PALS PROVIDER Course Study Guide/Pre-Test
|
|
|
- Avice Manning
- 6 years ago
- Views:
Transcription

1 PALS PROVIDER Course Study Guide/Pre-Test *PLEASE COMPLETE AND BRING THIS DOCUMENT WITH YOU TO CLASS* Heartland CPR, llc 8101 NW 10 th St, Suite #C3 Oklahoma City, OK *source: American Heart Association PALS Provider Manual supplementary material

2 PR interval: QRS complex: QT interval: Measures fro the beginning of the P wave to the beginning of the Q wave Normal: sec Measures from the beginning of the Q wave to the end of the S wave Normal: <0.12 sec Measures from the beginning of the Q wave to the end of the T wave Normal: Needs to be corrected for heart rate usually 0.44 to 0.32 sec (heart rate of bpm for both men and women) Intrinsic Rates: SA Node AV Node PF Method for estimating heart rate

3 To estimate heart rate, memorize the rate intervals: 300, 150, 100, 75, 60, 50, 40, and 30. This method estimates heart rate. Although there are other methods and tools available, this method does not require a 3-second or 6-second strip and it can be used easily at the bedside. 1. Pick a complex that falls on a heavy line 2. Estimate the rate by counting heavy boxes 3. Using 300, 150, 100, 75, 60, 50, 40, 30 Other heart rate measurements that can be used: Count the number of QRS complexes (R waves) on a 6-second strip and multiply by 10 Divide 300 by the number of large boxes between 2 consecutive QRS complexes (R waves) Divide 1500 by the number of tiny boxes between 2 consecutive QRS complexes (R waves) For atrial rate measurements, use the methods indicated above with P waves substituted for QRS complexes (R waves). Normal atrial rate: Normal ventricular rate:
4

5 1. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Regular; P to P is regular, bpm Regular; R to R is regular, bpm P wave before every QRS complex Unchanged unless aberrant conduction due to premature beat or increased rate PR: sec QRS: <0.12 sec Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:


6 2. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Regular; P to P is regular, <60 bpm Regular; R to R is regular, <60 bpm P wave before every QRS complex Unchanged unless aberrant conduction due to premature beat or increased rate PR: sec QRS: <0.12 sec Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:

7 3. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Regular; P to P is regular, >100 bpm Regular; R to R is regular, >100 bpm P wave before every QRS complex Unchanged unless aberrant conduction due to premature beat or increased rate PR: sec QRS: <0.12 sec Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:



8 4. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Regular; P to P is regular if P waves can be dentified, bpm Regular; R to R intervals are regular, bpm Difficult to detect or hidden because of the fast heart rate Unchanged unless aberrant conduction due to premature beat or increased rate PR: not measureable QRS: <0.12 sec Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:



9 5. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Absent Absent Absent Absent PR: absent QRS: absent Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:

10 6. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Obscured (see discussion below) Regular; R to R intervals are regular, >150 bpm Obscured (see discussion below) Wide and bizarre, unchanged unless aberrant conduction due to premature beat or increased rate PR: absent* QRS: >0.12 sec *Learn More-Advanced ECG. The rhythm strip here emphasizes the regular wide complex tachycardia (WCT) aspect of VT. In most patients a WCT will be ventricular tachycardia, especially with older age and history of cardiac disease or acute chest discomfort. In these settings, presume and treat as VT. With advanced rhythm training, you will learn that WCTs may be abnormally conducted supraventricular rhythms and look like VT. Careful examination of a rhythm strip attempts to identify atrioventricular dissociation (not shown here). The atria in VT continue to contract in most instances, and the atrial and ventricular impulses are dissociated. This leads to the footprints identifying VT on rhythm strips. These are (1) AV dissociation observed as P waves marching through the wide complexes and occasional fusion or Dressler s beats. Fusion beats occur when the atrial contraction by chance conducts part of the QRS complex. This also is an indication of independent atrial depolarization and AV dissociation. Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:

11 7. Atrial rate: Ventricular rate: P waves: QRS: Intervals: Absent Absent Absent Absent PR: absent QRS: absent Regular or irregular: P waves present: Atrial rate: Ventricular rate: PR interval: QRS interval: Notes:
12 8. Using a manual defibrillator and paddles in the pediatric setting, when would it be most appropriate to use the smaller pediatric sized paddles for shock delivery? a. if the patient weighs less than approximately 25 kg or is less than 8 years of age b. if the patient weighs less than approximately 10 kg or is less than 1 year of age c. whenever you can compress the victim s chest using only the heel of one hand d. to attempt synchronized cardioversion but not defibrillation 9. A pale and obtunded 3-year-old child with a history of diarrhea is brought to the hospital. Primary assessment reveals respiratory rate of 45/min with good breath sounds bilaterally. Capillary refill is 5 seconds and peripheral pulses are weak. After placing the child on a nonrebreathing face mask (10 L/min flow) with 100% Oxygen and obtaining vascular access, which of the following is the most appropriate immediate treatment for this child? a. administer a Dopamine infusion at 2 5 mcg/kg per minute b. obtain a chest x-ray c. begin a maintenance Crystalloid infusion d. administer a bolus of 20 ml/kg Isotonic Crystalloid 10. What is the correct chest compression rate per minute for infants and children? a. 90 to 100 compressions per minute b. 100 compressions per minute c. At least 100 compressions per minute d. 100 to 120 compressions per minute 11. Which of the following statements most accurately reflects the PALS recommendations for the use of Magnesium Sulfate in the treatment of cardiac arrest? a. Routine use of Magnesium Sulfate is indicated for shock-refractory monomorphic VT b. Magnesium Sulfate is indicated for Torsades de Pointes and VF/pulseless VT associated with suspected Hypomagnesemia c. Magnesium sulfate is indicated for VF refractory to repeated shocks and Amiodarone or Lidocaine d. Magnesium Sulfate is contraindicated in VT associated with an abnormal QT interval during the preceding Sinus Rhythm 12. Which of the following statements about Calcium is true? a. Calcium Chloride 10% has the same bioavailability of elemental Calcium as Calcium Gluconate in critically ill children b. routine administration of Calcium is not indicated during cardiac arrest c. the recommended dose is 1 2 mg/kg of Calcium Chloride d. indications for administration of Calcium include Hypercalcemia, Hypokalemia, and Hypomagnesemia
13 13. Which of the following statements about Endotracheal drug administration is true? a. Endotracheal drug administration is the preferred route of drug administration during resuscitation because it results in predictable drug levels and drug effects b. Endotraceal doses of resuscitation drugs in children have been well established and are supported by evidence from clinical trials c. Intravenous drug doses for resuscitation drugs should be used whether you give the drugs by the IV, Intraosseous (IO), or the Endotracheal route d. Endotracheal drug administration is the least desirable route of administration because this route results in unpredictable drug levels and effects 14. Initial impression of a 2-year-old female reveals her to be alert with mild breathing difficulty during inspiration and pale skin color. On primary assessment, she makes high-pitched inspiratory sounds (mild stridor) when agitated; otherwise her breathing is quiet. Her Sp02 is 95% and she has adequate distal breath sounds bilaterally. Which of the following would be the most appropriate treatment? a. administer humidified supplementary Oxygen as tolerated and continue evaluation b. perform immediate endotracheal intubation c. nebulize 2.5 mg of Albuterol d. administer an IV dose of Dexamethasone 15. An infant with a history of vomiting and diarrhea arrives by ambulance. During your primary assessment the infant responds only to painful stimulation. The upper airway is patent, the respiratory rate is 40/min with good bilateral breath sounds, and 100% oxygen is being administered. The infant has cool extremities, weak pulses and a capillary refill time of more than 5 seconds. The infant s blood pressure is 85/65 mm Hg and glucose concentration is 30 mg/dl (1.65 mmol/l). Which of the following is the most appropriate treatment to provide for this infant? a. Establish IV or IO access, administer 20 ml/kg Isotonic Crystalloid over minutes, and simultaneously administer D25W 2 4 ml/kg in a separate infusion b. Perform endotracheal intubation and administer Epinephrine 0.1 mg/kg 1:1000 via the endotracheal tube c. Establish IV or IO access and administer 20 ml/kg Lactated Ringer s solutions over 60 minutes d. Establish IV or IO access and administer 20 ml/kg D50.45% Sodium Chloride bolus over 15 minutes
14 16. You enter a room to perform and initial impression of a previously stable 10-year-old male and find him unresponsive and apneic. A code is called and bag-mask ventilation with 100% oxygen. The cardiac monitor shows a wide-complex Tachycardia. The boy has no detectable pulses so compressions and ventilations are provided. As soon as the defibrillator arrives you deliver an unsynchronized shock with 2 J/kg. The rhythm check after 2 minutes of CPR reveals VF. You then deliver a shock of 4 J/kg and resume immediate CPR beginning with compressions. A team member had established IO access, so you give a dose of Epinephrine, 0.01 mg/kg (0.1 ml/kg of 1:10000 dilution) IO when CPR is restarted after the second shock. At the next rhythm check, persistent VF is present. You administer a 4 J/kg shock and resume CPR. Based on the PALS Pulseless Arrest Algorithm, what are the next drug and dose to administer when CPR is restarted? a. Epinephrine 0.1 mg/kg (0.1 ml/kg of 1:1000 dilution) IO b. Amiodarone or Lidocaine c. Magnesium Sulfate mg/kg IO d. Atropine 0.02 mg/kg IO 17. Parents of a 1-year-old female phoned 911 when they picked up their daughter from the babysitter. Paramedics perform an initial impression revealing an obtunded infant with irregular breathing, bruises over the abdomen, abdominal distention, and cyanosis. Assisted bag-mask ventilation with 100% Oxygen is initiated. On primary assessment heart rate is 36/min, Sinus Bradycardia. Chest compressions are started with a 15:2 compression-to-ventilation ratio. The heart rate is now up to 150/min but there are weak central pulses and no distal pulses. Systolic blood pressure is 74 mm Hg. Of the following, which would be most useful in management of this infant? a. Atropine 0.02 mg/kg IV b. rapid bolus of 20 ml/kg of Isotonic Crystalloid c. synchronized cardioversion d. Epinephrine 0.01 mg/kg (0.1 ml/kg of 1:10000 dilution) IV 18. Which of the following most reliably delivers a high (90% or greater) concentration of inspired Oxygen in a toddler or older child? a. simple oxygen mask with 15 L/min Oxygen flow b. nasal cannula with 4 L/min Oxygen flow c. non-rebreathing face mask with 12 L/min Oxygen flow d. face tent with 15 L/min Oxygen flow 19. You are supervising another healthcare provider who is inserting an intraosseous (IO) needle into an infant s tibia. Which of the following signs should you tell the provider is the best indication of successful insertion into the bone marrow cavity? a. you are unable to aspirate any blood through the needle b. once inserted, the needle shaft moves easily in all directions within the bone c. fluids can be administered freely without local soft tissue swelling d. pulsatile blood flow will be present in the needle hub
15 20. Initial impression of a 9-year-old male with increased work of breathing reveals the boy to be agitated and leaning forward on the bed with obvious respiratory distress. You determine that he has asthma but does not carry an inhaler. He has nasal flaring, severe suprasternal muscular usage, and Sp02 is 96% (on non-rebreathing mask). What is the next medical therapy to provide to this patient? a. Amiodarone 5 mg/kg IV/IO b. Adenosine 0.1 mg/kg c. Procainamide 15 mg/kg IV/IO d. Albuterol by nebulization 21. You are called to help resuscitate an infant with severe symptomatic Bradycardia associated with respiratory distress. The Bradycardia persists despite establishment of an effective airway, oxygenation, and ventilation. There is no heart block present. Which of the following is the first drug you should administer? a. Dopamine b. Epinephrine c. Adenosine d. Atropine 22. A 7-year-old boy is found unresponsive, apneic, and pulseless. CPR is ongoing. The child is intubated and vascular access is established. The ECG monitor reveals an organized rhythm, but a pulse check reveals no palpable pulses. Effective ventilations and compressions are resumed, and an initial IV dose of Epinephrine is administered. Which of the following therapies should you perform next? a. attempt defibrillation at 4 J/kg b. attempt to identify and treat reversible causes (using the H s and T s as a memory aid) c. administer synchronized cardioversion at 1 J/kg d. administer Epinephrine 0.1 mg/kg IV (0.1 ml/kg of 1:1000 dilution) 23. Which of the following statements about the effects of Epinephrine during attempted resuscitation is true? a. Epinephrine improves coronary artery perfusion pressure and stimulates spontaneous contractions when Asystole is present b. Epinephrine decreases myocardial oxygen consumption c. Epinephrine decreases peripheral vascular resistance and reduces myocardial afterload so that ventricular contractions are more effective d. Epinephrine is contraindicated in ventricular fibrillation because it increases myocardial irritability
16 24. You are evaluating an irritable 6-year-old girl with mottled color. On primary assessment she is febrile (temperature 40C [104F]), and her extremities are cold (despite a warm ambient temperature in the room) with capillary refill of 5 seconds. Distal pulses are absent and central pulses are weak. Heart rate is 180/min, respiratory rate is 45/min, and blood pressure is 98/56 mm Hg. Which of the following most accurately describes the categorization of this child s condition using the terminology taught in the PALS Provider course? a. Compensated shock associated with Tachycardia and inadequate tissue perfusion b. Compensated shock requiring no intervention c. Hypotensive shock associated with inadequate tissue perfusion d. Hypotensive shock associated with inadequate tissue perfusion and significant hypotension 25. You have just assisted with the elective endotracheal intubation of a child with respiratory failure and a perfusion rhythm. Which of the following provides the most reliable, prompt assessment of a correct endotracheal tube placement in this? a. confirmation of appropriate oxygen and carbon dioxide tensions on arterial blood gas analysis b. auscultation of breath sounds over the lateral chest bilaterally plus presence of mist in the endotracheal tube c. clinical assessment of adequate bilateral breath sounds and chest expansion plus presence of exhaled C02 in a colorimetric detection device after delivery of 6 positivepressure ventilations d. absence of audible breath sounds over the abdomen during positive-pressure ventilation 26. An 18-month-old presents with a 1-week history of cough and runny nose. You perform an initial impression, which reveals a response only to painful stimulation. Respirations have fallen from 65/min to 10/min with severe inspiratory intercostal retractions. The heart rate is 160/min, Sp02 is 65% in room air, and capillary refill is less than 2 seconds. Which of the following is the most appropriate immediate treatment for this? a. administer 100% Oxygen by face mask, obtain an arterial blood gas, and establish vascular access b. establish vascular access and administer 20 ml/kg bolus of Isotonic Crystalloid c. administer 100% Oxygen by face mask, establish vascular access, and obtain a STAT chest x-ray d. open the airway and provide positive-pressure ventilation using 100% oxygen and a bag-mask device
17 27. An 8-year-old child was struck by a car. He arrives alert, anxious, and in respiratory distress. His cervical spine is immobilized, and he received a 10 L/min flow of 100% Oxygen by nonrebreather mask. Blood pressure is 70 mm Hg, and Sp02 84% after Oxygen administration. Breath sounds are absent over the right chest, and the trachea is deviated to the left. He has weak central pulses and absent distal pulses. Which of the following is the most appropriate immediate intervention for this child? a. provide bag-mask ventilation and call for a STAT chest x-ray b. establish IV access and administer a 20 ml/kg normal saline fluid bolus c. perform a needle decompression of the right chest and assist ventilation with a bag and mask if necessary d. perform endotracheal intubation and call for a STAT chest x-ray 28. You are transporting a 6-year-old endotracheally intubated patient who is receiving positivepressure mechanical ventilation. The child begins to move his head and suddenly becomes cyanotic and bradycardic. Sp02 is 65% with good pulse signal. You remove the child from the mechanical ventilator circuit and provide manual ventilation with a bag via the endotracheal tube. During manual ventilation with 100% Oxygen, the child s color and heart rate improve slightly and his blood pressure remains adequate. Breath sounds and chest expansion are present and adequate on the right side, but they are consistently diminished on the left side. The trachea is not deviated and the neck veins are not distended. A suction catheter passes easily beyond the tip of the endotracheal tube. Which of the following is the most likely cause of this child s acute deterioration? a. equipment failure b. tension pneumothorax on the right side c. tracheal tube displacement into the right main bronchus d. tracheal tube obstruction 29. A 3-year-old boy presents with multiple system trauma. The child was an unrestrained passenger in a motor vehicle crash. On primary assessment he is unresponsive to voice or painful stimulation. His respiratory rate is less than 6/min, heart rate is 170/min, systolic blood pressure is 60 mm Hg, capillary refill is 5 seconds, and Sp02 is 75% in room air. Which of the following most accurately summarized the first interventions you should take to support this child? a. open the airway (jaw-thrust technique) while stabilizing the cervical spine, administer positive-pressure ventilation with 100% Oxygen, and establish immediate IV/IO access b. establish immediate vascular access, administer 20 ml/kg Isotonic Crystalloid, and reassess the patient; if the child s systematic perfusion does not improve, administer ml/kg packed red blood cells c. provide 100% Oxygen by simple mask and perform a head-to-toe survey to identify the extent of all injuries; begin an Epinephrine infusion and titrate to maintain a systolic blood pressure of at least 76 mm Hg d. provide 100% Oxygen by simple mask, stabilize the cervical spine, establish vascular access, and provide maintenance IV fluids 30.


18 An 8-month-old male is brought in for evaluation of severe diarrhea and dehydration. The child becomes unresponsive and pulseless. You shout for help and start CPR at a compression rate of at least 100/min and compression-to-ventilation ratio of 15:2. The cardiac monitor shows the above rhythm. The infant is intubated and ventilated with 100% oxygen. An IO line is rapidly established and a dose of Epinephrine is given. Of the following choices for management, which would be most appropriate to give next? a. Normal Saline 20 ml/kg IV rapidly b. Amiodarone 5 mg/kg IO c. defibrillation 2 J/kg d. high-dose Epinephrine 0.1 mg/kg (0.1 ml/kg of 1:1000 dilution), IO 31. You are caring for a 3-year-old with vomiting and diarrhea. You have established IV access. When you place and orogastric tube, the child begins gagging and continues to gag after the tube is placed. The child s color has deteriorated; pulses are palpable but faint and the child is now lethargic. The heart rate is variable (range 44/min to 62/min). You begin bag-mask ventilation with 100% Oxygen. When the heart rate does not improve, you begin chest compressions. The cardiac monitor shows the above rhythm. Which of the following would be the most appropriate therapy to consider next? a. Cardiology consult for transcutaneous pacing b. Atropine 0.02 mg/kg IV c. Epinephrine 0.1 mg/kg (0.1 ml/kg of 1:1000 dilution) IV d. attempt synchronized cardioversion at 0.5 J/kg


19 32. EMS personnel report that the 3-year-old unresponsive, apneic child being transported became unresponsive upon arrival. The child is receiving CPR, including bag-mask ventilation with 100% Oxygen and chest compressions at a rate of at least 100/min. Compressions and ventilations are being coordinated at a ratio of 15:2. You confirm that apnea is present and that ventilation is producing bilateral breath sounds and chest expansion while a colleague confirms absent pulses. Cardiac monitor shows the above rhythm. A biphasic manual defibrillator is present. You quickly use the head-toe length of the child on a length-based, color-coded resuscitation tape to estimate the approximate weight as 15 kg. Which of the following therapies is most appropriate for this child at this time? a. attempt defibrillation at 30 J, then resume CPR beginning with compressions b. establish IV/IO access and administer Epinephrine 0.01 mg/kg (0.1 ml/kg of 1:10000 dilution) IV/IO c. establish IV/IO access and administer Amiodarone 5 mg/kg IV/IO d. establish IV/IO access and administer Lidocaine 1 mg/kg IV/IO 33. A child becomes unresponsive in the emergency department and is not breathing. You provide ventilation with 100% Oxygen. You are uncertain if a faint pulse is present with the above rhythm. What is your next action? a. start an IV and give Atropine 0.01 mg/kg IV b. order transcutaneous pacing c. start high quality CPR, beginning with compressions d. start an IV and give Epinephrine 0.01 mg/kg IV (0.1 ml/kg of 1:10000 dilution)
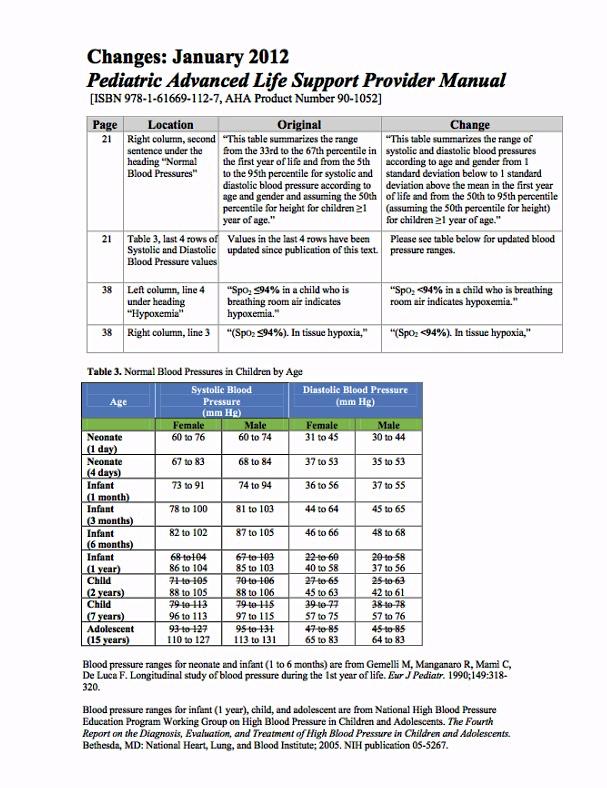
20 34. A 6-year-old female presents to the ER with a 3 day history of fever and is now lethargic. The patient is 20kg, BP 70/34 heart rate is 135 sinus tachycardia, respiratory rate 25bpm, and SpO2 is 94%. You are administering a fluid bolus of normal saline. What would be your next most appropriate action? a. obtain an abdominal CT b. administer antibiotics c. administer vasopressors d. administer glucose 35. You are the team leader for a 10-year-old male in cardiac arrest. The patient is intubated and has an IO in place. You note that Pete is compressing the chest at a rate of 115bpm, to a depth of 3 inches, and is allowing full recoil. What action should you take? a. nothing, Pete if performing the action correctly b. take over compressions c. politely request he adjust his depth to 2 inches d. politely request he decrease his compression rate to 100 bpm 36. What is a tool used for the rapid initial assessment in a pediatric patient? a. Pediatric Assessment Triangle b. Pediatric Glasgow Coma Scale c. Pediatric Assessment Flowchart d. Pediatric Appearance Table 37. You are caring for a 12-year-old that was recently resuscitated from cardiac arrest. He is intubated and is being ventilated with a BVM and O2 at 10lpm, he has an IO established in the L tibia, has received a fluid bolus, 3 rounds of epinephrine, amiodarone, and 2 defibrillation attempts. He remains unconscious, his heart rate is 110 bpm and an EKG reveals sinus intervention? a. initiate targeted temperate management b. administer antibiotics c. increase oxygen and titrate to a saturation of 94% - 99% d. establish an epinephrine drip 38. What would be considered a normal blood pressure for a 7-year-old female? a. 104/62 b. 84/40 c. 140/70 d. 78/30
21 39. You have just assisted in the intubation of an 8-year-old female. Upon reassessment, you note the patient to have a BP of 110/60, a heart rate of 40 sinus bradycardia with no block, and an O2 saturation of 93%. What is the most likely cause of the bradycardia and what is the most appropriate initial treatment? a. stimulation of the vagus nerve; perform compressions b. respiratory failure; administer albuterol c. stimulation if the vagus nerve; provide ventilations via BVM d. stimulation of the vagus nerve; administer atropine 40. What are the most common causes of pediatric cardiac arrest? a. myocardial infarction, hypothermia, and neglect b. hypotensive shock, respiratory failure, and head trauma c. respiratory failure, hypotensive shock, and sudden ventricular arrhythmia d. sudden ventricular arrhythmia, hypotensive shock, and neglect 41. You and a co-worker are caring for a critically ill child. During the course of care, the child declines into pulseless ventricular tachycardia. There is an AED immediately available. What series of actions should occur first? a. call for help, intubate the child, and administer epinephrine b. defibrillate, begin CPR, and call a specialist c. defibrillate, establish IV access, administer epinephrine d. defibrillate, begin CPR, and call for help 42. You and your team are caring for a 5 year old male in cardiac arrest who weights 33lbs. Your team leader requests you to administer 1mEq/kg of sodium bicarbonate via IO. What would be an example of closed loop communication? a. administering sodium bicarb b. okay, got it c. administering 15 miliequivalents of Sodium Bicarbonate d. administering 33 milligrams of Sodium Barcarbonate 43. You are caring for a child in cardiac arrest. CPR is in progress, an IO is in place, an advanced airway is in place, oxygen is being administered, and the patient is in a non-shockable rhythm. What would be the next most appropriate intervention or drug? a. administer 0.01mg/kg of 1:1000 epinephrine IO b. pronounce the patient deceased c. administer 0.01mg/kg of 1:10000 epinephrine IO d. consult a specialist Heartland CPR, llc Page 21 of 23 2/2/17
22 44. You are caring for a 10-year-old female presenting with a 1 week history of fever, cough, and shortness of breath. The patient exhibits a fever of 103F, a heart rate of 128bpm, a BP of 112/70, a respiratory rate of 36, an SpO2 of 88%, and lung sounds reveal crackles on the right inferior field. What is likely to be causing the patient's distress? a. upper airway obstruction b. lower airway obstruction c. lung tissue disease d. disordered control of breathing 45. What is one of the key anatomical differences of a child's airway? a. their larynx is cylindrical b. their tongue is comparatively larger in relation to other structures than an adult c. their airway is situated more posteriorly and superiorly d. there is no difference between an adult and child's airway 46. In which patient would insertion of an OPA be an appropriate intervention? a. 9-year-old female who is unresponsive and without a gag reflex b. 4-year-old male who is awake and alert exhibiting shortness of breath c. 2-year-old female who is unresponsive with a gag reflex d. 12-year-old male who is seizing 47. What is considered to be a normal capillary refill time? a. less than or equal to 5 seconds b. greater than 2 seconds c. less than or equal to 1 second d. leas than or equal to 2 seconds 48. In what situation is it appropriate to move straight to IO access? a. 7-year-old in cardiac arrest b. 4-year-old in compensated shock c. 13-year-old in respiratory distress d. it is never appropriate to perform an IO instead of an IV in pediatric patients Heartland CPR, llc Page 22 of 23 2/2/17
23 A 14 year old male presents to the ER complaining of respiratory distress which began after he was tackled in a game of football. Upon examination, you find the patient to be anxious, exhibiting a respiratory rate of 28, heart rate of 128, BP of 126/62, and an SpO2 of 91%. Lung sounds reveal clear left fields and absent right fields. 49. What is the likely cause of the child's distress? a. pneumonia b. pneumothorax c. asthma d. cardiac tamponade 50. If this child had presented in cardiac arrest, what intervention or medication would be utilized to correct the problem? a. antibiotic administration b. needle decompression c. albuterol administration d. chest tube insertion Heartland CPR, llc Page 23 of 23 2/2/17
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
PALS PRETEST. PALS Pretest
 PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
PALS PRETEST 1. A child with a fever, immune system compromise, poor perfusion and hypotension is most likely to be experiencing which type of shock A. cardiogenic B. Neurogenic C. Septic D. Hypovolemic
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Pediatric Resuscitation
 Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
PALS Study Guide 2016
 Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
Mandatory Precourse Self-Assessment at least 70% pass. Bring proof of completion to class. The PALS Provider exam is 50 multiple-choice questions. Passing score is 84%. Student may miss 8 questions. All
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Pediatric Advanced Life Support
 Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Pediatric Advanced Life Support Pediatric Chain of Survival Berg M D et al. Circulation 2010;122:S862-S875 Prevention Early cardiopulmonary resuscitation (CPR) Prompt access to the emergency response system
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
In accordance with protocols, this patient should be transported to which medical facility?
 NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
NOTE: Please select the most appropriate answer based on the Westchester Regional On-Line Medical Control Physician (OLMC) Regional System Overview, as well as current regional and state EMS protocols
Pediatric Advanced Life Support Overview Judy Haluka BS, RCIS, EMT-P
 Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Pediatric Advanced Life Support Overview 2006 Judy Haluka BS, RCIS, EMT-P General Our Database is lacking in pediatrics Pediatrics are DIFFERENT than Adults not just smaller The same procedure may require
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Learning Station Competency Checklists
 Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Learning Station Competency Checklists Cardiac Arrest: Shockable Rhythm Team Dynamics Practice Demonstrates effective team dynamics (see, below) Performs manual maneuvers to open airway* Initiates assisted
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of
 Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Daniel A. Beals MD, FACS, FAAP Pediatric Surgery and Urology Community Medical Center Associate Professor of Surgery and Pediatrics University of Washington Seattle Children s Hospital Objectives Define
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
ITLS Pediatric Provider Course Advanced Pre-Test
 ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Advanced Pre-Test 1. You arrive at the scene of a motor vehicle crash and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Michigan Adult Cardiac Protocols TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Portage County EMS Patient Care Guidelines. Cardiac Arrest
 Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
PEPP Course: PEPP BLS Pretest
 PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
PEPP Course: PEPP BLS Pretest 1. What is the best way to administer oxygen to a child in moderate respiratory distress? Nasal cannula Simple mask Nonrebreathing mask Bag-valve-mask device 2. A 2-year-old
CETEP PRE-TEST For questions 1 through 3, consider the following scenario:
 CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
CETEP PRE-TEST For questions 1 through 3, consider the following scenario: A two and half month infant comes to the health centre looking very lethargic. Her mother reports that the infant has felt very
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Advanced Cardiac Life Support ACLS
 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation
 Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
Student Guide Module 4: Pediatric Trauma
 Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Student Guide Module 4: Pediatric Trauma Problem based learning exercise objectives Understand how to manage traumatic injuries in mass casualty events. Discuss the features and the approach to pediatric
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Pediatric Assessment Triangle
 Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
Pediatric Assessment Triangle Katherine Remick, MD, FAAP Associate Medical Director Austin Travis County EMS Pediatric Emergency Medicine Dell Children s Medical Center Objectives 1. Discuss why the Pediatric
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Johnson County Emergency Medical Services Page 23
 Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
ITLS Pediatric Provider Course Basic Pre-Test
 ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
ITLS Pediatric Provider Course Basic Pre-Test 1. You arrive at the scene of a motor vehicle collision and are directed to evaluate a child who was in one of the vehicles. The patient appears to be a child
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
 Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Adult Advanced Cardiovascular Life Support. Emergency Procedures in PT
 Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
Protocol Update 2019
 Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Protocol Update 2019 There have been several questions revolving around protocol updates and how they are to be conducted. As many of you are aware there is a protocol submission process in the appendix
Note: See current PALS 2015 guidelines textbook as your PRIMARY Source. Posted November
 PALS PALS Helpful Helpful Hints Courtesy Hints are of Key Courtesy Medical of Resources, Key Medical Resources, www.cprclassroom.com PALS Helpful Hints 2015 Guidelines - December 2016 Mandatory precourse
PALS PALS Helpful Helpful Hints Courtesy Hints are of Key Courtesy Medical of Resources, Key Medical Resources, www.cprclassroom.com PALS Helpful Hints 2015 Guidelines - December 2016 Mandatory precourse
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
2. General Cardiac Arrest Protocol Medical Newborn/Neonatal. Protocol 8-3 Resuscitation 4. Medical Supraventricular
 PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
PEDIATRIC CARDIAC SECTION: Pediatric Cardiovascular Emergencies REVISED: 06/2017 Section 8 1. Cardiac Arrest Unknown Rhythm (i.e. Protocol 8-1 BLS) 2. General Cardiac Arrest Protocol 8-2 3. Medical Newborn/Neonatal
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
MASTER SYLLABUS
 A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005
 RESUSCITATION GUIDELINES 2005") THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
San Benito County EMS Agency Section 700: Patient Care Procedures
 Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
1. What would you do first to restore oxygenation and ventilation to an unresponsive, breathless, near-drowning victim?
 ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
Utah EMS Protocol Guidelines: Cardiac
 Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1
 POST-TEST: Module 1") Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Emergency Triage Assessment and Management (ETAT) POST-TEST: Module 1 For questions 1 through 3, consider the following scenario: A three year old comes with burns to her face and chest after a kerosene
Shifts 28, 29, 30 Quizzes
 Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing
 Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing Simulation Scenario #1 I. Title (ACS)-VF-Asystole-ROSC II. Target learner 6-7 medical students per team
Supplemental Digital Content 1. Simulation scenarios and critical action checklist for debriefing Simulation Scenario #1 I. Title (ACS)-VF-Asystole-ROSC II. Target learner 6-7 medical students per team
Paediatric Advanced Life Support
 Paediatric Advanced Life Support CNHE- Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Pathways leading to cardiac arrest in childhood 2 Age Groups Neonate: Newborn - 28days Infant:
Paediatric Advanced Life Support CNHE- Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Pathways leading to cardiac arrest in childhood 2 Age Groups Neonate: Newborn - 28days Infant:
Because the course covers a lot of material in a short amount of time, there is required prestudy material.
 Thank you for choosing SureFire CPR! This study guide is an outline to help you prepare for your upcoming PALS course. Even though there is a lot of information in this guide, it is important to have your
Thank you for choosing SureFire CPR! This study guide is an outline to help you prepare for your upcoming PALS course. Even though there is a lot of information in this guide, it is important to have your
Pediatric Advanced Life Support (PALS) Study Assistance. A guide for employees of Lake EMS
 Study Assistance. A guide for employees of Lake EMS") Pediatric Advanced Life Support (PALS) Study Assistance A guide for employees of Lake EMS Situation Much of the great care we perform relies on our protocols Our protocols are primarily based on the guidelines
Pediatric Advanced Life Support (PALS) Study Assistance A guide for employees of Lake EMS Situation Much of the great care we perform relies on our protocols Our protocols are primarily based on the guidelines
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Chapter 5 PEDIATRIC RESUSCITATION
 Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
Chapter 5 PEDIATRIC RESUSCITATION Lisa D. Heyden, MD This chapter discusses the 2010 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation and focuses on the resuscitation of pediatric
Manual Defibrillation. CPR AGE: 18 years LOA: Altered HR: N/A RR: N/A SBP: N/A Other: N/A
 ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
ROC AMIODARONE, LIDOCAINE OR PLACEBO FOR OUT OF HOSPITAL CARDIAC ARREST DUE TO VENTRICULAR FIBRILLATION OR TACHYCARDIA (ALPS) STUDY: MEDICAL CARDIAC ARREST MEDICAL DIRECTIVE An Advanced Care Paramedic
SUBCHAPTER 7. STANDING ORDERS FOR ADULT PATIENT Adopted 08/2011 Update 03/2013
 8:41-7.1 Scope SUBCHAPTER 7. STANDING ORDERS FOR ADULT PATIENT Adopted 08/2011 Update 03/2013 The following treatment protocols shall be considered standing orders when treating adult patients. For the
8:41-7.1 Scope SUBCHAPTER 7. STANDING ORDERS FOR ADULT PATIENT Adopted 08/2011 Update 03/2013 The following treatment protocols shall be considered standing orders when treating adult patients. For the
CONTENTS. Page 2 of 57
 CONTENTS List of Figures... 4 List of Tables... 5 Unit One: General Concepts... 6 PALS Preparation... 6 Organization of the PALS Course... 6 2015 PALS Guideline Changes... 7 Changes to Pediatric BLS in
CONTENTS List of Figures... 4 List of Tables... 5 Unit One: General Concepts... 6 PALS Preparation... 6 Organization of the PALS Course... 6 2015 PALS Guideline Changes... 7 Changes to Pediatric BLS in