Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
|
|
|
- Beatrice Atkins
- 6 years ago
- Views:
Transcription


1 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists
2 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately first-ever strokes and are recurrent Fifth leading cause of death Leading cause of long-term disability.
3 Epidemiology of stroke 2018 Someone has a stroke every 40 seconds Stroke kills someone every 4 minutes 1 of every 20 deaths in the US From 2004 to 2014 stroke death rate decreased by 28,7 pct and the total number decreased by 11.3 pct Stroke death declines have stalled since 2013 Stroke death rates have increased among Hispanics

4 Epidemiology of stroke 2018
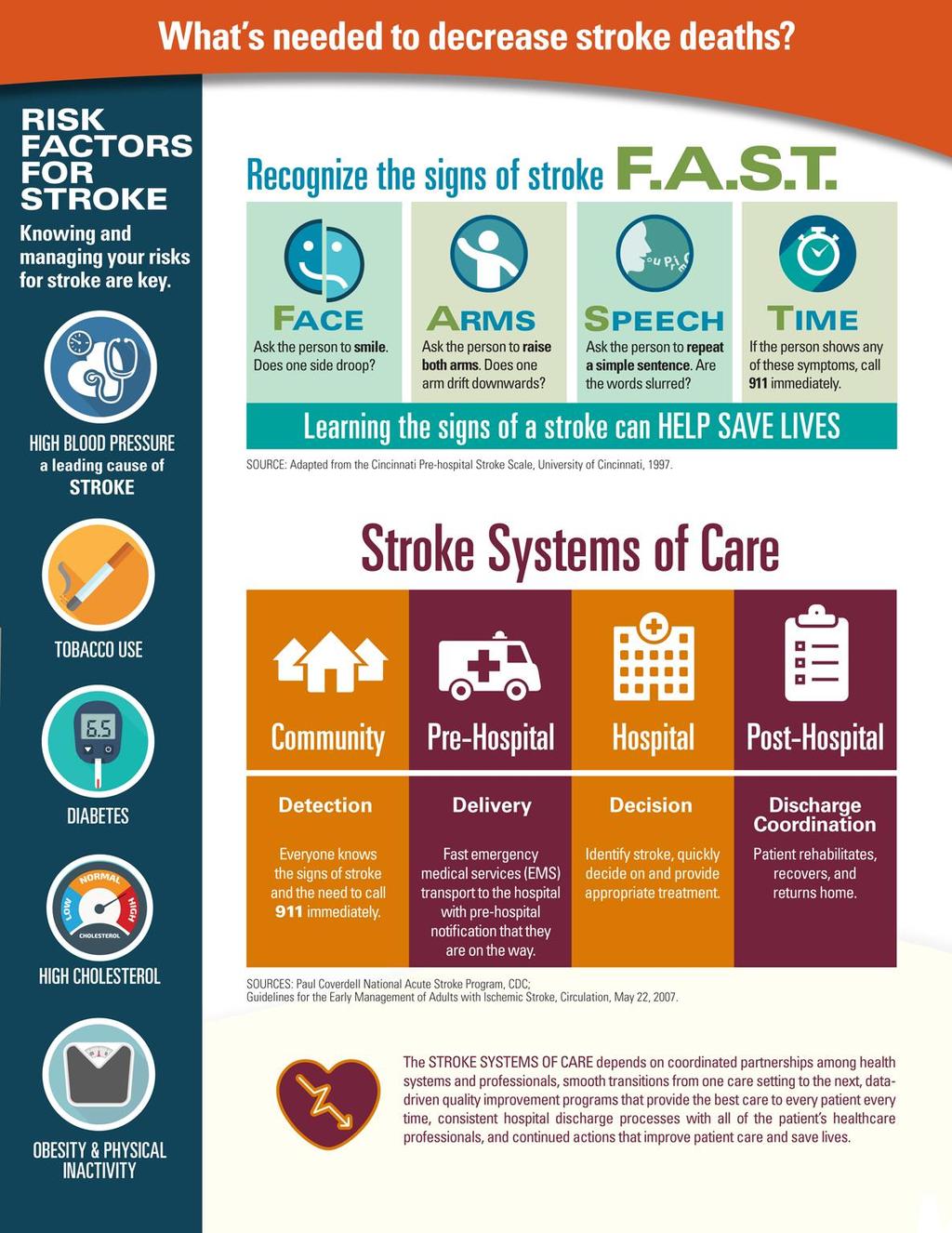
5 Risk Factors Smoking Physical inactivity Nutrition Obesity/Overweight Cholesterol High Blood Pressure Diabetes Mellitus Age (note that 34 pct are less than 65)
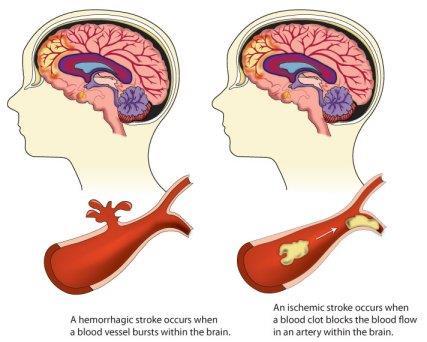
6 Stroke Focal neurological deficit caused by cerebrovascular event lasting at least 24 hours; usually of sudden onset Ischemia: 80-90% (thrombosis, embolism, hypotension) Hemorrhage: 10-20% (subarachnoid, intracerebral)

7 Type of strokes
8 TIA Focal neurological deficit caused by transient ischemia and resolving completely within 24 hours MRI changes in pct of cases pct will have a stroke within 3 months
9 Approach to Treatment of Stroke Does the patient have symptoms and signs consistent with a cerebrovascular event? (DIAGNOSIS) What can be done to limit or reverse the damage? (ACUTE TREATMENT) What can be done to reduce the risk of future events? (PREVENTION) What can we do to augment plasticity? (RECOVERY)
10 Diagnosis Based on history and physical exam Cohort of symptoms/signs referable to a vascular distribution No helpful lab tests, imaging usually normal acutely Non-contrast head CT: hemorrhage vs. ischemia Role of functional imaging for diagnosis? MRA, diffusion weighted MRI +/- perfusion MRI CT angiography, CT perfusion
11 Stroke Mimics Seizure with Todd s paralysis Hypo- or hyperglycemia Complicated migraine Mass lesion Reversible leukoencephalopathy Infection, toxic/metabolic problem superimposed upon a previous deficit Conversion disorder Other Note that up to 30% of patients treated with IVtPA were mimics
12 Stroke Masquerades Altered mental status TIA Vertigo Movement disorder Pain syndromes
13 Accurate Dx vs Metrics What is acceptable miss rate What is acceptable complication rate
14 Diagnostic approach to stroke What How Why
15 The Most Frequent Sites of Arterial and Cardiac Abnormalities Causing Ischemic Stroke Intracranial Atherosclerosis Carotid Plaque With Arteriogenic Emboli Aortic Arch Plaque Cardiogenic Emboli Penetrating Artery Disease Flow Reducing Carotid Stenosis Atrial Fibrillation Valve Disease Left Ventricular Thrombi Albers et al, Chest, 1998.
16 Therapeutic approach to stroke Limiting cellular injury Reperfusion Systemic complication Neurological complications Rehabilitation
17 Pathophysiology Gradient of blood flow reduction: Penumbra: injured but potentially salvageable tissue Mechanisms of ischemic injury in penumbra: Tissue acidosis Excitotoxicity Lipid catabolism/arachadonic acid cascade Free radicals Programmed cell death
18 Reperfusion Blood pressure management Thrombus removal
19 Systemic Complications Aspiration (feeding tube, intubation) DVT (subq Heparin and sequential compression devices) Infection (leading cause of late death) Skin breakdown (repositioning, inflating mattress) Glucose management (an evolving story) Malnutrition (swallow eval, feeding tube) Debilitation (early mobilization and therapy) Other medical co-morbidities
20 Neurologic Complications Increased intracranial pressure Hemorrhagic transformation Cytotoxic edema Edema maximal at hours, usually manifests as decline in level of consciousness Herniation is leading cause of death in acute setting (fatal arrhythmia is second) HEMICRANIECTOMY follow the protocol
21 Rehabilitation
22 Use of tpa
23
24 NINDS trials Dec 1995 NEJM 624 patients over 18 Double-blinded placebo controlled Treated within 3hrs (1/2-90min, ½-90 to 180min) FDA approved in 1996
25 Inclusion and Exclusion Criteria Inclusion Stroke within the first three hours after symptom onset If not witnessed, onset time was when the patient was last seen normal Non-contrast head CT without evidence of hemorrhage (or mass effect, edema) Exclusions Stroke or head trauma within 3 months Major surgery within 14 days Any history of intracranial hemorrhage (ICH) Symptoms suggestive of subarachnoid hemorrhage (SAH) Systolic BP > 185 mmhg Diastolic BP > 110 mmhg Patients were also excluded if aggressive measures were required to lower the blood pressure to within specified limits
26 Exclusions Rapidly improving or minor symptoms Gastrointestinal hemorrhage within 21 days Urinary tract hemorrhage within 21 days Arterial puncture at a noncompressable site within 7 days Seizures at the onset of stroke Patients taking oral anticoagulants
27 Exclusions Heparin within 48 hours AND an elevated PTT Patients with an elevated PT/INR > 1.6 Partial thromboplastin time = PTT; prothrombin time = PT, International Normalized Ratio = INR All of these are laboratory measures of anticoagulation related to heparin or coumadin use Platelet count below 100 x 10⁹/L Blood glucose < 50 mg/dl Blood glucose > 400 mg/dl
28 Time frame BOTTOM LINE: Appropriate patients without contraindications should be treated at 0-3 hours, as per the NINDS study protocol.
29 AHA/ASA new statement 2016 Expanding the use of IV tpa Include older patients >80 Include severe strokes NIHSS >25 (<3hrs) Include mild but disabling strokes (no exclusion) Time hrs (<80,no dm+htn,nihss<25) Rapidly improving symptoms Over 80 still shows better chance of being independent at 3 months Warfarin use (INR<1.7)but not other anti coagulants
30 Other Concerns Rapidly improving but still with moderate impairment Seizures at onset Psychogenic/mimics
31 The new time window hrs Carefully selected patients Age over 80 included Taking Warfarin but less than 1.7 INR Uncertainty if stroke is severe NIHSS >25
32 Evolving Time Window ECASS III: exclude age > 80, NIHSS > 25, diabetics with previous stroke; hrs after onset Benefit for thrombolysis! And beyond 4.5 hours? Data for endovascular therapy out 6-8 hours CALL THE STROKE TEAM OUT TO 8 HOURS
33 Secondary prevention of strokes Prevent medical complications Risk factor modification Especially treatments for HTN, DM, high cholesterol, and smoking cessation Medical or surgical therapy Must know mechanism of stroke Echo to look for cardiac source Imaging to look for carotid source Otherwise, standard anti-platelet therapy
34 Risk factor modification Nonmodifiable Age Race Gender Family history Modifiable HTN DM TIA s/previous strokes? Cardiac disease (?PFO) Atrial fibrillation Hypercholesterolemia Hypercoaguable states Obesity Alcohol/drugs Oral contraceptives Migraine headaches Cigarette smoking Autoimmune/inflammatory disease Homocysteine Sleep apnea
35 Stroke Recovery Rehabilitation Benefit is well established (?) Mechanism by which this facilitates recovery is unclear Begin OT, PT, Speech Therapy immediately Recovery maximal in first weeks, months; can continue INFINITELY (?)
36 Stroke Recovery: Rehabilitation What is remarkable is how much we don t know What predicts recovery? What prevents recovery? What dose of rehab to administer? What we can do besides rehab? How to measure function/recovery?
37
38 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Strategies for Stroke
 Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
Ischemic stroke is a complex disease, the management of which involves features of cardiology, internal medicine and rehabilitative medicine. Is there a thorough, yet simplified, approach to acute ischemic
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
STROKE PROGRAM PATIENT RESOURCE GUIDE
 STROKE PROGRAM PATIENT RESOURCE GUIDE TABLE OF Contents STROKE Prevention Stroke Prevention............................................ 1 Risk Factors for Stroke.......................................1
STROKE PROGRAM PATIENT RESOURCE GUIDE TABLE OF Contents STROKE Prevention Stroke Prevention............................................ 1 Risk Factors for Stroke.......................................1
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
GWTG Post-Discharge Follow-up Form
 Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Types of Stroke and Risk Factors There are two types of stroke, both of which result in a reduction in oxygen reaching the brain.
 Assessment and Management of Stroke Stroke is the fifth leading cause of death, as well as the leading cause of disability for Americans (Davis & Lockhart, 2016). Early evaluation and treatment of stroke
Assessment and Management of Stroke Stroke is the fifth leading cause of death, as well as the leading cause of disability for Americans (Davis & Lockhart, 2016). Early evaluation and treatment of stroke
Cardiovascular Diseases and Diabetes
 Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1
 VERSION 2.1") New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Sex Differences in Stroke Risk and Quality of Life after Stroke
 Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Sex Differences in Stroke Risk and Quality of Life after Stroke Cheryl Bushnell, MD, MHS Associate Professor of Neurology Director, WFB Stroke Center Disclosures Research funding from: World Federation
Recent Changes in IV TPA Recommendations. Ashish Masih, M.D Vascular Neurology
 Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
SHAZIA KHAN Assistant Prof. of Clinical Medicine. USC
 SHAZIA KHAN Assistant Prof. of Clinical Medicine. USC Learning objectives Review the pathophysiology, signs and symptoms of ischemic stroke. Familiarize our selves with the signs and symptoms. Use of ABCD,
SHAZIA KHAN Assistant Prof. of Clinical Medicine. USC Learning objectives Review the pathophysiology, signs and symptoms of ischemic stroke. Familiarize our selves with the signs and symptoms. Use of ABCD,
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Emergently? Michigan Institute for Neurological Disorders. Garden City Hospital, Garden City, Michigan
 Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
Acute ischemic stroke is a major cause of morbidity
 Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the