Management of Endoleaks. Michael Meuse, M.D Vascular and Interventional Radiology 12/14/09
|
|
|
- Ambrose Wells
- 6 years ago
- Views:
Transcription

1 Management of Endoleaks Michael Meuse, M.D Vascular and Interventional Radiology 12/14/09
2 Endoleak Failure to totally exclude the abdominal aortic aneurysm (AAA) from continued perfusion and pressurization
3 Demographics The reported incidence of endoleaks ranges from 15% to 25% within 30 days postoperatively. In a report from the EUROSTAR registry, the incidence of early endoleak was 18%. Sixty nine percent of these leaks were graft related. Seventy percent sealed spontaneously during the first 6 months without a difference between graft-related and non-graft-related endoleaks.

4 Endoleak types Type I endoleak Proximal or distal attachment Type II endoleak Retrograde branch flow Type III endoleak Structural defect or component junction Type IV endoleak Trans graft leakage or porosity
5 Endoleak Sub- Classification

6 Type I Endoleak Type I endoleak is caused by failure to achieve a circumferential seal at either the proximal (Type IA) or distal end (Type IB) of the stentgraft. Type IC endoleak is due to non-occluded iliac artery in patients with aorto-mono-iliac stent and femoral-femoral bypass. With Type I endoleak, the aneurysm is perfused directly from the aorta or the iliac arteries.
7 Type I Endoleak The overall incidence is 4.2% at 30 days, 3.5% within 1 year and 6.7% beyond 1 year The leak usually communicates through a channel (sometimes multiple channels) with the aneurysmal sac. There are several outflow vessels, mainly lumbar arteries and inferior mesenteric artery (IMA) that communicate with the channel and or the sac. The pressure within a Type I leak is systemic. The tension on the aortic wall remains high.
8 Type I Endoleak Causes of primary Type I endoleak include: Inappropriate anatomy, with a significantly angulated neck or conical neck Significant calcification/plaque at the proximal or distal landing zone A non-circular landing zone Malpositioning of the stent-graft Type of endograft Under-dilation of the stent-graft.
9 Type I Endoleak Secondary Type I endoleak can be due to: Aneurysm re-modeling, resulting in stent-graft migration Progressive dilatation of the proximal neck Design and dimensions of stent-grafts or unfavorable infrarenal necks, including the conically shaped neck and neck shorter than 15 mm. Grafts whose fixation relies on radial force have been reported to be more prone to caudal migration and Type I endoleak than grafts with hooks. Endothelialization of bare stents at the landing zones may contribute to a certain fixation, but endothelialization of the fabric itself does not happen.
10 Type I Endoleak Proximal bare stent separation and hook fractures are also causes of delayed Type I endoleak. Oversizing the graft by 20% is recommended to prevent a delayed endoleak. At the iliac level, Type IB endoleak occurs when the limb of the graft is too short or migrates upward due to the sac s retraction pressure and aortic distortion.
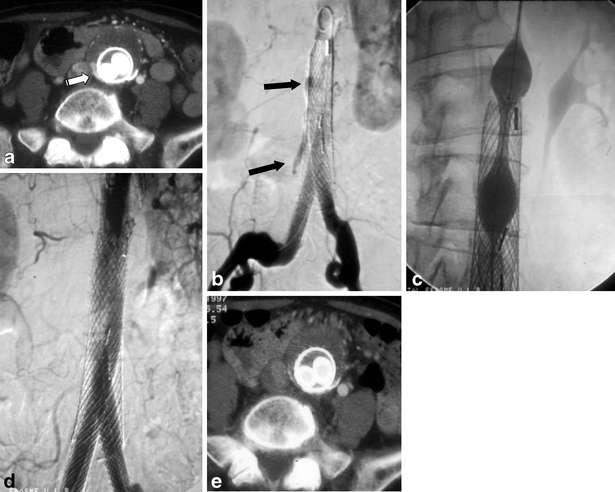
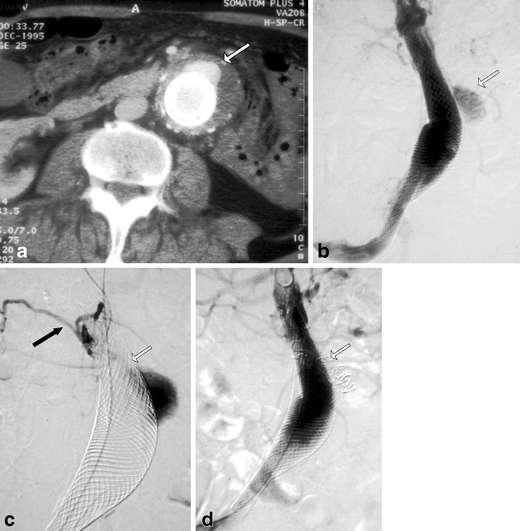
11 Treatment of Type I-A Endoleak If a Type I leak is present at the time of graft placement, it must be immediately treated because the aneurysm sac is exposed to systemic pressure. Placement of a proximal cuff or extension endograft is the most commonly used treatment in the case of a proximal endoleak associated with malpositioning, angulated neck or migration. This technique is not always feasible due to different anatomical and technical challenges. In the case of a proximal endoleak associated with an irregular neck with no migration, simple balloon angioplasty with large balloons (25 30 mm) or large Palmaz stent placement could be sufficient to apply the stent-graft to the aortic wall.

12
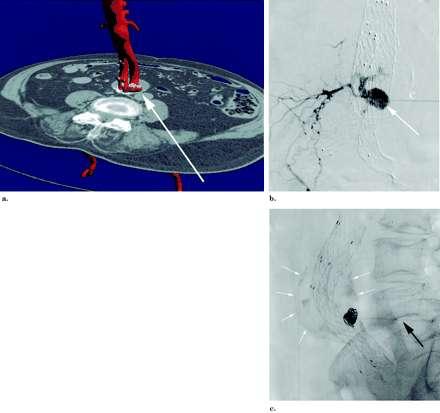
13 Embolization of Type I-A Endoleak Embolization and coiling of the aneurysmal sac and the outflow vessels has been proposed as an alternative treatment for Type I endoleak in selected patients The majority of patients treated with this technique had extensive medical co-morbidities and short or highly angulated proximal neck. Golzarian et al. described 32 patients with Type I endoleak. Embolization was successful in 29 patients with the occlusion of the outflow vessels and the aortic channel and/or sac. Three patients with large neck had persistent endoleak after several procedures. None of the patients with successful embolization developed a new endoleak or an aneurysmal expansion
14
15
16 Type I-B endoleak All treatment options for the Type IA endoleaks are valid for distal endoleak. In case of short landing or enlarged iliac artery, an extension endograft will be necessary. Occasionally Type I-B endoleaks can be treated with balloon angioplasty or bare stent implantation, allowing the sealing of the stent graft to the aortic wall. If the origin of internal iliac artery needs to be covered, it should be embolized to prevent from retrograde leak. Embolization of the sac or the channel, although feasible, is usually not indicated in Type I-B endoleak.

17 Type I-B Repair
18 Type II Endoleak The most common endoleak, Type II is the retrograde filling of the aneurysm mainly from lumbar arteries and/or IMA but also in rare situations from sacral, gonadal or accessory renal arteries. The overall incidence is 10.5%. In some series, up to 18.9% of individuals had a type II endoleak at one year.
19 Type II Endoleak Type II endoleaks can be associated with aneurysmal expansion and rupture; however, this risk is much less than with the Type I and III endoleaks (0.5 versus 3.4 %). A leak in the setting of a shrinking aneurysm can generally be followed, without immediate intervention. It is well established that up to 40% of Type II endoleaks will seal spontaneously. Some have advocated intervening in all endoleaks persisting beyond 3 6 months, while other groups recommended observing leaks in the absence of aneurysm expansion.

20 Type II Endoleak
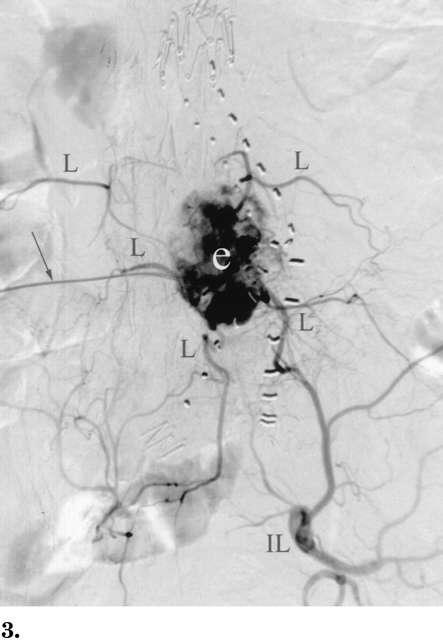
21 Treatment of Type II Endoleak Persistent Type II endoleaks usually have a complex architecture. They have been compared with an arteriovenous malformation, with the sac forming the nidus of the lesion. There are usually multiple inflow and outflow vessels. These vessels communicate through a channel. The channel is different from the endoleak sac that is generally seen during the angiogram and punctured in translumbar embolization. To achieve a successful embolization, the inflow vessels and the channel(s) need to be embolized. Like in embolization of Type I endoleak, the key is to disrupt the communications between the vessels involved in the leak
22 Treatment of Type II Endoleak There are two main approaches to embolize the patent feeding vascular branches. One is a transarterial and the other is a direct translumbar endoleak puncture. Using the trans-arterial approach, the aneurysmal sac can be access through the Inferior mesenteric artery (IMA) and lumbar arteries. Embolization of a patent lumbar artery can be performed by super selective catheterization of the iliolumbar and lumbar arteries. For IMA embolization, it can be performed retrogradely by superselective catheterization, with a microcatheter, to the superior mesenteric artery, the middle colic artery and arch of Riolan and marginal artery into the IMA. Coil embolization is the most common technique.

23 Arc of Riolan Channel between ingress and egress
24 Treatment of Type II Endoleak The other alternative for intervention is translumbar approach, in which careful correlation with prior CT helps to plan the puncture site in relation to stent graft. Using CT or fluoroscopic guidance, the access needle is aimed at direct puncture of the aneurysm sac to inject onyx or thrombin.
25 Direct translumbar endoleak puncture 19-gauge, 20-cm needle with a 5-F Teflon sheath Translumbar catheter can be used to take pressure measurements and to embolize the endoleak. Can be used to select the inferior mesenteric artery for embolization Embolization should continue until there is no further blood return and a static column of contrast is seen on a follow-up angiogram of the aneurysm sac. The most commonly used embolic agents are stainless steel or platinum coils Safe to traverse IVC from right sided approach Stavropoulos et al, J Vasc Interv Radiol 2003; 14:
26

27 Needle placement using a right-sided CT-guided approach through the retroperitoneum into the aneurysm sac Gorlitzer M. et al.; Interact CardioVasc Thorac Surg 2008;7:
28 Choice of Embolic Agent There are many choices regarding embolic agent. Permanent agents, such as coils are preferred. In most situations, if the channel between the inflow and outflow vessels is interrupted, the sac does not need to be embolized. In case of complex Type II endoleak, the filling of the endoleak cavity by translumbar approach without reaching the channel might not be sufficient to treat endoleak. Some authors support in addition to coils, use of either Gelfoam slurry, or thrombin. The use of several other agents has been successfully reported with trans-lumbar treatment of Type II endoleaks, including Onyx, Ethibloc, thrombin, and Cyano-acrylate.
29 Treatment with Onyx Onyx is a liquid embolic agent consisting of ethylene-vinyl-alcohol copolymer dissolved in DMSO. DMSO is an organic solvent, which causes weakening and degradation of plastics used in most currently marketed angiographic catheters. Fully DMSO-compatible catheters are therefore required for Onyx delivery. DMSO is compatible with Dacron and polytetrafluoroethylene and will not result in weakening of the fabrics used in currently marketed stent-grafts.
30 Treatment with Onyx Fills the endoleak sac completely, including all inflow and outflow vessels, without need for selective catheterization of each patent vessel Catheter occlusion with Onyx is unusual Onyx can be delivered in a slower, more controlled manner than other available liquid embolic agents, reducing this risk. Procedure times are shorter, the majority of patients can be treated on an outpatient basis. The opacity of Onyx results in considerable streak artifact on CT, making interpretation of images challenging
31
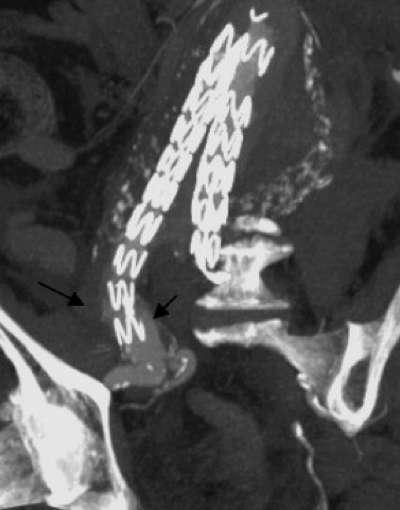
32 Type III Endoleak Type III endoleaks are caused by a structural failure of the implanted device, including: Junctional separation of modular components due to improper placement, migration, or changes in vessel morphology with aneurysm shrinkage. Holes in the fabric (usually suture holes). Fabric tears due to graft strut fracture or erosion.
33 Type III Endoleak This endoleaks are infrequent with an estimated incidence of 4% after 1 year. Type III leaks allow direct communication between the aorta and aneurysm sac. This results in systemic arterial pressure within the sac. Similar to Type I leaks, Type III endoleaks are considered to be very dangerous, since there is an acute re-pressurization of the sac and they need to be treated aggressively.


34 Type III Endoleak
35 Type III Treatment Angiography can confirm Type III endoleak after placement of the pigtail catheter in the stent graft, just above the flow divider. These endoleaks can usually be treated by placement of an additional extensor or a cuff at the level of the leak. The use of a bare metal stent has been used successfully to repair junctional stent-graft leaks.
36 Type III Treatment When the endoleak is due to perforation of the graft material, the only endovascular treatment option is relining the stent graft with a new bifurcated one or convert it to AUI graft with femoral femoral cross-over graft combined with deployment of an occluder in the contralateral side. Surgical conversion is the final option if those measures fail to salvage the problem.


37 Type III Repair
38 Type IV Endoleak Endoleaks that are caused by graft wall porosity are classified as type IV. These leaks are identified at the time of implantation as a blush seen during the immediate postimplantation angiogram, when patients are fully anticoagulated. They require no specific intervention except the normalization of the coagulation profile. Some believe that because these leaks are of no consequence and represent a successful endovascular procedure, they should not be classified as endoleaks. The diagnosis of a type IV endoleak should be one of exclusion because other types of leaks can masquerade as type IV.

39 Type IV Endoleak
40 Type V - Endotension Endotension originally was defined as expansion of the aneurysm sac after successful endovascular repair of abdominal aorta aneurysms. The term has now evolved to describe tension exerted on the aneurysm wall with or without the presence of an endoleak Some refer to endotension as a type V endoleak.
41 Type V - Endotension The exact cause of endotension is unknown: Clot provides an ineffective barrier to pressure transmission and that significant forces continue to affect the sac May represent existing types I, II, or III endoleaks that are occult to traditional imaging techniques Whatever the cause, the phenomenon of endotension could help to explain why approximately 20% of patients with stent graft show no evidence of aneurysm shrinkage after successful repair.
42 POSTOPERATIVE ENDOLEAK DIAGNOSIS Contrast enhanced CT scans performed at regular intervals. Performed at 30 days 90 days 6 months 12 months 18 months Then annually for the life of the patient
43 Limitations of CT in determining endoleak origins Directional flow cannot be accurately determined An endoleak seen on CT in continuity with a lumbar artery can represent either a type II leak if the flow in the lumbar is retrograde or a type I leak if the flow is antegrade (lumbar egress)
44 Ultrasound Surveillance A study published in JVS this year demonstrated that the ability to correctly identify the type of endoleak as confirmed at time of intervention was 74% with CDU imaging vs 42% by CT (P <.05). CDU, for the detection of endoleak requiring intervention, had a sensitivity of 90%, specificity of 81%, negative predictive value (NPV) of 99%, and positive predictive value (PPV) of 16% CT had a sensitivity of 58%, specificity of 87%, NPV of 98%, and PPV of 15%. Requires highly skilled US technicians. Endoleak after endovascular aneurysm repair: Duplex ultrasound imaging is better than computed tomography at determining the need for intervention Journal of Vascular Surgery, Volume 50, Issue 5, Pages G. Schmieder, C. Stout, G. Stokes, F. Parent, J. Panneton
45
46 Prevention of Endoleak Case Selection 20% oversizing of the endograft Generous overlapping of segments Graft covers the aorta and common iliac arteries from the renal arteries to the iliac artery bifurcation Prophylactic embolization of the internal iliac artery with common iliac artery aneurysm
47 Management of Endoleaks - Conclusion Type I: Immediate treatment. Balloon, cuff, Palmaz or conversion to open procedure Type II: Treat after 6 months if aneurysmal sac size does not decrease Late type I or III: treat immediately

48

49
50
51
52

53
54
55
56
57
Management of Endoleaks
 Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
Management of Endoleaks Murray Shames, MD Professor and Chief, Director Tampa General Hospital Aortic Program Vice Chair of Research, Dept. of Surgery Conflict of Interests: Speaker: Gore, Medtronic, Cook
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Endoleak Sealing after AAA Endovascular Repair. When and How?
 Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Endoleak Sealing after AAA Endovascular Repair. When and How? Poster No.: C-1086 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Quintana Blanco, B. González Humara, E. Torres Diez, C. Jimenez
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar. Saher Sabri,MD University of Virginia
 Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Approaches to type II Endoleaks: Transcaval, transarterial, translumbar Saher Sabri,MD University of Virginia Saher Sabri, M.D. Speakers Bureau: W.L.Gore & Associates, Abbott Type 2 Endoleaks after EVAR
Description. Section: Surgery Effective Date: April 15, Subsection: Surgery Original Policy Date: December 6, 2012 Subject:
 Last Review Status/Date: March 2015 Page: 1 of 6 Description Wireless sensors implanted in an aortic aneurysm sac after endovascular repair are being investigated to measure post procedural pressure. It
Last Review Status/Date: March 2015 Page: 1 of 6 Description Wireless sensors implanted in an aortic aneurysm sac after endovascular repair are being investigated to measure post procedural pressure. It
An endoleak is radiographic or ultrasonic evidence
 Complex Coil Embolization of Multiple Type II Endoleaks Liquid embolics, detachable coils, and plugs to repair an enlarging abdominal aortic aneurysm sac 5 years after EVAR. BY FRANK R. ARKO, MD; ABRAHAM
Complex Coil Embolization of Multiple Type II Endoleaks Liquid embolics, detachable coils, and plugs to repair an enlarging abdominal aortic aneurysm sac 5 years after EVAR. BY FRANK R. ARKO, MD; ABRAHAM
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Type II Endoleak Embolization Choice of Materials: EVOH, Glue, Thrombin & Coils. Michael S. Rosenberg, MD Assistant Professor of Radiology
 Type II Endoleak Embolization Choice of Materials: EVOH, Glue, Thrombin & Coils Michael S. Rosenberg, MD Assistant Professor of Radiology Michael Rosenberg, M. D. No relevant financial relationship reported
Type II Endoleak Embolization Choice of Materials: EVOH, Glue, Thrombin & Coils Michael S. Rosenberg, MD Assistant Professor of Radiology Michael Rosenberg, M. D. No relevant financial relationship reported
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Educational Exhibit Authors:
 Endoleaks in Abdominal Aortic Aneurysm Endoprosthesis: What radiologists need to know about Diagnostic, Characterization and Basic Management Strategies Poster No.: C-0150 Congress: ECR 2013 Type: Educational
Endoleaks in Abdominal Aortic Aneurysm Endoprosthesis: What radiologists need to know about Diagnostic, Characterization and Basic Management Strategies Poster No.: C-0150 Congress: ECR 2013 Type: Educational
symptomatic aneurysms or aneurysms that grow >1cm/yr
 1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
1. Elective repair for aneurysm >5.5 cm, symptomatic aneurysms or aneurysms that grow >1cm/yr 2. Ruptured AAA Aneurysm Detection and Management Study (ADAM) and UK Small Aneurysm Trial early open surgery
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
- to discuss the limits of traditional treatment options of type II endoleak after endovascular aneurysms repair (EVAR);
;") Transgluteal echo-guided arterial access: an unusual approach to treat type II endoleak following endovascular repair of an aortic and internal iliac artery aneurysm. Poster No.: C-0824 Congress: ECR 2014
Transgluteal echo-guided arterial access: an unusual approach to treat type II endoleak following endovascular repair of an aortic and internal iliac artery aneurysm. Poster No.: C-0824 Congress: ECR 2014
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Management of Endoleaks
 Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
Management of Endoleaks Sarah Ikponmwosa, MD Brooklyn VA 6/20/08 Questions Advantages of endovascular repair Definition of an endoleak Types of endoleaks Management of type lll endoleak Diagnosis of type
The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study,
 The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study, the 36 mm diameter Zenith Flex AAA Endovascular Graft
The clinical update for the Zenith AAA Endovascular Graft has included results from the Zenith AAA Endovascular Graft multi-center clinical study, the 36 mm diameter Zenith Flex AAA Endovascular Graft
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Technique and Tips for Complicated AAA Cases with Stent Graft
 Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
Technique and Tips for Complicated AAA Cases with Stent Graft Seung-Woon Rha, MD, PhD FACC, FAHA, FESC, FSCAI, FAPSIC Cardiovascular Center, Korea University Guro Hospital Mar 15, 2018 LINC AP 2018 Endoleak;
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
Aortic stents, types, selection, tricks in deployment.
 Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Faculty Disclosure. Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management. Background.
 Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
Glue, Particulates, Thrombin, Coils and the Kitchen Sink for Type II Endoleak Management Faculty Disclosure I disclose the following financial relationships: UCSF Vascular Symposium 2013 Receive grant/research
Cook Medical. Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training
 Cook Medical Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full-thickness,
Cook Medical Zenith Flex AAA Endovascular Graft with Z-Trak Introduction System Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full-thickness,
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Periprosthetic leak and rupture after endovascular repair of abdominal aortic aneurysm: The significance of device design for long-term results
 CASE REPORTS Periprosthetic leak and rupture after endovascular repair of abdominal aortic aneurysm: The significance of device design for long-term results Kirsten Krohg-Sørensen, MD, PhD, Magne Brekke,
CASE REPORTS Periprosthetic leak and rupture after endovascular repair of abdominal aortic aneurysm: The significance of device design for long-term results Kirsten Krohg-Sørensen, MD, PhD, Magne Brekke,
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair
 583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
583 Increased Flexibility of AneuRx Stent-Graft Reduces Need for Secondary Intervention Following Endovascular Aneurysm Repair Frank R. Arko, MD; W. Anthony Lee, MD; Bradley B. Hill, MD; Paul Cipriano,
Abdominal Aortic Aneurysm (AAA)
") Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Abdominal Aortic Aneurysm (AAA) Vascular Workshop: Objectives Anatomy Keith VanHaltren Indications Technique Cases Abdominal Aorta: Normal Size Abdominal aortic aneurysm: Definition Normal diameter of
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN
 Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Endoleaks after F-BEVAR How to Assess & Treat? Gustavo S. Oderich, MD Mayo Clinic Rochester, MN FACULTY DISCLOSURE Gustavo S. Oderich MD Consulting, DSMB, CEC* Cook Medical Inc., WL Gore, Lombardi Honoraria
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts
 Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Analysis of Type IIIb Endoleaks Encountered with Endologix Endografts Alan R. Wladis, MD, FACS, David Varnagy, MD, FACS, Manuel R. Perez-Izquierdo, MD, Mark Ranson, MD FACS, Delos Clift, MD FACS, Rebecca
Ancillary Components with Z-Trak Introduction System
 Ancillary Components with Z-Trak Introduction System Zenith Flex AAA Endovascular Graft Ancillary Components Converter Converters can be used to convert a bifurcated graft into an aortouniiliac graft if
Ancillary Components with Z-Trak Introduction System Zenith Flex AAA Endovascular Graft Ancillary Components Converter Converters can be used to convert a bifurcated graft into an aortouniiliac graft if
Hostile Proximal Neck: A New Conformable EVAR Device
 Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
Hostile Proximal Neck: A New Conformable EVAR Device Young-Guk Ko, M.D., Seoul, Korea Currently Available Devices for EVAR in Korea, 2018 Zenith Flex, Cook Endurant IIs, Medtronic INCRAFT, Cordis AFX2,
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type 1b Endoleak following an EVAR for Ruptured AAA
 Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
NEW INNOVATIONS IN ENDOLEAK MANAGEMENT
 DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
DISCLOSURES NEW INNOVATIONS IN ENDOLEAK MANAGEMENT Kelley HodgkissHarlow, MD, RPVI, FACS Vascular and Endovascular Surgery Kaiser Permanente, San Diego Nothing to disclose GOALS BACKGROUND Background Surveillance
Current Status of EVAR for Infrarenal AAA. 31 st Annual Florida Vascular Society. PENN Surgery
 Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Current Status of EVAR for Infrarenal AAA 31 st Annual Florida Vascular Society PENN Surgery No Disclosures Stent Grafts Design Related Differences What really matters? Modular Unibody Supported Unsupported
Zenith Renu AAA Converter Graft. Device Description Planning and Sizing Deployment Sequence Patient Follow-Up
 Zenith Renu AAA Converter Graft Device Description Planning and Sizing Deployment Sequence Patient Follow-Up Device description: Device indications The Zenith Renu AAA Converter Graft with Z-Trak Introduction
Zenith Renu AAA Converter Graft Device Description Planning and Sizing Deployment Sequence Patient Follow-Up Device description: Device indications The Zenith Renu AAA Converter Graft with Z-Trak Introduction
3. Endoluminal Treatment of Infrarenal Abdominal Aortic Aneurysm
 3. Endoluminal Treatment of Infrarenal Abdominal Aortic Aneurysm Hence J. M. Verhagen, Geoffrey H. White, Tom Daly and Theodossios Perdikides A 78-year-old male was referred for investigation and management
3. Endoluminal Treatment of Infrarenal Abdominal Aortic Aneurysm Hence J. M. Verhagen, Geoffrey H. White, Tom Daly and Theodossios Perdikides A 78-year-old male was referred for investigation and management
Case Report Late Type 3b Endoleak with an Endurant Endograft
 Case Reports in Radiology Volume 2015, Article ID 783468, 4 pages http://dx.doi.org/10.1155/2015/783468 Case Report Late Type 3b Endoleak with an Endurant Endograft Mehmet Barburoglu, 1 Bulent Acunas,
Case Reports in Radiology Volume 2015, Article ID 783468, 4 pages http://dx.doi.org/10.1155/2015/783468 Case Report Late Type 3b Endoleak with an Endurant Endograft Mehmet Barburoglu, 1 Bulent Acunas,
Endoleaks after endovascular aortic aneurysm repair. What a radiologist should know.
 Endoleaks after endovascular aortic aneurysm repair. What a radiologist should know. Poster No.: C-1370 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Gonzalez Nieto, C. Batz Colvée, M. M. Moreu
Endoleaks after endovascular aortic aneurysm repair. What a radiologist should know. Poster No.: C-1370 Congress: ECR 2013 Type: Educational Exhibit Authors: J. Gonzalez Nieto, C. Batz Colvée, M. M. Moreu
Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU)
") October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
THE ENDURANT STENT GRAFT IN HOSTILE ANEURYSM NECK ANATOMY
 THE ENDURANT STENT GRAFT IN HOSTILE ANEURYSM NECK ANATOMY Patrice Mwipatayi FCS (SA), MMed, FRACS Professor of Vascular surgery Royal Perth Hospital, University of Western Australia, Perth, WA Co-Authors:
THE ENDURANT STENT GRAFT IN HOSTILE ANEURYSM NECK ANATOMY Patrice Mwipatayi FCS (SA), MMed, FRACS Professor of Vascular surgery Royal Perth Hospital, University of Western Australia, Perth, WA Co-Authors:
Keagan Werner-Gibbings, 1 Chris Rogan, 2 and David Robinson Introduction. 2. Case Report
 Case Reports in Vascular Medicine Volume 2013, Article ID 861624, 4 pages http://dx.doi.org/10.1155/2013/861624 Case Report Novel Treatment of an Enlarging Internal Iliac Artery Aneurysm in Association
Case Reports in Vascular Medicine Volume 2013, Article ID 861624, 4 pages http://dx.doi.org/10.1155/2013/861624 Case Report Novel Treatment of an Enlarging Internal Iliac Artery Aneurysm in Association
GORE EXCLUDER AAA Endoprosthesis ANNUAL CLINICAL UPDATE OCTOBER Section I Clinical experience. Section II Worldwide commercial experience
 GORE EXCLUDER AAA Endoprosthesis ANNUAL CLINICAL UPDATE OCTOBER 2018 Abstract This annual clinical update provides a review of the ongoing experience with the GORE EXCLUDER AAA Endoprosthesis used in the
GORE EXCLUDER AAA Endoprosthesis ANNUAL CLINICAL UPDATE OCTOBER 2018 Abstract This annual clinical update provides a review of the ongoing experience with the GORE EXCLUDER AAA Endoprosthesis used in the
Endovascular Aneurysm Sealing System for Treating Abdominal Aortic Aneurysms: Early Outcomes from a Single Center
 Endovascular Aneurysm Sealing System for Treating Abdominal Aortic Aneurysms: Early Outcomes from a Single Center Thiti Chanmayka MD*, Anucha Ahooja MD**, Chalach Mitprachapranee MD*, Chawalit Wongbhuddha
Endovascular Aneurysm Sealing System for Treating Abdominal Aortic Aneurysms: Early Outcomes from a Single Center Thiti Chanmayka MD*, Anucha Ahooja MD**, Chalach Mitprachapranee MD*, Chawalit Wongbhuddha
TriVascular Ovation Prime Abdominal Stent Graft System
 TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
TriVascular Ovation Prime Abdominal Stent Graft System Science of the Seal O-Ring Sealing Technology O-Ring Sealing in Proven Engineering Solutions O-rings are designed to seal by blocking the flow of
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
Right Choice for Right Angles
 Right Choice for Right Angles The Anatomy of Technology Aorfix gives you technology that conforms to patient anatomy, optimising both procedure and post-operative performance. Fishmouth for optimum neck
Right Choice for Right Angles The Anatomy of Technology Aorfix gives you technology that conforms to patient anatomy, optimising both procedure and post-operative performance. Fishmouth for optimum neck
Primary to non-coronary IVUS
 codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
codes 2018 2018 codes Primary to non-coronary IVUS Page 2 All coding, coverage, billing and payment information provided herein by Philips is gathered from third-party sources and is subject to change.
14 Endoleak: Definition, Diagnosis, and Management
 Endoleak: Definition, Diagnosis, and Management 235 14 Endoleak: Definition, Diagnosis, and Management David Valenti and Jafar Golzarian CONTENTS 14.1 Introduction 235 14.2 Classification and Significance
Endoleak: Definition, Diagnosis, and Management 235 14 Endoleak: Definition, Diagnosis, and Management David Valenti and Jafar Golzarian CONTENTS 14.1 Introduction 235 14.2 Classification and Significance
Endoleak Visualized With Carbon Dioxide Angiography During Endovascular Aneurysm Repair Using the Endurant Stent-Graft
 172 J ENDOVASC THER 2014;21:172 176 CASE REPORT Endoleak Visualized With Carbon Dioxide Angiography During Endovascular Aneurysm Repair Using the Endurant Stent-Graft Robert P. Garvin, MD; Evan J. Ryer,
172 J ENDOVASC THER 2014;21:172 176 CASE REPORT Endoleak Visualized With Carbon Dioxide Angiography During Endovascular Aneurysm Repair Using the Endurant Stent-Graft Robert P. Garvin, MD; Evan J. Ryer,
Residual Dissection and False Lumen Aneurysm After TEVAR
 WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
WHAT WOULD YOU DO? Residual Dissection and False Lumen Aneurysm After MODERATOR: MARK FARBER, MD PANEL: YAZAN DUWAYRI, MD; MATTHEW J. EAGLETON, MD; WILLIAM D. JORDAN Jr, MD; TILO KÖLBEL, MD, PhD; AND ERIC
From 1996 to 1999, a total of 1,193 patients with
 THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
THE ANEURX CLINICAL TRIAL AT 8 YEARS Lessons learned following the US AneuRx clinical trial from 1996 to 2004. BY CHRISTOPHER K. ZARINS, MD From 1996 to 1999, a total of 1,193 patients with infrarenal
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany
 Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Treatment options for endoleaks: stents, embolizations and conversions
 Treatment options for endoleaks: stents, embolizations and conversions Poster No.: C-0861 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit G. Lombardi; napoli/it Arteries / Aorta, Abdomen,
Treatment options for endoleaks: stents, embolizations and conversions Poster No.: C-0861 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit G. Lombardi; napoli/it Arteries / Aorta, Abdomen,
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results
 Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results J. Brunkwall MD, Ph.D, FEBVS On behalf of the Pliant study groups E-liac Stent Graft System
Prospective Study of the E-liac Stent Graft System in Patients with Common Iliac Artery Aneurysm: 30-Day Results J. Brunkwall MD, Ph.D, FEBVS On behalf of the Pliant study groups E-liac Stent Graft System
Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management
 Review Article Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management Dania Daye, T. Gregory Walker Department of Radiology, Massachusetts General
Review Article Complications of endovascular aneurysm repair of the thoracic and abdominal aorta: evaluation and management Dania Daye, T. Gregory Walker Department of Radiology, Massachusetts General
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after Endovascular Aneurysm Repair with the Chimney Technique
 Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Case Reports in Vascular Medicine Volume 2016, Article ID 5307416, 4 pages http://dx.doi.org/10.1155/2016/5307416 Case Report A Case of Successful Coil Embolization for a Late-Onset Type Ia Endoleak after
Coding Changes for 2018
 Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular
Coding Changes for 2018 An overview of changes to interventional CPT coding that you need to know for practicing in 2018. BY KATHARINE L. KROL, MD, FSIR, FACR There are several coding changes for endovascular
COMPLICATIONS OF TEVAR
 COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability. Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands
 GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
GORE EXCLUDER AAA Endoprosthesis demonstrates long-term durability Michel Reijnen Rijnstate Hospital Arnhem, The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts
Hostile Neck During EVAR, The Role Of Endoanchores
 Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
2014 ANNUAL CLINICAL UPDATE. TriVascular Inc. Ovation and Ovation Prime Abdominal Stent Graft Systems
 2014 ANNUAL CLINICAL UPDATE TriVascular Inc. Ovation and Ovation Prime Abdominal Stent Graft Systems 2014 ANNUAL CLINICAL UPDATE TriVascular Inc. Ovation and Ovation Prime Abdominal Stent Graft Systems
2014 ANNUAL CLINICAL UPDATE TriVascular Inc. Ovation and Ovation Prime Abdominal Stent Graft Systems 2014 ANNUAL CLINICAL UPDATE TriVascular Inc. Ovation and Ovation Prime Abdominal Stent Graft Systems
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Complications of EVAR
 Complications of EVAR Is endovascular aneurysm repair still worth the trouble? BY ROBERT S. DIETER, MD, RVT; JEFFREY FREIHAGE, MD; PRANAB DAS, MD; LEONARDO CLAVIJO, MD; SOHAIL IKRAM, MD; KRISHNA MANNAVA,
Complications of EVAR Is endovascular aneurysm repair still worth the trouble? BY ROBERT S. DIETER, MD, RVT; JEFFREY FREIHAGE, MD; PRANAB DAS, MD; LEONARDO CLAVIJO, MD; SOHAIL IKRAM, MD; KRISHNA MANNAVA,
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry
 Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when?
 Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
Acute Type B dissection. Closure of the infra diaphragmatic tear: how and when? Prof. Olgierd Rowiński II Department of Clinical Radiology Medical University of Warsaw Disclosure Speaker name: Olgierd
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium
 How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
How to Categorize the Infrarenal Neck Properly? I Van Herzeele Dept. Thoracic and Vascular Surgery, Ghent University, Belgium Disclosure Speaker name: Isabelle Van Herzeele I have the following potential
Length Measurements of the Aorta After Endovascular Abdominal Aortic Aneurysm Repair
 Eur J Vasc Endovasc Surg 18, 481 486 (1999) Article No. ejvs.1999.0882 Length Measurements of the Aorta After Endovascular Abdominal Aortic Aneurysm Repair J. J. Wever, J. D. Blankensteijn, I. A. M. J.
Eur J Vasc Endovasc Surg 18, 481 486 (1999) Article No. ejvs.1999.0882 Length Measurements of the Aorta After Endovascular Abdominal Aortic Aneurysm Repair J. J. Wever, J. D. Blankensteijn, I. A. M. J.
Multi-detector CT angiographic imaging in the follow-up of patients after endovascular abdominal aortic aneurysm repair (EVAR)
") Insights Imaging (2012) 3:313 321 DOI 10.1007/s13244-012-0173-0 PICTORIAL REVIEW Multi-detector CT angiographic imaging in the follow-up of patients after endovascular abdominal aortic aneurysm repair
Insights Imaging (2012) 3:313 321 DOI 10.1007/s13244-012-0173-0 PICTORIAL REVIEW Multi-detector CT angiographic imaging in the follow-up of patients after endovascular abdominal aortic aneurysm repair
CPT 2018 Radiology Code Changes
 CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
CPT 2018 Radiology Code Changes CPT 2018 Radiology Code Changes The following is a listing of new Current Procedural Terminology (CPT ) codes and their descriptors as described in the CPT 2018 codebook.
Hypogastric Preservation Using Retrograde Endovascular Bypass
 Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Hypogastric Preservation Using Retrograde Endovascular Bypass Mathew Wooster MD, Adam Tanious MD, Brad Johnson MD, Murray Shames MD, Paul Armstrong MD, Martin Back MD Florida Vascular Society 30 th Annual
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs
 How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
Abdominal Aortic Aneurysm 가천대길병원 이상준
 Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Abdominal Aortic Aneurysm 가천대길병원 이상준 1 Definition Diameter of the aorta 1.5 times greater than normal. Most are infrarenal, and a significant number extend down into one or both iliac arteries Abdominal
Challenging anatomies demand versatility.
 Challenging anatomies demand versatility. The Distinct Advantages of Separating Seal and Fixation ANATOMICAL FIXATION Unlike proximal fixation designs, the AFX bifurcated unibody endograft allows for natural
Challenging anatomies demand versatility. The Distinct Advantages of Separating Seal and Fixation ANATOMICAL FIXATION Unlike proximal fixation designs, the AFX bifurcated unibody endograft allows for natural
Embolization for type 2 endoleak with sac expansion after endovascular repair of abdominal aortic aneurysm: safety and effectiveness
 DOI 10.1186/s40064-016-1934-x RESEARCH Open Access Embolization for type 2 endoleak with sac expansion after endovascular repair of abdominal aortic aneurysm: safety and effectiveness Kenji Kajiwara 1*,
DOI 10.1186/s40064-016-1934-x RESEARCH Open Access Embolization for type 2 endoleak with sac expansion after endovascular repair of abdominal aortic aneurysm: safety and effectiveness Kenji Kajiwara 1*,
CT approach to complications following endovascular stentgrafting of thoracic and abdominal aorta
 CT approach to complications following endovascular stentgrafting of thoracic and abdominal aorta Poster No.: C-1296 Congress: ECR 2011 Type: Educational Exhibit Authors: M. D. R. Matos, P. Ananias, H.
CT approach to complications following endovascular stentgrafting of thoracic and abdominal aorta Poster No.: C-1296 Congress: ECR 2011 Type: Educational Exhibit Authors: M. D. R. Matos, P. Ananias, H.
The evolution. AORFIX AAA Stent Graft now with the new AORFLEX Delivery System
 The evolution of AORFIX AORFIX AAA Stent Graft now with the new AORFLEX Delivery System The confident choice for the right angles AORFIX the only AAA stent graft approved for all angulations from 0 90,
The evolution of AORFIX AORFIX AAA Stent Graft now with the new AORFLEX Delivery System The confident choice for the right angles AORFIX the only AAA stent graft approved for all angulations from 0 90,
150 Aortic Aneurysm - Recent Advances is the occurrence and significance of endoleaks. White et al were the first to systematically describe and class
 Chapter 8 Endovascular Treatment of Endoleaks Following EVAR Zaiping Jing, Qingsheng Lu, Jiaxuan Feng and Jian Zhou Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54836
Chapter 8 Endovascular Treatment of Endoleaks Following EVAR Zaiping Jing, Qingsheng Lu, Jiaxuan Feng and Jian Zhou Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54836
Considerations for a Durable Repair
 Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Considerations for a Durable Repair Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University, Nuremberg, Germany Disclosures William Cook
Disclosures. EVAR follow-up: actual recommendation. EVAR follow-up: critical issues
 Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
Disclosures is it time to discuss individualized follow-up schemes based on preoperative anatomy and high quality completion angiography? Consultant / Speaker / Proctor Cook Cordis Medtronic Invatec W.L.
FROM THE EVERYDAY TO THE EXTRAORDINARY
 FROM THE EVERYDAY TO THE EXTRAORDINARY Created with the collaboration of more than 250 physicians around the world, ENDURANT empowers you to create stronger outcomes for more patients, including those
FROM THE EVERYDAY TO THE EXTRAORDINARY Created with the collaboration of more than 250 physicians around the world, ENDURANT empowers you to create stronger outcomes for more patients, including those