Educational Resource Advanced Life Support (ALS) Adult
|
|
|
- Harry Howard
- 6 years ago
- Views:
Transcription

")
1 Educational Resource Advanced Life Support (ALS) Adult June 2012
2 TABLE OF CONTENTS Table of Contents... 2 Introduction... 3 Acknowledgements... 3 Advanced Life Support (ALS)... 4 Defibrillation... 6 Medications in adult cardiac arrest... 9 Medications for dysrhythmias Tachyarrhymias Bradyarrhythmia Emergency transcutaneous pacing Intubation in the setting of cardiac arrest Medications for intubation Post-resuscitation care References... 46
3 INTRODUCTION The International Liaison Committee on Resuscitation (ILCOR) was founded on November 22, Its mission is to identify and review international science and knowledge relevant to cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) and when there is consensus to offer treatment recommendations. Researchers from the ILCOR member councils evaluate resuscitation science in 5-year cycles. The most recent International Consensus Conference was held in Dallas in February The Alfred Health Basic and Advanced Life Support Guidelines and Readings aim to provide a comprehensive and consistent approach to the management of cardio-pulmonary resuscitation, and has been developed utilising the evidence-based recommendations from ILCOR (2010), as well as the Australian Resuscitation Council (ARC) policy guideline statements. Chain of Survival The actions linking the adult victim of sudden cardiac arrest with survival are called the adult Chain of Survival. The links in the Chain of Survival used by many resuscitation councils include prevention of the arrest, early recognition of the emergency and activation of the emergency medical services (EMS) system, early and high-quality cardiopulmonary resuscitation (CPR), early defibrillation, rapid advanced life support (ALS), and post-resuscitation care. Introduction and Chain of Survival Acknowledgements A, Ballan, G Bingham, S Brack, E Burke, J Di Nunzio, S Dix, J Gasson, C Glatz, L Howard, M Logan, S Metcalf, S Musgrave, P Ross, G Robers, M Villella, J Watterson, J Williams
4 Advanced Life Support (ALS) ALS is basic life support (BLS) with the addition of defibrillation, intravenous insertion and medications, rhythm recognition and advanced airway management. ARC Advanced Life Support for Adults Flowchart (Figure 1) Shockable rhythms: Non-shockable rhythms: - Ventricular Fibrillation (VF) - Asystole - Pulseless Ventricular Tachycardia (VT) - Pulseless Electrical Activity (PEA) Key points from 2010 ARC Advanced Life Support for Adults flowchart: - Attach defibrillator and identify cardiac rhythm. If shockable shock - Minimise interruption to CPR during interventions - Precordial thump is not part of the ARC flowchart - All Alfred Health defibrillators have evidence to support use of 150 joule shocks during an Emergency Defibrillation - CPR is continued during drug administration and is only interrupted briefly during shocking phase of defibrillation - Attempts to secure airway should not delay CPR and should minimise interruptions to chest compressions - IV access (large bore antecubital fossa preferably) and fluid line should be obtained as soon as possible For shockable rhythms - Adrenaline 1mg should be administered after the second shock then after every second cycle (one cycle is 2 minutes of compressions and ventilations) - Amiodarone 300mg is administered after the third shock For non-shockable rhythms - Adrenaline 1mg should be administered immediately and then after every second cycle - Identify potentially reversible causes and conditions that may precipitate cardiac arrest or decrease the chance of successful resuscitation: Advanced Life Support 4 H s and 4 T s Hypovolaemia Hypoxaemia Hypothermia/Hyperthermia Hyper/hypokalaemia & metabolic disorders Tamponade, cardiac Tension pneumothorax Toxins/poisons/drugs Thrombosis, coronary/pulmonary

5 Figure 1 Adult Advanced Life Support Algorithm.
6 DEFIBRILLATION Defibrillation is the delivery of direct current counter-shock through the heart to simultaneously depolarise the myocardial cells, with the aim of enabling a higher inherent pacemaker to regain organised control of the cardiac rhythm. Defibrillation as soon as possible provides the best chance of survival in victims with VF or pulseless VT (ARC Guideline 11.4, December 2010). It is imperative that the person performing defibrillation is familiar with the operation of the defibrillator being used and is fully aware of the safety aspects required to perform the procedure. Biphasic Defibrillation Biphasic defibrillation delivers the energy waveform in two phases: the current flows in one direction in the first phase of the shock and then reverses direction for the second phase. All new defibrillators deliver shocks using a variety of biphasic waveforms. Although it has not been demonstrated conclusively in randomised clinical studies that biphasic defibrillators save more lives than monophasic defibrillators, biphasic defibrillators achieve higher first-shock success rates. A default biphasic energy level of 200J has been recommended as this falls within the range of published energy levels that have demonstrated efficacy for first and subsequent shocks (ILCOR, 2010). However other energy levels may be used providing there is relevant clinical data for a specific defibrillator that suggests that an alternative energy level provides adequate shock success (Successfully achieving an organised rhythm following first shock in over 90% of cases). Defibrillation All Alfred Health defibrillators have data meeting this for 150J shocks. Indications - VF and Pulseless VT - Fine VF masquerading as Asystole Procedure for Defibrillation - Place the pads on the chest - One hands free pad is placed on the right subclavicular parasternal region over the 2 nd intercostal space, whilst the other is placed on the mid-axilla line at the 6 th intercostal space (cardiac apex). - As it approaches the 2 minute cycle to assess rhythm, CPR must continue until the defibrillator has been charged.
7 Placement of pads - Ensure proper skin preparation and that the pads are not in contact with anything else on the chest (ECG leads, dressings, internal devices, medication patches) as these can cause decreased conduction and burn the patient - Dial the energy select button to 150 joules - Inform all staff that the defibrillator is charging (call out loudly), CPR must continue until the defibrillator has reached 150J - Stop CPR to assess rhythm o If non-shockable rhythm dump charge and immediately continue CPR o If shockable rhythm - - Ensure that the patient is not touching any metal. - Ensure that personnel are not in contact with any fluids on the floor. - Check that the correct energy setting has been selected - Look around the bed area to ensure no-one is touching the patient, recheck the rhythm and shout stand clear shocking - Push the shock button. - Immediately recommence CPR Defibrillation Defibrillation Safety - The person performing the defibrillation is entirely responsible for the safety of the procedure and of all personnel in the vicinity. - Be aware of electrical hazards (water, metal fixtures, oxygen and flammable substances). - Ensure that pads are firmly in place (there must be good contact with the skin). - If the patient has excessive chest hair, it may be necessary to clip or shave chest hair where the pads need to be located. Confirmation of Defibrillation - Check that the patient has a motor response to the defibrillation (if not therapeutically paralysed) indicating that a shock has been delivered. - Evidence of shock delivery will also be seen on the paper print out
8 Failure to Deliver Shock If failure to deliver the shock occurs, troubleshoot the following possible causes: - Defibrillator may be in synchronised mode. - Ensure pads connector is connected to the defibrillator - Check battery is charged. Emergency Synchronised Direct Current Reversion (DCR) The delivery of the shock is synchronised to the R wave on the patient s ECG delivering the shock in the non-vulnerable period of the myocardial action potential. This reduces the risk of causing R on T phenomenon and inducing VF/VT. Indications For haemodynamically compromised patients with the following arrhythmias: - Supra Ventricular Tachycardia (SVT) - Atrial Tachycardia - Atrial Fibrillation with a rapid ventricular response (AF) - Atrial Flutter - Conscious Ventricular Tachycardia (VT). Procedure The technique for synchronised DCR is mostly the same as for non-synchronised defibrillation. The differences between the two are: - Where possible, obtain consent from the patient - Check the patient is adequately sedated with appropriately trained staff to manage the airway - Consider the need to administer analgesia concurrently with sedation - Engage the SYNC button - Check the SYNC function has been engaged: marker is highlighted on the R wave, SYNC is displayed on the screen and the light is flashing. - Select required energy level (25 50 Joules for biphasic defibrillator). Defibrillation Precordial Thump A precordial thump is not part of the ARC Advanced Life Support for Adults flowchart. It may however be considered for patients with monitored, pulseless ventricular tachycardia if a defibrillator is not immediately available. A precordial thump is a single sharp blow delivered to the patient s chest. A precordial thump should not be used in patients with a recent sternotomy (eg. for coronary artery grafts or valve replacement), or recent chest trauma. It serves to deliver approximately 5 Joules of energy to the myocardium. Technique The fist is raised cm above the patient s chest and is brought down sharply at the level of mid-sternum using the ulna aspect of the fist
9 MEDICATIONS IN ADULT CARDIAC ARREST No medication has been shown to improve long-term survival in humans after cardiac arrest. Priorities are defibrillation, oxygenation and ventilation together with cardiac compressions Intravenous (IV) - IV drug administration is preferable - If there are no visible peripheral veins, the external jugular vein should be considered - Avoid lower limb veins due to impairment of venous return below the diaphragm during cardiac arrest - IV drug administration must be followed by a fluid flush of at least ml and CPR Intraosseous (IO) - Is the preferred route if IV access is not available - If IV access cannot be established, IO drug delivery will achieve adequate plasma concentrations Endotracheal - If IV/IO access can not be attained and an endotracheal tube (ETT) is present, some medication can be administered via the ETT - Absorption is variable and plasma concentrations are substantially lower than when the same drug is delivered IV (increase in dose 3-10 times) - Adrenaline, lignocaine and atropine are the only drugs that can be given via the ETT - Dilution with water may achieve better drug absorption - The frequency of administration should be the same as that used for intravenous administration of the above drugs. - This route can not be used if a laryngeal mask is present. Medications in Adult Cardiac Arrest - 9 -
10 ADRENALINE Actions - Naturally occurring catecholamine with alpha and beta effects. - Administered during cardiac arrest to cause peripheral vasoconstriction via its alpha-adrenergic action, thus directing available cardiac output to the brain and myocardium. - It may facilitate defibrillation by improving myocardial blood flow during CPR. Indications - Ventricular fibrillation (VF) / Pulseless ventricular tachycardia (VT) after initial counter shocks have failed (after second shock then after every second cycle) - Asystole and pulseless electrical activity (PEA) immediately (then every second cycle) Dosage - 1 mg (1:10,000 or 1:1000) IV push - May be given via ETT (3 times the dose diluted with ml sterile H 2 O). - Higher doses have not been shown to improve long-term outcomes Adverse Effects - Tachyarrhythmia s - Hypertension post resuscitation - Tissue necrosis at site of extravasation AMIODARONE Actions - First line anti-arrhythmic for VF and pulseless VT - Class III antiarrhythmic agent, having mainly potassium channel blocking properties. It prolongs the refractory period of atrial, nodal, and ventricular tissue by prolonging the action potential duration. - It also effects sodium and calcium channels, and has some alpha and beta adrenergic blocking properties. - Reduces the rate of impulse conduction through the AV node. - Decreases sinus node automaticity. Medications in Adult Cardiac Arrest Indications - VF/pulseless VT (after third shock) - Consider administration for prophylaxis of recurrent VF/VT
11 Dosage and administration - Initial dose is 300 mg IV slow push in the arrest situation - Flush IV access line with 20 ml of 5% glucose prior to and following Amiodarone administration as Amiodarone is incompatible with Normal Saline - For treatment of uncompromised tachyarrhythmias, amiodarone 300mg should be administered as an infusion over 20 to 30 minutes (diluted in 5% glucose) - Additional 150mg IV slow push may be considered 3 5 minutes after first. - May require infusion of 10-50mg/kg over 24 hours Adverse Effects - AV Blocks - Prolonged QT interval - Hypotension - Bradycardia LIGNOCAINE Lignocaine may be used in situations where amiodarone cannot be used or where ventricular ischaemic tissue is the possible cause of arrest. Actions - Class 1b sodium channel blocker. - Shortens action potential duration. - Suppresses automaticity of ventricular ectopic foci. - Action is restricted to ischaemic ventricular myocardial cells. Indications - VF / Pulseless VT refractory to defibrillation - May be used as prophylaxis for recurrent VF or VT Dosage and Administration mg/kg IV slow push. - Additional dose of mg/kg may be considered. - May be given via the ETT. - It is not recommended to commence a lignocaine infusion until return of spontaneous circulation (ROSC) Medications in Adult Cardiac Arrest Adverse Effects - Coma - Seizure activity - Decreases effectiveness of defibrillation - Hypotension
12 CALCIUM Actions - Calcium is essential for normal nerve and muscle activity - Transiently increases myocardial contractility and excitability and systemic vascular resistance. Dosage and Administration - Usual adult bolus dose is 5 to 10 ml of 10% calcium chloride - Alternately 10ml of 10% calcium gluconate Adverse Effects - Possible increase in myocardial and cerebral tissue injury by mediating cell death - Tissue necrosis at site with extravasation Note Routine administration of calcium is not recommended. Consider for Hyperkalaemia, Hypocalcaemia, Calcium channel blocker therapy or overdose MAGNESIUM Actions - Magnesium is an electrolyte essential for maintaining membrane stability - Hypomagnesaemia causes myocardial hyperexcitability, especially in the presence of hypokalaemia and digoxin toxicity Indications - Magnesium should be given for hypomagnesaemia and torsades de pointes, but there is insufficient data to recommend for or against its routine use in cardiac arrest. Consider administration for: - Cardiac arrest associated with digoxin toxicity - VF/pulseless VT (when refractory to defibrillation and adrenaline) - Documented hypokalaemia Dosage and Administration - 5mmol IV slow push - May be repeated once. - Followed by an infusion of 20mmol MgSO4 over 4 hours. Medications in Adult Cardiac Arrest Adverse Effects - Rapid administration of Magnesium may cause asystole or significant clinical hypotension. - Excessive use may cause respiratory failure and respiratory muscle weakness
13 POTASSIUM CHLORIDE Actions - Potassium is an electrolyte essential for maintaining membrane stability - Hypokalaemia, especially in the setting of digoxin therapy and hypomagnesaemia, may lead to life threatening ventricular arrhythmias. Indications: Consider for - Persistent VF due to documented or suspected hypokalaemia Dosage and Administration - Bolus of 5mmol IV slow push Adverse Effects - Excessive use will cause hyperkalaemia with bradycardia, hypotension and possible asystole. - Extravasation may cause tissue necrosis. SODIUM BICARBONATE (NaHCO3) Actions - Sodium Bicarbonate is an alkalising solution used in situations of severe metabolic acidosis - In most cardiac arrests, effective CPR and adequate ventilation negates the need for early use of N a HCO 3. Indications - Treatment of documented metabolic acidosis - Hyperkalaemia - Tricyclic overdose - Prolonged arrest (greater than 15 minutes) Dosage and Administration - 1 mmol per kg is initially given over 2 to 3 minutes, then as guided by arterial blood gases. Adverse Effects - Metabolic alkalosis - Hypokalaemia - Hypernatraemia - Hyperosmolality - Intracellular acidosis - Sodium bicarbonate and adrenaline or calcium when mixed together may inactivate each other and precipitate and block the line Note Routine administration for the treatment of cardiac arrest is not recommended NaHCO3 administration must be accompanied by adequate ventilation and CPR to prevent rebound intracellular acidosis caused by excessive CO 2 production. Medications in Adult Cardiac Arrest
14 MEDICATIONS FOR DYSRHYTHMIAS ATROPINE Actions Atropine is an anticholinergic agent. It blocks parasympathetic innervation, allowing the sympathetic nervous system to dominate. Indications Initial pharmacological treatment for symptomatic patients in: - Severe bradycardia - 2 nd Degree AV block (type II) - Complete heart block Dosage - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg Adverse Effects - Tachyarrhythmias - Pupillary dilatation - Increased intracranial pressure - Urinary retention - Excitement - Delirium Note There will be no response in heart transplantation patients (Consider Isoprenaline) Medications for Dysrhythmias
15 ADENOSINE Actions - Adenosine transiently blocks the conduction of impulses through the AV node interrupting re-entry pathways through the node - It has an extremely short half-life of 0.6 to 10 seconds - It should be given quickly through a large bore cannula in the antecubital fossa or central line as a rapid push followed by a rapid flush - Adverse effects are usually transient and well tolerated because of the short half life Indications - Haemodynamically stable Supraventricular Tachycardia (SVT) - Paroxysmal SVT Contraindications - Second and third degree AV blocks - Sick Sinus Syndrome - Will not revert AF or A/Flutter - Acute Asthma (can precipitate bronchospasm) - Long QT syndrome - Decompensated heart failure Dosage and Administration - Adenosine 6mg rapid IV push followed by 20 ml flush - If there is no response to 6mg give a 12mg bolus followed by a 20 ml flush (which may be repeated) Adverse Effects - Sinus arrest (2 10 seconds) - AV Blocks - Sinus bradycardia - Hypotension - Dyspnoea - Facial flushing - Feelings of impending doom - Headache - Chest pressure/pain Medications for Dysrhythmias

16 VENTRICULAR TACHYCARDIA (VT) Characteristics - Ventricular Tachycardia is a wide complex regular tachycardia - Rhythm originates in the ventricles - Usually occurs as a result of an irritable ventricular focus - Precipitating factors include: AMI, ischaemia, metabolic derangement, acid/base derangement, and cardiomyopathy ECG Characteristics Rate: bpm Rhythm: Regular P Wave: If seen, dissociation is present PR Interval: Not applicable QRS: Wide, greater than 0.14 seconds A patient who has a rhythm of VT on the monitor can be: - Conscious and haemodynamically stable (uncompromised) - Conscious and haemodynamically unstable (compromised) - Pulseless and unconscious Management Conscious stable VT: - 12 lead ECG, continuous cardiac monitoring, oxygen and large bore IVC mg IV amiodarone over 20 to 60 minutes followed by an infusion of 1g over 24 hours - Frequent BP and assessment of GCS - Place hands free defibrillation pads on patient s chest in case of decompensation Conscious Unstable VT: - Continuous cardiac monitoring, oxygen and large bore IVC (x2) - Urgent 12 lead ECG - Airway management - Emergency synchronised cardioversion with sedation, +/-analgesia Cardiac Rhythm Identification & Management Pulseless - Management as per ARC flowchart shockable rhythm (see below: Management of VF)

17 VENTRICULAR FIBRILLATION (VF) Characteristics - Ventricular Fibrillation is chaotic ventricular activity that produces no cardiac output - Irregular and disorganised electrical activity - Rarely is this rhythm self-limiting - Fine VF may masquerade as asystole - Non-synchronous defibrillation has been shown to be the most effective method of terminating this rhythm and should be administered as soon as possible ECG Characteristics Rhythm: chaotic, irregular Rate: unable to be measured as there are no P waves or QRS complexes P wave: absent; wavy irregular deflections; varying size, shape and height; coarse or fine PR interval: not measurable QRS complex: absent Management of shockable rhythms (VF and VT) - Start CPR (30 compressions to 2 breaths) - Attach defibrillator and confirm rhythm is shockable - Shock at 150 joules (single shock) - Immediately recommence CPR and obtain IV access - Continue CPR for 2 minutes - Reassess rhythm and administer 2 nd shock if still in shockable rhythm - Recommence CPR and administer Adrenaline 1mg IV - Administer Adrenaline after every 2 nd cycle (every 4 minutes) - Reassess rhythm and administer 3 rd shock if still in shockable rhythm - Recommence CPR and administer Amiodarone 300 mg IV - Continue CPR and reassess rhythm every 2 minutes - Identify and correct potential causes: 4H s and 4T s - Consider NaHCO3 1mmol/kg IV slowly over 2 to 3 minutes (For prolonged arrests >15mins or when indicated by ABGs). - Continue resuscitation until a perfusing rhythm is re-established or the decision is made to discontinue resuscitation. Cardiac Rhythm Identification & Management
 ECG Characteristics Rate: 200 250 bpm Rhythm: May be regular or slightly irregular P Wave: Not")
18 TORSADE d POINTES Characteristics - Polymorphic Ventricular Tachycardia (VT) - Twisting of the Points - QRS complexes appear to twist or undulate around the isoelectric line - Associated with a prolonged QT interval - Mechanism is as yet unknown - May degenerate into Ventricular Fibrillation (VF) ECG Characteristics Rate: bpm Rhythm: May be regular or slightly irregular P Wave: Not observed PR Interval: Not applicable QRS: Wide, undulating QT Interval: Prolonged. Greater than seconds Management - Confirm rhythm - Commence CPR if no output - Remove any agent known to cause prolonged QT interval (eg Class Ia Antiarrhythmics, sotalol, amiodarone, phenothiazides, some antibiotics (erythromycin), cisapride, tricyclic antidepressants) - Correct electrolyte abnormalities (especially hypokalaemia) - Administer a bolus of 5 mmol of magnesium intravenously over 10 minutes - May be repeated once and followed by an infusion of 20 mmol over four hours - Torsades may also be precipitated by organophosphate poisoning - Defibrillation is often transient in reverting Torsades - Acute cardiac pacing is recommended for patients presenting with torsades de pointes due to heart block and symptomatic bradycardia - If adverse signs develop: immediate synchronised cardioversion Cardiac Rhythm Identification & Management
19 ASYSTOLE Characteristics - The absence of any electrical activity on the monitor - There is also no mechanical activity (cardiac output) and the patient is unconscious - There may be an occasional non-perfusing wide complex beat seen on the monitor - Asystole has a much poorer prognosis than PEA and VF/VT rhythms - Defibrillation is only indicated if there is reason to believe that the asystole may possibly be fine VF. Management - Confirm asystole in at least two leads and absence of cardiac output - Commence CPR - Increase amplitude (could be fine VF) - Obtain IV access - Administer Adrenaline 1mg IV push immediately - Administer Adrenaline 1 mg after every second cycle (every 4 minutes) - Defibrillate if there is a possibility the rhythm could be fine VF - Identify and treat reversible causes: 4 H s and 4 T s o Hypovolaemia o Hypoxaemia o Hyper/hypokalaemia & metabolic disorders o Hypothermia/Hyperthermia o Tamponade, cardiac o Tension pneumothorax o Toxins/poisons/drugs o Thrombosis, coronary/ pulmonary Car diac Rhythm Identification & Management
20 PULSELESS ELECTRICAL ACTIVITY (PEA) Characteristics - Pulseless Electrical Activity is the presence of a normally perfusing electrical rhythm but without a detectable cardiac output. - Caused by a reversible abnormality - Electrical activity on the monitor is a far more favourable rhythm than asystole. Management - Confirm rhythm and absence of cardiac output - Commence CPR - Obtain IV access - Administer Adrenaline 1mg IV push immediately - Administer Adrenaline 1 mg after every second cycle (every 4 minutes) - Identify and treat reversible causes: 4 H s and 4 T s o Hypovolaemia o Hypoxaemia o Hyper/hypokalaemia & metabolic disorders o Hypothermia/Hyperthermia o Tamponade, cardiac o Tension pneumothorax o Toxins/poisons/drugs o Thrombosis, coronary/ pulmonary Cardiac Rhythm Identification & Management

21 TACHYARRHYTHMIAS If the patient has developed a narrow complex tachyarrhythmia and has become symptomatic, there is a need for prompt intervention. If the patient is not haemodynamically compromised, pharmacological reversion or rate reduction of their arrhythmia may be appropriate. Emergency Synchronised Cardioversion is necessary for haemodynamically compromised patients. If the patient fails to maintain a cardiac output (no blood pressure or carotid pulse not palpable), then CPR must be instigated immediately. Cardiac Rhythm Identification & Management
, often triggered by stimulants such as alcohol, caffeine and other drugs, or maybe due to ischaemic heart disease.")
22 SUPRAVENTRICULAR TACHYCARDIA (SVT) Characteristics - Accelerated rhythm originating above the ventricles - Mechanism is often re-entry in nature - Occurs due to pre-excitation syndromes (accessory AV pathways), often triggered by stimulants such as alcohol, caffeine and other drugs, or maybe due to ischaemic heart disease. - Patient often experiences palpitations - Patient may present haemodynamically stable or symptomatic with hypotension or syncope ECG Characteristics Rate: Rhythm: P Wave: Atrial equals the ventricular rate: bpm Regular Usually not visible making the exact mechanism of the tachycardia uncertain PR Interval: Unable to measure as P waves are hidden QRS: Normal morphology, narrow complex Management - In the absence of adverse features, start with vagal manoeuvres - Pharmacological intervention with Adenosine - Adenosine 6mg rapid IV push followed by 20 ml flush, if there is no response to 6mg give a 12mg bolus followed by a 20 ml flush (which may be repeated) - If Adenosine is contraindicated or fails to terminate SVT (without demonstrating it is atrial flutter), give a calcium channel blocker (eg Verapamil 2.5 to 5 mg IV over 2 minutes) - Emergency synchronised cardioversion if the patient is haemodynamically compromised CARDIAC Rhythm Identification & Management
 or fine (small) waves - Atrial kick (loss of 30% of volume in the ventricles before")
23 ATRIAL FIBRILLATION (AF) Characteristics - Ectopic focus in the atria - Atria are depolarised at rapid rates > 400 times per minute - Chaotic, multitude of electrical sites generate impulses uncoordinated activity causing the heart to quiver rather than contract - Fibrillatory waves can be coarse (large) or fine (small) waves - Atrial kick (loss of 30% of volume in the ventricles before systole) is lost due to the quivering - Non-contracting atria also tend to pool blood within the chambers increasing the potential for thrombus formation - AV node can not conduct impulses at such a fast rate, therefore only a percentage of the impulses pass through to the ventricles explaining the irregular ventricular rate - Ventricular rate < 100 bpm - controlled atrial fibrillation - Ventricular rate >100 bpm - atrial fibrillation with a rapid ventricular response - In individuals with healthy hearts usually temporary and may be associated with emotional stress, excessive alcohol or an acute illness (pneumonia, sepsis, PE and thyrotoxicosis). - Chronic AF is commonly caused by valvular heart disease, hypertension, coronary heart disease and post cardiac surgery ECG Characteristics Rhythm: Irregular Rate: Atrial rate > 400 bpm; ventricular rate dependant on the number of impulses conducted through to the ventricles P waves: Fibrillatory waves replace P waves PR interval: Nil QRS complex: Normal Management - Haemodynamically compromised patients : Emergency Synchronised Cardioversion is indicated - Pharmacological treatment for stable patients: Beta blockers, Digoxin, Amiodarone and Verapamil may be used for rate control. Choice of drug will depend on a number of factors including: persistent or permanent AF and presence or absence of heart failure Cardiac Rhythm Identification & Management

24 ATRIAL FLUTTER Characteristics - Atria are depolarised at a rate of approximately 300 times per minute - Waveforms that resemble saw teeth flutter waves - AV node only conducts some of the impulses to protect the ventricles - If the AV node allows every second impulse through the AV junction to the ventricles, then this is a 2:1 conduction (for every two flutter waves only one is followed by a QRS). - Atrial flutter can also have a variable conduction block - 2:1 conduction has a ventricular rate of 150 bpm, 3:1 conduction has a ventricular rate of 100 and 4:1 conduction has a ventricular rate of 75 - Often associated with cardiac disease, cardiomyopathy, ischaemia, congestive cardiac failure ECG Characteristics Rhythm: Usually regular ventricular rate, but a variable AV block will produce an irregular rhythm Rate: Atrial rate approximately 300 bpm Ventricular rate may vary depending on the degree of AV block P Wave: Flutter waves PR Interval: Not measurable QRS complex: Normal morphology and duration Management - Haemodynamically compromised patients : Emergency Synchronised Cardioversion is indicated - Pharmacological treatment for the stable patient may include: Amiodarone, Digoxin, Beta Blockers Cardiac Rhythm Identification & Management
25 BRADYARRHYTHMIAS The definition of a bradyarrhythmia is a heart rate less then 60 beats per minute; however for some people a heart rate of less than 60 beats per minutes is normal. The most common symptoms of bradycardia include: - Syncope - Shortness of breath - Dizziness - Chest pain The following adverse signs suggest a need for immediate treatment: - Systolic BP less than 90 mmhg - Heart rate less than 40 beats per minute and symptomatic - Ventricular arrhythmia - Heart failure - Heart rate less than 60 bpm with signs of poor perfusion A pulseless patient with a bradyarrhythmia (PEA) requires CPR and management according to the ARC Advanced Life Support for Adults flowchart. Rhythms include - Sinus Bradycardia - 1 st Degree AV Block - 2 nd Degree Type I and Type II AV Block - 2:1 AV Block - 3 rd Degree AV Block - Idioventricular Rhythm Cardiac Rhythm Identification & Management

26 Cardiac Rhythm Identification & Management

27 SINUS BRADYCARDIA Characteristics - Caused by increased vagal stimulation or decreased sympathetic tone - Increased ventricular filling time due to prolonged diastole - Relatively benign rhythm - Common in very fit athletic people - Significant bradycardia may cause syncope ECG Characteristics Rate: Rate is less than 60 bpm Atrial rate equals the ventricular rate Rhythm: Regular, unless sinus arrhythmia present P Wave: P wave present before every QRS complex PR Interval: PR interval is between seconds QRS: Present after every P wave and of normal interval of seconds Management - Initial pharmacological treatment for symptomatic patients is Atropine - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg - If Atropine is unsuccessful, adrenaline is the second line agent - Adrenaline is administered at a rate of 2 10 mcg/minute to maintain a satisfactory heart rate and blood pressure Cardiac Rhythm Identification & Management

28 1 ST DEGREE ATRIOVENTRICULAR (AV) BLOCK Characteristics - Sinus Rhythm - Electrical impulses are delayed in the AV node longer than normal (reflected in the longer than normal PR interval) - All impulses are conducted to the ventricles, but with a delayed conduction time ECG Characteristics Rate: Usually between bpm Rhythm: Usually Regular P Wave: P wave present before every QRS complex PR Interval: PR interval is greater than 0.20 seconds QRS: Present after every P wave and of normal interval of seconds Management - May be a normal finding in some individuals - May occur in the setting of Inferior MI - May be associated with Digitalis toxicity - Usually requires no medical intervention If the patient is bradycardiac and symptomatic: - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg Cardiac Rhythm Identification & Management

29 2 ND DEGREE TYPE I AV BLOCK (WENCKEBACH) (MOBITZ TYPE I) Characteristics - Not all atrial impulses are conducted to the ventricles - Mechanism involves the progressive lengthening of the PR interval as a result of AV refractoriness until there is eventual failure to conduct an impulse to the ventricles - After the non-conducted P wave, the sequence begins again - Often transient and rarely progresses to Type II - Often associated with Inferior and Right Ventricular MI, Digitalis toxicity, Post-op cardiothoracic surgery - May occur in very fit, athletic people ECG Characteristics Rate: Atrial rate is greater than the ventricular rate Rhythm: Regularly Irregular P Wave: Normal morphology, regular PR Interval: Progressively lengthens until a QRS is dropped QRS: Normal Interval; does not follow every P wave Management - Monitor patient s cardiac rhythm and cardiac output - Usually transient and does not require medical intervention - Identify and treat any underlying cause(s) If the patient is bradycardic and symptomatic: - Initial pharmacological treatment for symptomatic patients is Atropine - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg Cardiac Rhythm Identification & Management
 or every second P wave not conducted to the ventricles (2:1 regular ventricular rhythm discussed later) - Less common but")
30 2 ND DEGREE TYPE II AV BLOCK (MOBITZ II) Characteristics - Not all atrial impulses are conducted through to the ventricles - Occurs in the Bundle of His or bundle branches - Manifests in two ways: sporadic or regular non-conduction of P waves (irregular ventricular rhythm) or every second P wave not conducted to the ventricles (2:1 regular ventricular rhythm discussed later) - Less common but more serious than Second Degree Type I - Can deteriorate rapidly to third degree AV block or ventricular standstill - Associated with anterior septal MI, conduction system disease, digitalis toxicity ECG Characteristics Rhythm: Atrial rate regular. Ventricular rate usually regular but may be irregular if AV conduction ratios vary Rate: Atrial rate greater than the ventricular rate, can occur at a sinus rate Ventricular rate will depend on number of impulses conducted to ventricles P wave: Present, normal morphology, periodically non-conducted, P P interval is regular PR interval: Normal and constant for conducted beats QRS: May be narrow or wide Management - If the patient is asymptomatic: IV access, continuous cardiac monitoring, frequent observations of BP and GCS and have Atropine and pacing accessible - Initial pharmacological treatment for symptomatic patients is Atropine - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg - If Atropine is unsuccessful, Adrenaline is the second line agent - Adrenaline is administered at a rate of 2 10 mcg/minute to maintain a satisfactory heart rate and blood pressure - Patients who fail to respond to pharmacotherapy may require electrical pacing Cardiac Rhythm Identification & Management
 - Twice as many P waves than QRS complexes - Unable to determine whether 2 nd degree Type I or Type II Management - Monitor cardiac rhythm and cardiac output If the patient is")
31 2:1 AV BLOCK Characteristics - Conduction ratio is 2:1 (number of P waves to QRS complexes) - May involve the AV Node or Sub-Nodal tissue - May be associated with Inferior MI (AV Node) or Anterior MI (Sub-Nodal) - Twice as many P waves than QRS complexes - Unable to determine whether 2 nd degree Type I or Type II Management - Monitor cardiac rhythm and cardiac output If the patient is symptomatic: - Initial pharmacological treatment for symptomatic patients is Atropine - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg - If Atropine is unsuccessful, Adrenaline is the second line agent - Adrenaline is administered at a rate of 2 10 mcg/minute to maintain a satisfactory heart rate and blood pressure - Patients who fail to respond to pharmacotherapy may require cardiac pacing Cardiac Rhythm Identification & Management

32 3 RD DEGREE AV BLOCK (COMPLETE HEART BLOCK) Characteristics - No atrial impulses are transmitted to the ventricles - Atria and ventricles beat independently of each other - AV dissociation - Absolutely no relationship between the atrial and ventricular activity - Atria paced by the sinus node at a sinus rate, ventricles are either paced by an escape pacemaker located in the AV junction at a rate of bpm, or in the ventricles at a rate of bpm (sometimes less) - Patients may be asymptomatic or symptomatic if the ventricular rate is too slow severely decreasing cardiac output resulting in poor organ perfusion - May be temporary or permanent - May result from inferior MI, ischaemic heart disease, drug effects (digitalis and amiodarone), hyperkalaemia or chronic degenerative changes in the conduction system. ECG Characteristics Rhythm: Atrial and ventricular rate are regular Rate: Atrial rate is usually normal Ventricular rate less than atrial rate: rate of bpm (if paced by AV junction), rate of bpm or less (if paced by ventricles) P wave: Sinus P waves with no constant relationship to the QRS, can be found hidden in the QRS complexes and T wave PR interval: Variable QRS complex: Normal if block is located at level of AV node or bundle of His, wide if block located at level of bundle branches Management - Continuous cardiac monitoring and BP and If the patient is symptomatic - Initial pharmacological treatment for symptomatic patients is Atropine - Atropine is administered IV in doses of 500 to 600 mcg - This dose can be repeated every 3 to 5 minutes up to a total of 3 mg - If Atropine is unsuccessful, Adrenaline is the second line agent - Adrenaline is administered at a rate of 2 10 mcg/minute to maintain a satisfactory heart rate and blood pressure - Patients who fail to respond to pharmacotherapy may require temporary pacing Cardiac Rhythm Identification & Management

33 VENTRICULAR STANDSTILL Characteristics - Absence of electrical activity in the ventricles - When the escape pacemaker fails in heart block - There is normal atrial activity with no ventricular activity - There is no cardiac output, pulse or blood pressure and the patient becomes unconscious immediately ECG characteristics Rhythm: No ventricular rhythm Regular atrial rhythm Rate: No ventricular rate Atrial rate is usually normal P waves: Regular, sinus P waves PR interval: Nil QRS complex: Nil Management - Commence CPR - Administer Adrenaline 1mg IV push immediately - Administer Adrenaline 1 mg after every second cycle (every 4 minutes) - Identify and treat reversible causes: 4 H s and 4 T s - External pacing Cardiac Rhythm Identification & Management

34 JUNCTIONAL RHYTHM Characteristics - Delayed heartbeat originating from an ectopic focus in the AV junction - Occurs when the rate of depolarisation of the SA node falls below the rate of the AV node - May also occur due to SA or AV block - May be secondary to digoxin toxicity, cardiac surgery or an inferior MI - May be accompanied by symptoms such as palpitations, fatigue, dyspnoea, presyncope or may be entirely asymptomatic ECG Characteristics Rhythm: Regular Rate: 40 to 60 bpm. May also present as accelerated > 60 bpm P wave: Absent or retrograde presentation PR interval: Not measurable QRS complex: Normal < 0.12 seconds Management - Continuous cardiac monitoring and BP if the patient is symptomatic - Investigation of the cause - Specific suppressive treatment is rarely required as this rhythm serves as a protective mechanism - In patients with complete AV block, high-grade AV block, or symptomatic sick sinus syndrome, a permanent pacemaker may be needed Cardiac Rhythm Identification & Management

35 IDIOVENTRICULAR RHYTHM Characteristics - Arrhythmia originating in a secondary pacemaker site in the ventricle - Escape or rescue rhythm, protective mechanism, impulse initiated when higher pacemaker sites have failed - Lasts for three or more consecutive beats - Usually transient or intermittent - Rate may be increased accelerated idioventricular rhythm - Often seen post myocardial infarction thought to be a reperfusion arrhythmia ECG Characteristics Rhythm: Regular Rate: 30 to 40 bpm (sometimes less) P wave: Absent PR interval: Not measurable QRS complex: Wide > 0.12 seconds Management - Monitor rhythm and cardiac output - Identify cause and treat - Usually requires no therapy, unless patient becomes haemodynamically compromised Cardiac Rhythm Identification & Management

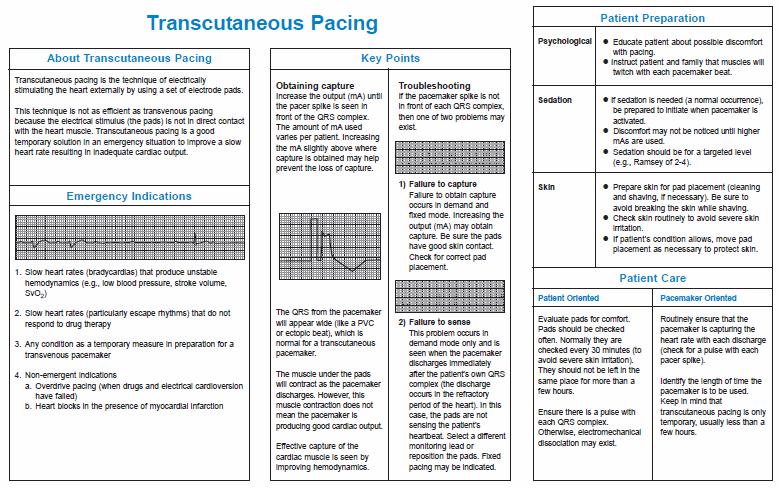
36 EMERGENCY TRANSCUTANEOUS PACING The concept of cardiac pacing is simple: the heart is a muscle that will contract when stimulated by an electrical impulse regardless of the origin of the impulse. Emergency transcutaneous pacing is indicated for those patients that are haemodynamically unstable due to poor cardiac output secondary to an abnormally slow or absent heartbeat and have not responded to medication therapy. Transcutaneous pacing is most effective in patients who have a primary rate related problem and whose myocardial contractibility is effective and intact, for example, 3 rd degree heart block. Transcutaneous (External) Pacing Many of the newer defibrillators have built-in external cardiac pacing abilities. It is important to fully understand how to access the functions of and perform the procedure of emergency transcutaneous cardiac pacing. Further details of the machines available at Alfred Health are in Appendix I and II. Procedure for Transcutaneous Pacing - Commence basic life support (BLS) to provide oxygenation, ventilation and circulatory support - Attach the hands free electrode pads to the patient s chest placing them in the anterior apex position (right of sternum, sub-clavicular and 6 th intercostal region over the apex of the heart) - Alternatively the pads may be placed in the anterior posterior position (anterior pad placed to left of sternum at 5 th intercostal space, with posterior pad placed directly between the inferior border of the scapula and spine) - Ensure good contact between pads and skin - Turn dial on defibrillator to pacer - Set pace maker to desired rate (approximately 80 bpm) - Start pacing - Decrease amplitude to 30 ma - Slowly increase amplitude until capture is achieved (a pacing spike before every QRS complex) - Monitor haemodynamic responsiveness to pacing (BP, GCS, Pulse) - Monitor for consistent capture - Consider sedation and/or analgesia if patient becomes responsive or is awake. Anterior pad placement Anterior- posterior pad placement Emergency Transcutaneous Pacing
37 INTUBATION IN THE SETTING OF CARDIAC ARREST There is insufficient evidence to support or refute the use of any specific technique to maintain an airway and provide ventilation in adults with cardiopulmonary arrest. Either bag valve mask (BVM) alone or in combination with tracheal intubation is acceptable ventilation during CPR. Rescuers must weigh the risks and benefits of intubation versus the need to provide effective chest compressions. The intubation attempt will require interruption of chest compressions, however once an advanced airway is in place, ventilation will not require interruption of chest compressions. An attempt at intubation must not interrupt cardiac compressions for more than 20 seconds. Intubation may be deferred until ROSC. OTHER INDICATIONS FOR INTUBATION - Loss of gag/cough reflex; that is, the ability to protect the airway (for example, head injury with GCS <8) to prevent aspiration - Airway obstruction: acute laryngeal oedema, for example, inhalation burns, epiglottitis - Anticipated loss of control of airway, for example, neck trauma, acute stridor - Worsening respiratory distress PREPARATION FOR INTUBATION - Connect an adult air viva with appropriate size mask to oxygen and place at the head of the bed for pre-oxygenation of patient prior to intubation - Select appropriate size ETT (male size 8 to 9 mm and female size 7 to 8 mm) - Open tube and inflate the balloon with a 10 ml syringe to check for patency and no air leak - Deflate cuff - If introducer is requested by person performing intubation, insert adult introducer (stylet) into lumen of the ETT (end of stylet should just sit flush with tip of the ETT bevel) - Apply lubrication to tube - Check laryngoscope handle is securely attached to the blade and light source is adequate - Trache tape to secure ETT - Bougie for difficult intubations - ETCO 2 monitor - Yankauer sucker attached to suction and turned on and at head of bed - Set up cannulation pack if patient not already cannulated (preferably 2 large bore IV cannulae) ml N/Saline primed for drug and flush line (pump IV line) Intubation

38 - Draw up anaesthetic drugs and label syringes - Check portable ventilator connections and settings - Suggested initial settings SIMV (+/- Pressure Support), PEEP 5, Frequency (RR) 10 to 12, FiO2 100%, Tidal Volume 5 to 7 mls/kg CRICOID PRESSURE Cricoid pressure compresses the upper oesophagus decreasing the likelihood of passive regurgitation in the unconscious patient. Cricoid pressure should not be used if there is swelling of the front of the neck from recent trauma or if the anatomy is difficult to define. It should not be performed at any time, if there are active vomiting attempts by the victim. Particularly in the setting of trauma, remember to protect the cervical spine. If feasible, the patient would be in a position that allowed intubation. This may require support under the back of the head. Note: The routine use of cricoid pressure to prevent aspiration in cardiac arrest is not recommended. If cricoid pressure is used during cardiac arrest, the pressure should be adjusted, relaxed, or released if it impedes ventilation or placement of an advanced airway. Identify the cricoid and thyroid cartilages (fig 2). Intubation Upon advice from the person responsible for the airway, place the thumb and middle finger on either side of the cricoid cartilage, with the fingers together and the index finger above, in the space between the cricoid and thyroid cartilages (figure 3). Apply pressure directly backwards and maintain until advised to release
39 MEDICATIONS FOR INTUBATION Rapid Sequence Induction (RSI) is otherwise known as the technique for crash intubation. It is usually performed in an emergency situation and the drugs used include induction agents (sedatives) and paralysing agents. Note: RSI is not used in the cardiac arrest situation. Induction Agents (Sedatives) Sodium Thiopentone is a rapidly acting barbiturate - An intravenous injection of sodium thiopentone causes loss of consciousness within 15 to 30 seconds and lasts for 5 to 10 minutes - Sodium Thiopentone (500 mgs) is prepared by dissolving powder in sterile water and diluted up to 20 ml (25 mg/ml) Recommended dosage is approximately 3 to 7 mg/kg for adults and children. Sodium Thiopentone: - Decreases contractility - Increases heart rate, coronary blood flow and oxygen demand of the heart - Decreases venous tone causing pooling of blood in the peripheral veins (can cause hypotension in hypovolemic patients) Propofol is a short acting anaesthetic agent suitable for induction and maintenance of anaesthesia in adults. - Rapid onset of action, approximately 30 seconds - Propofol can cause hypotension and decreased heart rate Intubation Recommended dosage is 1.0 to 2.5mg/kg for induction by slow intravenous injection. Repeated boluses of 25 mg to 50 mg may be given if required. For maintenance, a continuous infusion of 4 to 12 mg/kg/hr should be commenced. Fentanyl is an opioid analgesic. - Peak analgesic effect occurs within several minutes and duration of action is 30 to 60 minutes Recommended dosage for induction of anaesthesia is 50 to 100 mcg intravenously and repeated at 2 to 3 minutely intervals. Fentanyl can cause bradycardia and muscle rigidity. Midazolam is a short acting sedative used for induction of anaesthesia and for conscious sedation. Midazolam has amnestic properties. Contraindications: myesthesia gravis and hypersensitivity to benzodiazepines. Recommended dosage is 3 to 10 mg by slow IV injection
40 Ketamine is a rapid acting general anaesthetic agent used prior to administration of other general anaesthetic agents - Onset of action is rapid; a 2mg/kg intravenous injection produces anaesthesia within 30 seconds and lasts for 5 to 10 minutes - Elevation of BP begins shortly after injection, reaches a maximum within a few minutes and returns to pre-anaesthetic values within 15 minutes. - Consider use in haemodynamically unstable patients and asthmatics Contraindications: any condition in which a significant elevation in BP would be hazardous. Paralysing Agents Suxamethonium is a short acting depolarising neuromuscular blocking agent. Onset of action is 30 to 60 seconds post IV injection and duration of action is approximately 3 to 7 minutes Recommended dosage is 1 to 2 mg/kg. Contraindications: recent burns, increased potassium levels, severe muscle trauma or allergy. Suxamethonium: - Can cause bradycardia especially with second dose (more common in children), which may be prevented by prior administration of atropine - Increased serum potassium levels by 1mmol/L with greater increases in patients with recent burns, paraplegia and severe muscle trauma - Increased intracranial and intraocular pressure Intubation Vecuronium is an intermediate acting non-neuromuscular blocking agent. - Vecuronium is prepared by dissolving the powder in water immediately prior to use. Recommended dosage: 0.08 to 0.1 mg/kg (2 to 8 mg prn) and will produce relaxation for 15 to 60 minutes. Rocuronium: is an intermediate acting non-depolarising neuromuscular blocking agent - Rocuronium has a relatively fast onset of action, but variable often within 60 seconds post-intravenous injection of 0.6mg/kg and has duration of 30 to 40 minutes. Maintenance dosage: 0.15mg/kg bodyweight
41 ASSISTING WITH INTUBATION Following pre-oxygenation, sedation and paralysis: - Head positioning neck slightly flexed and head extended with pillow under the head and neck, not under the shoulder (if spinal injury is suspected, spinal immobilisation must be maintained throughout procedure) - Apply cricoid pressure (as previously discussed) - Assist with insertion of ETT by passing the laryngoscope, then the Yankauer sucker to clear airway prior to insertion of tube, then the ETT - Once the ETT is inserted, inflate cuff with 10 ml syringe - Connect CO 2 monitor and air viva to ETT - Check capnograph waveform on monitor - Auscultate lungs for equal air entry - Auscultate neck to listen for air leak around cuff - Secure ETT with trache tape - Attach ventilator to ETT - Document size of ETT, length of ETT to lips, ventilator settings and baseline observations - Ensure post ETT insertion CXR is attended and if ETT is advanced or pulled back that the new position of tube is documented. Intubation
42 POST-RESUSCITATION CARE After the return of spontaneous circulation, the resuscitation of the patient does not stop. It is essential that cardiac monitoring and constant maintenance of airway, breathing, and circulation continues. Interventions in the postresuscitation period are likely to significantly influence the final outcome. Hypoxic brain injury, myocardial injury or subsequent organ failure are the predominant causes of morbidity and mortality after cardiac arrest. The aims of therapy after initial resuscitation are to: - Continue respiratory support - Maintain cerebral perfusion - Treat and prevent cardiac arrhythmias - Determine and treat the cause of the arrest Treatment Recommendations Blood pressure - Aim for a BP equal to the patient s usual BP or at least a systolic pressure greater than 100mmHg Oxygenation - Once ROSC has been established, oxygen should be titrated to achieve a SaO2 of 94 98% (confirmed by arterial blood gas analysis). Control of arterial carbon dioxide - Maintain normocarbia - Hyperventilation may be detrimental and should be avoided - Arterial blood gas measurements should be used to titrate ventilation in the immediate post-resuscitation period, rather than end tidal CO 2 levels. Blood glucose control - Several human studies have documented a strong association between high blood glucose after resuscitation from cardiac arrest and poor neurologic outcome - Monitor blood glucose frequently and treat hyperglycaemia (>10mmol/L) with insulin but avoid hypoglycaemia Post Resuscitation Care Prophylactic antiarrhythmics - May be reasonable to continue an infusion of an antiarrhythmic that successfully restored a stable rhythm during resuscitation - If no antiarrhythmic drug was used during resuscitation from a shockable rhythm, an antiarrhythmic drug may be considered to prevent recurrent VF Temperature control and Induced Hypothermia - Induced hypothermia has been shown to be beneficial in some patients still comatose after ROSC
43 - Comatose adult patients with return of spontaneous circulation after an out-of-hospital VF arrest should be cooled to 32 to 34 ºC for 12 to 24 hours. - Induced hypothermia may also benefit comatose adult patients with return of spontaneous circulation after an out-of-hospital cardiac arrest from a non-shockable rhythm or cardiac arrest in hospital - Rapid infusion of ice-cold intravenous fluid 30ml/kg is a safe, feasible and simple method of initially lowering core temperature by up to 1.5ºC, as are application of ice packs - Hyperthermia should be avoided Monitoring and Investigations Central Nervous System - Ensure adequate oxygenation (titrate FiO2 according to SaO2) - Maintain perfusion pressure (MAP) - GCS Cardiovascular System - Avoid persistent hypotension and optimise organ perfusion with inotropic support - Blood for biochemical analysis: U&E, FBE, Troponin I and CK, Magnesium, LFT s, Calcium - Perform 12-lead ECG - Continuous cardiac monitoring - Consider invasive monitoring (Arterial line and CVC line) - Identify complications of CPR (tension pneumothorax and tamponade) Respiratory System - Chest XRAY (check ETT and line position, assess for complications of CPR - pneumothorax, fractured ribs and aspiration) - Assess ABG s and titrate FiO2 accordingly - Mechanical Ventilation, ETCO 2 and PaCO 2 monitoring Post Resuscitation Care Renal System - Consider indwelling catheter for hourly urine measures - Maintain accurate fluid balance - Check Urea &. Creatinine Other considerations - Notify and inform the patient s Parent Unit and the patient s relatives of what has occurred - Inform and reassure the patient - Organise transfer and paperwork - Consider and organise a debriefing for staff involved in the resuscitation and care of the patien

44 APPENDIX I PHILLIPS HEARTSTREAM TRANSCUTANEOUS PACING
45 - 45 -

46 APPENDIX II PHILLIPS HEARTSTART MRX TRANSCUTANEOUS PACING
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005
 RESUSCITATION GUIDELINES 2005") THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
HealthCare Training Service
 HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
HealthCare Training Service Advanced Life Support Exam Time: Perusal Time: 20 minutes 5 minutes Total Marks: 25 Instructions: Read each question carefully. Using a pencil, record your response to each
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
ADVANCED LIFE SUPPORT
 ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
ANSWERS IN ITALICS WITH REFERENCES 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care professionals equipped with a manual defibrillator, the providers
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Department of Paediatrics Clinical Guideline. Advanced Paediatric Life Support. Sequence of actions. 1. Establish basic life support
 Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Paediatric Life Support Sequence of actions 1. Establish basic life support 2. Oxygenate, ventilate, and start chest compression: - Provide positive-pressure ventilation with high-concentration
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Cardiac Pacing. Learning outcomes. Introduction. The cardiac impulse - its formation and its failure CHAPTER. To understand:
 Cardiac Pacing CHAPTER 10 Learning outcomes To understand: The indications for cardiac pacing in the peri-arrest setting How to perform percussion pacing How to apply non-invasive, transcutaneous electrical
Cardiac Pacing CHAPTER 10 Learning outcomes To understand: The indications for cardiac pacing in the peri-arrest setting How to perform percussion pacing How to apply non-invasive, transcutaneous electrical
TEACHING BASIC LIFE SUPPORT (& ALS)
") TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
TEACHING BASIC LIFE SUPPORT (& ALS) Anton Koželj, R.N., B. Sc., lecturer Faculty of Health Sciences, University of Maribor Žitna ulica 15, 2000 Maribor, Slovenia Fact s To know-how to perform basic life
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
Figure 2. Normal ECG tracing. Table 1.
 Figure 2. Normal ECG tracing that navigates through the left ventricle. Following these bundle branches the impulse finally passes to the terminal points called Purkinje fibers. These Purkinje fibers are
Figure 2. Normal ECG tracing that navigates through the left ventricle. Following these bundle branches the impulse finally passes to the terminal points called Purkinje fibers. These Purkinje fibers are
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
 Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Advanced Life Support
 Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Standard Operating Procedure 2.1 Advanced Life Support Position Responsible: Head of Operations CGC Approved: October 2017 Related Documents Further Information 1.0 Background Magpas Resuscitation Policy
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Outline of the 2005 European Resuscitation Council Guidelines
 Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Practice Guidelines Launch Outline of the 2005 European Resuscitation Council Guidelines Mary Rose Cassar, Diane Tabone Introduction Resuscitation guidelines are revised and updated about every 5 years
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
RN-BC, MS, CCRN, FAHA
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! 1 A. Atropine
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
OBJECTIVE. 1. Define defibrillation. 2. Describe Need and history of defibrillation. 3. Describe the principle and mechanism of defibrillation.
 Defibrillators OBJECTIVE 1. Define defibrillation. 2. Describe Need and history of defibrillation. 3. Describe the principle and mechanism of defibrillation. 4. Types and classes of defibrillator 5. Describe
Defibrillators OBJECTIVE 1. Define defibrillation. 2. Describe Need and history of defibrillation. 3. Describe the principle and mechanism of defibrillation. 4. Types and classes of defibrillator 5. Describe
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Advanced Cardiac Life Support G 2010
 Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Pediatric advanced life support. Management of decreased conscious level in children. Virgi ija Žili skaitė 2017
 Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Pediatric advanced life support. Management of decreased conscious level in children Virgi ija Žili skaitė 2017 Life threatening conditions: primary assessment, differential diagnostics and emergency care.
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO
 Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHA Director The Center of Excellence in Education Director of HERO Follow me on Twitter! CEE Med Updates@BarbaraFurryRN Like me on Facebook! What is a
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Paediatric Advanced Life Support SUPERSEDED
 Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
Paediatric Advanced Life Support Introduction There is concern that resuscitation from cardiac arrest is not performed as well as it might because the variations in guidelines for different age groups
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9
 CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
CARDIAC EMERGENCIES Other Cardiac Dysrhythmias C9 ATRIAL FLUTTER Variable rate depending on block. Atrial rate between 250-350, saw-tooth pattern. (see Appendix B for energy settings for bi-phasic low
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Resuscitation Checklist
 Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Resuscitation Checklist Actions if multiple responders are on scene Is resuscitation appropriate? Conditions incompatible with life Advanced decision in place Based on the information available, the senior
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
! YOU NEED TO MONITOR QT INTERVALS IN THESE PATIENTS.
 Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
THE HEART THE CIRCULATORY SYSTEM
 THE HEART THE CIRCULATORY SYSTEM There are three primary closed cycles: 1) Cardiac circulation pathway of blood within the heart 2) Pulmonary circulation blood from the heart to lungs and back 3) Systemic
THE HEART THE CIRCULATORY SYSTEM There are three primary closed cycles: 1) Cardiac circulation pathway of blood within the heart 2) Pulmonary circulation blood from the heart to lungs and back 3) Systemic
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
Cardioversion / Defibrillation / Transcutaneous Pacer Helpful Hints [ZOLL] 2018
![Cardioversion / Defibrillation / Transcutaneous Pacer Helpful Hints [ZOLL] 2018](/thumbs/81/84173335.jpg "Cardioversion / Defibrillation / Transcutaneous Pacer Helpful Hints [ZOLL] 2018") Cardioversion / Defibrillation / Transcutaneous Pacer Helpful Hints [ZOLL] 08 4 Universal cable may be inserted to the side Defib Short Block to perform 0 J check Universal Cable must be connected to APEX
Cardioversion / Defibrillation / Transcutaneous Pacer Helpful Hints [ZOLL] 08 4 Universal cable may be inserted to the side Defib Short Block to perform 0 J check Universal Cable must be connected to APEX
Cardiac Arrhythmias. For Pharmacists
 Cardiac Arrhythmias For Pharmacists Agenda Overview of the normal Classification Management Therapy Conclusion Cardiac arrhythmias Overview of the normal Arrhythmia: definition From the Greek a-, loss
Cardiac Arrhythmias For Pharmacists Agenda Overview of the normal Classification Management Therapy Conclusion Cardiac arrhythmias Overview of the normal Arrhythmia: definition From the Greek a-, loss
The ECG Course. Boone County Fire Protection District EMS Education
 The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
The ECG Course Level I G rated material AV Blocks What Causes AV Block? Long list of bad things that includes ischemia and.. Old age / disease Medications or drugs Electrolyte imbalances Physiologic Blocks
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Chad Morsch B.S., ACSM CEP
 What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
What Is Cardiac Stress Testing? Chad Morsch B.S., ACSM CEP A Cardiac Stress Test is a test used to measure the heart's ability to respond to external stress in a controlled clinical environment. Cardiac
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS