Prevention and Management of hypertensive stroke. Content. What are the clinical and radiological manifestations for HT-related stroke?
|
|
|
- Elijah Lang
- 6 years ago
- Views:
Transcription

1 Prevention and Management of hypertensive stroke Dr. LO, Man-wai MBChB (CUHK) MRCP (UK) MPH (CUHK) FHKCP FHKAM (Medicine) Specialist in Neurology Dept. of Medicine Queen Elizabeth Hospital 4 Dec 2006 Content How does HT cause stroke? What are the clinical and radiological manifestations for HT-related stroke? How should we lower BP in acute stroke? What is the current concepts in anti- hypertensive therapy for prevention of first and recurrent stroke? 1

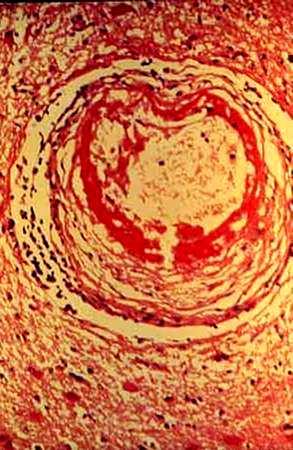
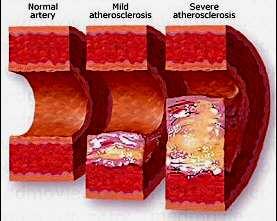
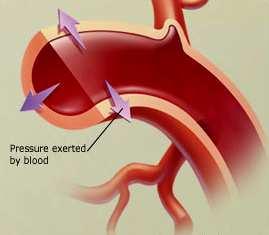
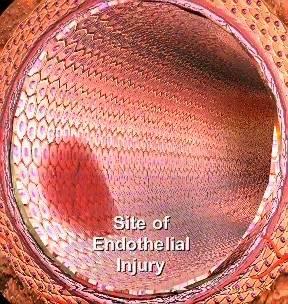
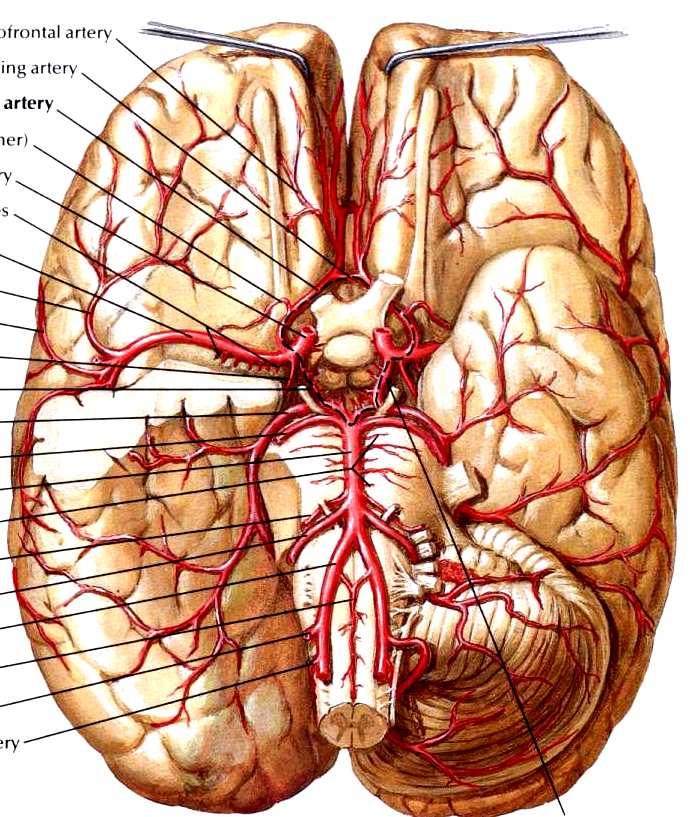
2 How does HT cause stroke? Lipohyalinosis Fibrinoid degeneration Atherosclerosis 2
3 3

4 4


5 Cortical infarction MCA territory infarction 5




6 ACA territory infarction PCA territory infarction 6


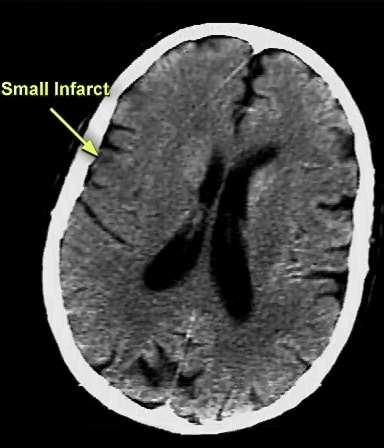
7 ACA MCA PCA Lacunar Infarct 7

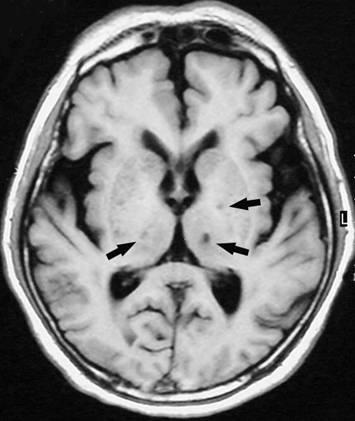
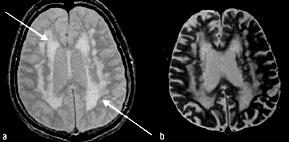
8 Lacunar Infarct Binswanger s disease 8
9 Binswanger s disease Subcortical arteriosclerotic encephalopathy Chronic small vessel disease Vascular parkinsonism Lower half parkinsonism Binswanger s disease Apathy Gait apraxia Small step gait Hyperreflexia Extensor plantar reflexes Subcortical dementia cognitive slowing 9
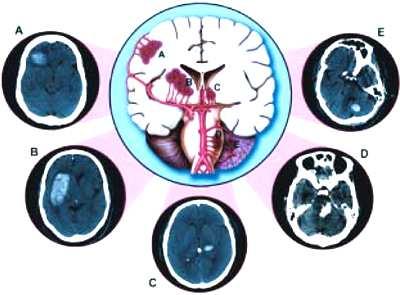
10 Cardioembolic stroke hypertensive hemorrhage 10


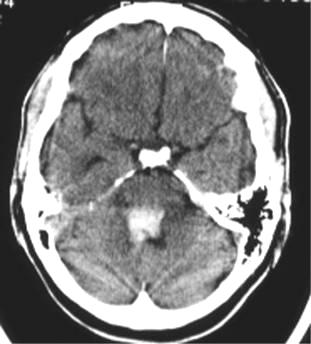

11 Basal ganglia haemorrhage Pontine haemorrhage 11


12 Cerebellar haemorrhage Subarachnoid haemorrhage 12


13 SAH Antiplatelet agents Aspirin small benefit in reducing the death and recurrent stroke rate net decrease of 9 deaths or occurrences of further stroke per 1000 patients (level Ia) 13

14 IV thrombolysis FDA approval 1996 iv tpa <3 hr improved outcome at 3 months NINDS TPA-treated group were at least 30% more likely to have minimal or no disability at 3 months Benefit were consistent regardless of age, stroke subtype or prior use of aspirin 14
 Mortality rate in both")
15 6.4% tpa vs. 0.6% in placebo (within 36hrs) Mortality rate in both treatment group was similar at 3mo & at 1 year 15




16 Intra-arterial arterial thrombolysis MERCI balloon guide catheter FDA August 11, st medical device specifically indicated to - retrieve blood clots from the brain in ischemic stroke for - patients who fail or are ineligible for iv tpa 16

17 BP lowering in acute phase Ischaemic penumbra 17

18 Ischaemic penumbra Cerebral autoregulation 18
19 Cerebral autoregulation CBF Normotensive patient Hypertensive patient Mean arterial BP BP management in acute ischaemic stroke CBF is pressure dependent in ischaemic brain regions Further reduction irreversibly injure the ischaemic penumbra increase stroke volume 19
20 BP management in acute ischaemic stroke Transient HT common after acute ischaemic stroke Causes: anxiety pain neuroendocrine factors stroke location compensatory response to brain hypoxia or increased ICP BP management in acute ischaemic stroke Manage stress responses, pain, nausea and vomiting, bladder distension or other sources of anxiety Early BP elevations often decline spontaneously during the first minutes to hours May not require pharmacologic Rx 20
21 Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome Castillo J, Leira R, Garcia MM, Serena J, Blanco M, Davalos A. Stroke Feb;35(2): Epub 2004 Jan 15. Power Grade 3/5 Power Grade 1/5 Anti-HT Drug for BP 180/90 21
22 Stroke in evolution? Non-specific Failure of collateral circulation Systemic hypotension Cardiac arrthymia Embolization or propagation of thrombus Progressive occlusion of vessel lumen Psychological depression Sepsis Seizures Any conditions deserve BP lowering? AMI Aortic dissection Hypertensive encephalopathy Severe left heart failure Post-thrombolysis 22
23 Consensus for BP Mx (not eligible for thrombolysis) SBP <220 mm Hg or DBP <120 mm Hg SBP >220 mm Hg or DBP mm Hg DBP >140 mm Hg Observe BP unless end organ involvement Labetalol OR nicardipine (target 10% 15% 15% reduction) Sodium nitroprusside 0.5 µm/kg per min IV with continuous BP monitoring (target 10% 15% 15% reduction) Guidelines for the Early Management of Patients With Ischemic Stroke Stroke. 2003;34:1056 Resume previous anti-ht Rx? Those already taking anti-ht Rx: Resume drugs to avoid rebound HT Maintain: SBP mm Hg DBP < 120 mm Hg 23
24 Labetolol Selective α 1 antagonist ß 1 & ß 2 antagonist Decrease systemic vascular resistance through α blockade Beta-blocking reflex tachycardia induced by vasodilatation Labetolol Does not affect cerebral blood flow Dosing regimen 10-20mg iv (over min) every 15-20min Doubing of each subsequent dose is recommended 24
25 Sublingual Nifedipine Should be avoided Cause precipitous reduction in BP X Adalat 5mg S.L. stat Bring home message: Don t t lower BP in acute ischaemic stroke if SBP <220 mm Hg or DBP <120 mm Hg 25
26 Managing HT in ICH limited observational data no data from randomized clinical trials left with consensus opinion and our best judgement balancing the two competing issues: Rebleeding Secondary brain injury BP lowering to limit hematoma expansion, non- nervous system organ injury AHA Scientific Statement Guidelines for the Management of Spontaneous ICH Stroke. 1999;30: SBP >230 mm Hg DBP >140 mm Hg on 2 readings 5 minutes apart SBP 180 to 230 mm Hg DBP 105 to 140 mm Hg or MAP 130 mm Hg on 2 readings 20 minutes apart SBP <180 mm Hg DBP <105 mm Hg If ICP monitoring is present Nitroprusside IV labetalol, esmolol, enalapril Observe Keep cerebral perfusion pressure > 70mmHg 26

27 Primary prevention 27
28 Risk factors for stroke Non-modifiable Modifiable Non-white ethnicity Male sex Older age Positive family history HT Smoking Excessive alcohol intake (>60g/d) Obesity Dyslipidaemia DM Carotid artery disease AF CHF Blood Pressure and Stroke: An Overview of Published Reviews Carlene M.M. Lawes,, Derrick A. Bennett, Valery L. Feigin,, and Anthony Rodgers Stroke :

29 BP level & risk of vascular disease JNC VII Risk begins at 115/75 mmhg No limits below this point No J-curve J response Classification of BP by JNC 7 SBP Stage 2 HT Stage 1 HT Prehypertension Normal DBP 29

30 Which drug should we use? Any class effect? Comparison with placebo Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomized trials. Lancet. 2003;362:

31 Direct comparison between anti-ht regimen Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomized trials. Lancet. 2003;362: Size does matter Size (intensity) of BP Type of anti-ht Rx 31

32 Compelling reasons & recommendations Diuretic B-blocker ACEI ARB CCB Aldosterone Antagonist CHF Post-MI High CHD risk DM CRF Recurrent CVA 32
33 SBP Stage 2 HT Stage 1 HT Prehypertension Normal DBP Lifestyle modification Compelling indications? Y treat SBP Stage 2 HT Stage 1 HT Prehypertension Normal DBP Lifestyle modification Treat with thiazide ACEI, ARB, BB, CCB, or combination 33


34 SBP Stage 2 HT Stage 1 HT Prehypertension Normal DBP Lifestyle modification 2 drugs combinations Thiazide + ACEI/ARB/BB/CCB Central Pontine Myelinolysis 34

35 What are the risk factors for thiazide induced hyponatremia? Age Low body mass Hypokalemia Risk factors for thiazide-induced induced hyponatraemia. K.M. Chow, C.C. Szeto,, T.Y.-H. Wong, C.B. Leung P.K.-T. Li Q J Med 2003; 96: Stroke prevention in Diabetics 40 60% adult with type 2 DM have HT Any difference in BP management for this special group of patients to prevent stroke? 35
36 % relative risk reduction UKPDS Event Rates for Select Endpoints With Tight vs Less Tight Blood Pressure Control Events per 1000 patient yrs P=0.005 Any DM-related endpoint P=0.02 P=0.01 P=0.009 DMrelated death Tight (n=758) mean achieved BP 144/82 mmhg Less tight (n=390) mean achieved BP 154/87 mmhg Stroke Microvascular complications UKPDS Group. BMJ. 1998;317: UKPDS Relative Risk Reduction for Intensive vs Less Intensive Glucose Control P< P< P= P=0.05 P= Microalbuminuria at 12 yrs Retinopathy Any DM endpoint Microvascular complications Myocardial Infarction Over 10 years, HbA 1c was 7.0% ( ) in the intensive group (n=2,729) compared with 7.9% ( ) in the conventional group (n=1,138). UKPDS Group. Lancet. 1998;352:
37 UKPDS Findings: Tight BP Control vs. Intensive Glucose Control Tight vs. Less tight BP control reduces risk of Any diabetes-related endpoint 24% P=0.005 Microvascular complications 37% P=0.009 Stroke 44% P=0.01 Intensive vs. Conventional glucose control policy reduces risk of Any diabetes-related endpoint 12% P=0.03 Microvascular complications 25% P<0.01 Myocardial infarction 16% P=0.05 UKPDS Group. BMJ. 1998;317: UKPDS Group. Lancet. 1998;352: Is ACEI/ARB better for diabetics?? Angiotensinogen Non-renin (eg tpa) Renin Angiotensin I Bradykinin Non-ACE (eg chymase) ACE Angiotensin II Inactive peptides AT 1 AT 2 ATn 37
38 ABCD, CAPPP, FACET and UKPDS Meta-Analysis Is ACEI superior to other agents in the prevention of cardiovascular events in hypertensive type 2 diabetics? Size ACEI Others ABCD 470 enalapril nisoldipine CAPPP 572 captopril Diuretic or BB FACET 380 fosinopril amlodipine UKPDS 758 captopril atenolol Pahor M, et al. Diabetes Care. 2000;23: Relative Risk Reduction With ACEIs in ABCD, CAPPP and FACET % relative risk reduction 0 AMI CVS Event All-cause Stroke Mortality NS P< P< P=0.01 Pahor M, et al. Diabetes Care. 2000;23:
39 MICRO-HOPE substudies of DM patients Ramipril (n = 3,577) Events per patient group (%) RR=25% P<0.001 Combined primary endpoint* RR=33% P=0.007 Stroke Placebo RR=22% P=0.01 Myocardial infarction Ramipril RR=37% P<0.001 Cardiovascular death *The occurrence of myocardial infarction, stroke or cardiovascular death HOPE Study Investigators. Lancet. 2000;355: LIFE Study Diabetes Subgroup (Lorsartan) Endpoints No. of events P value Adjusted hazard ratio (95% CI) Composite CV Death Stroke 116 NS 21% Myocardial infarction 91 NS Total Mortality Favors 1 Favors 1.5 losartan atenolol Lindholm LH, et al. Lancet. 2002;359:

40 Implications Tight control of HT with ACEI or ARB treatment reduces the risk of stroke in persons with DM Glycemic control reduces microvascular complications, but evidence showing a reduction in stroke risk with tight glycemic control is lacking ASA/AHA 2006 recommendation Primary stroke prevention for Diabetics Tight BP control Keep BP < 130/ 80 mmhg Consider ACEI/ ARB 40

41 Case scenerio Chan Tai Man M/52 BP 145/ 85 p70 Hstix 2hr pp 16.3 Hypertension Primary Prevention x Stroke x Stroke Secondary Prevention 41
42 ACEI for 2 nd stroke prevention? HOPE Ramipril vs. Placebo for 1013 patients with Hx of stroke/tia 24% RR (95% CI, 5 40) stroke, MI or vascular death; (n =1013) BP lowering 3/2mm Hg (Office BP) HOPE substudy (Ambulatory BP) 10/4 mmhg reduction over 24hr 17/8 mmhg reduction during nighttime BP lowering effect leading to stroke risk reduction? Comparative Effects of Ramipril on Ambulatory and Office Blood Pressures Per Svensson; Ulf de Faire; Peter Sleight; Salim Yusuf; Jan Östergren Hypertension. 2001;38:e28 PROGRESS (perindopril) N = 6105 Hx of stroke or TIA ACEI, ACEI + indapamide Recurrent CVA: 43% RRR (95% CI 30 54); 12/5 mmhg Recurrent major CVS events: 40% RRR (95% CI 29 49) No benefit when ACEI was given alone Benefit also shown in normotensive patients PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. Lancet. 2001;358:

43 AHA/ ASA Guideline 2006 Secondary Prevention of Stroke All patients with ischaemic stroke or TIA Anti-HT Rx How much? Benefit seen in reduction of ~10/5 mmhg Normal BP < 120/80 mmhg by JNC-7 43

44 AHA/ ASA Guideline 2006 Secondary Prevention of Stroke Which drug? Optimal regimen uncertain Available data support: Diuretic Diuretic + ACEI Individualized with patient characteristics Key message Benefit for HT Rx is clear Choice of agent must be individualized Reduction of BP is generally more important than specific agent Size does matter! 44
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Managing Hypertension in the Perioperative Arena
 Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Managing Hypertension in the Perioperative Arena Optimizing Perioperative Management Strategies for Hypertension in the Cardiac Surgical Patient Objectives: Treatment of hypertensive emergencies. ALBERT
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE
 BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
BLOOD PRESSURE MANAGEMENT IN THE ACUTE PHASE Ελένη Κορομπόκη, MD, PhD, FESO Α Νευρολογική Κλινική, ΕΚΠΑ, Αιγινήτειο Νοσοκομείο Κλινική Ερευνήτρια, Department of Stroke Medicine, Imperial College London,
Disclosures. Hypertension: Nationwide Dilemma. Learning Objectives. What s Currently Recommended? Specific Concerns 3/9/2012
 How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
How Should We ACCOMPLISH Good Blood Pressure Control In Our VETS? Disclosures No conflicts of interest to disclose Updates in the Management of HypertensionIn the Elderly Antoine T. Jenkins, Pharm.D.,
Are Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Especially Useful for Cardiovascular Protection?
 EVIDENCE-BASED CLINICAL MEDICINE Are Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Especially Useful for Cardiovascular Protection? Hean Teik Ong, FRCP, FACC, FESC Purpose:
EVIDENCE-BASED CLINICAL MEDICINE Are Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers Especially Useful for Cardiovascular Protection? Hean Teik Ong, FRCP, FACC, FESC Purpose:
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS. Prevention of Stroke Evidence Tables Blood Pressure Management
 CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Blood Pressure Management Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE Writing Group 2017 Heart and Stroke Foundation September
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS Blood Pressure Management Wein T, Gladstone D (Writing Group Chairs) on Behalf of the PREVENTION of STROKE Writing Group 2017 Heart and Stroke Foundation September
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
BLOOD PRESSURE-LOWERING TREATMENT
 BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Dysglycaemia and Hypertension. Dr E M Manuthu Physician Kitale
 Dysglycaemia and Hypertension Dr E M Manuthu Physician Kitale None Disclosures DM is MI equivalent MR FIT Objective was to assess predictors of CVD mortality among men with and without diabetes and
Dysglycaemia and Hypertension Dr E M Manuthu Physician Kitale None Disclosures DM is MI equivalent MR FIT Objective was to assess predictors of CVD mortality among men with and without diabetes and
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia?
 2012. 4. 20-21 춘계심장학회 _ 부산 Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia? Jeong Bae Park, MD, PhD Cardiology, Cheil General Hospital, Kwandong University, Seoul, Korea The Pulse : revived
2012. 4. 20-21 춘계심장학회 _ 부산 Can Anti-hypertension Therapy Reverse Vascular Aging and Dementia? Jeong Bae Park, MD, PhD Cardiology, Cheil General Hospital, Kwandong University, Seoul, Korea The Pulse : revived
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
GOING BEYOND HYPERTENSION CONTROL
 From bench to practice: hypertension control GOING BEYOND HYPERTENSION CONTROL Prof. Dr. Maria DOROBANTU, FESC,FACC CAROL DAVILA UNIVERSITY OF MEDICINE OF BUCHAREST EMERGENCY HOSPITAL OF BUCHAREST, CARDIOLOGY
From bench to practice: hypertension control GOING BEYOND HYPERTENSION CONTROL Prof. Dr. Maria DOROBANTU, FESC,FACC CAROL DAVILA UNIVERSITY OF MEDICINE OF BUCHAREST EMERGENCY HOSPITAL OF BUCHAREST, CARDIOLOGY