RENAL ARTERY STENOSIS. Grand Rounds 10/11/2011
|
|
|
- Garey Rose
- 6 years ago
- Views:
Transcription
1 RENAL ARTERY STENOSIS Grand Rounds 10/11/2011
2 ARAS Prevalence- 0.5% overall population, 5.5% in ckd pts No correlation between ischemic nephropathy and severity of stenosis Increased risk of vascular events- CAD 67% vs 25%, CVA-37% vs 12%, PVD-56% vs 13%, CKD- 25% vs 2% (medicare database) Renovascular htn 5 yr survival 45%, 18% once on dialysis
 70,")
3 RESISTIVE INDEX Kidney International (2006) 70,
4 FACTORS THAT PLAY ROLE IN RVD VEGF has been shown in animal models to be crucial for preservation of renal microvasculature and promotes vascular proliferation and endothelial repair. Hypoxia-inducible factor (HIF)-1, matrix metalloproteinases (MMP)-2, MMP-9, membranetype MMP (MT-MMP), plasminogen activator inhibitor (PAI)-1, tissue transglutaminase (ttg), and transforming growth factor (TGF)-beta are other factors shown to play a role.
5 CARDIAC RISK IN RAS Cardiotonic steroids are a group of steroids recently discovered in the plasma and urine of pts with CHF, CKD and MI. Object of the study is to test the effect of renal ischemia on marinobufagenin (MBG) in humans
6 RESULTS
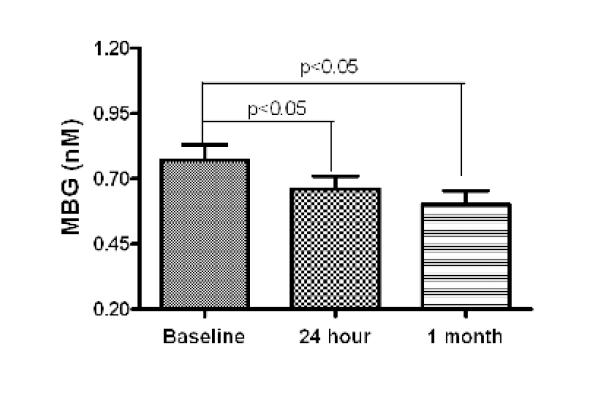
7 RESULTS
8 MBG VS GFR CHANGE
9 CONCLUSIONS MBG levels are increased in RAS and treatment reduces levels In patients with b/l RAS decrease in MBG correlates with gfr change suggesting possible role of MBG in maintaining GFR in global ischemia
10 TREATMENT OF ARAS Medical therapy Percutaneous Angioplasty / stent Surgical angioplasty
11 WHAT IS CRITICAL RAS?
12 ASTRAL TRIAL-METHODS Multicenter, randomized, unblinded Medical treatment included antiplatelet, statins and bp control 403 in each arm Inclusion criteria- 59% had >70% stenosis or renal dysfunction creat >1.7 or both 6% from medical crossed over to intervention grp
13 END POINTS Primary end point Rate of progression of renal dysfunction (Using reciprocal creat over time) Secondary end points Renal events- AKI, dialysis, txp or nephrectomy Vascular events- MI, angina, stroke
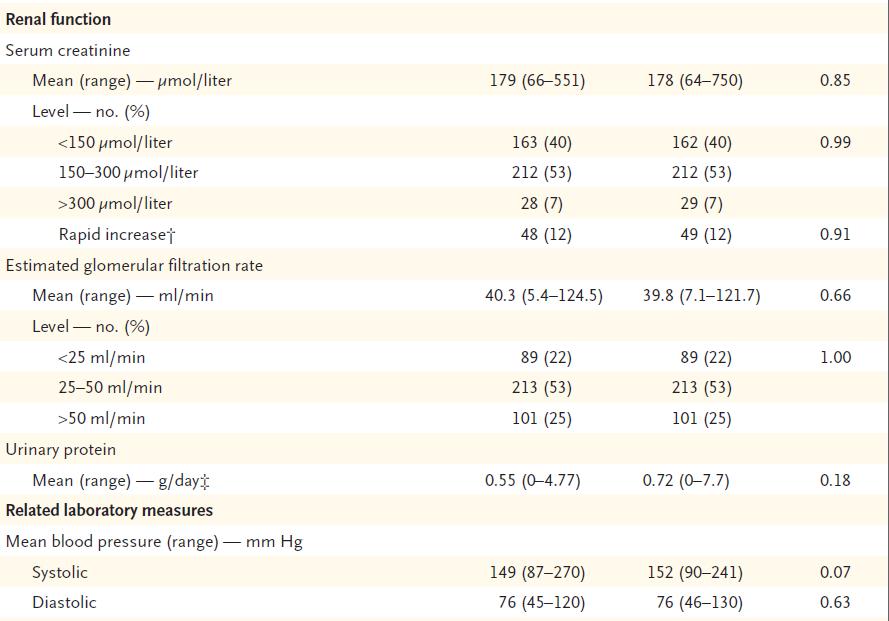
14 PATIENT CHARACTERISTICS
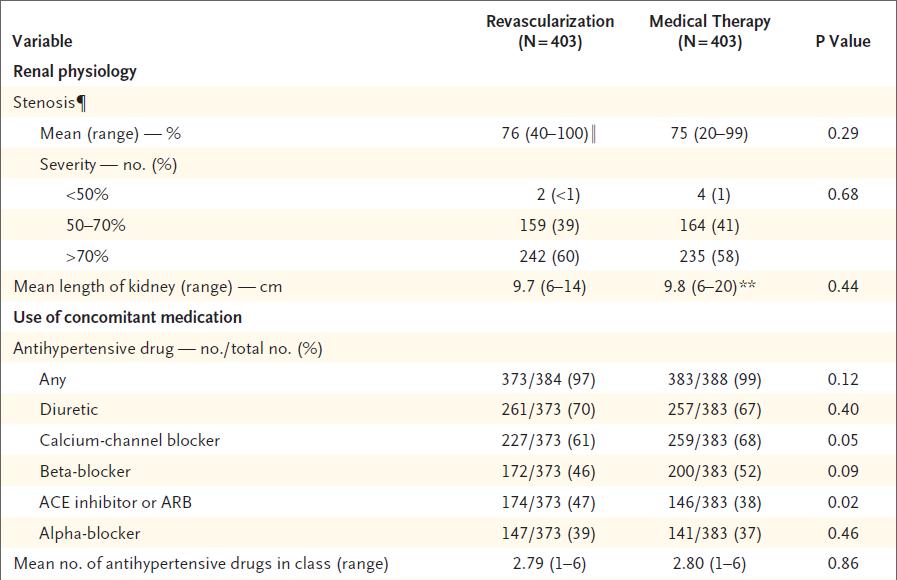
15 PATIENT CHARACTERISTICS
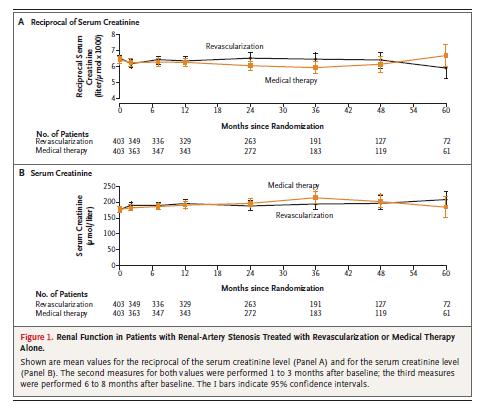
16 RESULTS
17 RESULTS
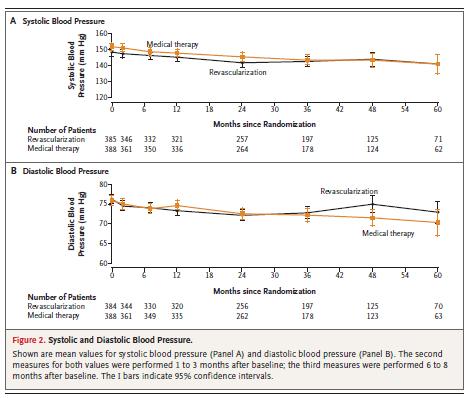
18 EVENTS

19 SURVIVAL
20 CONCLUSIONS- ASTRAL No evidence of a worthwhile clinical benefit in the initial years after revascularization in patients with atherosclerotic renal-artery stenosis. No significant improvements in blood pressure or reductions in renal or cardiovascular events or mortality were seen
21 FOLLOW UP TO ASTRAL Single center observational study Selected 127 pts who underwent intervention b/w not included in ASTRAL Primary end point- rate of decline of gfr before and after revascularization Mean follow up 2.8yrs
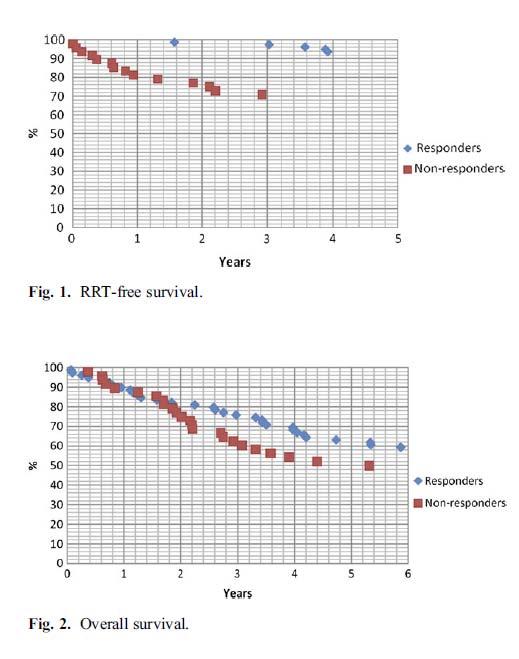
22 RESULTS

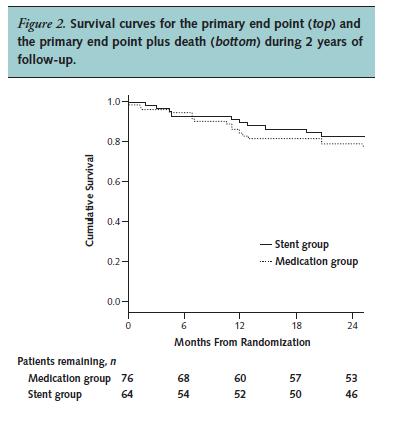
23 STAR TRIAL
24 Primary end point- >20% decline in creatinine clearance Secondary end point- cardiovascular morbidity and mortality Study under powered to provide definite estimate of efficacy
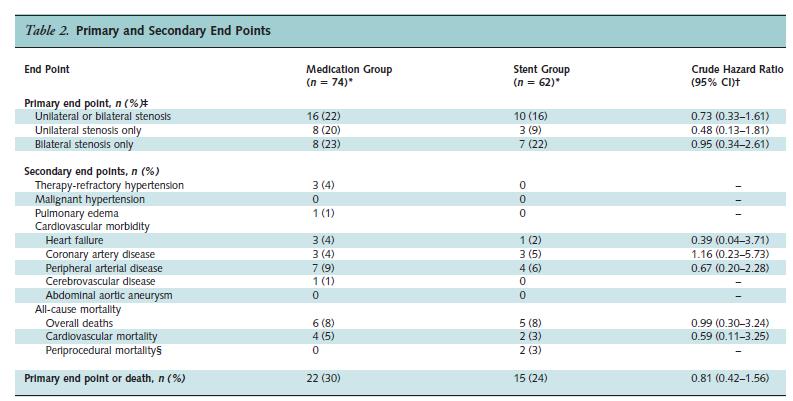
25 RESULTS
26
27 STAR TRIAL- CONCLUSIONS No statistically significant difference in progression of renal failure over 2 years in those treated with stenting and medication compared with those treated with medication only Stent-related complications occurred- 2 procedure-related deaths, 1 death secondary to an infected hematoma and 1 case of deterioration of renal function resulting in dialysis
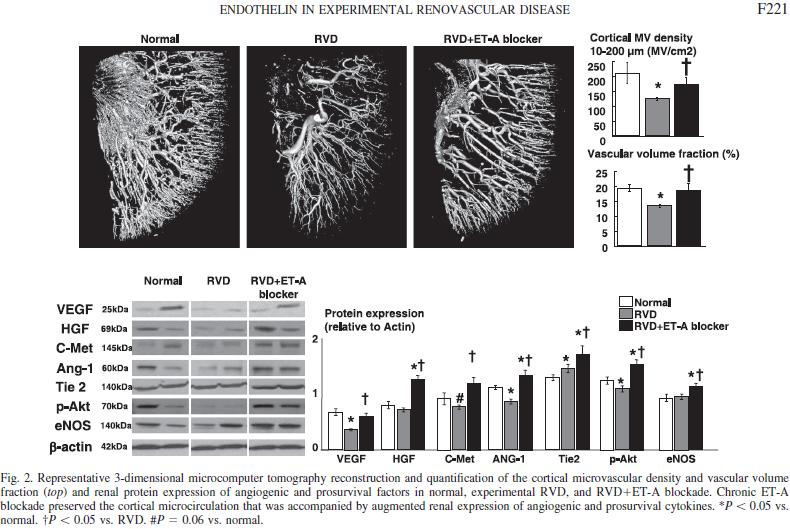
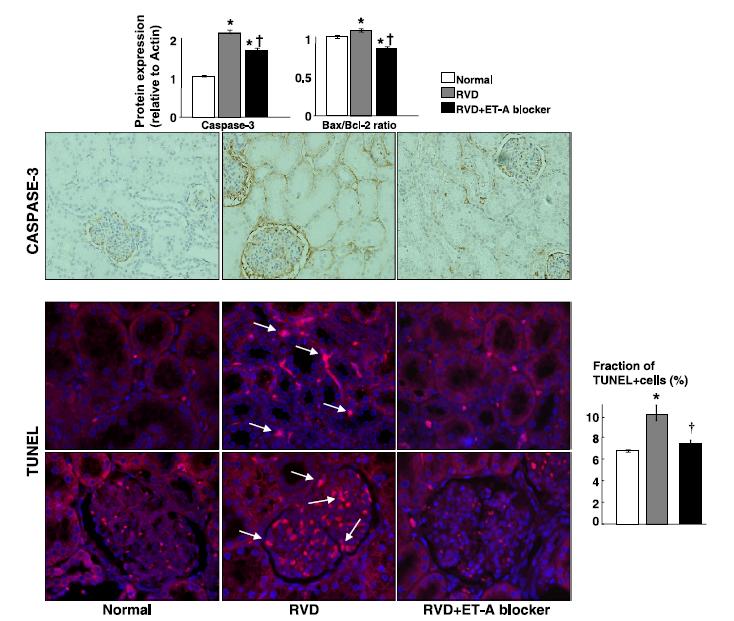
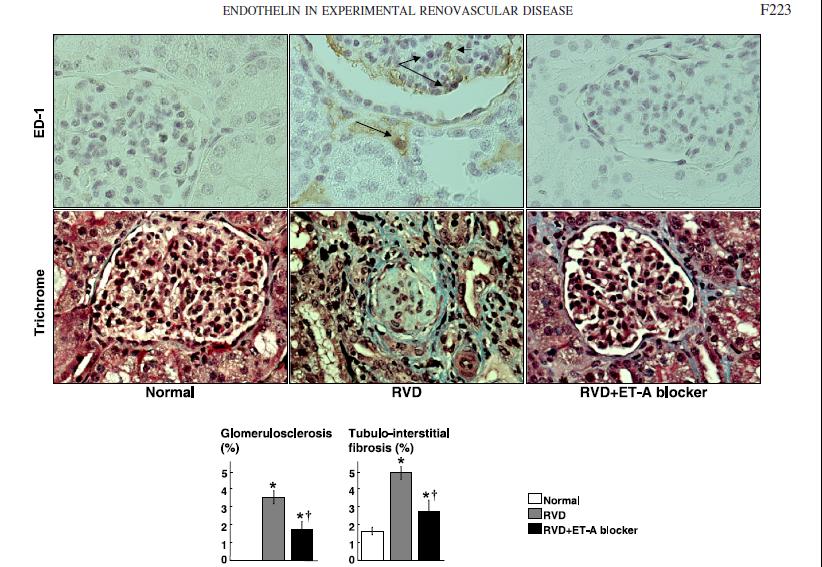
28 WHAT S NEW.. Endothelin A receptor blockade Chronic ET-A receptor blockade would preserve the hemodynamics and function and slow the progression of injury in the stenotic kidney. Underlying mechanisms of renoprotection of ET- A blockade are associated with stimulation of the VEGF and HGF pathway 14 pigs unilateral stenosis induced gradually with coil insertion 7 treated with Endothelin A rp blockade and 7 as control. Also normal animal used as control.
29 RESULTS
30 RESULTS
31
32
33
34 CONCLUSIONS Chronic ET-A blockade preserved the hemodynamics and function of the stenotic kidney despite the similar degree of renal artery stenosis and hypertension in RVD and RVDET-A pigs independent of blood pressure ET-A blockade also augmented renal expression of HGF, a pleiotropic growth factor with robust direct and VEGF-mediated angiogenic effects
35 TRAS Incidence -2-7% 3 main sites - At anastamosis surgical site - Distal site of anastamosis- cause unclear - Multiple stenosis in distal arterial brancheslikely sec to chronic rejection Risk factors- CMV and DGF No change in need of anti- hypertensives post intervention and overall graft survival remains unchanged. Ponticelli et al.transplant International, 2011
36 THANK YOU
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Renal Artery Stenting
 Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10
Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10
Effective Health Care
 Number 5 Effective Health Care Comparative Effectiveness of Management Strategies for Renal Artery Stenosis Executive Summary Background Renal artery stenosis (RAS) is defined as the narrowing of the lumen
Number 5 Effective Health Care Comparative Effectiveness of Management Strategies for Renal Artery Stenosis Executive Summary Background Renal artery stenosis (RAS) is defined as the narrowing of the lumen
Renal Artery Stenosis: Insights from the CORAL Trial
 Renal Artery Stenosis: Insights from the CORAL Trial Christopher J. Cooper, M.D., FACC, FACP Dean and Senior Vice President University of Toledo, College of Medicine President, Ohio Chapter ACC State of
Renal Artery Stenosis: Insights from the CORAL Trial Christopher J. Cooper, M.D., FACC, FACP Dean and Senior Vice President University of Toledo, College of Medicine President, Ohio Chapter ACC State of
Disclosure of Potential Conflicts. Renal Artery Stenosis. RAS Epidemiology. Road Map. Background. ASDIN 7th Annual Scientific Meeting
 Renal Artery Stenosis Disclosure of Potential Conflicts Cytopherx, Inc. R4 Vascular, Inc. Bard Peripheral Vascular Spectranetics, Inc. Alexander S. Yevzlin, MD Associate Professor of Medicine (CHS) ASDIN
Renal Artery Stenosis Disclosure of Potential Conflicts Cytopherx, Inc. R4 Vascular, Inc. Bard Peripheral Vascular Spectranetics, Inc. Alexander S. Yevzlin, MD Associate Professor of Medicine (CHS) ASDIN
PCI for Renal Artery stenosis
 PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
PCI for Renal Artery stenosis Why should we treat Renal Artery Stenosis? Natural History of RAS RAS is progressive disease Study Follow-up (months) Pts Progression N (%) Total occlusion Wollenweber Meaney
Case yr old lady; type 2 Diabetes 10 yrs; PVD; hypertension
 Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
Does this patient have flash pulmonary oedema? Philip A Kalra Professor of Nephrology, Salford Royal Hospital and University of Manchester, UK 73 yr old lady; type 2 Diabetes 1 yrs; PVD; hypertension Acute
MEET /06/2013 SESSION : RENAL AND VISCERAL
 MEET 2003 11/06/2013 SESSION : RENAL AND VISCERAL AFTER 35 YEARS, WHAT ARE THE INDICATIONS AND RESULTS OF PTRA IN PATIENTS WITH RI OR RVH? THOMAS SOS, MD NYPH CORNELL New York, NY THOMAS SOS, MD NYPH CORNELL
MEET 2003 11/06/2013 SESSION : RENAL AND VISCERAL AFTER 35 YEARS, WHAT ARE THE INDICATIONS AND RESULTS OF PTRA IN PATIENTS WITH RI OR RVH? THOMAS SOS, MD NYPH CORNELL New York, NY THOMAS SOS, MD NYPH CORNELL
CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective
 CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective Michael R. Jaff, DO Massachusetts General Hospital Boston, Massachusetts, USA Michael R. Jaff, DO Conflicts of Interest
CORAL Trial Aftermath: What Do We Do Now? Renal Revascularization in Perspective Michael R. Jaff, DO Massachusetts General Hospital Boston, Massachusetts, USA Michael R. Jaff, DO Conflicts of Interest
RENAL ARTERY PTA. JH PEREGRIN IKEM, Prague
 RENAL ARTERY PTA JH PEREGRIN IKEM, Prague PTRA/Stenting PTRA technical success rate > 90 % In some patients helps control hypertension In some patients can improve kidney function Serious complications
RENAL ARTERY PTA JH PEREGRIN IKEM, Prague PTRA/Stenting PTRA technical success rate > 90 % In some patients helps control hypertension In some patients can improve kidney function Serious complications
Renal Intervention. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Consensus Core Set: Cardiovascular Measures Version 1.0
 Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Renal Artery Disease. None > 65,000,000. Learning objectives: Renal Artery Disease
 Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD
 Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
Safety of Single- Versus Multi-vessel Angioplasty for Patients with AMI and Multi-vessel CAD Mun K. Hong, MD Associate Professor of Medicine Director, Cardiovascular Intervention and Research Weill Cornell
RAS Epidemiology. Renal Artery Stenosis. Pathophysiology of RAS. Disclosure of Potential Conflicts. Background Pathophysiology of RAS.
 Renal Artery Stenosis RAS Epidemiology Common Disease Incidence General Population 0.1% Hypertensive Population 4% HTN & Suspected CAD 10-20% Malignant HTN 20-30% Malignant HTN and CKD 30-40% Alexander
Renal Artery Stenosis RAS Epidemiology Common Disease Incidence General Population 0.1% Hypertensive Population 4% HTN & Suspected CAD 10-20% Malignant HTN 20-30% Malignant HTN and CKD 30-40% Alexander
Salvageability of renal function following renal revascularization in children with Takayasu arteritis-induced renal artery stenosis
 Salvageability of renal function following renal revascularization in children with Takayasu arteritis-induced renal artery stenosis Obiagwu P 1, Gajjar P 1, Scott C 1, Numanoglu A 2, McCulloch M, 1 Nourse
Salvageability of renal function following renal revascularization in children with Takayasu arteritis-induced renal artery stenosis Obiagwu P 1, Gajjar P 1, Scott C 1, Numanoglu A 2, McCulloch M, 1 Nourse
Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
 Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 8:87-91, 2010 doi: 10.5049/EBP.2010.8.2.87 Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
Review ISSN 1738-5997 (Print) ISSN 2092-9935 (Online) Electrolyte Blood Press 8:87-91, 2010 doi: 10.5049/EBP.2010.8.2.87 Atherosclerotic Renovascular Hypertension : Lessons from Recent Clinical Studies
In the name of GOD. Animal models of cardiovascular diseases: myocardial infarction & hypertension
 In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
In the name of GOD Animal models of cardiovascular diseases: myocardial infarction & hypertension 44 Presentation outline: Cardiovascular diseases Acute myocardial infarction Animal models for myocardial
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
BEST OF Groupe Vasculaire Thrombose
 BEST OF Groupe Vasculaire Thrombose Serge Kownator (Thionville) Claire Mounier Vehier (Lille) Gérard Helft (Paris) Victor ABOYANS (Limoges) Boris ALEIL (Strasbourg) Serge COHEN (Marseille) Joseph EMMERICH
BEST OF Groupe Vasculaire Thrombose Serge Kownator (Thionville) Claire Mounier Vehier (Lille) Gérard Helft (Paris) Victor ABOYANS (Limoges) Boris ALEIL (Strasbourg) Serge COHEN (Marseille) Joseph EMMERICH
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Masahiko Fujihara, MD
 Verify the efficacy of renal artery stenting to define the predictive factors by physiological assessment with pressure wire gradient VERDICT study Masahiko Fujihara, MD Kishiwada Tokushukai Hospital Osaka,
Verify the efficacy of renal artery stenting to define the predictive factors by physiological assessment with pressure wire gradient VERDICT study Masahiko Fujihara, MD Kishiwada Tokushukai Hospital Osaka,
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Prof. Michael Joannidis Medical Intensive Care and Emergency Unit Department of Internal Medicine Medical University Innsbruck Innsbruck, Austria
 1 di 27 Prevention of AKI: experimental promises and clinical realities Michael Joannidis, Innsbruck, Austria Chairs:Norbert Lameire, Ghent, Belgium Gert Mayer, Innsbruck, Austria Prof. Michael Joannidis
1 di 27 Prevention of AKI: experimental promises and clinical realities Michael Joannidis, Innsbruck, Austria Chairs:Norbert Lameire, Ghent, Belgium Gert Mayer, Innsbruck, Austria Prof. Michael Joannidis
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
TCT mdbuyline.com Clinical Trial Results Summary
 TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
TCT 2012 Clinical Trial Results Summary FAME2 Trial: FFR (fractional flow reserve) guided PCI in all target lesions Patients with significant ischemia, randomized 1:1 Control arm: not hemodynamically significant
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
ASYMPTOMATIC CAROTID STENOSIS WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS
 CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON SURVIVAL PREDICTIONS") WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
WE CAN (AND SHOULD) CHOOSE PATIENTS FOR ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON S ASYMPTOMATIC CAROTID STENOSIS TREATMENT BASED ON DISCLOSURES INDIVIDUAL None A patient with an asymptomatic 90%
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Chapter 2: Identification and Care of Patients With Chronic Kidney Disease
 Chapter 2: Identification and Care of Patients With Chronic Kidney Disease Introduction The examination of care in patients with chronic kidney disease (CKD) is a significant challenge, as most large datasets
Chapter 2: Identification and Care of Patients With Chronic Kidney Disease Introduction The examination of care in patients with chronic kidney disease (CKD) is a significant challenge, as most large datasets
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
Immediate Normalisation of Blood Pressure following Intervention in Functional Total Occlusion of Unilateral Renal Artery with an Atrophic Kidney
 Immediate Normalisation of Blood Pressure following Intervention in Functional Total Occlusion of Unilateral Renal Artery with an Atrophic Kidney Dr Parminder Singh Otaal Assistant Professor Department
Immediate Normalisation of Blood Pressure following Intervention in Functional Total Occlusion of Unilateral Renal Artery with an Atrophic Kidney Dr Parminder Singh Otaal Assistant Professor Department
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital
 VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
VCU Pauley Heart Center: A 2009 US News Top 50 Heart and Heart Surgery Hospital Complex PCI: Multivessel Disease George W. Vetrovec, MD. Kimmerling Chair of Cardiology VCU Pauley Heart Center Virginia
Chapter 4: Cardiovascular Disease in Patients with CKD
 Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
Chapter 4: Cardiovascular Disease in Patients with CKD The prevalence of cardiovascular disease (CVD) was 65.8% among patients aged 66 and older who had chronic kidney disease (CKD), compared to 31.9%
Pre-op Risk Assessment. Hal Blanks MD FACC
 Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Pre-op Risk Assessment Hal Blanks MD FACC Objectives: Identify and manage patients with known or suspected CAD and other cardiac diseases who are at risk of cardiac complications during noncardiac surgery.
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Cardiovascular Disease in CKD. Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center
 Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Cardiovascular Disease in CKD Parham Eftekhari, D.O., M.Sc. Assistant Clinical Professor Medicine NSUCOM / Broward General Medical Center Objectives Describe prevalence for cardiovascular disease in CKD
Chapter 4: Cardiovascular Disease in Patients With CKD
 Chapter 4: Cardiovascular Disease in Patients With CKD Introduction Cardiovascular disease is an important comorbidity for patients with chronic kidney disease (CKD). CKD patients are at high-risk for
Chapter 4: Cardiovascular Disease in Patients With CKD Introduction Cardiovascular disease is an important comorbidity for patients with chronic kidney disease (CKD). CKD patients are at high-risk for
Renal PEI: critical appraisal
 Renal PEI: critical appraisal On Topaz M.D., F.A.C.C.,F.S.V.M. Professor of Medicine & Pathology Director, Interventional Cardiology McGuire Veterans Medical Center Virginia Commonwealth University Richmond,
Renal PEI: critical appraisal On Topaz M.D., F.A.C.C.,F.S.V.M. Professor of Medicine & Pathology Director, Interventional Cardiology McGuire Veterans Medical Center Virginia Commonwealth University Richmond,
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Surgery Grand Rounds
 Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
Surgery Grand Rounds Coronary Artery Bypass Grafting versus Coronary Artery Stenting Charles Ted Lord, R1 Coronary Artery Disease Stenosis of epicardial vessels Metabolic & hematologic Statistics 500,000
03/07/ Background. + High Risk Features Are Prevalent in Dialysis Patients
 + When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
+ When Does Cardiovascular Disease Preclude Consideration of Renal Transplantation? Kul Aggarwal, MD, MRCP (UK), FACC Professor of Clinical Medicine Division of Cardiology University of Missouri & Chief,
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Pre-operative Evaluations. Objectives. General Considerations. FP Consultation Considerations. CV Credits 7/24/2017. Brian Bachelder, MD Akron, Ohio
 Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
Pre-operative Evaluations Brian Bachelder, MD Akron, Ohio Objectives Discuss the perioperative cardiopulmonary evaluation and management of patients undergoing non-cardiac surgery Objectively estimate
RENAL TRANSPLANT PATIENTS WITH HIGH-FLOW AVF: WHEN & HOW TO INTERVENE Stuart Greenstein, MD Abdominal Organ Transplant Division Albert Einstein
 RENAL TRANSPLANT PATIENTS WITH HIGH-FLOW AVF: WHEN & HOW TO INTERVENE Stuart Greenstein, MD Abdominal Organ Transplant Division Albert Einstein College of Medicine Montefiore Medical Center, Bronx, NY
RENAL TRANSPLANT PATIENTS WITH HIGH-FLOW AVF: WHEN & HOW TO INTERVENE Stuart Greenstein, MD Abdominal Organ Transplant Division Albert Einstein College of Medicine Montefiore Medical Center, Bronx, NY
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Contrast-Induced Nephropathy: Evidenced Based Prevention
 Contrast-Induced Nephropathy: Evidenced Based Prevention Michael J Cowley, MD, FSCAI Nothing to disclose Contrast-Induced Nephropathy (CIN) Definitions New onset or worsening of renal function after contrast
Contrast-Induced Nephropathy: Evidenced Based Prevention Michael J Cowley, MD, FSCAI Nothing to disclose Contrast-Induced Nephropathy (CIN) Definitions New onset or worsening of renal function after contrast
Joshua A. Beckman, MD. Brigham and Women s Hospital
 Peripheral Vascular Disease: Overview, Peripheral Arterial Obstructive Disease, Carotid Artery Disease, and Renovascular Disease as a Surrogate for Coronary Artery Disease Joshua A. Beckman, MD Brigham
Peripheral Vascular Disease: Overview, Peripheral Arterial Obstructive Disease, Carotid Artery Disease, and Renovascular Disease as a Surrogate for Coronary Artery Disease Joshua A. Beckman, MD Brigham
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
Renovascular Hypertension and Ischemic Nephropathy: 2018
 Renovascular Hypertension and Ischemic Nephropathy: 2018 2 nd International Renal Conference Brugge, Belgium March, 2018 Stephen C. Textor, M.D. Nephrology and Hypertension Professor of Medicine Mayo Clinic
Renovascular Hypertension and Ischemic Nephropathy: 2018 2 nd International Renal Conference Brugge, Belgium March, 2018 Stephen C. Textor, M.D. Nephrology and Hypertension Professor of Medicine Mayo Clinic
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
SAMMPRIS. Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis. Khalil Zahra, M.D
 SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
A Closer Look: Renal Artery Stenosis. Renal artery stenosis (RAS) is defined as a TOPICS FROM CHEP. Shawn s stenosis
 is defined as a TOPICS FROM CHEP. Shawn s stenosis") TOPICS FROM CHEP A Closer Look: Renal Artery Stenosis On behalf of the Canadian Hypertension Education Program (CHEP), Dr. Tobe gives an overview of renal artery stenosis, including the prevalence, screening
TOPICS FROM CHEP A Closer Look: Renal Artery Stenosis On behalf of the Canadian Hypertension Education Program (CHEP), Dr. Tobe gives an overview of renal artery stenosis, including the prevalence, screening
Endovascular treatment
 210..217 NEPHROLOGY 2010; 15, S210 S217 doi:10.1111/j.1440-1797.2009.01243.x Endovascular treatment Date written: February 2009nep_1243 Final submission: August 2009 Authors: Robert MacGinley, Subramanian
210..217 NEPHROLOGY 2010; 15, S210 S217 doi:10.1111/j.1440-1797.2009.01243.x Endovascular treatment Date written: February 2009nep_1243 Final submission: August 2009 Authors: Robert MacGinley, Subramanian
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY
 SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
SANWICH TECHNIQUE TO REDUCE COMPLICATIONS WHEN TREATING BILATERAL INTERNAL ILIAC ARTERY TRAN TRA GIANG.MD Interventional cardiovascular department Hanoi Heart Hospital, Hanoi, Viet Nam Nothing to Disclose
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Diabetic Kidney Disease: Update. GKA Master Class. Istanbul 2011
 Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Diabetic Kidney Disease: Update GKA Master Class Istanbul 2011 DKD: Challenging dogmas Old Dogmas Type 1 and Type 2 DN have the same natural history Microalbuminuria is an early stage of DN Tight Glycemia
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines
 Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Evidence-Based Management of CAD: Last Decade Trials and Updated Guidelines Enrico Ferrari, MD Cardiac Surgery Unit Cardiocentro Ticino Foundation Lugano, Switzerland Conflict of Interests No conflict
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Update in Nephrology. Case: Question 1. Case presentation. Acute Kidney Injury. For her hypertension management, you decide to:
 Update in Nephrology Chronic Kidney Disease Renoprotection and Proteinuria, ACE and/or ARB Anemia management Update in Nephrology Renal artery stenosis Nephrogenic systemic fibrosis Division of Nephrology
Update in Nephrology Chronic Kidney Disease Renoprotection and Proteinuria, ACE and/or ARB Anemia management Update in Nephrology Renal artery stenosis Nephrogenic systemic fibrosis Division of Nephrology
University of Groningen. Acute kidney injury after cardiac surgery Loef, Berthus Gerard
 University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT
 FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
FFR vs icecg in Coronary Bifurcations FIESTA ClinicalTrials.gov Identifier: NCT01724957 Dobrin Vassilev MD, PhD Assoc. Prof. in Cardiology Head Cardiology Clinic, Alexandrovska University Hospital Medical
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Revascularization of swine renal artery stenosis improves renal function but not the changes in vascular structure
 http://www.kidney-international.org & 21 International Society of Nephrology Revascularization of swine renal artery stenosis improves renal function but not the changes in vascular structure Frederic
http://www.kidney-international.org & 21 International Society of Nephrology Revascularization of swine renal artery stenosis improves renal function but not the changes in vascular structure Frederic
Takayasu disease Is it still a room for intervention? NO YES. BUT
 Takayasu disease Is it still a room for intervention? NO YES. BUT Z. Tazi Mezalek Internal Medicine Department Mohammed V University Ibn Sina Hospital - Rabat - Maroc Disclosure Speaker name: TAZI MEZALEK
Takayasu disease Is it still a room for intervention? NO YES. BUT Z. Tazi Mezalek Internal Medicine Department Mohammed V University Ibn Sina Hospital - Rabat - Maroc Disclosure Speaker name: TAZI MEZALEK
Ischemic Heart Disease Interventional Treatment
 Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Ischemic Heart Disease Interventional Treatment Cardiac Catheterization Laboratory Procedures (N = 11,61) is a regional and national referral center for percutaneous coronary intervention (PCI). A total
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Postoperative monitoring after
 Postoperative monitoring after kidney transplantation Bundit sakulchairungrueng,md Vascular and Transplantation Unit Faculty of Medicine Ramathibodi Hospital Mahidol University Reference Introduction A
Postoperative monitoring after kidney transplantation Bundit sakulchairungrueng,md Vascular and Transplantation Unit Faculty of Medicine Ramathibodi Hospital Mahidol University Reference Introduction A
Management of stable CAD FFR guided therapy: the new gold standard
 Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
Management of stable CAD FFR guided therapy: the new gold standard Suleiman Kharabsheh, MD Director; CCU, Telemetry and CHU Associate professor of Cardiology, Alfaisal Univ. KFHI - KFSHRC Should patients
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone