Management of Resistant Hypertension in Diabetes
|
|
|
- Buck Sims
- 6 years ago
- Views:
Transcription
1 Management of Resistant Hypertension in Diabetes Soon Hee Lee, M.D., Ph.D. Divisoin of Endocrinology & Metabolism, Department of Internal Medicine, Busan Paik Hospital, College of Medicine, Inje University, Busan, South Korea
2 DIABETES FACT SHEET IN KOREA 2013
3 Hypertension Jun;51(6): Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive agents of different classes. Ideally, 1 of the 3 agents should be a diuretic & all agents should be prescribed at optimal dose amounts.
4 Definition Highlights Use of diuretic recommended but not required before diagnosing resistant hypertension. Doses should be optimal but not necessarily maximal before diagnosing resistant hypertension. Controlled resistant hypertension: high blood pressure controlled but with use of 4 of more agents should be considered resistant. Hypertension Jun;51(6):

5 2013 ESH/ESC Guidelines Journal of Hypertension 2013, 31:
6 Guideline Comparisons of Goal BP and Initial Drug Therapy for Adults with Hypertension Guideline Population Goal BP, mm Hg JNC Hypertension guideline Initial Drug Treatment Options General 60 y <150/90 Nonblack: thiazide-type diuretic, ACEI, ARB, or CCB General <60 y <140/90 Black: thiazide-type diuretic or CCB Diabetes <140/90 Thiazide-type diuretic, ACEI, ARB, or CCB CKD <140/90 ACEI or ARB NICE 2011 General <80 y <140/90 <55 y: ACEI or ARB General 80 y <150/90 55 y or black: CCB KDIGO 2012 CKD no proteinuria CKD + protein uria 140/90 ACEI or ARB 130/80 JAMA. 2013;():. doi: /jama
7 Recommendations: Hypertension/Blood Pressure Control Goals People with diabetes and hypertension should be treated to a systolic blood pressure goal of <140 mmhg B Lower systolic targets, such as <130 mmhg, may be appropriate for certain individuals, such as younger patients, if it can be achieved without undue treatment burden C Patients with diabetes should be treated to a diastolic blood pressure <80 mmhg B ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S36
8 Am J Med Sci Dec;298(6): Critical Importance of Adequate Diuretic Therapy 23/32 patients referred for management of resistant hypertension had evidence of expanded extracellular volume by nuclear study None had clinical evidence of expanded extracellular volume All were already on diuretic therapy
9 Critical Importance of Adequate Diuretic Therapy Control improved in patients treated with potent thiazide diuretics (indapamide, metolazone, or larger doses of hctz, etc.) or given multiple daily doses of loop diuretics Patients with co-existent renal disease may require more intensive diuretic therapy
10 Med J Aust Feb 12;1(7):213-5.
11 Prevalence Prevalence is unknown, but observational and clinical trials suggest it is a common clinical problem. In a recent analysis of National Health and Nutrition Examination Survey (NHANES) participants being treated for hypertension, only 53% were controlled to <140/90 mm Hg. 1 of NHANES participants with CKD, only 37% were controlled to <130/80 mm Hg 2 and only 25% of diabetic participants were controlled to <130/85 mm Hg. 1 In the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) after approximately 5 years of follow-up, 27% of participants were on 3 or more medications. 3 1 Hajjar I, Kotchen TA. JAMA 2003; 2 Peralta CA et al. Hypertension 2005; 3 Cushman WC et al. Clin Hypertens.



12 In General Population - Low In Specialized Clinics -15% In Clinical Trials* - 30% *ALLHAT, CONVINCE, LIFE, INSIGHT
13 Patient Characteristics Associated with Resistant Hypertension High baseline blood pressure Older age Obesity Excessive dietary salt ingestion Chronic kidney disease Diabetes Left ventricular hypertrophy Female gender Hypertension Jun;51(6):
14 Lifestyle Factors Contributing to Resistant Hypertension Obesity or overweight High salt diet Physical inactivity Ingestion of low-fiber, high-fat diet Heavy alcohol ingestion Hypertension Jun;51(6):
15 Causes of Resistance to Hypertension Treatment Poor adherence with prescribed medications Inaccurate blood pressure measurement White coat hypertension & Pseudohypertension Secondary causes of HTN & interfering substance Hypertension Jun;51(6):
16 The Importance of Adherence Only 1/2 to 2/3 of patients take at least 75% of prescribed antihypertensive medicines of those taking < 75%, only 37% achieved BP goal of those taking >= 75%, 81% achieved goal Arch Intern Med Aug;147(8):
17 Techniques to Improve Adherence Education of the patient Increases awareness but less effect on behavior Minimize the number of pills Combination pills (ACEi/diuretic, ARB/diuretic, ARB/Ca-blocker, etc.) Minimize the frequency Increase the frequency of visits Use of care managers
18 Causes of Resistance to Hypertension Treatment Poor adherence with prescribed medications Inaccurate blood pressure measurement White coat hypertension & Pseudohypertension Secondary causes of HTN & interfering substance Hypertension Jun;51(6):

19 Accurate Reading of Blood Pressure Cuff bladder encircle >80% pts arm sphygmomanometer Deflate 2-3mm per second Siting comfortably Back supported Legs uncrossed Upper arm bared Cuff bladder at heart level SBP INACCURATELY HIGH IF: patient is supine, crossed legs, cuff below the heart, arm unsupported, undersized cuff. AHA guidelines
20 Causes of Resistance to Hypertension Treatment Poor adherence with prescribed medications Inaccurate blood pressure measurement White coat hypertension & Pseudohypertension Secondary causes of HTN & interfering substance Hypertension Jun;51(6):
21 White Coat Hypertension 20-30% of Apparently Resistant Hypertension may be due to White-Coat Hypertension Patients with WCH have an increased risk of CV events and often have some degree of end organ damage Use home or ambulatory monitoring to sort out

22 Journal of Hypertension 2013, 31:

23 Home and Ambulatory BP Monitoring (ABPM) Often lower than office readings Journal of Hypertension 2013, 31:

24 Pseudohypertension Osler s Maneuver (the radial artery remains palpable due to calcification and thickening despite inflation of cuff above systolic pressure) Poorly reproducible Dinamap -like devices may be more accurate in this setting Direct Intra-arterial measurement is the only definitive way to establish the diagnosis, but this is uncommonly done
25 Causes of Resistance to Hypertension Treatment Poor adherence with prescribed medications Inaccurate blood pressure measurement White coat hypertension & Pseudohypertension Secondary causes of HTN & interfering substance Hypertension Jun;51(6):
26 Secondary Causes of Resistant Hypertension Common Obstructive sleep apnea Renal parenchymal disease Primary aldosteronism Renal artery stenosis Hypertension Jun;51(6):
27 Secondary Causes of Resistant Hypertension Uncommon Pheochromocytoma Cushing s disease Hyperparathyroidism Aortic coarctation Intracranial tumor Hypertension Jun;51(6):
28 Primary Aldosteronism and Diabetes Type 2 diabetic patients are frequently affected by hypertension, and approximately 50 75% fail to achieve satisfactory blood pressure control. This is one cause of the high incidence of cardiovascular complications, such as heart failure, stroke, and kidney disease. A close relationship between aldosterone and insulin resistance has been demonstrated: hyperinsulinemia stimulates the production of aldosterone, and an excess of mineralocorticoids can cause the resistant hypertension observed in diabetic patients. Int J Hypertens. 2011;2011:162804
29

30 J Hypertens Oct;31(10):
31 Substances that Can Interfere with Blood Pressure Control Non-Narcotic Analgesics - Non-steroidal anti-inflammatory agents including aspirin - Selective COX-2 inhibitors Sympathomimetic agents - decongestants - diet pills - cocaine Stimulants -methylphenidate -dexmethylphenidate, -dextroamphetamine - amphetamine, methamphetamine -modafinil Hypertension Jun;51(6):
32 Substances that Can Interfere with Blood Pressure Control Alcohol Oral contraceptives Cyclosporine Erythropoietin Natural licorice Herbal compounds - ephedra - ma huang Hypertension Jun;51(6):
33 Exclude pseudoresistance Identify and reverese contributing factor Discontiue and/or minimizie interfering substance Screen of secondary causes of Hypertension Diagnosis of true resistant Hypertension
34 Treatment of Resistant Hypertension Non-Pharmacologic Recommendations Weight loss Regular exercise (at least 30 min most days of the week) Low dietary salt ingestion (<100 meq sodium/24-hr) Moderate alcohol ingestion (no more than 2 drinks per day for most men and 1 drink per day for women or lighter weight persons) Ingestion of low-fat, high-fiber diet Treat obstructive sleep apnea if present Hypertension Jun;51(6):
35 Treatment of Resistant Hypertension Pharmacologic Recommendations Withdrawal or down titration of interfering substances as possible Use of a long-acting thiazide diuretic, preferably chlorthalidone Combine agents with different mechanisms of action Recommended triple regimen of -ACE inhibitor or ARB - Calcium channel blocker -Thiazide diuretic Hypertension Jun;51(6):
36 Treatment of Resistant Hypertension Consider addition of mineralocorticoid receptor antagonist Use of loop diuretic may be necessary in patients with CKD (creatinine clearance <30 ml/min) Hypertension Jun;51(6):
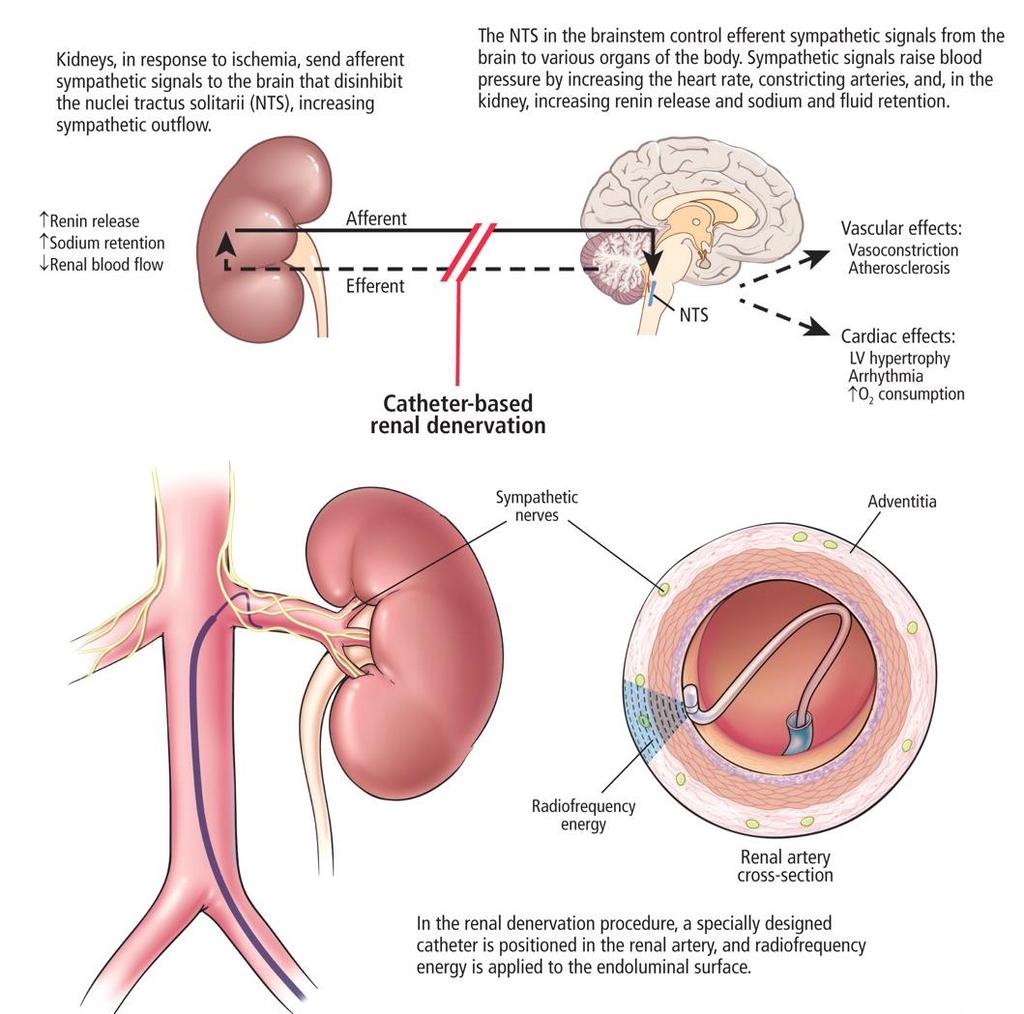
37 Non Pharmacological Approaches The following procedures are invasive and irreversible Implantable pulse generators perivascular carotid sinus leads to be surgically implanted Renal Denervation
38 Renal Sympathetic Activation: Efferent Nerves Kidney as Recipient of Sympathetic Signals Renal Efferent Nerves Renin Release RAAS activation Sodium Retention Renal Blood Flow


39 Renal Sympathetic Activation: Afferent Nerves Kidney as Origin of Central Sympathetic Drive Vasoconstriction Atherosclerosis Insulin Resistance Sleep Disturba nces Renal Afferent Nerves Hypertrophy Arrhythmia Oxygen Consumption Renin Release RAAS activation Sodium Retention Renal Blood Flow
40


41 Renal Nerve Anatomy Nerves arise from T10-L2 The nerves arborize around the artery and primarily lie within the adventitia Vessel Lumen Media Adventitia Renal Nerves 41 41





42 Renal Nerve Anatomy Allows a Catheter-Based Approach Spacing of e.g. 5 mm. Renal artery access via standard interventional technique 4-6 two-minute treatments per artery Proprietary RF generator Automated Low power Built-in safety algorithms 42


 - 12-month data \ Expanded Cohort* This")
 -36-month follow-up *Expanded results presented at")
43 Symplicity HTN-1 Lancet. 2009;373: Hypertension. 2011;57: Initial Cohort Reported in the Lancet, 2009: -First-in-man, non-randomized -Cohort of 45 patients with resistant HTN (SBP 160 mmhg on 3 anti-htn drugs, including a diuretic; egfr 45 ml/min) - 12-month data \ Expanded Cohort* This Report (Symplicity HTN-1): -Expanded cohort of patients (n=153) -36-month follow-up *Expanded results presented at the American College of Cardiology Annual Meeting 2012 (Krum, H.)
44 Symplicity HTN-1: BP Reductions through 3 years BP change (mmhg) Systolic BP Diastolic BP -35 P<0.01 for from BL for all time points M (n=143) 3 M (n=148) 6 M (n=144) 12 M (n=130) 18 M (n=107) 24 M (n=59) 30 M (n=24) 36 M (n=24) *Expanded results presented at the American College of Cardiology Annual Meeting 2012 (Krum, H.)

45 Symplicity HTN-2 Lancet. 2010;376: Purpose: To demonstrate the effectiveness of catheter-based renal denervation for reducing blood pressure in patients with uncontrolled hypertension in a prospective, randomized, controlled, clinical trial Patients: 106 patients randomized 1:1 to treatment with renal denervation vs. control Clinical Sites: 24 centers in Europe, Australia, & New Zealand (67% were designated hypertension centers of excellence) Symplicity HTN-2 Investigators. Lancet. 2010;376:
46 Symplicity HTN-2 Trial Treatment-resistant HTN population BL OBP 178/97 mmhg 49 Renal Denervation, 51 Control Age 58 years BMI 31 kg/m² 40% with Diabetes egfr 77* Avg # meds 5.2 Renal Denervation and Control groups generally well-matched Inclusion Criteria: Office SBP 160 mmhg ( 150 mmhg with type II diabetes mellitus) Stable drug regimen of 3+ more anti-htn medications Age years Exclusion Criteria: Haemodynamically or anatomically significant renal artery abnormalities or prior renal artery intervention egfr < 45 ml/min/1.73m 2 (MDRD formula) Type 1 diabetes mellitus Contraindication to MRI Stenotic valvular heart disease for which reduction of BP would be hazardous MI, unstable angina, or CVA in the prior 6 months *MDRD, ml/min/1.73m 2 Symplicity HTN-2 Investigators. Lancet. 2010;376:
47 * Crossed-over with ineligible BP (<160 mmhg) Symplicity HTN-2: Patient disposition Screening Assessed for Eligibility (n=190) Randomised (n=106) Excluded During Screening, Prior to Randomisation (n=84) BP < 160 at Baseline Visit (after 2-weeks of medication compliance confirmation) (n=36; 19%) Ineligible anatomy (n=30; 16%) Declined participation (n=10; 5%) Other exclusion criteria discovered after consent (n=8; 4%) 6-month Primary End-Point Allocated to RDN n=52 Treated n=49 Analysable Allocated to Control n=54 Control n=51 Analysable Crossover n=46 2 LTFU 12-month Post- Randomisation 12-month post-rdn n=47 Per protocol, 6-mo Post-RDN (Crossover) n=35 Not-per-protocol*, 6 -mo Post-RDN (Cros sover) n=9
48 Symplicity HTN-2: Primary Endpoint 10 0 from Baseline -10 to 6 Months (mmhg -20 ) and Latest Follow-up Primary Endpoint (6M post Randomisation) RDN (n = 49) Control (n = 51) Systolic -12 Diastolic 1 Systolic 0 Diastolic p <0.01 for difference between Renal denervation and Control from Baseline to 12 Months (mm Hg) Latest Follow-up (12M post Randomisation) RDN (n= 47) -28 Systolic -10 Diastolic p <0.01 for from baseline Primary Endpoint: 84% of RDN patients had 10 mmhg reduction in SBP 10% of RDN patients had no reduction in SBP Latest Follow-up: Control crossover (n = 35): -24/-8 mmhg (Analys is on patients with SBP 160 mmhg at 6 M) Expanded results presented at the American College of Cardiology Annual Meeting 2012 (Esler, M.)
49 Symplicity HTN-2: Lancet Conclusions Catheter-based renal denervation, done in a multicentre, randomised trial in patients with treatment-resistant essential hypertension, resulted in significant reductions in BP. The magnitude of BP reduction can be predicted to affect the development of hypertension-related diseases and mortality The technique was applied without major complications. This therapeutic innovation, based on the described neural pathophysiology of essential hypertension, affirms the crucial relevance of renal nerves in the maintenance of BP in patients with hypertension. Catheter-based renal denervation is beneficial for patients with treatment-resistant essential hypertension. Symplicity HTN-2 Investigators. Lancet. 2010;376:
50 Symplicity 3 HTN Trial 535 patients with resistant HTN in 87 US medical centers Intervention: Radiofrequency ablation vs sham control. Radomization: 2/3 intervention, 1/3 Sham Endpoints: safety and efficacy at 6 months Results: did not show a significant reduction of systolic blood pressure in patients with resistant hypertension 6 months after renal-artery denervation as compared with a sham control. N Engl J Med Apr 10;370(15):

51 N Engl J Med Apr 10;370(15):

52 Journal of Hypertension 2013, 31:

53 Journal of Hypertension 2013, 31:
54 Conclusions Patients with RHTN should be screened for reversible causes of hypertension, such as renal artery stenosis, primary aldosteronism, and obstructive sleep apnea. Patients should be counseled about potentially modifiable lifestyle factors, such as sodium intake, weight loss, diet, and exercise. Combination therapy with different antihypertensive classes is crucial in the effective treatment of RHTN. This should ideally include a thiazide-like diuretic The role of aldosterone excess in the pathogenesis of RHTN is being increasingly recognized, and addition of a mineralocorticoid receptor antagonist as a fourth-line antihypertensive agent is recommended. Overall, renal denervation and carotid baroreceptor stimulation should be restricted to resistant hypertensive patients at particularly high risk, after fully documenting the inefficacy of additional antihypertensive drugs to achieve BP control. Integrated Blood Pressure Control 2013: Journal of Hypertension 2013, 31:
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Catheter-Based Renal Denervation (RDN)
") Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Hypertension lecture 3: Catheter-Based Renal Denervation (RDN) Adapted from slides prepared by Dr IOEBRAHIM, UNITAS HOSPITAL and others Hypertension Epidemiology 30% Untreated 35% Treated & Controlled
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
How to Manage Resistant Hypertension Min Su Hyon, MD
 How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 22 June 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension
 Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
Catheter-Based Renal Sympathetic Denervation in the Management of Resistant Hypertension Henry Krum, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski, Krzysztof Bartus, Boguslaw Kapelak, Horst
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Real World Experience with Renal Denervation Therapy
 JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
JCR 2013 Real World Experience with Renal Denervation Therapy Seung-Hyuk Choi Division of Cardiology Samsung Medical Center Seoul, Korea Hypertension A Major Public Health Burden Astonishing prevalence
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Treating Hypertension With a Catheter..Wait What? COI 5/3/2013. Worldwide Prevalence of Hypertension Is Increasing
 Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Treating Hypertension With a Catheter..Wait What? David P. Lee, M.D. 4 May 2013 Stanford University COI Medtronic: Research Grant, Consultant Boston Scientific: Research Grant, MAB Worldwide Prevalence
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
What We've Learned from Simplicity HTN-1,2, and Registries
 ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
ANGIOPLASTY SUMMIT-TCTAP 2012 Seoul, Korea, April 24-27, 2012 What We've Learned from Simplicity HTN-1,2, and Registries Horst Sievert, Ann-Kathrin Ziegler, Benjamin Kaltenbach, Ilona Hofmann, Undine Pittl
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension
 Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Catheter-Based Renal Denervation Reduces Total Body and Renal Noradrenaline Spillover and Blood Pressure in Resistant Hypertension Murray Esler, Markus Schlaich, Paul Sobotka, Rob Whitbourn, Jerzy Sadowski,
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL
 CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE HYPERTENSION PROTOCOL Douglas G. Kelling Jr., MD Carmella Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised, April 8, 2012 The information contained in this protocol
Renal denervation: Current evidence and remaining uncertainties
 Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
Renal denervation: Current evidence and remaining uncertainties Michel Azizi Georges Pompidou European Hospital Hypertension Unit ESH excellence Center Paris Descartes University Clinical Investigation
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study
 Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Hypertension: the Heart Vs the Kidney. George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi
 Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
Hypertension: the Heart Vs the Kidney George Moturi Physician/Nephrologist Aga Khan Hospital Nairobi 24 th Feb, 2017 Travel facilitation from Novartis Disclaimer Systolic blood pressure (SBP) of at least
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
noradrenaline spillover and systemic blood pressure in patients with resistant hypertension
 Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Effects of renal sympathetic denervation on noradrenaline spillover and systemic blood pressure in patients with resistant hypertension Markus Schlaich Neurovascular Hypertension & Kidney Disease Laboratory
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
IMET 2000 PAL International Medical Education Trust Palestine What the GP Should Know about Hypertension
 What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
What the GP Should Know about Hypertension Raed Abu Sham a, M.D Internist and Cardiologist Cardiac Pacing and Electrophysiologist Impact of Age on Blood Pressure Prevalence of HTN according to Age Fast
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
major public health burden
 HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
HYPERTENSION INTRODUCTION Hypertension is one of the major public health burden in the recent times. Hypertension remains a challenging medical condition among the noncommunicable diseases of ever growing
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Stephen G. Worthley 1, Gerard T. Wilkins 2, Mark W. Webster 3,Joseph K. Montarello 1, Paul T. Antonis 4, Robert J. Whitbourn 5, Roderic J.
 Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Six Month Results of First-in-Human Sympathetic Renal Artery Denervation Using a Next Generation Multi-Electrode Renal Artery Denervation System in Patients with Drug-Resistant Hypertension Stephen G.
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
AHA Scientific Statement
 AHA Scientific Statement REPRINT Resistant Hypertension: Diagnosis, Evaluation, and Treatment A Scientific Statement From the American Heart Association Professional Education Committee of the Council
AHA Scientific Statement REPRINT Resistant Hypertension: Diagnosis, Evaluation, and Treatment A Scientific Statement From the American Heart Association Professional Education Committee of the Council
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Renal Denervation for Resistant Hypertension
 Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Renal Denervation for Resistant Hypertension James W. Choi MD FACC FSCAI Cardiology Consultants of Texas Director Interventional Cardiology Fellowship Baylor University Medical Center Baylor Heart & Vascular
Update on renal denervation: Latest data
 LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
LINC 2018 Update on renal denervation: Latest data Felix Mahfoud Saarland University Hospital, Germany Potential Conflicts of Interest I have the following potential conflicts of interest to report: Research
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Christopher Valentine, MD
 Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
Resistant Hypertension Christopher Valentine, MD Program Director, Nephrology Fellowship Program Department of Internal Medicine Division of Nephrology The Ohio State University Wexner Medical Center Disclosures
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Managing High Blood Pressure Naturally. Michael A. Smith, MD Life Extension s Healthy Talk Series
 Managing High Blood Pressure Naturally Michael A. Smith, MD Life Extension s Healthy Talk Series Part 1 What is Blood Pressure? Blood Pressure Systole Systolic Forward Pressure 110 mmhg 70 mmhg Diastole
Managing High Blood Pressure Naturally Michael A. Smith, MD Life Extension s Healthy Talk Series Part 1 What is Blood Pressure? Blood Pressure Systole Systolic Forward Pressure 110 mmhg 70 mmhg Diastole
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Byeong-Keuk Kim, MD, PhD. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Byeong-Keuk Kim, MD, PhD Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea BP change (mmhg) from Baseline to 6 Months (mmhg) Catheter-based renal
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA