Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
|
|
|
- Isaac Cummings
- 6 years ago
- Views:
Transcription
1 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09

2 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s: Polio epidemic 1980 s 1990 s 2000 s Positive pressure ventilation with tracheostomy NIV used in COPD Increasing use of NIV in non-copd settings Pierson. Resp Care 2009 NPPV standard of care for COPD exacerbation
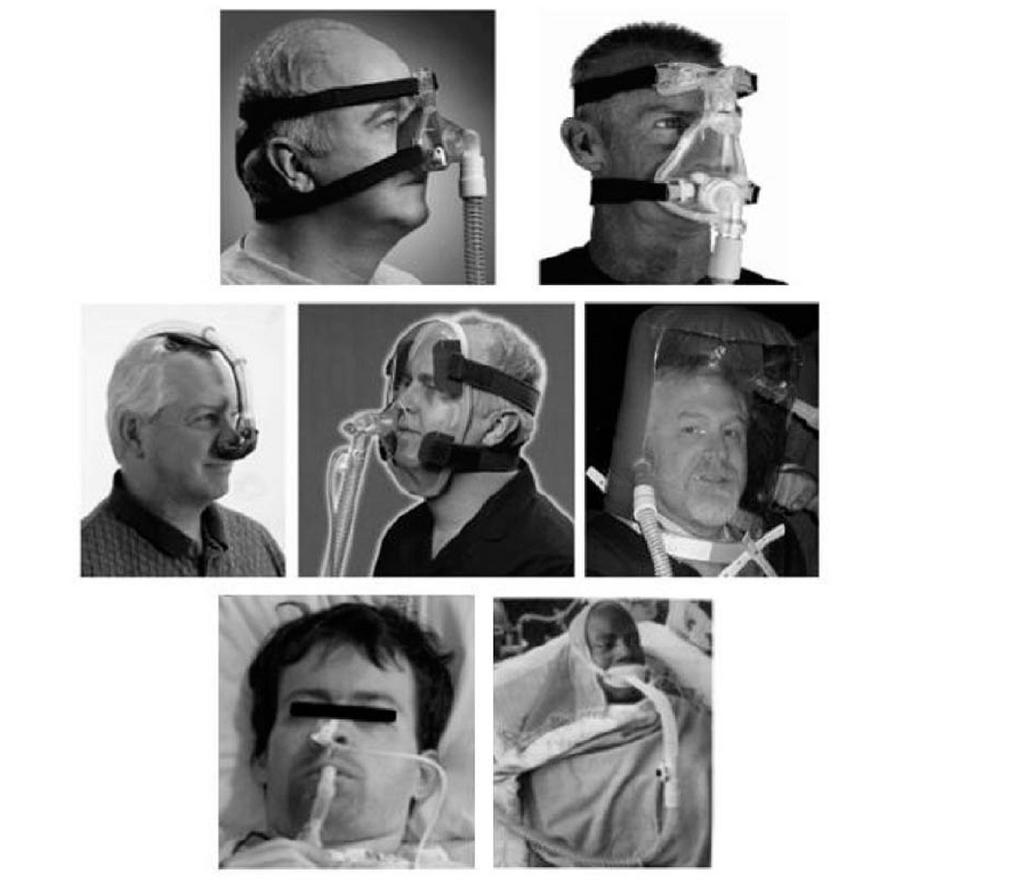
3 Terminology NIV No evidence supporting one specific type of NIV Mask vs nasal Nasal equally effective in increasing FRC Helmet CPAP» More comfortable, allows communication, less claustrophobia NPPV = PSV + PEEP
4
5 Benefits of NIV Reduced infectious complications Multiple PRCT evidence Earlier extubation in COPD patients Potential avoidance of endotracheal intubation Avoidance / reducing need for sedation
6 Risks of NIV Gay. Resp Care 2009
7 NIV for AECOPD 1a evidence: Reduces intubation rates Reduced mortality rate (25 9%) Reduced hospital stays Aspiration events very infrequent NPPV considered first line therapy in this scenario` Plant, et al. Thorax 2001
8 Acute Cardiogenic Pulmonary Edema 1a evidence, Multiple metanalyses and RCT s: CPAP and NPPV lower intubation and mortality rates compared to O2 therapy CPAP should be initial choice for CPE management
9 Immunocompromised patients 1a evidence Reduced mortality rate (50 vs 81%) in immunocompromised ARF patients receiving NIV vs. supplemental O2
10 ARDS Lacking PRCT s No benefit demonstrated with NIV in ARDS Antonelli et al, Crit. Care Med 2007: Prospective observational study 147 ARDS patients treated with NPPV 53% avoided intubation Significantly reduced hospital mortality and VAP compared to those intubated
11 NPPV vs ETI in ARF PRCT: 64 pts. with hypoxemic ARF (medical / surgical) Inclusion: P/F < 200, RR > 35, accessory muscle use PNA, Trauma, Surgical (thoracic, vascular, orthopadic, GI), cardiogenic pulm. edema Exclusion: COPD hemodynamic instability Immunosuppressed neurologic disease > 2 organ system failure Facial deformity. Recent oral, esophageal, or gastric surgery Intervention: NPPV up to 10cm H2O, to maintain Vt 8-10 cc/kg and FiO2 <60% Conversion to ETI: Failure to maintain PaO2 > 65 mmhg Need for airway protection (altered mental status, copious secretions Hemodynamic instability Antonelli, et al. NEJM 1998
12 55% surgical / trauma patients Antonelli, et al. NEJM 1998
13 P/F similar in NIV compared to conventional ventilation Antonelli, et al. NEJM 1998
14 Caveat: Ventilator time NIV failure:15 d NIV success: 2 Control: 6 Results: Success: 69% avoided ETI Decreased PNA & sinusitis rate 3% vs 31% (P = 0.003) 1 patient who failed NPPV No NPPV patients Trend toward reduced mortality and ICU stay in NIV group P= Antonelli, et al. NEJM 1998
15 Chest Trauma RCT (1990): Fewer complications and shorter hospital stay for NIV + epidural compared to ETI PRCT (2005): 43 pts, flail chest: CPAP vs ETI (both with IV sedation): trend toward lower rate pulmonary complications Lower hospital mortality 9% vs 33% (NS) Gunduz, et al. Emerg. Med J. 2005
16 Post-operative use of NIV
17 Extubation failure SICU: 3 6% MICU 12 19% Significance of reducing Extubation Failure 7 X increase in mortality, or 30-40% in hospital mortality in pts requiring re-intubation Epstein, et al. Chest 1997
18 Postoperative respiratory failure: % of cases of respiratory failure VA database Aortic Procedures Non-Aortic procedures < 24hr Post Op Days Thompson, et al. Arch Surg VA centers, 2003: 1021 men undergoing major abdominal surgery ASA III, IV; 32% with COPD; 38% smokers 12% overall respiratory failure (intubation > 24 hrs or re-intubation post-op) (23% aortic, 7% non-aortic cases)
19 Major elective abdominal surgery Multicenter, RCT: CPAP vs standard O2 209 patients, post-op ARF: Inclusion: ARF P/F <300 (1 hr post-op, on FiO2 30%) Laparotomy > 90 minute viscera exposure Whipple, gastrectomy, colectomy, hepatectomy, liver transplant, retroperitoneal mass resection < 80yrs old Exclusion: Cardiac disease (MI, CHF), or recent cardiac / aortic surg. COPD / asthma BMI > 40, h/o infection, immunocompromised state Shock, ARDS, albumin < 3 g/dl, Cr > 3.5mg/dL, Hgb <7 g/dl, ph < 7.3 Intervention: Venturi mask (FiO2 50%) vs. CPAP at 7.5cm H2O Squadrone, et al. JAMA 2005
20 Major elective abdominal surgery P= % (9) NNT: 11 Compare to published re-intubation rate: 5 19% in SICU / Trauma settings Squadrone, et al. JAMA % (1) Indication for intubation: SaO2 < 80% ph < 7.3, pco2 > 50 Patient distress GCS <9 Cardiac arrest Hemodynamic instability
21 Major elective abdominal surgery Significant reduction in PNA and nosocomial infections Mortality rate not significantly affected
22 Post-cardiac surgery 468 CABG and Valve replacement patients Exclusion: EF < 40%, periop MI, post-op pressors, severe COPD, or if intubated > 18 hrs post-op. Randomized to nasal CPAP or Venturi mask + icpap (10 q 4hr) CPAP at 10 cm, at least 6 hrs. (15hrs) Controls received intermittent CPAP 10minuts q4hr Reduced pulmonary complications (PNA, reintubation, P/F <100): 5% vs 10% complication rate in NPPV vs control (P=0.03) 1.3% vs 2.5% reintubation rate Zarbock, et al. Chest 2009;135:1252 (Germany)
23 Thoracoabdominal Aortic Repair 50 patients randomized to standard O2 or ncpap postextubation Intervention: hr ncpap (10cm H20) immediately following extubation Re-intubation rate: 4 vs 16% No mortality data given Kindgen-Milles, et al. Chest 2005;128:821
24 Thoracoabdominal Aortic Repair Hospital LOS reduced by 12 days in ncpap group (P<0.05) Kindgen-Milles, et al. Chest 2005;128:821
25 NPPV in post-operative transplant recipients 5% PNA rate in transplant recipients Crude mortality rate of 37% ETI most important predisposing risk factor for PNA
26 NPPV for post-op ARF in solid organ transplant recipients PRCT: N=40 Liver, Lung, Kidney transplants Inclusion ARF: P/F < 200, RR > 35, accessory muscle use Control: Venturi Mask, FiO2 > 40% Intervention: NPPV, PEEP up to 10cm H2O Target Vt 8-10cc/kg Continuously applied ETI criteria: Failure to maintain PaO2 > 65 mmhg Copious secretions, poor airway protection Antonelli et al. JAMA 2000
27 NPPV in solid organ transplant Mean duration of NPPV: 50hrs Lower re-ntubation rate: 20% vs 70% (P=0.002) Majority intubated within 24 hr of randomization Significantly lower rates of Septic complications Fatal complications ICU mortality Insignificant trend toward fewer PNA in NPPV group (not adequately powered) Antonelli et al. JAMA 2000
28 Post-lung resection PRCT, N = 48: NPPV vs. supplemental O2 S/p lobectomy, bilobectomy, pneumonectomy ARF: P/F < 200, RR > 25 Exclusion: upper airway obstruction, copious secretions, agitation, hemodynamic instability, MOF Level of consciousness and ph not considered NPPV, Vt 8-10 cc/kg Continuous application, avg. 2.1 days 14 hr NPPV per day. Results: Mortality (120 d) Re-intubation rate NPPV No NPPV 12.5% (P=0.045) 37.5% 21% (P=0.035) 50% Auriant, et al. AJRCCM. 2001
29 Subject profile Baseline : Pulmonary Summary of PRCT trials PaCO2 (mmhg) Complication (%) Intervention ph PNA (%) Mortality (%) Treatment failure (%) Esteban NEJM 2004 N = 221 Post-extubation failure (25% surgical/trauma) CPAP vs Supplemental O vs 14 (P = 0.048) 48 vs 47 (NS) Ferrer AJRCCM 2003 N = 105 ARF (PaO2<60) (40% trauma or surgical) BiPAP: 16/7 cmh2o (84hr) vs Venturi mask vs 24 (NS) 20 vs 39 (P=0.025) (90 day) 13 vs 28 (P=0.01) Antonelli NEJM 1998 N=64 ARF (P/F <200) (55% surgical) NPPV (15hr) Vt: 10cc/kg vs ETI; Vt 10cc/kg vs 31 (P=0.003) 31 vs 50 (NS) 31% Squadrone JAMA 2005 N = 209 ARF (P/F < 300) Major abd. Surgery CPAP (19hr) vs Venturi Mask (22hrs) vs 10 (P=0.02) 1 vs 10 (P=0.005) Kindgen- Milles Chest 2005 N = 50 Thoracoabdominal aortic repair Immediate ncpap (22 hr) vs Venturi Mask w IMV 10 q4hr 28 vs 96 P= vs 12 4 vs 16 Zarbock Chest 2009 N = 500 Cardiac surgery Immediate ncpap (9-16hr) vs Venturi mask + IMV 10 q4hr 5 vs 10 P= vs vs 2.5 Auriant AJRCCM 2001 N = 48 ARF (P/F < 200) Lung resection NPPV; Vt: 8-10 cc/kg Vs Supplemental O vs 37.5 (P = 0.045) 21 vs 50 (P=0.035) Antonelli JAMA 2000 N= 40 ARF s/p Transplant (P/F < 200) NPPV (50hr) vs Venturi mask vs 20 (NS) 20 vs vs 70
30 Conflicting trials Esteban, et al. NEJM 2004: Multicenter PRCT, N=221. NNVP for post-extubation failure Compared mask to CPAP Reintubation rate: 48% vs 47% Mortality rate: 24% vs 14% Problems: Only 25% surgical or trauma patients Average ventilator time prior to extubation failure and randomization: 7 days ARF definition (P/F < 160 vs , PaCO2 > 45) Interrupted NVVP (pt.s allowed to drink and discontinue for 20 minutes at a time)
31 Predicting NPPV Failure 1033 COPD exacerbation patients treated with NPPV 77% avoided intubation Post-operative patients excluded Predictors of failure for COPD patients: APACHE score ph RR GCS Confalonieri, et al. Eur Resp. J 2005;25:348


32 Predictors at admission and at 2 hrs 2 hrs after NPPV initiation
33 When to consider NPPV? Medical indications: COPD exacerbation Immunosuppressed Cardiogenic pulmonary edema DNR / DNI patients Surgical patients at risk of re-intubation Prophylactic post-extubation use in thoracoabdominal aortic and cardiac patients
34 Contraindications for NPPV Cardiac or respiratory arrest Inability to protect airway, high risk of aspiration Upper airway obstruction Encephalopathy Severe GI bleed Facial surgery or trauma Severe hemodynamic instability / shock Multiple organ failure ALI / ARDS with severe hypoxemia or acidosis

35 Summary of data PRCT s of surgical patients: reduction in pulmonary complications and PNA reduction in reintubation rates compared to standard therapy
36 Thank You
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Non-invasive Positive Pressure Mechanical Ventilation: NIPPV: CPAP BPAP IPAP EPAP. My Real Goals. What s new in 2018? OMG PAP?
 Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
Non-invasive Positive Pressure Mechanical Ventilation: What s new in 2018? Geoffrey R. Connors, MD, FACP Associate Professor of Medicine University of Colorado School of Medicine Division of Pulmonary
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ
 PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
PAPER DE LA VNI EN LA RETIRADA DE LA VENTILACIÓ INVASIVA I FRACÀS D EXTUBACIÓ Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial
. A randomized controlled trial") CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
NIV in COPD Acute and Chronic Use
 NIV in COPD Acute and Chronic Use Dr C M Chu MD, MSc, FRCP, FCCP Consultant Physician Department of Medicine & Geriatrics United Christian Hospital, Hong Kong NIV in COPD I. AE-COPD/ARF II. III. Weaning
NIV in COPD Acute and Chronic Use Dr C M Chu MD, MSc, FRCP, FCCP Consultant Physician Department of Medicine & Geriatrics United Christian Hospital, Hong Kong NIV in COPD I. AE-COPD/ARF II. III. Weaning
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016
 Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
High Flow Oxygen Therapy in Acute Respiratory Failure. Laurent Brochard Toronto
 High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
High Flow Oxygen Therapy in Acute Respiratory Failure Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical research projects from the
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
Haut debit nasal ou BiPAP? Laurent Brochard Toronto
 Haut debit nasal ou BiPAP? Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical trials from the following companies: General Electric
Haut debit nasal ou BiPAP? Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical trials from the following companies: General Electric
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
To Tube or Not to Tube: Invasive vs Non-Invasive Mechanical Ventilation
 To Tube or Not to Tube: Invasive vs Non-Invasive Mechanical Ventilation Presented by: Mark Rose, BS, RRT (THD Staff RT and Collin College Clinical Instructor) @ 7th Annual SCCM Texas Chapter Symposium
To Tube or Not to Tube: Invasive vs Non-Invasive Mechanical Ventilation Presented by: Mark Rose, BS, RRT (THD Staff RT and Collin College Clinical Instructor) @ 7th Annual SCCM Texas Chapter Symposium
NIV in acute hypoxic respiratory failure
 All course materials, including the original lecture, are available as webcasts/podcasts at www.ers-education. org/niv2009.htm NIV in acute hypoxic respiratory failure Educational aims This presentation
All course materials, including the original lecture, are available as webcasts/podcasts at www.ers-education. org/niv2009.htm NIV in acute hypoxic respiratory failure Educational aims This presentation
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Non-invasive Ventilation
 Non-invasive Ventilation 163 29 Non-invasive Ventilation AM BHAGWATI Artificial ventilatory support has became an integral component in the management of critically ill patients in the intensive care units.
Non-invasive Ventilation 163 29 Non-invasive Ventilation AM BHAGWATI Artificial ventilatory support has became an integral component in the management of critically ill patients in the intensive care units.
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด
 Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Quando la NIV non basta. Andrea Vianello Fisiopatologia e Terapia Intensiva Respiratoria Ospedale-Università di Padova
 Quando la NIV non basta Andrea Vianello Fisiopatologia e Terapia Intensiva Respiratoria Ospedale-Università di Padova Sixty-two RCTs including a total of 5870 patients Overall NIV failure: 16.3% NIV Real
Quando la NIV non basta Andrea Vianello Fisiopatologia e Terapia Intensiva Respiratoria Ospedale-Università di Padova Sixty-two RCTs including a total of 5870 patients Overall NIV failure: 16.3% NIV Real
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Non-Invasive Ventilation
 Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
Khusrav Bajan Head Emergency Medicine, Consultant Intensivist & Physician, P.D. Hinduja National Hospital & M.R.C. 112 And the Lord God formed man of the dust of the ground and breathed into his nostrils
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Alma Mater University of Bologna. Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy
 Alma Mater University of Bologna Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy Conflict of Interest I have affiliations with, special interests, or have conducted business with the
Alma Mater University of Bologna Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy Conflict of Interest I have affiliations with, special interests, or have conducted business with the
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
A study of non-invasive ventilation in acute respiratory failure
 Original Research Article A study of non-invasive ventilation in acute respiratory failure Nilima Manohar Mane 1, Jayant L. Pednekar 2, Sangeeta Pednekar 3* 1 Consultant Physician and Diabetologist, Apollo
Original Research Article A study of non-invasive ventilation in acute respiratory failure Nilima Manohar Mane 1, Jayant L. Pednekar 2, Sangeeta Pednekar 3* 1 Consultant Physician and Diabetologist, Apollo
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
COMPLICACIONS DE LA VENTILACIÓ MECÀNICA NO INVASIVA
 COMPLICACIONS DE LA VENTILACIÓ MECÀNICA NO INVASIVA Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es Barcelona, 3 de novembre
COMPLICACIONS DE LA VENTILACIÓ MECÀNICA NO INVASIVA Dr. Miquel Ferrer UVIIR, Servei de Pneumologia, Hospital Clínic, IDIBAPS, CibeRes, Barcelona. E- mail: miferrer@clinic.ub.es Barcelona, 3 de novembre
WALTER O DONOHUE LECTURE: HUMIDFIED HIGH FLOW CANNULAE OXYGEN THERAPY
 WALTER O DONOHUE LECTURE: HUMIDFIED HIGH FLOW CANNULAE OXYGEN THERAPY NICHOLAS S. HILL, MD PROFESSOR OF MEDICINE TUFTS MEDICAL CENTER BOSTON, MA NICHOLAS S. HILL, MD, is Chief of the Division of Pulmonary,
WALTER O DONOHUE LECTURE: HUMIDFIED HIGH FLOW CANNULAE OXYGEN THERAPY NICHOLAS S. HILL, MD PROFESSOR OF MEDICINE TUFTS MEDICAL CENTER BOSTON, MA NICHOLAS S. HILL, MD, is Chief of the Division of Pulmonary,
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Extubation Failure & Delay in Brain-Injured Patients
 Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults
 BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults British Thoracic Society Intensive Care Society Introduction Acute Hypercapnic Respiratory Failure (AHRF)
BTS/ICS Guidelines for the ventilatory management of acute hypercapnic respiratory failure in adults British Thoracic Society Intensive Care Society Introduction Acute Hypercapnic Respiratory Failure (AHRF)
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Respiratory Failure how the respiratory physicians deal with airway emergencies
 Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione
![Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione](/thumbs/79/78902905.jpg "Tissue is the Issue. PEEP CPAP FiO2 HFNC PSV HFNC. DO 2 = CO [(Hb x 1.34) SaO PaO 2 ] perfusione") Tissue is the Issue perfusione PEEP CPAP FiO2 HFNC PSV HFNC DO 2 = CO [(Hb x 1.34) SaO 2 + 0.003 PaO 2 ] O2 HFNC PEEP CPAP PSV ARF ACPE HIGH FLOW NASAL CANNULA High and Exact FiO2, High Flow heating and
Tissue is the Issue perfusione PEEP CPAP FiO2 HFNC PSV HFNC DO 2 = CO [(Hb x 1.34) SaO 2 + 0.003 PaO 2 ] O2 HFNC PEEP CPAP PSV ARF ACPE HIGH FLOW NASAL CANNULA High and Exact FiO2, High Flow heating and
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. This online publication has been corrected. The corrected
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. This online publication has been corrected. The corrected
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date (DD/MMM/YYYY) (DD/MMM/YYYY) Gender Female Male Date of surgery (DD/MMM/YYYY)
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date (DD/MMM/YYYY) (DD/MMM/YYYY) Gender Female Male Date of surgery (DD/MMM/YYYY)
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Effective Health Care Program
 Comparative Effectiveness Review Number 68 Effective Health Care Program Noninvasive Positive-Pressure Ventilation (NPPV) for Acute Respiratory Failure Executive Summary Background Acute respiratory failure
Comparative Effectiveness Review Number 68 Effective Health Care Program Noninvasive Positive-Pressure Ventilation (NPPV) for Acute Respiratory Failure Executive Summary Background Acute respiratory failure
WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE
 European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
Non-invasive ventilation for surgical patients with acute respiratory failure. Byoung Chul Lee, Kyu Hyouck Kyoung, Young Hwan Kim, Suk-Kyung Hong
 J Korean Surg Soc 2011;80:390-396 DOI: 10.4174/jkss.2011.80.6.390 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Non-invasive ventilation for surgical patients
J Korean Surg Soc 2011;80:390-396 DOI: 10.4174/jkss.2011.80.6.390 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Non-invasive ventilation for surgical patients
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE. Data Collection Forms
 Acute Respiratory Failure Section WEAN SAFE. Data Collection Forms") European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE Data Collection Forms Study ID: Date of Data collection: FORM 0: - ORGANIZATIONAL DATA OF THE PARTICIPATING
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE Data Collection Forms Study ID: Date of Data collection: FORM 0: - ORGANIZATIONAL DATA OF THE PARTICIPATING
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
ORIGINAL ARTICLE. Kai-Yan Yu 1*, Lei Zhao 2*, Zi Chen 3, Min Yang 1. Introduction
 ORIGINAL ARTICLE Noninvasive positive pressure ventilation for the treatment of acute respiratory distress syndrome following esophagectomy for esophageal cancer: a clinical comparative study Kai-Yan Yu
ORIGINAL ARTICLE Noninvasive positive pressure ventilation for the treatment of acute respiratory distress syndrome following esophagectomy for esophageal cancer: a clinical comparative study Kai-Yan Yu
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
Keiko Nakazato 1,2*, Shinhiro Takeda 1,2, Keiji Tanaka 2 and Atsuhiro Sakamoto 1. Abstract
 Nakazato et al. Journal of Cardiothoracic Surgery 2012, 7:41 RESEARCH ARTICLE Open Access Aggressive treatment with noninvasive ventilation for mild acute hypoxemic respiratory failure after cardiovascular
Nakazato et al. Journal of Cardiothoracic Surgery 2012, 7:41 RESEARCH ARTICLE Open Access Aggressive treatment with noninvasive ventilation for mild acute hypoxemic respiratory failure after cardiovascular
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Mechanical Ventilation. Acute Heart Failure. Abdo Khoury MD, MScDM Research Group on Ventilation Inserm 808 CIC-IT
 Mechanical Ventilation in Acute Heart Failure Abdo Khoury MD, MScDM Research Group on Ventilation Inserm 808 CIC-IT Department of Emergency Medicine & Critical Care Franche-Comté University - Medical &
Mechanical Ventilation in Acute Heart Failure Abdo Khoury MD, MScDM Research Group on Ventilation Inserm 808 CIC-IT Department of Emergency Medicine & Critical Care Franche-Comté University - Medical &
Non-invasive ventilation (NIV)
") Non-invasive ventilation And the Lord God formed a man from the dust of the ground, and breathed into his nostrils the breath of life, and the man became a living being. B. Buyse (MD, PhD) Dept. of Pulmonology,
Non-invasive ventilation And the Lord God formed a man from the dust of the ground, and breathed into his nostrils the breath of life, and the man became a living being. B. Buyse (MD, PhD) Dept. of Pulmonology,
Acute Applications of Noninvasive Positive Pressure Ventilation* Timothy Liesching, MD; Henry Kwok, MD, FCCP; and Nicholas S.
 reviews Acute Applications of Noninvasive Positive Pressure Ventilation* Timothy Liesching, MD; Henry Kwok, MD, FCCP; and Nicholas S. Hill, MD, FCCP Noninvasive positive-pressure ventilation (NPPV) has
reviews Acute Applications of Noninvasive Positive Pressure Ventilation* Timothy Liesching, MD; Henry Kwok, MD, FCCP; and Nicholas S. Hill, MD, FCCP Noninvasive positive-pressure ventilation (NPPV) has
ARF. 8 8 (PaO 2 / FIO 2 ) NPPV NPPV ( P = 0.37) NPPV NPPV. (PaO 2 / FIO 2 > 200 PaO 2 / FIO 2 NPPV > 100) (P = 0.02) NPPV ( NPPV P = 0.
 NPPV NPPV ( P = 0.37) NPPV NPPV. (PaO 2 / FIO 2 > 200 PaO 2 / FIO 2 NPPV > 100) (P = 0.02) NPPV ( NPPV P = 0.") Monica Rocco, MD; Donatella Dell'Utri, MD; Andrea Morelli, MD; Gustavo Spadetta, MD; Giorgio Conti, MD; Massimo Antonelli, MD; and Paolo Pietropaoli, MD (ARF) (NPPV) 19 ARF ( 8 8 3 ) NPPV 19 (PaO 2 / FIO
Monica Rocco, MD; Donatella Dell'Utri, MD; Andrea Morelli, MD; Gustavo Spadetta, MD; Giorgio Conti, MD; Massimo Antonelli, MD; and Paolo Pietropaoli, MD (ARF) (NPPV) 19 ARF ( 8 8 3 ) NPPV 19 (PaO 2 / FIO
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Distress During RSV Season
 Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
High Flow Humidification Therapy, Updates.
 High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
ECMO in oncology and immunosupressed patients. Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna
 ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is
ECMO in oncology and immunosupressed patients Peter Schellongowski Department of Medicine I Intensive Care Unit 13.i2 Medical University of Vienna ECMO in immunocompromised patients? Is it feasible? Is