New updates on Hypertension and Heart Failure 2015 Yiu Kai Hang
|
|
|
- Owen Ellis
- 6 years ago
- Views:
Transcription
1 New updates on Hypertension and Heart Failure 2015 Yiu Kai Hang MD, MBBS, MRCP, FHKCP, FHKAM, FRCP (Edin) Clinical Associate Professor Cardiology Division, Department of Medicine, HKU Honorary Consultant, QMH Honorary Consultant, HK Sanatorium Hospital
2 New updates on Hypertension




3 Guidelines for Hypertension Management 2003 JNC JNC ESH/ESC 2013 AHA/ACC/DCD 2013 CHEP 2012KDIGO NICE Chinese Guideline for HT 2009ESH/ESC
4
5 What is the target?
6 Revisit the JNC 7 guidelines Blood pressure goal: <140/90 mmhg for most patients <130/80 mmhg for patients with DM/CKD
7 JNC8: BP goal for elderly patients Age, mmhg All cause mortality Heart failure Stroke CHD 60,<150 (HYVET) (SHEP,HYVET) (Syst-eur,SHEP, HYVET) (Syst-eur,SHEP) BP goal 80,< ,<150 (HYVET) (Syst-eur,SHEP) ,<140 (JATOS VALISH) (JATOS VALISH) (JATOS VALISH) (JATOS VALISH) :agree; :disagree - :N/A Note: # HYVET was stopped early because of a 21% reduction in mortality in the active treatment group. If the study had not been stopped early, the reduction in fatal or non fatal stroke may have been significant by the end of the trial. ; *EWPHE: an 11% reduction in non fatal cerebrovascular events at one year (p <0.05) and a 32% non significant decrease (p = 0.16) in cerebrovascular mortality at the end of the trial In elderly 60,lower the SBP to<150mmhg is associated with statistically significant improvement in CCV outcome BP goal for elderly patients: < 150/90 mmhg
8 JNC 8: BP goal for patients with CKD Age,mmHg GFR ESRD CCV event Mortality BP goal <70 (CKD subgroup) <130/80 vs <140/90 (AASK MDRD REIN-2) (AASK MDRD REIN-2) (AASK) (AASK) <70 (proteinurea subgroup) <130/80 vs <140/90 (AASK* MDRD # ) (AASK REIN-2) :agree; :disagree - :N/A Note: # MDRD:proteinurea>3g/24hr group ; *AASK:proteinurea>300mg/d group vs <300mg/d group In adults <70 years with CKD, the evidence is insufficient to determine if there is a benefit in mortality or CCV outcomes with antihypertensive drug therapy to a goal <130/80mmHg compared with <140/90mmHg BP goal for patients with CKD: < 140/90 mmhg
9 JNC 8: BP goal for diabetes Age, mmhg All-cause mortality DM related endpoints Heart failure stroke CHD Diabetes <150 (Syst-Eur UKPDS SHEP) (UKPDS) _ (Syst-Eur UKPDS) (SHEP) BP goal Diabetes <120 vs <140 50years with diabetes <80 vs <90 _ (ACCORD) (ACCORD) _ (ACCORD) (HOT) (ACCORD) (HOT) diabetes* <80 vs <90 (ABCD hypertension) (HOT UKPDS) :agree; :disagree - :N/A Note: *diabetes subgroup:sbp: mmhg or DBP:80-89mmHg or hypertensive patients In absence of RCTs addressed whether treatment to an SBP goal < 140 mm Hg compared with <150mmHg improves health outcomes in adults with diabetes and hypertension, the panel recommends BP goal for patients with DM: < 140/90 mmhg

10 JNC 8: more lenient systolic blood pressure goal Treat to 150/90 in patients aged over 60 and 140/90 for everybody else.
11 Which drug?

12 Revisit the JNC 7 guidelines Preferred initial therapy: Thiazide-type diuretics

13 JNC 8: no preference among initial drugs General population CKD presented Diuretics is no longer the single best initial drug. New guideline recommends: No preference among the 4 initial drugs: thiazide diuretic, ACEI, ARB and CCB. For black patients: CCB or diuretics should be recommended. For CKD patients: ARB or ACEI should be included to improve kidney outcome.


14 Guideline Comparisons of Goal BP and Initial Drug Therapy for Adults With Hypertension
15 Single or combination therapy?
16 Revisit the JNC 7 guidelines Strategy to dose: Optimize the first agent before adding the second agent

17 JNC8: If goal BP is not reached within 1 month, adjust the treatment regimen until goal is reached The main objective of hypertension treatment is to attain and maintain BP goals! If BP goal is not achieved within 1 month: Increase dose of initial drug Start combination therapy Either separate of single pill Destination is important and not the journey!
,two")

, titrate and/or add drug from different class BP at goal?")


18 2013 AHA/ACC/CDC: initiation of combination therapy in patients at stage 2 hypertension SBP>160mmHg or DBP>100mmHg (stage 2 hypertension),two drugs preferred lifestyle modification and thiazide and ACEI /ARB or CCB or consider ACEI and CCB Recheck and review readings in 2-4 weeks* NO Thiazide for most patients or ACEI ARB CCB or combo If currently on BP med(s), titrate and/or add drug from different class BP at goal? YES Recheck and review readings in 2-4 weeks* BP at goal? No Optimize dosage or add medications Address adherence, advise on selfmonitoring, and request readings from home and other settings Consider secondary causes Yes observation Consider referral to HTN specialist Go AS, et al. Hypertension Nov 15.
19 Why combination? There is a need for multiple agents to achieve target SBP goals Trial (SBP achieved) ASCOT-BPLA (136.9 mmhg) ALLHAT (138 mmhg) IDNT (138 mmhg) RENAAL (141 mmhg) UKPDS (144 mmhg) ABCD (132 mmhg) MDRD (132 mmhg) HOT (138 mmhg) AASK (128 mmhg) Bakris et al. Am J Med 2004;116(5A):30S 8; Dahlöf et al. Lancet 2005;366: Number of medications
20 SBP<140mmHg patients(%) Most patients cannot achieve their BP goal with monotherapy A randomized, parallel, cross-over designed study to evaluate proportion of patient who achieve SBP < 140 mmhg with different monotherapy Efficacy in elderly patients whose BP is un-controlled 100% 80% 60% 40% 20% 17% 18% 23% 27% 0% β-blocker ACEI Diuretics CCB Morgan TO, et al. AJH. 2001;14:
21 Blood Pressure has Multiple Regulatory Pathways Hypertension: a multi-factorial disease Patient 1 Patient 2 Patient 3 Sympathetic nervous system Renin-angiotensin system Total body sodium B. Waeber, March 2007

22 Initial SPC vs. Sequential Add-on Sequential add-on A A+D Initial combination A/D Sympathetic nervous system b-blockers Renin-angiotensin system/vasoconstriction Total body sodium BP = SV x HR x TPR Salt reduction, CCB, diuretics More effective More sustainable Fewer side effects Better compliance ACE-I, ARB, DRI,
23 Which combination?

24 Which combination preferred? Recommendation from ESH/ESC 2013 guidelines: possible but less well tested combination useful combination with some limitation preferred combinations not recommended combination
25 ESH/ESC 2013 guidelines: Drug to be preferred in specific conditions Condition drug ARB CCB Diuretic ACEI BB Asymptomatic organ damage LVH Asymptomatic atherosclerosis Microalbuminuria Renal dysfunction Clinical CV events Previous stroke Previous myocardial infarction Angina pectoris Heart failure Aortic aneurysm Atrial fibrillation, prevention Atrial fibrillation, ventricular rate control # ESRD/proteinuria Peripheral artery disease Other ISH (elderly) Metabolic syndrome Diabetes mellitus Pregnancy Methyldopa Blacks
26 Which combination preferred? Recommendation from NICE 2011 guidelines: <55 years 55 years or black patients at any age Step 1 ACEI / ARB CCB Step 2 ACEI / ARB + CCB Step 3 ACEI / ARB + CCB + diuretic Step 4 Add further diuretic therapy, α-blocker, or β-blocker. Consider seeking specialist advice National Institute for Health and Clinical Excellence (NICE) (2011) Hypertension: Hypertension: Clinical management of primary hypertension in adults London: NICE. Available from
27 Low-dose CCB ARB therapy is efficacious in getting patients to BP goal (<140/90 mmhg) Patients achieving BP goal (%) * N=137 0 CCB ARB CCB + ARB *p<0.05 vs CCB and ARB alone Andreadis et al. J Hum Hypertens 2005;19:491 6
28 Significantly smoother BP variation and higher trough-to-peak ratio with low-dose CCB ARB BP (mmhg) variability :00 AM :00 12:00 AM PM *p<0.05 vs CCB and ARB alone Values in boxes represent trough-to-peak ratio Andreadis et al. J Hum Hypertens 2005;19:491 6 CCBs ARBs CCB + ARB 2:00 PM 4:00 PM 0.950* :00 PM 8:00 PM 10:00 PM 12:00 AM 2:00 AM 4:00 AM Variability in blood pressure itself has detrimental effects Fluctuating BP signals high risk 6:00 AM
29 Safety profile of different ARBs ARB LVH HF MI/CAD High Risk HT DN IGT Losartan LIFE ELITE OPTIMAL RENAAL Valsartan VaHeFT VALIANT VALUE MARVAL NAVIGATOR Irbesartan IDNT/IRMA Candesartan CHARM CALM Telmisartan ONTARGET/TR ASCEND* Omesartan ROADMAP VaHeFT Valsartan Heart Failure Trial /VALIANT Valsartan in Acute Myocardial Infarction Trial CHARM Candesartan in Heart failure Assessment of Reduction in Mortality and Morbidity OPTIMAL Optimal Trial In Myocardial Infarction with Angiotensin II Antagonist Losartan/ RENAAL Reduction of Endpoints in NIDDM with Ang II Antagonist Losartan MARVAL Microalbuminuria Reduction with Valsartan trial IDNT and IRMA Irbesartan Diabetic Nephropathy Trial & IRbesartan microalbuminuric DM in HT CALM Candesartan And Lisinopril Microalbumiuria ONTARGET The ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial Telmisartan Randomised Assessment Study in ACE-Intolerant Subjects with Cardiovascular Disease* NAVIGATOR - Nateglinide and Valsartan in Impaired Glucose Tolerance Outcomes Research
30 Amlodipine/Valsartan has superior BP-lowering efficacy compared with monotherapies 0 Amlodipine 10 mg Valsartan 160 mg Amlodipine/Valsartan 10/160 mg N=42 Change from baseline in systolic BP (mmhg) 23.5 * *p<0.001 vs monotherapies Mild-to-moderate HTN = DBP >95 and <110 mmhg Fogari et al. J Hypertens 2006;24(Suppl 4):S34
31 Amlodipine/Valsartan: appropriate BP reductions across all grades of hypertension Mean change in mean sitting SBP from baseline (mmhg) 0 10 Mild HTN 1 (DBP mmhg SBP mmhg) n=69 Moderate HTN 1 (DBP mmhg SBP mmhg) n=140 Stage 2 HTN 2 (DBP 110 mmhg <120 mmhg) n=64 Systolic BP 180 mmhg 2 n= Dose: 10/160 mg Dose: 5 10/160 mg 43 DBP reduction (mmhg) Poldermans et al. Clin Ther 2007;29(2): Data from Poldermans et al. J Hypertens 2006;24(Suppl 4):S20 (poster)


32 Oedema CCB dilates arteries Veins remain constricted ARB dilates arteries and veins Capillary overload forces fluid into surrounding tissue Reduces CCB-induced peripheral oedema Single mode of action of the CCB Dual mode of action of the CCB ARB
33 Amlodipine/Valsartan reduces the incidence of amlodipine-associated peripheral oedema Peripheral oedema (%) * Placebo (n=337) Valsartan (n=921) Amlodipine (n=460) Amlodipine/Valsartan (n=1,437) *p= vs amlodipine Novartis data on file
 40 30 33 N=220 20 * 13 10 0 Amlodipine/Valsartan Amlodipine/atenolol 10/160 mg 10/100 mg *p<0.")
34 Amlodipine/Valsartan prevents recurrence of atrial fibrillation more effectively than atenolol/valsartan during a 1-year follow-up Patients with at least one symptomatic or non-symptomatic ECG-documented episode of atrial fibrillation (% incidence) N= * Amlodipine/Valsartan Amlodipine/atenolol 10/160 mg 10/100 mg *p<0.01 vs amlodipine/atenolol Titration to maximum dose of amlodipine Mugellini et al. J Hypertens 2006;24(Suppl 4):S5
35 Single pill or free combination?
36 Single-pill combination vs free combination Single pill Free Simplicity of treatment + Compliance + Efficacy + + Tolerability +* Price + Flexibility +** ++ *Lower doses generally used in single-pill combinations **An increasing number of single-pill combinations are becoming available with a range of doses + = potential advantage Burnier, et al. Am J Hypertens 2006;19:1190 6; Neutel. Hypertension. Companion to Brenner & Rector s The Kidney. 2 nd ed. Philadelphia: Elsevier Saunders, p

37 Meta-Analysis of SPC vs Free Combination of Antihypertensive Agents Compliance Ratio Systolic BP ASCOT Study 21% 4.1 mmhg Adverse Events Diastolic BP 20%! Gupta AK, et al. Hypertension 2010;55: Gupta AK, et al. Hypertension 2010;55: mmhg
38 BP respondent rate (%) Valsartan/amlodipine single-pill combination significantly increase respondent rate compared with free combination SPC:valsartan/amlodipine Free combination:arb+ccb 81 days observation: 66.0% month 90 days observation: 54.0% P=0.04 The study included 812 patients: 414 on valsartan-based SPCs (209 on valsartan/amlodipine and 205 on valsartan/hctz) and 398 on ARB-based FCs (200 on ARB + CCB and 198 on ARB + HCTZ). BP target:<140/90mmhg(dm or CKD patients <130/80mmHg) Chang J, et al. Curr Med Res Opin Sep;26(9):
39 EXCITE: prospective, multinational, non-interventional, real-world study Amlodipine/valsartan OR Amlodipine/valsartan/HCT Visit 1 Baseline Optional Visit 2 13 weeks Observational period of 26 weeks ± 8 weeks Visit 3 26 weeks End of study Khan et al. Ther Adv Cardiovasc Dis Apr;8(2):45-55

40 EXCITE: data analyzed from >9700 patients with hypertension pooled from 13 countries Kuwait Bahrain Lebanon Qatar UAE South Korea Taiwan Hong Kong Oman Pakistan Philippines Egypt Indonesia Patients from Saudi Arabia were excluded from this analysis due to non-compliance with the study protocol. Safety data from this country are the subject of a separate report. Adil Hospital Lahore, Lahore, Pakistan. Real-life effectiveness, safety, and tolerability of amlodipine/valsartan or amlodipine/valsartan/hydrochlorothiazide single-pill combination in patients with hypertension from Pakistan. Ther Adv Cardiovasc Dis Apr;8(2):45-55
41 Change in mean sitting BP (mmhg) EXCITE: significant BP reductions from baseline across all treatment dosages in the AML/VAL group AML/VAL dose (mg) Overall 5/80 5/160 10/160 5/320 10/320 (n=8264) (n=1428) (n=4839) (n=1941) (n=28) (n=24) BL mssbp/msdbp (mmhg) 160.9/ / / / / / % CI (LL,UL) Overall 5/80 5/160 10/160 5/320 10/320 mssbp 31.42, , , , , , msdbp 16.79, , , , , , Khan et al. Ther Adv Cardiovasc Dis Apr;8(2):45-55
42 Change in mean sitting BP (mmhg) EXCITE: incremental BP reductions with AML/VAL across prior antihypertensive monotherapy classes Prior antihypertensive monotherapy BL mssbp/msdbp (mmhg) 0 5 Overall ACEi ARB CCB Beta-blocker Diuretic (n=2575) (n=653) (n=581) (n=781) (n=546) (n=14) 158.7/ / / / / / % CI (LL,UL) Overall ACEi ARB CCB Beta-blocker Diuretic mssbp 30.50, , , , , , msdbp 16.61, , , , , , Post-hoc analysis. Baseline defined as prior to start of AML/VAL. End of study defined as Visit 3 (Week 26). Included only patients who did not take any antihypertensive medication during the observational period, in addition to AML/VAL, and did not switch to AML/VAL/HCT. No additional treatment prior to study entry was received. Khan et al. Ther Adv Cardiovasc Dis Apr;8(2):45-55
43 EXCITE: Target BP achievement BP target achieved AML/VAL N= 8603 n (%) AML/VAL/HCT N=1191 n (%) Total N=9794 n (%) Therapeutic goal SBP<140 mmhg and DBP <90 mmhg 5822 (69.9) 832 (70.9) 6654 (70.0) SBP response SBP <140 mmhg or a reduction of 20 mmhg from baseline DBP response DBP <90 mmhg or a reduction of 10 mmhg from baseline 7305 (89.5) 1058 (91.0) 8363 (89.7) 6876 (91.8) 965 (91.4) 7841 (91.8)
44 Summary of the updated hypertension guidelines Loosened SBP target <140 for general; <150 for elderly Simplified drug regimen The initial drug chosen broaden to diuretics, CCB, ACEI and ARB. Initiation of combined therapy: SBP>160 and/or DBP>100 (stage 2 hypertension) mild elevation of BP (stage 1 hypertension) in presence of multiple risk factors, organ damages, DM, CKD or associated CV risk Emerging role of single-pilled combination
45 New updates on Heart Failure
46 Definitions of Heart Failure Heart failure is the pathophysiological state in which the heart is unable to pump blood at a rate commensurate with the requirements of the metabolizing tissues or can do so only from an elevated filling pressure. Eugene Braunwald


47 Annual Incidence of New Cases of HF Framingham Heart Study
48 NORMAL
49
50
51 SYSTOLIC HEART FAILURE
52
53
54
55
56
57
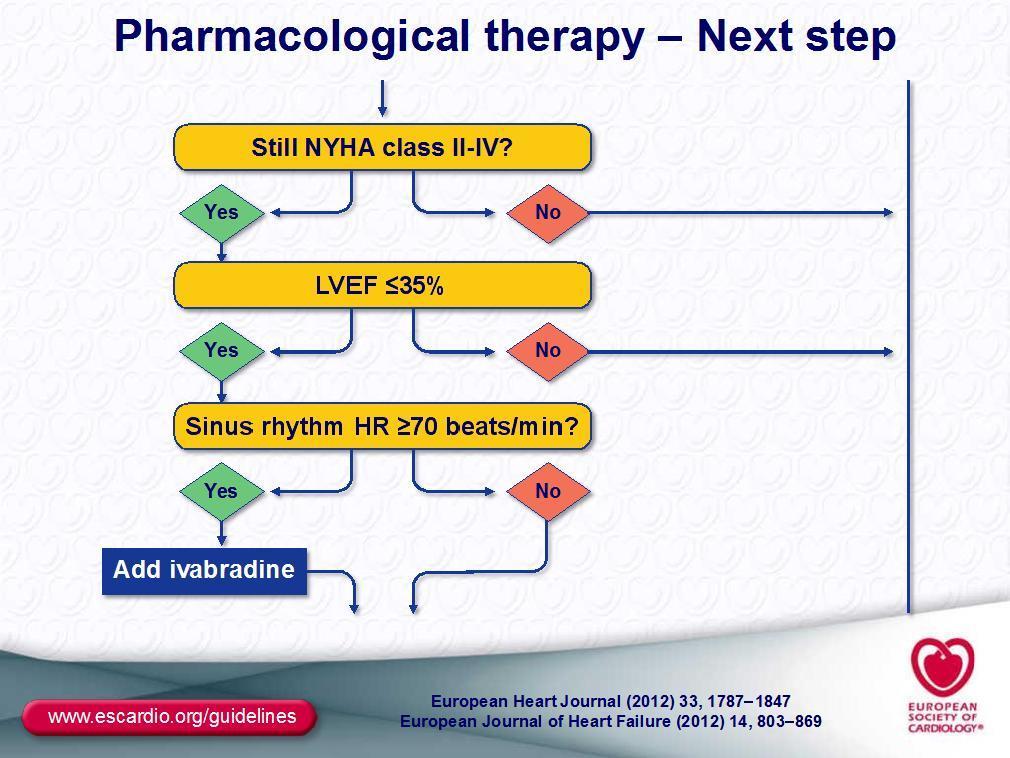
58 Ivabradine Ivabradine acts by reducing the heart rate via specific inhibition of the funny channel, a mechanism different from beta blockers and calcium channel blockers Blocking this channel reduces cardiac pacemaker activity, slowing the heart rate and allowing more time for blood to flow to the myocardium
59 Aim To assess the effect of ivabradine on outcomes in heart failure patients on recommended background therapies with heart rates 75 bpm in the SHIFT trial Bö hm M, Borer J, Ford I, et al. Clin Res Cardiol. 2013;102(1):

60 Baseline characteristics Ivabradine Placebo n=2052 n=2098 Mean age, years Male, % BMI, kg/m Mean HF duration, years HF ischemic cause, % NYHA class III, % NYHA class IV, % 2 2 Mean LVEF, % Mean HR, bpm Bö hm M, Borer J, Ford I, et al. Clin Res Cardiol. 2013;102(1):
61 Baseline background treatment Ivabradine n=2052 Placebo n=2098 β-blockers, % At least half target dose At target dose ACE inhibitors/arbs, % Diuretics (excludes AAs), % Aldosterone antagonists, % Bö hm M, Borer J, Ford I, et al. Clin Res Cardiol. 2013;102(1):
62 Patients with primary composite end point (%) Effect of ivabradine on primary outcome CV death or hospitalization for HF Hazard ratio= P< Placebo Ivabradine Time (months) Bö hm M, Borer J, Ford I, et al. Clin Res Cardiol. 2013;102(1):
63 Effect of ivabradine on major outcomes Hazard ratio 95% CI P Primary composite end point Cardiovascular mortality Hospitalization for worsening HF Death from HF All-cause mortality All-cause hospitalization Any cardiovascular hospitalization < < < < Favors ivabradine Favors placebo Bö hm M, Borer J, Ford I, et al. Clin Res Cardiol. 2013;102(1):
64
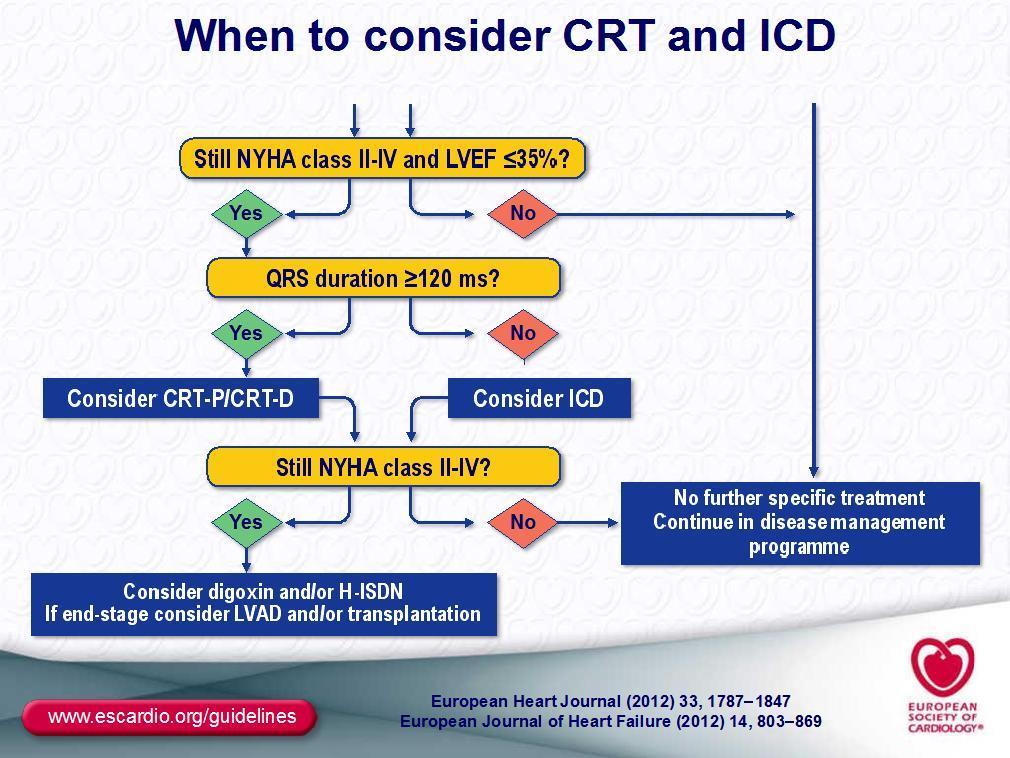
65 Summary of the updated heart failure guidelines Use of ivabradine in patients with impaired LVEF <35% and heart rate >70 bpm on optimal medical therapy Expand indication of device therapy (CRT/ICD) The use of LVAD implemented


66 Guidelines are trying to help
67 THANK YOU
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management
 Changing the Landscape of BP Management") Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
RAS Blockade Across the CV Continuum
 A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
A Summary of Recent International Meetings RAS Blockade Across the CV Continuum Copyright New Evidence Presented at the 2009 Congress of the European Society of Cardiology (August 29-September 2, Barcelona)
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
A Fresh Look at ARBs : Focus on HF survival data
 A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
A Fresh Look at ARBs : Focus on HF survival data Seok-Min Kang, MD, Ph D. Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea HF specialists ARBs,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
The Road to Renin System Optimization: Renin Inhibitor
 The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
The Road to Renin System Optimization: Renin Inhibitor A New Perspective on the Renin-Angiotensin System (RAS) Yong-Jin Kim, MD Seoul National University Hospital Human and Economic Costs of Hypertension
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Ferrari R, Fox K, Bertrand M, Mourad J.J, Akkerhuis KM, Van Vark L, Boersma E.
 Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
Effect of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers on cardiovascular mortality in hypertension: a meta-analysis of randomized controlled trials Ferrari R, Fox K, Bertrand
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Conflict of Interest Disclosure
 HYPERTENSION UPDATE: NEW JNC 8 Guideline vs OLD Federal Motor Carrier Safety Regulations PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# Conflict
HYPERTENSION UPDATE: NEW JNC 8 Guideline vs OLD Federal Motor Carrier Safety Regulations PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# Conflict
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Conflicts of Interest. Hypertension Guidelines Have Your Blood Pressure Up? Learning Objectives-Technician. Learning Objectives-Pharmacist
 Conflicts of Interest Hypertension Guidelines Have Your Blood Pressure Up? Diana Isaacs, PharmD, BCPS, BC-ADM, has no actual or potential conflicts of interest in relation to this program. Diana Isaacs,
Conflicts of Interest Hypertension Guidelines Have Your Blood Pressure Up? Diana Isaacs, PharmD, BCPS, BC-ADM, has no actual or potential conflicts of interest in relation to this program. Diana Isaacs,
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
Cardiac Protection across the cardiac continuum. Dong-Ju Choi, MD, PhD College of Medicine Seoul National University
 Cardiac Protection across the cardiac continuum Dong-Ju Choi, MD, PhD College of Medicine Seoul National University Renin Angiotensin Cascade Nitric oxide (NO) Bradykinin Degradation products ACE ACEI
Cardiac Protection across the cardiac continuum Dong-Ju Choi, MD, PhD College of Medicine Seoul National University Renin Angiotensin Cascade Nitric oxide (NO) Bradykinin Degradation products ACE ACEI
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London
 Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Objective & Outline. How the JNC Process Has Evolved. Expertise Represented on JNC 8 Panel
 Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017
 Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Preventing the cardiovascular complications of hypertension
 European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
European Heart Journal Supplements (2004) 6 (Supplement H), H37 H42 Preventing the cardiovascular complications of hypertension Peter Trenkwalder* Department of Internal Medicine, Starnberg Hospital, Ludwig
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,