUBING FLOWS PRESSURES OXYGEN ATOR PUMP CaO2 ECMO VENTILATOR INTERACTION GAS EXCHANGE FiO 2 PEEP RR V T PIP
54 THANK YOU
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
FOCUS CONFERENCE 2018
 FOCUS CONFERENCE 2018 Current Practice in Pediatric and Neonatal Extracorporeal Life Support Daniel W. Chipman, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
FOCUS CONFERENCE 2018 Current Practice in Pediatric and Neonatal Extracorporeal Life Support Daniel W. Chipman, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECLS. The Basics. Jeannine Hermens Intensive Care Center UMC Utrecht
 ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
ECLS The Basics Jeannine Hermens Intensive Care Center UMC Utrecht Conflict of interest None Terminology ECMO - ExtraCorporeal Membrane Oxygenation ECLS - ExtraCorporeal Life Support PLS - Veno-venous
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ECMO as a bridge to durable LVAD therapy. Jonathan Haft, MD Department of Cardiac Surgery University of Michigan
 ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
ECMO as a bridge to durable LVAD therapy Jonathan Haft, MD Department of Cardiac Surgery University of Michigan Systolic Heart Failure Prevalence 4.8 million U.S. 287,000 deaths per year $39 billion spent
Healing Breath. Disclosures. anuola. Extracorporeal Membrane Oxygenation Principles: Rest your lungs. Objectives ECMO: 8/28/17
 anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
anuola Healing Breath ECMO Program of Hawaii Extracorporeal Membrane Oxygenation Principles: Rest your lungs Len Y. Tanaka, MD September 12, 2017 Disclosures No financial disclosures. However this presentation
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care
 Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
Lesta Whalen, MD Medical Director, Sanford ECMO Pediatric Critical Care Disclosures I have no financial disclosures. The use of certain devises for providing long-term cardiopulmonary support is investigational.
ECMO for Refractory Septic Shock Prof. Alain Combes
 ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
ECMO for Refractory Septic Shock Prof. Alain Combes Service de Réanimation ican, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris
Extra Corporeal Life Support for Acute Heart failure
 Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
Extra Corporeal Life Support for Acute Heart failure Benjamin Medalion, MD Director Heart and Lung Transplantation Department of Cardiothoracic Surgery Rabin Medical Center, Beilinson Campus, Israel Mechanical
ECMO Experience from ECMO-ICU, Karolinska
 ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
EXTRA CORPOREAL MEMBRANE OXYGENATION
 EXTRA CORPOREAL MEMBRANE OXYGENATION Basic Overview and Case Study Bob Hayes, Chief Perfusionist Enloe Medical Center Jenny Humphries, RN, BSN, MBA, CFRN Chief Flight Nurse, Enloe FlightCare Normal Cardiopulmonary
EXTRA CORPOREAL MEMBRANE OXYGENATION Basic Overview and Case Study Bob Hayes, Chief Perfusionist Enloe Medical Center Jenny Humphries, RN, BSN, MBA, CFRN Chief Flight Nurse, Enloe FlightCare Normal Cardiopulmonary
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know!
: What Every Pharmacist Needs to Know!") Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Mechanical Circulatory Support (MCS): What Every Pharmacist Needs to Know! Matthew A. Wanat, PharmD, BCPS, BCCCP, FCCM Clinical Assistant Professor University of Houston College of Pharmacy Clinical Pharmacy
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ECMO CPR. Ravi R. Thiagarajan MBBS, MPH. Cardiac Intensive Care Unit
 ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECMO for cardiac arrest patients: Update 2017
 ECMO for cardiac arrest patients: Update 2017 Lim Swee Han MBBS (NUS), FRCS Ed (A&E), FRCP (Edin), FAMS Senior Consultant, Department of Emergency Medicine, Singapore General Hospital Adjunct Associate
ECMO for cardiac arrest patients: Update 2017 Lim Swee Han MBBS (NUS), FRCS Ed (A&E), FRCP (Edin), FAMS Senior Consultant, Department of Emergency Medicine, Singapore General Hospital Adjunct Associate
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
ECMO Primer A View to the Future
 ECMO Primer A View to the Future Todd J. Kilbaugh Assistant Professor of Anesthesiology, Critical Care Medicine, and Pediatrics Director of The ECMO Center at the Children s Hospital of Philadelphia Disclosures
ECMO Primer A View to the Future Todd J. Kilbaugh Assistant Professor of Anesthesiology, Critical Care Medicine, and Pediatrics Director of The ECMO Center at the Children s Hospital of Philadelphia Disclosures
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Cardiopulmonary System
 Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
Dana Oakes, BA, RRT NPS Author/Speaker Cardiopulmonary System Main Purpose Main Function Main Goal Oxygen Delivery Adequate Perfusion (deliver adequate oxygen and nutrients; remove metabolic waste) Tissue
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
Artificial Lung: A New Inspiration
 Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome
 CASE REPORT Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome Wen-Je Ko,* Hsao-Hsun Hsu, Pi-Ru Tsai When all conventional treatments for respiratory failure
CASE REPORT Prolonged Extracorporeal Membrane Oxygenation Support for Acute Respiratory Distress Syndrome Wen-Je Ko,* Hsao-Hsun Hsu, Pi-Ru Tsai When all conventional treatments for respiratory failure
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
CPB pump flow, and effective Flow in patient. 1
 Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
LV Distension and ECLS Lungs
 LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
LV Distension and ECLS Lungs Kevin W. Hatton, MD, FCCM Interim Vice-Chair for Anesthesiology Research Division Chief, Anesthesiology Critical Care Medicine Program Director, Anesthesiology Critical Care
ISPUB.COM. Concepts Of Neonatal ECMO. D Thakar, A Sinha, O Wenker HISTORY PATIENT SELECTION AND ECMO CRITERIA
 ISPUB.COM The Internet Journal of Emergency and Intensive Care Medicine Volume 5 Number 2 D Thakar, A Sinha, O Wenker Citation D Thakar, A Sinha, O Wenker.. The Internet Journal of Emergency and Intensive
ISPUB.COM The Internet Journal of Emergency and Intensive Care Medicine Volume 5 Number 2 D Thakar, A Sinha, O Wenker Citation D Thakar, A Sinha, O Wenker.. The Internet Journal of Emergency and Intensive
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC.
 PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
PATIENT SELECTION FOR ACUTE APPLICATION OF ECMO, ECCOR, ETC. J. CHRISTOPHER FARMER, MD PROFESSOR OF MEDICINE CHAIR OF CRITICAL CARE MEDICINE MAYO CLINIC PHOENIX, AZ Dr. Chris Farmer is a critical care
Bridging With Percutaneous Devices: Tandem Heart and Impella
 Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Bridging With Percutaneous Devices: Tandem Heart and Impella DAVID A. BARAN, MD, FACC, FSCAI SYSTEM DIRECTOR, ADVANCED HEART FAILURE, TX AND MCS SENTARA HEART HOSPITAL NORFOLK, VA PROFESSOR OF MEDICINE
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Cardiovascular Institute
 Allegheny Health Network Cardiovascular Institute Extracorporeal Membrane Oxygenation (ECMO) Program Our patient survival rate is higher than the national average. ECMO experts. Multidisciplinary team.
Allegheny Health Network Cardiovascular Institute Extracorporeal Membrane Oxygenation (ECMO) Program Our patient survival rate is higher than the national average. ECMO experts. Multidisciplinary team.
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Management of Cardiogenic Shock. Dr Stephen Pettit, Consultant Cardiologist
 Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Dr Stephen Pettit, Consultant Cardiologist Cardiogenic shock Management of Cardiogenic Shock Outline Definition, INTERMACS classification Medical management of cardiogenic shock PA catheters and haemodynamic
Echo assessment of patients with an ECMO device
 Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Echo assessment of patients with an ECMO device Evangelos Leontiadis Cardiologist 1st Cardiology Dept. Onassis Cardiac Surgery Center Athens, Greece Gibbon HLM 1953 Goldstein DJ et al, NEJM 1998; 339:1522
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
ECCO 2 Removal The Perfusionists Perspective
 ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
DO 2 > VO 2. The amount of oxygen delivered is a product of cardiac output (L/min) and the amount of oxygen in the arterial blood (ml/dl).
 and the amount of oxygen in the arterial blood (ml/dl).") Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Epidemiology of Heart Failure in Adults
 Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Cardiac Critical Care : Focused on IABP & PCPS Epidemiology of Heart Failure in Adults Prevalence Incidence Mortality 2004 Hospital Cost 2007 2004 Age 20+ (New Cases) All Ages Discharges Age 35+ 2004 All
Extracorporeal support in acute respiratory failure. Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London
 Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
The Role of ECMO in Thoracic Surgery. Matthew Hartwig, MD
 The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
The Role of ECMO in Thoracic Surgery Matthew Hartwig, MD Disclosure Slide Consultant for Mallincrodkt and Quark Pharmaceuticals Case #1 28 y.o. female with tracheal mass No previous medical or surgical
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
Mechanics of Cath Lab Support Devices
 Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Mechanics of Cath Lab Support Devices Issam D. Moussa, MD Chief Medical Officer First Coast Cardiovascular Institute, Jacksonville, FL Professor of Medicine, UCF, Orlando, FL None DISCLOSURE Percutaneous
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation
 as a Bridge to Decision in Lung Transplantation") Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
to optimize By Jin Xiong Lian, BSN, RN, CNS
 Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Goal Directed Perfusion: theory, clinical results, and key rules
 Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Management of Acute Shock and Right Ventricular Failure
 Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
Management of Acute Shock and Right Ventricular Failure Nader Moazami, MD Department of Thoracic and Cardiovascular Surgery and Biomedical Engineering, Cleveland Clinic NONE Disclosures CARDIOGENIC SHOCK
ECMO vs. CPB for Intraoperative Support: How do you Choose?
 ECMO vs. CPB for Intraoperative Support: How do you Choose? Shaf Keshavjee MD MSc FRCSC FACS Director, Toronto Lung Transplant Program Surgeon-in-Chief, University Health Network James Wallace McCutcheon
ECMO vs. CPB for Intraoperative Support: How do you Choose? Shaf Keshavjee MD MSc FRCSC FACS Director, Toronto Lung Transplant Program Surgeon-in-Chief, University Health Network James Wallace McCutcheon
Management of Respiratory Failure: The Surgical Perspective. When Traditional Respiratory Support Techniques fail. ARDS: Evidence Based Practice
 Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
Critical Care Medicine and Trauma Management of Respiratory Failure: The Surgical Perspective Jasleen Kukreja, M.D. Division of Cardiothoracic Surgery University of California San Francisco When Traditional
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
Extracorporeal Life Support Organization (ELSO) General Guidelines for all ECLS Cases August, 2017
 General Guidelines for all ECLS Cases August, 2017") Extracorporeal Life Support Organization (ELSO) Introduction General Guidelines for all ECLS Cases August, 2017 This guideline describes prolonged extracorporeal life support (ECLS, ECMO), applicable to
Extracorporeal Life Support Organization (ELSO) Introduction General Guidelines for all ECLS Cases August, 2017 This guideline describes prolonged extracorporeal life support (ECLS, ECMO), applicable to
Associated clinical guidelines/protocols: Comprehensive GOSH ECMO guidelines are available in the ECMO office.
 Disclaimer: The Great Ormond Street Paediatric Intensive Care Training Programme was developed in 2004 by the clinicians of that Institution, primarily for use within Great Ormond Street Hospital and the
Disclaimer: The Great Ormond Street Paediatric Intensive Care Training Programme was developed in 2004 by the clinicians of that Institution, primarily for use within Great Ormond Street Hospital and the
Permissive hypoxaemia. Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK
 Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Which mechanical assistance for cardiogenic shock?
 Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
Which mechanical assistance for cardiogenic shock? Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre et Marie Curie Sorbonne
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure August, 2017
 Guidelines for Adult Respiratory Failure August, 2017") Introduction Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure August, 2017 This guideline describes prolonged extracorporeal life support (ECLS, ECMO), applicable
Introduction Extracorporeal Life Support Organization (ELSO) Guidelines for Adult Respiratory Failure August, 2017 This guideline describes prolonged extracorporeal life support (ECLS, ECMO), applicable
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the PreSep oximetry catheter for continuous central venous oximetry (ScvO 2 ) 3 The Vigileo
Beyond the Golden Hour: Caring for the ICU Boarder
 Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Anesthetic Management of the Patient on Veno-Venous ECMO Who Requires Emergent Surgery Michael A. Fierro, M.D. Duke University, Durham, NC
 Session: L233 Session: L441 Anesthetic Management of the Patient on Veno-Venous ECMO Who Requires Emergent Surgery Michael A. Fierro, M.D. Duke University, Durham, NC Disclosures: This presenter has no
Session: L233 Session: L441 Anesthetic Management of the Patient on Veno-Venous ECMO Who Requires Emergent Surgery Michael A. Fierro, M.D. Duke University, Durham, NC Disclosures: This presenter has no
E-CPR National Trends & Local Plans
 E-CPR National Trends & Local Plans Objectives What is E-CPR? Jon Marinaro MD FCCM Chief, Surgical Critical Care UNM Associate Director UNM Adult ECMO Program Why would one do it? Evidence behind E-CPR?
E-CPR National Trends & Local Plans Objectives What is E-CPR? Jon Marinaro MD FCCM Chief, Surgical Critical Care UNM Associate Director UNM Adult ECMO Program Why would one do it? Evidence behind E-CPR?
E-CPR National Trends & Local Plans
 E-CPR National Trends & Local Plans Jon Marinaro MD FCCM Chief, Surgical Critical Care UNM Associate Director UNM Adult ECMO Program Objectives What is E-CPR? Why would one do it? Evidence behind E-CPR?
E-CPR National Trends & Local Plans Jon Marinaro MD FCCM Chief, Surgical Critical Care UNM Associate Director UNM Adult ECMO Program Objectives What is E-CPR? Why would one do it? Evidence behind E-CPR?