Congenital Heart Disease An Approach for Simple and Complex Anomalies
|
|
|
- Jonah Hubbard
- 6 years ago
- Views:
Transcription

1 Congenital Heart Disease An Approach for Simple and Complex Anomalies Michael D. Pettersen, MD Director, Echocardiography Rocky Mountain Hospital for Children Denver, CO None Disclosures 1
2 ASCeXAM Contains questions on general congenital heart disease, not adult CHD Study guide contain all of the information in this talk plus addition topics that will be helpful for the exam There have been a few questions on fetal echo which have appeared on the ASCeXAM which are covered in the handout Insider information provided in study guide topics that have appeared on prior exams (last page of study guide) Which heart defect is more common? 1. Tetralogy of Fallot 2. Transposition of the Great Arteries 3. Aortic Stenosis 4. Coarctation of the Aorta 5. Atrioventricular Canal 2
3 What is the most common defect seen with Down syndrome (trisomy 21)? 1. Patent Ductus Arteriosus 2. Tetralogy of Fallot 3. Aortic Stenosis 4. Ventricular septal defect 5. Coarctation of the Aorta Congenital Heart Disease Spectrum of Congenital Heart Disease - Incidence % of live births * >30,000 individuals/year in U.S. 50% simple shunts (ASD, VSD, PDA) 20% simple obstruction 30% complex * Excludes MVP (4-6%) & Bicuspid AV (1-2%) 3
4 Congenital Heart Disease Spectrum of Congenital Heart Disease - Frequency Cardiac Malformation % of CHD M:F Ratio Ventr. Septal Defect :1 Patent Ductus Arter :2-3 Tetralogy of Fallot :1 Atrial Septal Defect 7-8 1:2-4 Pulmonary Stenosis 7-8 1:1 Transp. of Grt. Art :1 Coarctation of Aorta :1 AV Septal Defect 2-7 1:1 Aortic Stenosis 2-5 4:1 Truncus Arteriosus 1-2 1:1 Tricuspid Atresia 1-2 1:1 Tot. Anom Pulm Veins 1-2 1:1 Congenital Heart Disease Common Syndromes/Chromosomal Anomalies Anomaly Trisomy 21 Trisomy 18 Trisomy 13 Turner Noonan Williams Holt-Oram Marfan DiGeorge Associations VSD, AV Canal VSD, PDA VSD, PDA, Dextrocardia Coarctation, AS PS, HCM Supravalvar AS, Peripheral PS ASD Aortic root dilation, MVP VSD, arch anomalies, TOF 4
5 Congenital Heart Disease Currently over 1 million patients over 18 with CHD are alive in this country This increases at 4-5% per year 20,000 cardiac surgical procedures for CHD/year >90% of children with CHD survive to adulthood The majority of adult CHD patients will be post-op The ASCeXAM does not cover much post-op disease, but has asked questions about operations Congenital Heart Disease A Brief History of Operations Year Physician Procedure 1938 Gross Ligation of PDA 1944 Blalock, Taussig Syst.-pulm. shunt 1945 Gross, Crafoot Repair of coarctation 1946 Potts Aorta to LPA shunt/direct anastamosis 1952 Muller Pulm. artery band 1953 Gibbon Repair of ASD 1954 Lillehei Repair of VSD 1954 Glenn SVC-PA shunt Mustard/Senning Atrial correction of TGA 1955 Lillehei, Kirklin Repair of tetralogy of Fallot 1960 Waterston Aorta to RPA shunt/direct anastamosis 1964 Rastelli Conduit replacement of PA 1967 Rashkind Balloon atrial septostomy 1971 Fontan, Kreutzer Repair of tricuspid atresia 1976 Jatene Arterial switch for TGA 1978 Cold blood cardioplegia 5


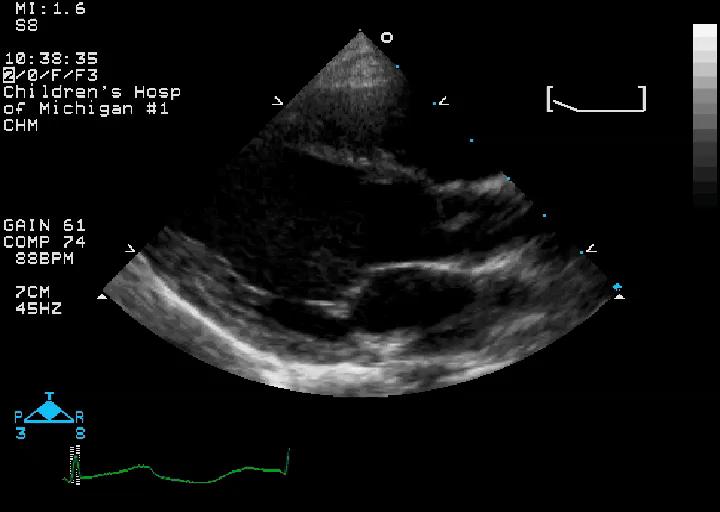
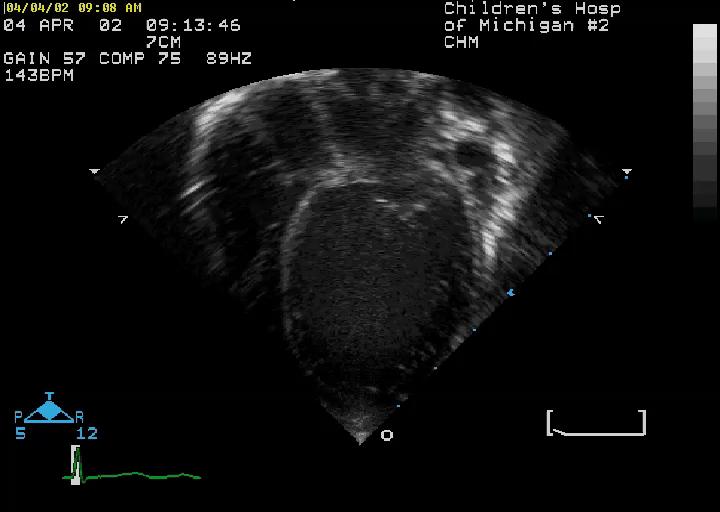
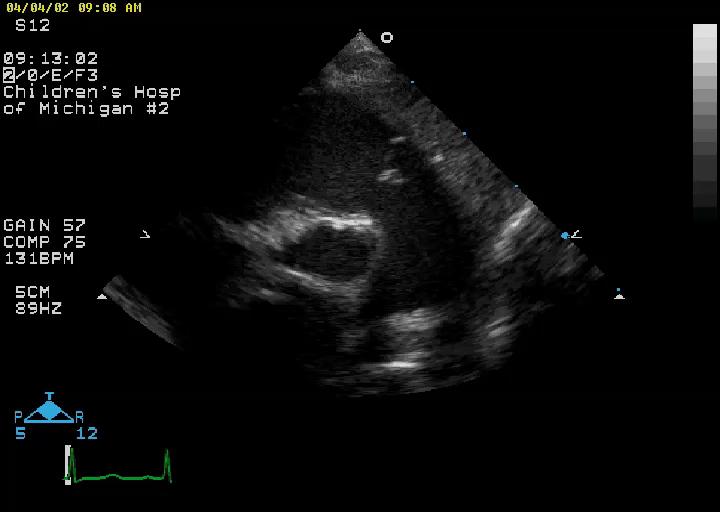
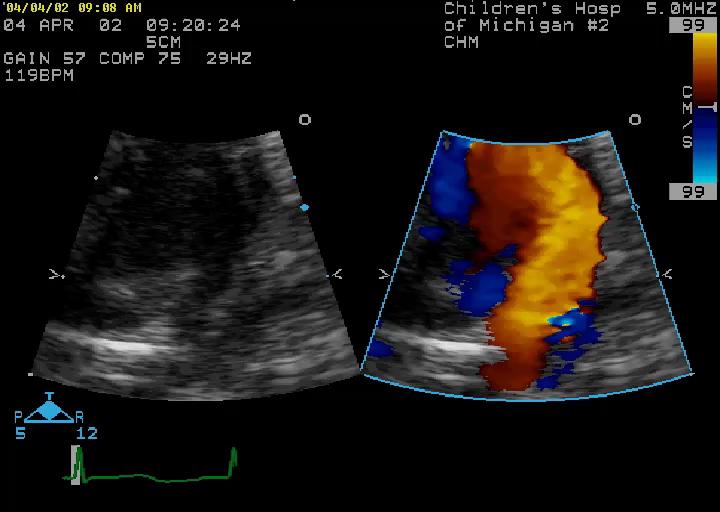
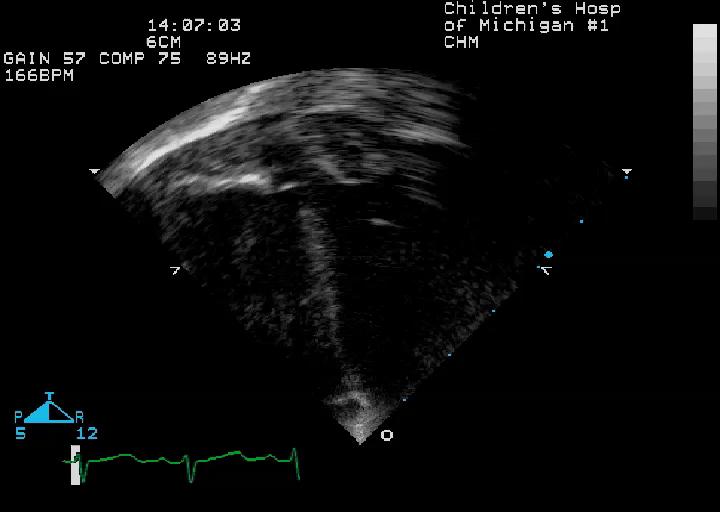
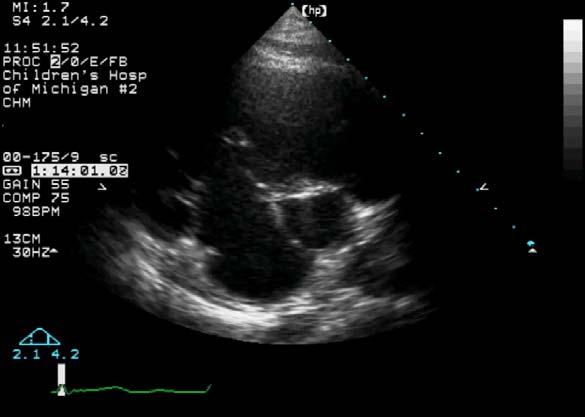
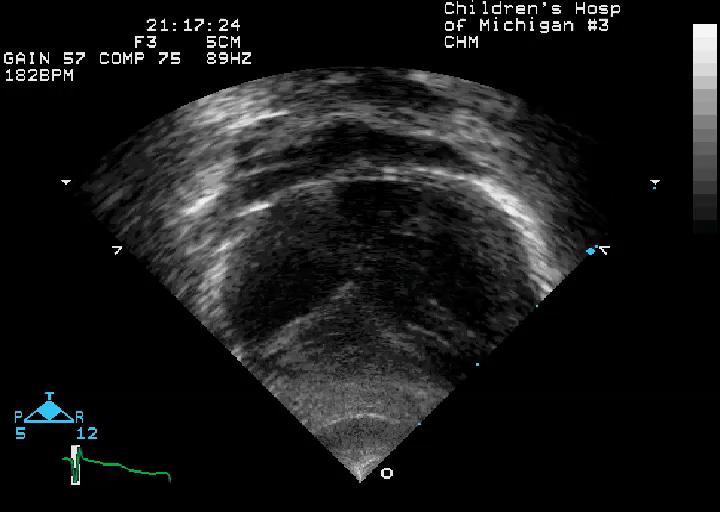
6 Case 1-3 month old with a murmur, tachypnea and failure to thrive Case 1-3 month old with a murmur, tachypnea and failure to thrive 6

7 Case 1-3 month old with a murmur, tachypnea and failure to thrive Case 1-3 month old with a murmur, tachypnea and failure to thrive 7
8 Case 1-3 month old with a murmur, tachypnea and failure to thrive Case 1-3 month old with a murmur, tachypnea and failure to thrive 8
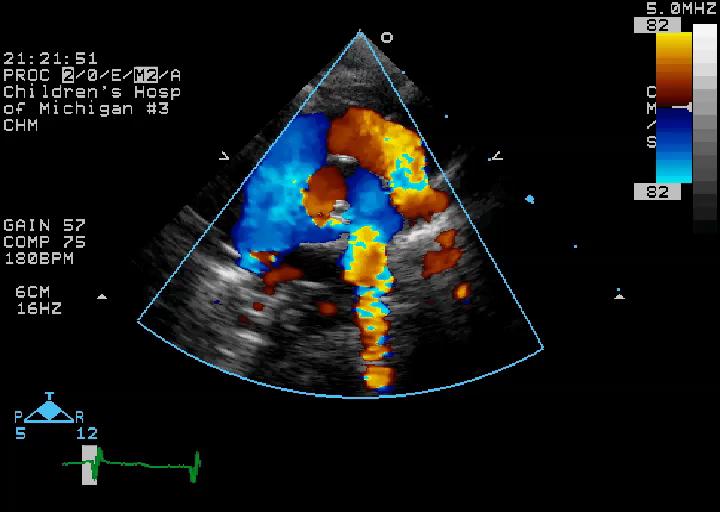
9 The defect shown in this example is: 1. Secundum VSD 2. Sinus Venosus VSD 3. Perimembranous VSD 4. Inlet VSD 5. Supracristal VSD An isolated VSD will generally produce enlargement of which chamber(s): 1. Left atrium, Left ventricle 2. Right ventricle 3. Right ventricle, pulmonary artery 4. Aorta 5. Right ventricle, right atrium 9
10 What is the right ventricular pressure? 1. Normal 2. Supra systemic 3. Systemic 4. Can t tell from information given 5. Want to go home now Ventricular Septal Defect Clinical Most common defect, 25% of CHD Shunt flow usually left to right in infants and children Symptoms depend on the size of the defect Large - >50% of aortic annulus size Medium % of annulus size Small - <25% of annulus size Large VSDs result in pulmonary edema tachypnea, poor feeding, failure to thrive in infants In un-operated patients with large defects pulmonary vascular disease develops shunt reversal and cyanosis (Eisenmenger s complex) 10
11 Ventricular Septal Defect Anatomy SVC RA MPA PERIMEMBRANOUS 2 SUPRACRISTAL 3 MUSCULAR 2 4 INLET AO 1 4 LA IVC 4 3 RV LV 3 RIGHT VENTRICULAR VIEW LEFT VENTRICULAR VIEW Ventricular Septal Defect Parasternal Short Axis - Base Defects seen in this region are perimembranous RV Supracristal VSD's are seen here PA RA LA IVC 11

12 Ventricular Septal Defect Parasternal Short-Axis - Mid-Ventricle Muscular (trabecular) VSD's can be seen anywhere along the septum from this view RV LV Ventricular Septal Defect Parasternal Short-Axis "Sweep" VSD 12
13 Ventricular Septal Defect Apical Four- Chamber View RA LA Inlet VSD's are best seen from this view. Apical muscular VSD's can be seen from this view. Size may vary from tiny to large. RV LV Ventricular Septal Defect Apical Five-Chamber View RA AO LA This view nicely demonstrates a perimembranous VSD and its relationship to the aortic and tricuspid valves RV LV 13
14 Case 1- Review Case 1- Review 14

15 Case 1- Review Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur 15
16 Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur 16

17 Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur 17

18 Ventricular Septal Defect Case 2 8 y.o. with asymptomatic murmur The defect shown in this example is: 1. Secundum VSD 2. Sinus Venosus VSD 3. Perimembranous VSD 4. Inlet VSD 5. Supracristal VSD 18

19 Question 10 - A common complication of this defect is: 1. Pulmonary valve endocarditis 2. Aortic regurgitation 3. Aortic dissection 4. Tricuspid regurgitation 5. Right ventricular enlargement Case 2- Review 19

20 Case 2- Review Case 2- Review 20

21 Supracristal VSD Aortic Cusp Prolapse RV AO LV LA Ventricular Septal Defect Case 3 No questions 21


22 Ventricular Septal Defect Case 3 No questions Ventricular Septal Defect Case 3 No questions 22


23 Ventricular Septal Defect Case 3 No questions Ventricular Septal Defect Case 3 No questions 23

24 Ventricular Septal Defect Case 3 No questions VSD gradient = 53 mmhg BP = 72/38 mmhg RVSP = = 19 mmhg 24

25 Case 4 6 y.o. with continuous murmur Case 4 6 y.o. with continuous murmur 25

26 Case 4 6 y.o. with continuous murmur Case 4 6 y.o. with continuous murmur 26

27 Case 4 6 y.o. with continuous murmur Case 4 6 y.o. with continuous murmur 27
28 Case 4 6 y.o. with continuous murmur Peak Gradient = 104 mmhg The Doppler tracing in this case implies: 1. Severe pulmonary hypertension 2. Severe systemic hypertension 3. Severe coarctation of the aorta 4. Normal pulmonary artery pressure 5. Severe pulmonary artery stenosis 28
29 Patent Ductus Arteriosus Clinical Continuous murmur in older patients Bounding pulses, wide pulse pressure, respiratory symptoms in neonates with a large PDA Large PDA will act much like a large VSD, producing pulmonary over-circulation and signs/symptoms of congestive heart failure A small PDA is generally hemodynamically insignificant but is at risk for endarteritis Patent Ductus Arteriosus Anatomy Innom. Vein PDA AO MPA LPA Desc AO 29
30 Patent Ductus Arteriosus Ductal View Parasternal Ductal View (High Left Parasternal) LV RV PA PDA LA Desc AO Patent Ductus Arteriosus Doppler Flow Pattern RV LV LA PA AO Continuous Flow with Systolic Peak Systolic PA pressure = SBP 4V PDA 2 30
31 Patent Ductus Arteriosus Clinical management Large PDAs in preterm infants Pharmacologic closure indomethacin or ibuprofen Surgical closure left lateral thoracotomy Small PDA in older infants and children Catheter closure device or coil Case 4 - Review 31


32 Case 4 - Review Peak Gradient = 104 mmhg Case 5 Large PDA 32

33 Case 5 Large PDA Case 5 Large PDA 33

34 Case 5 Large PDA Case 5 Large PDA 34

35 Case 5 Large PDA Case 5 Large PDA 35
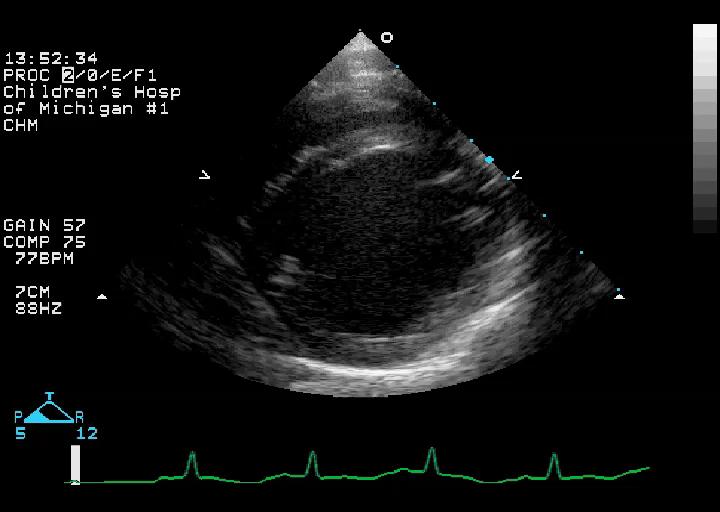
36 Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur 36

37 Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur 37

38 Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur 38

39 Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur 39

40 Case 6 Asymptomatic 3 month old with cyanosis and a cardiac murmur The defect shown in this example is: 1. Single ventricle 2. Transposition of the great arteries 3. Perimembranous VSD 4. Tetralogy of Fallot 5. Complete atrioventricular canal 40
41 Tetralogy of Fallot Background Accounts for 10-13% of congenital heart disease Most common cyanotic CHD Usually present as asymptomatic murmur Cyanosis usually develops/progresses with time Anatomy Ventricular Septal Defect Overriding Aorta RV outflow obstruction RV hypertrophy Conal Septum Malalignment Tetralogy of Fallot Anatomic Variables AO AO AO RA RA RA RV LV RV LV RV LV "Pink Tetralogy" Mild Pulmonary Stenosis Classic Tetralogy Severe Tetralogy or Pulmonary Atresia 41
42 Tetralogy of Fallot Associated Anomalies Valvular pulmonary stenosis % Right aortic arch - 25% Atrial septal defect - 15% Coronary anomalies - 5% Muscular VSD - 2% Tetralogy of Fallot Parasternal Long Axis View "Malalignment" VSD with Aortic Override RV Hypertrophy RV AO LV CS LA Mitral-Aortic Continuity 42
43 Outflow VSD "Malalignment" type Tetralogy of Fallot Parasternal Short Axis - Base RV PA RV Hypertrophy Infundibular & Valvular Stenosis RA LA IVC Position of "Overriding" Aorta Tetralogy of Fallot Apical Five-Chamber RA LA AO Outlet VSD with Aortic Override RV LV 43

44 Tetralogy of Fallot Subcostal RV Inflow/Outflow View RA MPA RV The right ventricular outflow obstruction is seen in this view. This is often the best angle for Doppler interrogation of the RVOT Case 6 - Review 44
45 Case 6 - Review Case 6 - Review 45
46 Tetralogy of Fallot Surgical Intervention Timing usually during first 6 months VSD closure, relief of RVOTO obstruction Many repairs require a trans annular RV outflow patch with results in chronic severe pulmonary regurgitation Likely need for late pulmonary valve replacement Rastelli type repair (VSD closure + RV to pulmonary artery conduit) may be required for complex anatomy pulmonary atresia, coronary anomalies 46
47 Case 7 1 day old infant with tachypnea and SaO2 of 76% Case 7 1 day old infant with tachypnea and SaO2 of 76% 47
48 Case 7 1 day old infant with tachypnea and SaO2 of 76% Case 7 1 day old infant with tachypnea and SaO2 of 76% 48
49 What congenital heart defect is shown: 1. Perimembranous VSD 2. Truncus arteriosus 3. Corrected transposition of the great arteries (L-TGA) 4. Complete transposition of the great arteries (D-TGA) 5. Tetralogy of Fallot Which of the following is the preferred surgical palliation of this defect? 1. Rastelli operation 2. Mustard operation 3. Jatene operation 4. Konno operation 5. Fontan operation 49
50 D-Transposition of the Great Arteries Most common cyanotic CHD presenting in the newborn nursery 4-8% of CHD Very high mortality without intervention (90% at 1 year of life) D-TGA Intact Septum D-TGA w/ VSD RA AO PA RA AO PA RV LV RV LV D-Transposition of the Great Arteries Associated Anomalies VSD 40-45% Coronary anomalies ~ 40% Pulmonary stenosis (valve or sub valve) - 25% ASD PDA Coarctation - 5% 50
51 D-Transposition of the Great Arteries Parasternal Long Axis View RV AO LV MPA LA D-Transposition of the Great Arteries Parasternal Short Axis - Base RV AV PV RA LA IVC 51

52 D-Transposition of the Great Arteries High Parasternal Short Axis - Base AO PA RA Case 7 Review 52

53 Case 7 Review Case 7 Review 53
 Has been largely abandoned VSD closure/ RV-PA conduit (Rastelli) Performed within the first few months of life Used in the setting of d-tga")
54 Case 7 Review D-Transposition of the Great Arteries Interventions Atrial balloon septostomy (Rashkind) Increases saturation by improving atrial mixing Arterial switch (Jatene) Performed within the first 1-2 weeks of life Atrial switch (Mustard/Senning) Has been largely abandoned VSD closure/ RV-PA conduit (Rastelli) Performed within the first few months of life Used in the setting of d-tga with PS/sub-PS Requires conduit replacement/ future surgery 54


55 D-TGA Intervention-Rastelli Procedure RA AO PA RA AO PA RV LV RV LV D-TGA Atrial Switch (Mustard/Senning) Operation Gaca A M et al. Radiology 2008;247:

56 TGA Jatene Arterial Switch Operation 56

57 Case 8 12 year old with asymptomatic murmur Case 8 12 year old with asymptomatic murmur 57

58 Case 8 12 year old with asymptomatic murmur Case 8 12 year old with asymptomatic murmur 58
59 Case 8 12 year old with asymptomatic murmur Case 8 12 year old with asymptomatic murmur 59
60 Case 8 12 year old with asymptomatic murmur The defect shown in this example is: 1. Secundum ASD 2. Sinus Venosus ASD 3. Perimembranous ASD 4. Primum ASD 5. Coronary sinus ASD 60
61 A common associated defect with this anomaly, shown in this case, is: 1. Bicuspid aortic valve 2. Perimembranous VSD 3. Patent ductus arteriosus 4. Coarctation of the aorta 5. Cleft mitral valve Atrioventricular Septal Defects -3-5% of CHD -High incidence in Down Syndrome -Physiology depends on which anatomic defects are present Primum ASD Inlet VSD Complete AVSD 1. Primum ASD 2. Inlet VSD 3. Common AV Valve Partial AVSD 1. Primum ASD 2. No VSD 3. Cleft Mitral Valve 61
62 Complete Atrioventricular Canal Associated Anomalies Patent ductus arteriosus Hypoplasia of one ventricle AV valve problems - regurgitation LVOT obstruction Atrioventricular Canal Long Axis View Normal AV Canal AO AO LV LA LV LA Mitral valve has abnormal orientation and often has abnormal chordal attachments across the LV outflow area 62

63 Normal Cleft Mitral Valve Parasternal Short-Axis View Inlet VSD's occur in this location Cleft Partial Atrioventricular Canal Apical 4-Chamber View Complete RA LA Primum ASD AV Valves at same level RA LA RV LV Inlet VSD RV LV 63
64 Atrioventricular Canal Defects Subcostal Views LA "Gooseneck" deformity RA LV AO RV RA Primum ASD and Inlet VSD RV LV Atrioventricular Canal Defects Subcostal Short Axis Views Wide Antero-septal Tricuspid Commissure RVOT Systole RVOT Diastole RV LV RV LV Cleft Mitral Valve "Common" AV Valve 64


65 Case 8 Review Case 8 Review 65

66 Case 8 Review Case 8 Review 66

67 Case 9 Complete AV Canal 67


68 Case 9 Complete AV Canal Case 9 Complete AV Canal 68

69 Case 9 Complete AV Canal Case 9 Complete AV Canal 69


70 Case 9 Complete AV Canal Case 9 Complete AV Canal 70
 Complete AVSD - marked volume and pressure overload (VSD shunt physiology) AV valve regurgitation may exacerbate volume overload and symptoms of heart")
71 Case 9 Complete AV Canal AV Septal Defects Physiology Physiology dependent on which components of AV septal defect are present If 1 ASD and no VSD - physiology similar to isolated ASD (right sided volume overload) Complete AVSD - marked volume and pressure overload (VSD shunt physiology) AV valve regurgitation may exacerbate volume overload and symptoms of heart failure 71
72 AV Septal Defects Surgical Intervention Partial AVSD Usually electively repaired at age 2-4 years Complicating features (AVV regurgitation, LVOTO) may necessitate earlier intervention Complete AVSD Usually repaired by 6 months of age (earlier in trisomy 21) to prevent pulmonary vascular obstructive disease AV Septal Defects Outcomes After Surgery Surgical outcomes 3-4% operative mortality for complete AVSD <1% operative mortality for partial AVSD Late reoperation in 10-15% Left AV valve regurgitation Left ventricular outflow tract obstruction Hypoplasia of the outflow tract Accessory AV valve tissue Discrete subaortic membrane 72
73 Truncus Arteriosus Anatomy Characteristic anatomy characterized by: Single arterial vessel that arises from the base of the heart and gives origin to: Systemic arteries Pulmonary arteries Coronary arteries Single semilunar valve 73
74 Truncus Arteriosus Anatomy Type I Type III Type II Associated Defects Abnormal coronaries (37-49%) Right aortic arch (30%) Abnormal truncal valve Absent pulmonary artery (16%) Interrupted aortic arch (15%) Left SVC (12%) Secundum ASD (9-20%) Truncus Arteriosus Clinical Aspects Patients usually present due to the presence of a cardiac murmur Complete mixing of systemic and pulmonary venous blood results in cyanosis Excessive pulmonary blood flow causes sign and symptoms of congestive heart failure The cyanosis is generally mild 74


75 Truncus Arteriosus Treatment Requires surgical repair in the first weeks of life Median sternotomy requiring bypass Palliative PA band rarely used in the current era Rastelli type repair Close VSD to truncus Disconnect PAs RV to PA conduit RA RV AO LV PA Case 10 Truncus Arteriosus 75

76 Case 10 Truncus Arteriosus Case 10 Truncus Arteriosus 76


77 Case 10 Truncus Arteriosus Case 10 Truncus Arteriosus 77


78 Case 10 Truncus Arteriosus Case 10 Truncus Arteriosus 78


79 Case 10 Truncus Arteriosus Case 10 Truncus Arteriosus 79

80 Case 10 Truncus Arteriosus 80
81 Total Anomalous Pulmonary Venous Return AO Anatomic Types AO MPA MPA RA RV Supra cardiac LV RA RV Infracardiac LV AO MPA AO MPA RA Cardiac RV LV RA RV Coronary sinus LV Total Anomalous Pulmonary Venous Return Echo Clues Enlarged right heart Right to left atrial shunting Unusual membranes in left atrium Abnormal flow in systemic venous system Obstruction may occur at different levels Most common - infracardiac May be remarkably asymptomatic (in absence of obstruction) 81

82 Case 12 Supra cardiac TAPVR Case 12 Supra cardiac TAPVR 82

83 Case 12 Supra cardiac TAPVR Case 12 Supra cardiac TAPVR 83

84 Case 12 Supra cardiac TAPVR 84
 Mitral")
85 Anomalous Left Coronary Artery From the Pulmonary Artery - ALCAPA Rare congenital anomaly Usually presents at 2-3 m of age Results in severe LV ischemia Present as dilated CM, CHF ECG often diagnostic Patients survive w/ collateral flow Surgery done to re-implant vessel Anomalous Left Coronary Artery Echocardiographic Clues Left ventricular dysfunction (usually severe) Mitral insufficiency due to LV dilation/dysfunction, papillary muscle infarction Endocardial fibroelastosis of LV and/or papillary muscles Failure to identify proximal LCA from aorta Unusual flow into main pulmonary artery 85


86 Anomalous Left Coronary Artery From the Pulmonary Artery - ALCAPA Case 11 ALCAPA 86

87 Case 11 ALCAPA Case 11 ALCAPA 87
88 Case 11 ALCAPA Case 11 ALCAPA 88

89 Case 11 ALCAPA 89


90 Good Luck On Your Exam Questions? 90
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Congenital Heart Disease: Physiology and Common Defects
 Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Congenital Heart Disease: Physiology and Common Defects Jamie S. Sutherell, M.D, M.Ed. Associate Professor, Pediatrics Division of Cardiology Director, Medical Student Education in Pediatrics Director,
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases
 Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Echocardiographic assessment in Adult Patients with Congenital Heart Diseases Athanasios Koutsakis Cardiologist, Cl. Research Fellow George Giannakoulas Ass. Professor in Cardiology 1st Cardiology Department,
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Surgical Procedures. Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder
 PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
PEDIATRIC Review Surgical Procedures Atrial Septal Defect repair: Direct suture of small ASDs Patch repair Transcatheter closure with a prosthetic device called occluder Balloon atrial septostomy (Rashkind)
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Slide 1. Slide 2. Slide 3 CONGENITAL HEART DISEASE. Papworth Hospital NHS Trust INTRODUCTION. Jakub Kadlec/Catherine Sudarshan INTRODUCTION
 Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
Slide 1 CONGENITAL HEART DISEASE Jakub Kadlec/Catherine Sudarshan NHS Trust Slide 2 INTRODUCTION Most common congenital illness in the newborn Affects about 4 9 / 1000 full-term live births in the UK 1.5
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE
 By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
By Dickens ATURWANAHO & ORIBA DAN LANGOYA MAKchs, MBchB CONGENTAL HEART DISEASE Introduction CHDs are abnormalities of the heart or great vessels that are present at birth. Common type of heart disease
Adel Hasanin Ahmed 1 ASD
 Adel Hasanin Ahmed 1 ASD Atrial septal defect (ASD) is the commonest form of congenital heart disease seen in adults. The commonest form of defect is the secundum ASD, accounting for two thirds of cases,
Adel Hasanin Ahmed 1 ASD Atrial septal defect (ASD) is the commonest form of congenital heart disease seen in adults. The commonest form of defect is the secundum ASD, accounting for two thirds of cases,
NASCI 2012 Segmental Analysis
 NASCI 2012 Segmental Analysis Frandics Chan, M.D., Ph.D. Stanford University Medical Center Lucile Packard Department Children s of Radiology Hospital Menagerie of Congenital Cardiac Lesions 1. Absent
NASCI 2012 Segmental Analysis Frandics Chan, M.D., Ph.D. Stanford University Medical Center Lucile Packard Department Children s of Radiology Hospital Menagerie of Congenital Cardiac Lesions 1. Absent
Echocardiography in Adult Congenital Heart Disease
 Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Echocardiography in Adult Congenital Heart Disease Michael Vogel Kinderherz-Praxis München CHD missed in childhood Subsequent lesions after repaired CHD Follow-up of cyanotic heart disease CHD missed in
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Anomalous Systemic Venous Connection Systemic venous anomaly
 World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
World Database for Pediatric and Congenital Heart Surgery Appendix B: Diagnosis (International Paediatric and Congenital Cardiac Codes (IPCCC) and definitions) Anomalous Systemic Venous Connection Systemic
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
Most common fetal cardiac anomalies
 Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
Most common fetal cardiac anomalies Common congenital heart defects CHD % of cardiac defects Chromosomal Infants Fetuses anomaly (%) 22q11 deletion (%) VSD 30 5~10 20~40 10 PS 9 5 (PA w/ VSD) HLHS 7~9
List of Videos. Video 1.1
 Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Video 1.1 Video 1.2 Video 1.3 Video 1.4 Video 1.5 Video 1.6 Video 1.7 Video 1.8 The parasternal long-axis view of the left ventricle shows the left ventricular inflow and outflow tract. The left atrium
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
"Lecture Index. 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.
 Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development.") "Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
"Lecture Index 1) Heart Progenitors. 2) Cardiac Tube Formation. 3) Valvulogenesis and Chamber Formation. 4) Epicardium Development. 5) Septation and Maturation. 6) Changes in Blood Flow during Development.
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin. Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong
 Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Perimembranous VSD: When Do We Ask For A Surgical Closure? LI Xin Department of Cardiothoracic Surgery Queen Mary Hospital Hong Kong Classification (by Kirklin) I. Subarterial (10%) Outlet, conal, supracristal,
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Heart and Soul Evaluation of the Fetal Heart
 Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Heart and Soul Evaluation of the Fetal Heart Ivana M. Vettraino, M.D., M.B.A. Clinical Associate Professor, Michigan State University College of Human Medicine Objectives Review the embryology of the formation
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Congenital Heart Disease: Cyanotic Lesions. Amitesh Aggarwal
 Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Congenital Heart Disease: Cyanotic Lesions Amitesh Aggarwal 12 y/o male admitted because of dyspnea and cyanosis Patient has been cyanotic since few months after birth Has episodes of tachypnea and worsening
Screening for Critical Congenital Heart Disease
 Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Screening for Critical Congenital Heart Disease Caroline K. Lee, MD Pediatric Cardiology Disclosures I have no relevant financial relationships or conflicts of interest 1 Most Common Birth Defect Most
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Paediatrics Revision Session Cardiology. Emma Walker 7 th May 2016
 Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Paediatrics Revision Session Cardiology Emma Walker 7 th May 2016 Cardiovascular Examination! General:! Make it fun!! Change how you act depending on their age! Introduction! Introduce yourself & check
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical)
") September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
September 26, 2012 Philip Stockwell, MD Lifespan CVI Assistant Professor of Medicine (Clinical) Advances in cardiac surgery have created a new population of adult patients with repaired congenital heart
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Congenital Heart Disease II: The Repaired Adult
 Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Congenital Heart Disease II: The Repaired Adult Doreen DeFaria Yeh, MD FACC Assistant Professor, Harvard Medical School MGH Adult Congenital Heart Disease Program Echocardiography Section, no disclosures
Pediatric Board Review Congenital Heart Disease. Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University
 Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
Pediatric Board Review Congenital Heart Disease Steven H. Todman, M.D. Pediatric Cardiologist Louisiana State University Our Mission To discuss various types of congenital heart disease that are commonly
ASCeXAM / ReASCE. Practice Board Exam Questions. Tuesday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
September 28-30, 2018
 September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
September 28-30, 2018 Course Director Optimizing Detection of Congenital Heart Disease: Important Anatomic Cardiac Regions The Top 5 Critical Anatomic Regions in Fetal Cardiac Imaging Alfred Abuhamad,
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
Introduction. Pediatric Cardiology. General Appearance. Tools of Assessment. Auscultation. Vital Signs
 Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Introduction Pediatric Cardiology An introduction to the pediatric patient with heart disease: M-III Lecture Douglas R. Allen, M.D. Assistant Professor and Director of Community Pediatric Cardiology at
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Adult Congenital Heart Disease
 Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult Congenital Heart Disease Anne Marie Valente, MD Boston Adult Congenital Heart Disease and Pulmonary Hypertension Program Division of Cardiology Brigham and Women s Hospital, Boston Children s Hospital
Adult congenital heart disease Complex plumbing made simple
 Adult congenital heart disease Complex plumbing made simple James Oliver Leeds Bayer Disclosures Q 1. With respect to atrial septal defects: 1. Severe right heart volume loading is generally a contraindication
Adult congenital heart disease Complex plumbing made simple James Oliver Leeds Bayer Disclosures Q 1. With respect to atrial septal defects: 1. Severe right heart volume loading is generally a contraindication
Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs)
") Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs) Manny Gaziano, MD, FACOG obimages.net obimages.net@gmail.com Acknowledgements: Krista Wald, RDMS, sonographer,
Making Sense of Cardiac Views and Imaging Characteristics for 13 Congenital Heart Defects (CHDs) Manny Gaziano, MD, FACOG obimages.net obimages.net@gmail.com Acknowledgements: Krista Wald, RDMS, sonographer,
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
TGA Surgical techniques: tips & tricks (Arterial switch operation)
") TGA Surgical techniques: tips & tricks (Arterial switch operation) Seoul National University Children s Hospital Woong-Han Kim Surgical History 1951 Blalock and Hanlon, atrial septectomy 1954 Mustard et
TGA Surgical techniques: tips & tricks (Arterial switch operation) Seoul National University Children s Hospital Woong-Han Kim Surgical History 1951 Blalock and Hanlon, atrial septectomy 1954 Mustard et
The role of intraoperative TOE in congenital cardiac surgery
 The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
The role of intraoperative TOE in congenital cardiac surgery Justiaan Swanevelder Dept of Anaesthesia Groote Schuur and Red Cross War Memorial Children s Hospitals University of Cape Town, South Africa
Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute
 Clinic Mazankowski Heart Institute") Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute Brief Overview of Congenital Heart Disease Spectrum disorder Treatment & Impact
Pamela Heggie, RN BN Clinic Coordinator Northern Alberta Adult Congenital Heart (NAACH) Clinic Mazankowski Heart Institute Brief Overview of Congenital Heart Disease Spectrum disorder Treatment & Impact
Congenital Heart Disease. Mohamed Waheed Elsharief.
 Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Congenital Heart Disease Mohamed Waheed Elsharief. Objectives l By the end of this lecture you should be able to Fetal Circulation l For the fetus the placenta is the oxygenator so the lungs do little
Atrioventricular Canal (Septal) Defects. Norman H Silverman MD. D Sc (Med),FACC, FAHA
 Defects. Norman H Silverman MD. D Sc (Med),FACC, FAHA") Atrioventricular Canal (Septal) Defects Norman H Silverman MD. D Sc (Med),FACC, FAHA Embryology of the A-V Canal Looping NHS. Formation of the Atrial Septum Embryology of the A-V Canal NHS. Development
Atrioventricular Canal (Septal) Defects Norman H Silverman MD. D Sc (Med),FACC, FAHA Embryology of the A-V Canal Looping NHS. Formation of the Atrial Septum Embryology of the A-V Canal NHS. Development
Surgical options for tetralogy of Fallot
 Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
Surgical options for tetralogy of Fallot Serban Stoica FRCS(CTh) MD ACHD study day, 19 September 2017 Anatomy Physiology Children Adults Complications Follow up Anatomy Etienne Fallot (1850-1911) VSD Overriding
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Tetralogy of Fallot (TOF) repair, Ventriculotomy Coarctation repair, Other
 repair, Ventriculotomy Coarctation repair, Other") Tier 1 Surgery Form Date of Surgery DD/MM/YYYY Primary Cardiac Procedure Select the patient's primary surgical procedure. If the patient has multiple operating room visits, these should be reported on
Tier 1 Surgery Form Date of Surgery DD/MM/YYYY Primary Cardiac Procedure Select the patient's primary surgical procedure. If the patient has multiple operating room visits, these should be reported on
DIAGNOSIS, MANAGEMENT AND OUTCOME OF HEART DISEASE IN SUDANESE PATIENTS
 434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
Echocardiography in adult congenital heart disease
 S12 Department of Cardiology, Royal Hospital for Sick Children, Glasgow G3 8SJ, UK A Houston S Lilley T Richens University Department of Medicine and Therapeutics, Western Infirmary, Glasgow G11 6NT, UK
S12 Department of Cardiology, Royal Hospital for Sick Children, Glasgow G3 8SJ, UK A Houston S Lilley T Richens University Department of Medicine and Therapeutics, Western Infirmary, Glasgow G11 6NT, UK
pulmonary valve on, 107 pulmonary valve vegetations on, 113
 INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
بسم هللا الرحمن الرحيم. The cardio vascular system By Dr.Rawa Younis Mahmood
 بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
بسم هللا الرحمن الرحيم The cardio vascular system By Dr.Rawa Younis Mahmood Introduction Evaluation of the cardio vascular system depend on history and physical examination by : Asking about cyanosis,blueness
Echocardiography in Congenital Heart Disease
 Chapter 44 Echocardiography in Congenital Heart Disease John L. Cotton and G. William Henry Multiple-plane cardiac imaging by echocardiography can noninvasively define the anatomy of the heart and the
Chapter 44 Echocardiography in Congenital Heart Disease John L. Cotton and G. William Henry Multiple-plane cardiac imaging by echocardiography can noninvasively define the anatomy of the heart and the
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
Double Outlet Right Ventricle with Anterior and Left-Sided Aorta and Subpulmonary Ventricular Septal Defect
 Case Report Double Outlet Right Ventricle with Anterior and Left-Sided rta and Subpulmonary Ventricular Septal Defect Luciana Braz Peixoto, Samira Morhy Borges Leal, Carlos Eduardo Suaide Silva, Sandra
Case Report Double Outlet Right Ventricle with Anterior and Left-Sided rta and Subpulmonary Ventricular Septal Defect Luciana Braz Peixoto, Samira Morhy Borges Leal, Carlos Eduardo Suaide Silva, Sandra
13/06/ Year Old Man BAV Valvotomy Age 7 Years. 47-Year Old Man. Patent Ductus Arteriosus
 2018 MFMER slide-1 2018 MFMER slide-3 2018 MFMER slide-5 2018 MFMER slide-2 2018 MFMER slide-4 2018 MFMER slide-6 47-Year Old Man BAV Valvotomy Age 7 Years Congenital Heart Disease Workshop The aorta will
2018 MFMER slide-1 2018 MFMER slide-3 2018 MFMER slide-5 2018 MFMER slide-2 2018 MFMER slide-4 2018 MFMER slide-6 47-Year Old Man BAV Valvotomy Age 7 Years Congenital Heart Disease Workshop The aorta will
Adults with Congenital Heart Disease
 Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Adults with Congenital Heart Disease Edward K. Rhee, MD, FACC Director, Pediatric-Adult Congenital Arrhythmia Service SJHMC Disclosures & Disclaimer I have no lucrative financial relationships with industry
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Double outlet right ventricle: navigation of surgeon to chose best treatment strategy
 Double outlet right ventricle: navigation of surgeon to chose best treatment strategy Jan Marek Great Ormond Street Hospital & Institute of Cardiovascular Sciences, University College London Double outlet
Double outlet right ventricle: navigation of surgeon to chose best treatment strategy Jan Marek Great Ormond Street Hospital & Institute of Cardiovascular Sciences, University College London Double outlet
Notes: 1)Membranous part contribute in the formation of small portion in the septal cusp.
Membranous part contribute in the formation of small portion in the septal cusp.") Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
Embryology 9 : Slide 16 : There is a sulcus between primitive ventricular and bulbis cordis that will disappear gradually and lead to the formation of one chamber which is called bulboventricular chamber.
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
How to Recognize a Suspected Cardiac Defect in the Neonate
 Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Neonatal Nursing Education Brief: How to Recognize a Suspected Cardiac Defect in the Neonate https://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/
Adult Congenital Heart Disease T S U N ` A M I!
 Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Adult Congenital Heart Disease T S U N ` A M I! Erwin Oechslin, MD, FRCPC, FESC Director, Congenital Cardiac Centre for Adults University Health Network Peter Munk Cardiac Centre / Toronto General Hospital
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging
 Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
Total Anomalous Pulmonary Venous Connections: Anatomy and Diagnostic Imaging Timothy Slesnick, MD March 12, 2015 Congenital Cardiac Anesthesia Society Annual Meeting Disclosures I will discuss the use
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations