Results from the MAJESTIC clinical trial
|
|
|
- Donald Bailey
- 6 years ago
- Views:
Transcription
, show that an endovascular strategy is cost-effective")
1 Issue 66 June 2015 Michael Dake: Arch branched device Janet Powell: Profile Andrew Holden: Bioresorbable stents Page 2 Page 24 One-year IMPROVE data suggest benefit of EVAR in ruptured aneurysms Results from the 12-month data of the randomised controlled IMPROVE trial, presented for the first time at CX 2015 (28 April 1 May, London, UK), show that an endovascular strategy is cost-effective when compared to open repair in the treatment of ruptured abdominal aortic aneurysms. The one-year data also revealed that the endovascular strategy conferred no survival benefit over open repair, except a trend towards benefitting women. It also showed that the endovascular strategy enabled more patients to be discharged from hospital to home, and significantly faster than with open repair. Patients also have an excellent quality of life with endovascular strategy, if they survive the rupture, delegates heard. Twelve-month outcomes from the individual patient data meta-analysis of three randomised controlled trials of ruptured aneurysms [ie. the Dutch AJAX trial, the French ECAR trial and the UK IMPROVE trial] also showed a trend towards survival benefit for endovascular aneurysm repair (EVAR), but this was not statistically significant. A CX audience poll in the session revealed that nearly 80% agreed that the 12-month results of the IMPROVE trial encouraged them to perform EVAR more often. Janet Powell, Imperial College, London, UK, presented the latest data from the IMPROVE (Immediate management of the patient with rupture: Open vs. endovascular repair) trial that reported one-year outcomes following either a strategy of endovascular repair first or open repair of ruptured abdominal aortic aneurysm. The results demonstrate no survival benefit for the endovascular strategy for ruptured aneurysm at one year. However, an endovascular-first strategy for the management of ruptured aneurysms does offer patients faster discharge with better quality of life and it is also cost-effective. Both these factors are necessary for patient and clinical decision-making, delegates heard. These data were published in April in the European Heart Journal (EHJ). IMPROVE, a pragmatic, multicentre (29 UK and one Canada) trial randomised 613 patients with a clinical diagnosis of ruptured aneurysm, 316 patients to an endovascular-first strategy (if aortic morphology was suitable and open repair if not) and 297 to open repair. Powell also drew attention to CX 2015 voting Do IMPROVE trial results at 12 months encourage you to perform EVAR more often? No 22% Yes 78% the fact that at baseline, the characteristics of the two groups were similar with almost three-quarters in each group being men. The aneurysms in this trial were also very large with average diameters in each group being over 8cm, she said. The principal one-year outcome was mortality and secondary outcomes were reinterventions, hospital discharge, health-related quality-of-life, costs, quality-adjustedlife-years and cost-effectiveness. At CX 2015, Powell noted that the trial was designed to answer the question of what to do with a patient who presents to the emergency room with a diagnosis of ruptured abdominal aortic aneurysm. What we had anticipated was that using an endovascular strategy, wherever it was morphologically feasible, we could reduce 30-day operative mortality from 47% in the open repair group to 33% where endovascular repair was used extensively, she said. Powell added: At one year, all-cause mortality was 41.1% for the endovascular strategy group and 45.1% for the open repair group (p=0.325) with similar reintervention rates in each. A subgroup analysis showed a stronger benefit for the endovascular strategy in women versus men. The endovascular strategy group and open repair groups had average total hospital stays of 17 and 26 days, respectively. The 30-day mortality results, the primary outcome, previously published in the British Medical Journal (BMJ) in 2014, also found no difference in 30-day mortality between the endovascular strategy group and the open repair group and subgroup analysis showed a strong benefit for the endovascular strategy in women compared with men. Pooled individual patient data outcomes Ron Balm presented the 12-month outcomes meta-analysis from the individual patient data from the three randomised controlled trials of ruptured aneurysms; the Dutch AJAX trial (Annals of Surgery 2013), the French ECAR trial (EJVES 2015) and the UK IMPROVE trial. These were all trials that were performed on patients with a clinical suspicion of ruptured aneurysm. In the AJAX trial the 30-day mortality in both groups was approximately 25%, in ECAR it was 22% and in IMPROVE, which had a slightly different study design, it was 35% in each group (BMJ 2014), but all failed to demonstrate the benefit of EVAR in the emergent setting. The results were hampered by the fact that open repair performed so much Continued on page 2 Page 13 New Eluvia drugeluting stent shows 94.4% primary patency rate at nine months Results from the MAJESTIC clinical trial assessing the performance of the Eluvia drug-eluting stent (Boston Scientific) in femoropopliteal artery lesions show a high primary patency rate and low reintervention rate at nine months. The data were presented at the Charing Cross Symposium (28 April 1 May 2015, London, UK). The objective of the MAJESTIC trial was to determine whether the Eluvia drug-eluting stent showed acceptable performance when treating superficial femoral and proximal popliteal artery lesions up to 110mm in length as compared to a literature-derived performance goal, with a primary endpoint of primary patency at nine months. The trial enrolled 57 patients in Europe, Australia and New Zealand. The mean age was 69.3±9.3 years, and the average lesion length was 70.8±28.1mm. Principal investigator Stefan Müller-Hülsbeck, Flensburg, Germany, who presented the results at CX, said that MAJESTIC included a high percentage of complex lesions, and added, It is important to note that 64.9% of lesions were severely calcified and 46.2% were total occlusions. In addition 77% of lesions extended into the distal portion of the superficial femoral artery, and 9% extended into the proximal popliteal artery. The trial results showed a 94.4% primary patency rate with Eluvia at nine months, and a 3.6% target lesion revascularisation rate at the Continued on page 2 Stefan Müller-Hülsbeck VascularNews.com VN App
 including all patients, and the second contained only those patients with proven rupture")

2 2 Updates June 2015 One-year IMPROVE data suggest benefit of EVAR in ruptured aneurysms Continued from page 1 better than we expected, Balm noted. The pooled inpatient data was subjected to two different analyses; the first was an analysis (as randomised) including all patients, and the second contained only those patients with proven rupture and a restricted cohort from the IMPROVE trial who were anatomically suitable for EVAR. The 30-day survival data showed no significant benefit for endovascular repair. A subgroup analysis of age, sex and Hardman disability index showed that age and New Eluvia drug-eluting stent shows 94.4% primary patency rate at nine months Continued from page 1 same time point. Primary patency was defined as duplex ultrasound PSVR 2.5 and absence of target lesion revascularisation or bypass. I have not seen clinical data this impressive for a vascular stent that has to perform in an environment as challenging as the superficial femoral artery, said Müller-Hülsbeck. Because of forces created by knee flexion, there is an increased risk of restenosis, but we are seeing little evidence of this in the MAJES- TIC trial. The Eluvia device also showed an excellent safety profile, with a major adverse rate of 3.6% at nine months, driven by the two target lesion revascularisations. There were no deaths or amputations. In MAJESTIC, 92.3% of patients treated with the Eluvia stent had no or minimal claudication (Rutherford 0 1) at nine months. The mean ankle brachial index improved from 0.73±0.22 at baseline to 1.01±0.18 at nine months. The Eluvia Stent System is a stent purposebuilt for the superficial femoral artery and uses a polymer and paclitaxel combination designed to facilitate a sustained drug release to reduce restenosis. The system is built on the Innova Stent System platform consisting of a selfexpanding nitinol stent with a paclitaxel-eluting biostable polymer matrix loaded on a lowprofile delivery system. According to Boston Scientific, the stent architecture features a closed-cell design at each end of the stent for more predictable deployment, and an open-cell design along the stent body for improved flexibility, strength and fracture resistance. The Eluvia Stent System is pending CE mark and is not available for use or sale in the USA. The 12-month results will be presented later this year. Boston Scientific at CX 2015 Hardman index had no influence on the main results, but female sex was identified as benefitting from endovascular repair. The time to discharge alive from primary admission was also significantly better for patients undergoing EVAR when compared to those undergoing open repair. We also looked at the influence of neck diameter, neck length and neck angulation. Longer neck lengths resulted in better survival for all patients, Balm said. In the pooled results of all patients, the three-month mortality rate included only those patients who were fit for endovascular repair, which reduces the number of patients in the IMPROVE trial. There seems to be a benefit for endovascular repair but this is statistically not significant, he said. Summarising the survival results of all pooled patients to one year, Balm said, there is an apparent advantage for EVAR, but this was not statistically significant. These findings led Balm to conclude that the early data from the pooled inpatient data meta-analysis did not suggest that there was any survival benefit for EVAR. At one year, the small survival advantage of EVAR is not significant. Yet, although endovascular repair does not offer a significant survival advantage, endovascular repair should be used more widely. Open repair must remain available for those unsuitable for conventional EVAR, Balm maintained. Early results with a new thoracic branched device for the arch are promising Michael Dake, Stanford, USA, presented the initial results with the GORE TAG Thoracic Branch Endoprosthesis (TBE), a new device for treatment of the aortic arch at the Charing Cross Symposium (28 April 1 May, London, UK). Dake told delegates that the GORE TAG TBE is a single branch device that consists of an aortic component, a side branch component and an optional aortic extender. The side branch component is delivered through a sheath and docks into the aortic component portal which allows for perfusion of a single arch branch vessel. The device is currently being studied in a zone 2 (left subclavian) feasibility study and a zone 0/1 (brachiocephalic and left common carotid) early feasibility study in the USA. Currently, there are 20 patients (10 men and 10 women, mean age 75.4 years) successfully enrolled in zone 2 and one patient enrolled in zone 0/1. All 20 patients in zone 2 had successful access and deployment of the TBE device with the side branch component patent at the end of the procedure. Additionally, all side branch components remain patent. At one month, there have been no reported patient deaths or stroke. The left ankle brachial index (1.1) remains the same from pre-procedure to one month. There were no endoleaks that required reintervention. The first two zone 0 patients were treated with the TBE device at the University of Pittsburgh Medical Center by Michel Makaroun, and at the Mayo Clinic by Gustavo Oderich. The protocol requires the patient to be treated in two phases with phase 1 revascularisation and phase 2 endovascular procedure. In phase 1, the patient underwent cervical debranching of the arch via a carotid to carotid bypass followed by a left carotid to left subclavian transposition. The proximal left common carotid and left subclavian artery was suture ligated. Dake spoke about the patient treated about Makaroun and said the patient tolerated the procedure well without any neurological complications. The patient was assessed and deemed stable to proceed to phase 2 after 24 hours. In phase 2, the aortic component was advanced and deployed at the target location near the brachiocephalic artery. The sheath was advanced without difficulty into the portal of the aortic component into the brachiocephalic artery. The side branch component was advanced and deployed. Final arteriography showed excellent flow into the arch vessels, aneurysm exclusion, and complete apposition of the aortic component both proximally and distally. Michael Dake Dake concluded: These early results are promising with 100% technical success and side branch patency along with 0% death or stroke at one month. Valiant Mona LSA Another device designed to enable the treatment of the arch and descending aorta is the Valiant Mona LSA branch thoracic stent graft system. Medtronic has announced the start of a new feasibility study to evaluate the safety and effectiveness of the investigational device. In April, Cleveland Clinic cardiothoracic surgeon Eric Roselli successfully completed the first implant in the study. He serves as the study s national primary investigator. The study aims to enrol 24 subjects at up to seven sites in USA. The purpose of the study is to characterise the safety and effectiveness of the investigational device acutely and at 30 days. Based on the Valiant Captivia thoracic stent graft system, the Valiant Mona LSA system consists of two pieces a main graft for placement in the aneurysmal segment of the aorta, and a branch graft for placement in the left subclavian artery. In their deployed state, the system s two pieces fit together to exclude the aneurysm and maintain patency of the artery. The main graft features a tapered opening, or cuff, which is oriented toward the left subclavian artery. The branch graft fits inside the cuff and terminates in the artery. The Valiant Mona system has previously been studied as part of an early feasibility pilot programme for medical devices initiated by the FDA in It was one of nine devices selected by the FDA for the programme. Results from this previous evaluation were presented at the VEITHsymposium in November 2014.
3
 are female gender, smoking, increasing age and mean arterial pressure, but there are still few useful indicators of how to manage screen-detected aneurysms to stop")
4 4 Abdominal aorta June 2015 Still few useful indicators of how to prevent aneurysm growth and rupture According to Janet Powell, Imperial College, London, UK, the highest risk factors for rupture of abdominal aortic aneurysms (AAA) are female gender, smoking, increasing age and mean arterial pressure, but there are still few useful indicators of how to manage screen-detected aneurysms to stop them enlarging. Powell put forward this view during a session at CX 2015 (28 April 1 May, London, UK) that explored epidemiology, indications and medical management of abdominal aortic aneurysms. In trying to work out what makes aneurysms grow, Powell said that mostly the mundane cardiovascular risk factors have been looked at alcohol, diet, obesity, smoking, medicines taken, exercise taken. Turning to the existing and ongoing randomised trials that provide evidence for growth factors, she pointed out that three trials have already been completed and have not had a positive result AAA:STOP, PHAST and AORTA. Even in 2015, it is quite difficult to find information about trials because some still remain unregistered. Large epidemiological studies have mainly shown us about the risks for developing aneurysms, but the focus has been on baseline risk factors, not aneurysm progression, she said. Powell referred to RESCAN, a large international project with the primary purpose of looking at optimal surveillance intervals for small aortic aneurysms. The project consisted of an individual patient data meta-analysis of small aneurysms, their growth and rupture in more than 15,000 persons. As we all know, growth rate increases with aortic diameter just 1.34mm a year for the smallest aneurysms and 3.63mm when it comes to 5cm aneurysms with exactly the same growth rate between men and women, she pointed out. When it comes to smoking, Powell maintained that the data are remarkably consistent that it increases aneurysm growth rate but that the effect is modest. Similarly, the effect of diabetes to slow or reduce the aneurysm growth rate is very consistent, but small. So we identified out of the available baseline data we had only two factors in these 15,000 patients that influenced growth rate and both effects were relatively modest smoking increases, diabetes decreases. Cholesterol, blood pressure, statins, anti-hypertensive drugs and aspirin had no effect, and the year of enrolment [ ] had absolutely no effect either. Disappointing, Powell stated. Rupture rates Even though rupture of small aneurysms is not common, the findings from the study were more revealing, Powell said. RESCAN showed that the smallest of aneurysms take eight or more years before the risk of rupture is anything substantive, but as the diameter increases, so does the risk of rupture. But even for a 5cm aneurysm, it is more than year before risk of rupture exceeds 1%. Powell pointed to some strong associations with factors that increase rupture rates. Most notable, the fact that in women, there is fourfold increase in rupture rates vs. men. With smokers there is a twofold increase, with a far bigger effect on rupture than on growth. Mean arterial pressure increases rupture rate, as does age. The older you are, the more likely your aneurysm is to rupture for any given diameter. So we cannot have any of this ageism, we need to treat aneurysms in older people too, Powell maintained. In the EVAR 2 trial, and subsequently reproduced in other papers, Powell noted that aortic neck length was associated with rupture. She added that the shape of the aneurysm might have mattered, and a long neck was associated with relative protection from aneurysm rupture. Where are we in 2015? For rupture, there are some strong factors increasing risk: female gender, smoking (which we can do something about), increasing age, higher mean arterial pressures (we could have more effective blood pressure control), and the fact that a long aneurysm neck could just be protective. However, for growth, the effects that we have identified are modest: smoking, which increases it, and diabetes, which is protective, Powell said. She re-stressed that both of those growth effects are modest, adding that, unfortunately this leaves us in a position that as yet we have few useful indicators of how to manage screen-detected aneurysms to stop them enlarging other than the old classic that was used for intermittent claudication stop smoking and possibly keep walking. Aneurysm sealing evidence continues to build The 12-month outcomes of patients treated with the Nellix system are encouraging for the development of endovascular sealing (EVAS) as the next gold standard treatment, according to Matt Thompson (London, UK), with a low overall endoleak rate and an acceptable reintervention rate. Thompson told the Charing Cross Symposium (28 April 1 May, London, UK) audience that EVAS may address some of the issues that we have with long-term durability follow-up with conventional endografts; however, that is all dependent on the long-term results. The 12-month results of the EVAS FORWARD Global Registry include data from 300 patients (split into four cohorts) treated at 30 centres, who will be followed-up to five years. The registry was started after about 200 commercial implantations of Nellix, so this is really quite early on in the experience, said Thompson. Following a device iteration in 2016, further patients will be enrolled in the registry. In addition, an investigational device exemption (IDE) study in the USA has now finished enrolment of 180 patients and there will be continued access to the device in the centres involved. This all means that there will be somewhere in the region of 1,000 patients who are prospectively monitored in a risk-adjudicated registry that will provide evidence for this procedure. The registry is based on real-world experience, and there was no prospective screening of patients, meaning that it has enrolled quite a number of challenging patients. The registry employs independent adverse events adjudication with primary outcomes typical of endovascular aneurysm repair (EVAR) therapy. The patients were divided into four cohorts. Cohort 1 were patients treated within the instructions for use, with neck length 10mm and infrarenal angle 60 degrees (n=192, 65%). Cohort 2 had neck length 5 10mm and infrarenal angle degrees (n=39, 13%). Cohort 3 included patients with juxtarenal aneurysms neck length 90 degrees (n=37, 13%), and cohort 4 included patients with ruptured aneurysms and EVAR revisions (n=25, 9%). Thompson pointed out that the EVAS FORWARD registry is different from other registries (such as the ENGAGE and Matt Thompson GREAT registries) as it includes a larger proportion of complex abdominal aortic aneurysms. There were nine (3.4%) patients who had one or more major adverse events at 30 days, including three all-cause deaths (1.1%), all of which were perioperative and related to hospital-acquired pneumonia, aspiration pneumonia or gastrointestinal haemorrhage. There were also nine (2.7%) patients who reported one or more major adverse events at 30 days including seven (2.7%) cases of allcause death none of these deaths were aneurysm-related. Thompson reported eight (3%) incident endoleaks at 30 days. Six of these were type Ia and six were type Ib with one type II which then resolved. The message to take out of this is that there is a learning curve to this procedure, Thompson told the audience, and we think probably three out of six type Ia were related to low implantation of the device or under filling of the bags. Four of the type Ia were successfully treated with coil embolisation and the use of Onyx, and two patients remained untreated with a type Ia endoleak. After one month and out to the end of follow-up, four more type 1 endoleaks have been reported, all of which have had a successful secondary intervention. Thompson showed the audience a comparison between Nellix and the IDE studies of several other devices, showing a comparatively low number of persisting endoleaks at 12 months for Nellix, with a rate of just 0.7%, all of which were type Ia or Ib. The rate of persisting endoleaks in the other six devices varied from %. The potential absence of type II endoleaks was, according to Thompson, one of the attractions of Nellix for many of us, and one that has been realised. Three ruptures were reported in the follow-up period. The two remaining patients with untreated type I endoleaks were treated with open conversion or iliac extensions. The third rupture was due to a retroperitoneal haematoma and was treated with an open conversion. Freedom from all-cause mortality at 30 days was 98.9% (AAA-related, 98.9%) and 96% (AAA-related, 98.9%) at one year. This mortality rate of just 4% is probably half of what you would expect seeing as it is a challenging group. With regard to all-cause mortality, Thompson recommended that the audience watch this space.
5

6 6 Thoracic aorta June 2015 Despite endovascular revolution, 65% say heyday of open repair in aortic arch continues There have been vast technological advances that have enabled the final frontier of the aorta, the diseased ascending aorta and arch, to be treated by completely endovascular means. Simultaneously, there have also been advances in open repair. Also, with perioperative stroke remaining a risk with thoracic endovascular aortic repair (TEVAR), the high incidence of cerebral embolisation with the procedure is a problem that needs wider recognition, delegates heard at the Charing Cross Symposium (28 April 1 May, London, UK). In a panel discussion during the session on interventions for ascending aorta and aortic arch, Roger Greenhalgh, chairman of the CX Organising Board, pressed the panel to comment on patient mortality after open repair and endovascular repair. For a 70-year-old patient, the in-hospital mortality rate for open arch repair is around 5% and major postoperative morbidity is up to 19%, even when there is involvement of the aortic valve, said Stephen Large, Cambridge, UK. With endovascular repair, it approaches 10% including emergencies and high risk patients often being refused for open surgery, said Dittmar Böckler, Heidelberg, Germany. Subsequently, 65% of the CX 2015 audience voted against the motion that the heyday of open aortic surgery is over. Silent cerebral infarction Richard Gibbs, London, UK, told delegates that there was a high rate of embolisation during arch and descending thoracic intervention that could be observed as silent cerebral infarction on new imaging techniques. The results from the study he presented showed that there is a 70% silent cerebral infarction on MRI and that there is postoperative neurocognitive decline in patients with silent cerebral infarctions. Gibbs made the point that stroke, which was caused by cerebral embolisation, was a relatively crude surrogate, but a clinically relevant measure of microembolisation. The stroke rate for TEVAR ranges between 3% and 6%, said Gibbs, with embolisation being caused by the passage of stiff wires, soft wires, devices and manipulation within the diseased aorta. The risk factors are the atheromatous burden within the aorta and using a proximal landing zone. Hypotension is also very important, he said. A much subtler way of looking at microembolisation is with diffusion-weighted magnetic resonance (MR) that detects acute ischaemia that is due to cerebral oedema. These lesions appear within 24 hours of the insult and last up to 14 days, and show as hyperintense bright areas that are easy to recognise, Gibbs noted. Gibbs then showed diffusion-weighted cerebral MR images from a patient who had silent cerebral infarctions but did not develop signs or symptoms of clinical stroke following TEVAR. Therefore what we see here is silent stroke, or silent cerebral infarction, which is imaging evidence of cerebral infarction, without a history of acute neurological dysfunction attributable to the lesion, Gibbs said. He qualified that he believed the term silent cerebral infarction is a misnomer because there is an increasing body of evidence that suggests that silent cerebral infarction is associated with depression, dementia, Alzheimer s, future increased risk of stroke and mortality. Published literature shows a significant rate of cerebral infarction with various different interventions involving the arch and unsurprisingly transcatheter aortic valve implantation (TAVI), which is the biggest device and causes the most cerebral infarction, he explained. When it comes to TEVAR, there is not much information available in the literature, and one paper suggests that there is a 63% risk of cerebral infarction with the procedure, said Gibbs referring to the data from 19 patients from Kahlert et al published in the Annals of Thoracic Surgery in 2014 that found diffusion-weighted MR evidence of cerebral infarction after TEVAR in 12 of 19 (63%) undergoing the procedure for a variety of indications. There was no overt clinical stroke seen in these patients. Gibbs then presented the pilot work done by his team on the rates of silent cerebral infarctions during TEVAR, the presence of silent cerebral infarction on MR and whether there are neurocognitive changes afterwords. We included 44 patients undergoing TEVAR and looked at the burden of atheroma within the arch of the descending aorta based on the American Heart Association grading method. The patients had bidirectional transcranial Doppler, which is a direct measure of cerebral microembolisation. A subset of these patients had pre-and postoperative MR looking for more evidence of infarction (23 patients). Another subset had neurocognitive assessment before the intervention, after the intervention in hospital and eight weeks later to see if any changes persist, said Gibbs. Forty-one TEVAR procedures involving the arch and descending aorta were performed for a variety of pathologies. Of these 21 were standard and 20 were complex involving the use of branches, scallops or adjunctive surgical procedures. We had fairly proximal landing zones, he noted. Looking at the specific procedural steps, we see clearly that stent graft deployment carries the most significant rate of embolisation, said Gibbs. He then showed a transcranial Doppler during stent graft deployment where a burst of cerebral embolisation was visible in both hemispheres. The highest activity of cerebral embolisation was when the device was deployed. Increased embolisation was associated with the left hemisphere more than the right; stent manipulation more than wire and catheter passage; a higher grade of atheroma compared to a lower grade (so a higher burden of disease); chronic rather than acute disease. Patients who had a stroke had the highest rate of embolisation. A proximal landing zone rather than distal one had a higher rate of cerebral embolisation. In the group where we looked for evidence of silent cerebral infarction, 70% (16/23) of our patients had this, mostly in the left hemisphere and mostly in the territory served by the middle cerebral artery. Ten per cent of these patients had a clinical stroke, said Gibbs. When the researchers selected the data for older patients from the group, they found that executive function diminished and stayed down at eight weeks, memory diminished and manual dexterity got worse. There is a significantly high rate of cerebral embolisation during TEVAR and the more proximal you go, the worse it is. There is a definitive and radiologically proven damage to the brain and these patients do pay a price for this. We have to be thinking about how we can intervene [either pharmacologically or by using devices], concluded Gibbs. Reconstruction of the ascending aorta Rodney White, Torrance, USA, spoke about ascending aortic reconstruction and the progress that has been made evaluating Richard Gibbs endografts for ascending aortic pathologies. He told delegates about a study that is being conducted as an FDA-approved investigational device exemption (IDE) study. The co-principal investigators for the study (White and Ali Khoynezhad) have successfully completed a five-patient feasibility study, and are now continuing to enrol patients in an expanded study at Harbor-UCLA Medical Center and at Cedars Sinai Medical Center in the Los Angeles area. There are anecdotal reports of successful ascending aortic endograft repairs, but no study specifically designed to address many unique characteristics of the ascending aorta including diameters larger than the descending aorta, increased aortic wall motility, and requirements for precise deployment similar to TAVI procedural and imaging requirements, he said. The IDE study was initially designed to evaluate non-aneurysmal tubular ascending aortic lesions including intramural haematomas, pseudoaneurysms, and type A dissections. Specifically designed Valiant Captivia endografts (Medtronic) are available for this study. During the first 18 months of the study, White said, we have learned several key considerations for accomplishing successful ascending aortic endograft deployments. All procedures were performed in a state-ofthe-art hybrid interventional room, with the same team that routinely performs transcatheter aortic valve implantation procedures to ensure maximal patient protection and multispecialty collaboration. According to White, preliminary results of this study have demonstrated that the Valiant Captivia endografts can be deployed accurately and are stable without migration or other deformity to beyond one year. Positive remodelling of the excluded segments assimilates performance of devices in the descending aorta. Experienced hybrid room staff and multidisciplinary team are Continued on page 8
7


8 8 Thoracic aorta June 2015 Despite endovascular revolution, 65% say heyday of open repair in aortic arch continues Continued from page 6 required, with transapical delivery of devices being evaluated similarly to the evolution of transapical delivery of transcatheter aortic valve implantation devices, he said. Scarcity of literature on proximal landing zone and TEVAR outcomes Dittmar Böckler stated that while the relationship between the proximal landing zone and outcome was well-documented in the EVAR literature, there were very few publications focused on how the proximal landing zone influences patient outcomes with TEVAR in the arch, and noted the low level of evidence. There are no randomised controlled trial data on open versus endovascular approaches and there are no metaanalyses. The data come from limited European registry data from the Relay registry, Traviata registry and European CTAG registry, he noted. Böckler drew attention to the fact that there was no consensus in the literature and guidelines on the appropriate proximal neck length and that this variation was reflected in the instructions for use from manufacturers, as the target landing zone is depending on stent graft diameter. The appropriate proximal landing zone for TEVAR is not defined. Arch type and atheroma seem to influence stroke risk during TEVAR in the arch. There is a strong need for new refined conformable devices in the arch including branched stent graft technology, Böckler said. Value of medication Frank Lederle, Minneapolis, USA, speaking on the value of medication such as statins before aortic arch catheterisation, stated that there was very little trustworthy randomised controlled trial data to go by. He reviewed evidence that bears on whether perioperative statins or aspirin benefit patients having a thoracic aortic procedure. Analyses showing the benefit of perioperative use rely on weak and doubtful studies. When it comes to aspirin, there are no data on perioperative benefit, but there is increased major and minor bleeding, he said. Lederle drew attention to the fact that many patients with aortic aneurysm have arteriosclerotic cardiovascular disease and should be on statins and aspirin long-term. There is no good evidence that statins or aspirin improve longterm outcomes for patients with aortic arch patients without arteriosclerotic cardiovascular disease, so some of these patients will not be on these medications. Questions remain on whether patients are on them long-term and whether they should be used perioperatively, he said. Open surgery Stephen Large, Cambridge, UK, a cardiac surgeon, outlined the case for open surgery in interventions for ascending and arch of the aorta, the current gold standard approach. Large noted that not operating resulted in a dreadful attrition. We know that there is an increase in attrition correlated with the increase in aneurysm size, the hinge point being around 5.5cm in the ascending and arch, which is associated with an acceleration in terms of stroke, dissection rupture and death, he said. What we very often do in the ascending aorta is deal with an associated post-aortic valvular lesion either by an interposition graft, that is something placed above the coronary artery ostia, really at the level of the sinotubular junction, and right up to the origin of the innominate artery a true ascending aortic replacement. We can, if we are in trouble (of course with involvement of pathology within the aortic root), replace the aortic root and that always requires reimplantation of the coronary ostia, which brings a raft of problems of threatening ischaemia with it. Up until relatively recently, this involved automatic replacement of the aortic valve. There is now a keen interest in considering valve preservation procedures, something that I have fought against for many years, because the aortic valve is embryologically of the same origin as the ascending aorta. Piergiorgio Cao However, counterintuitively, it appears that the aortic valve fares very well. So what to do with the arch? We can replace it with a tube graft and address each of the usual three arch vessels. Or we can translocate the whole of the aortic arch vessels permitting the use of either replacement or stenting. As cardiac surgeons, we find ourselves replacing the ascending aorta in an emergency as a life-saving procedure for dissection. We, of course, will look at ascending aortic aneurysms for elective surgery for prognostic issues and this is often in conjunction with other procedures in the chest such as aortic valve replacement, he said. Endovascular procedures a valid alternative in selected patients Piergiorgio Cao, Rome, Italy, speaking on branched stent grafts for the treatment of complex arch lesions, said that any repair of aortic arch remains demanding and exposes patients to mortality and stroke risks that are not negligible. Open repair is the gold standard, and hybrid and endovascular repair are valid alternatives, mostly in patients who are at high risk for surgery, he noted. Cao defined the morphological feasibility to receive endovascular treatment as the presence of a proximal landing in the ascending aorta (zone 0) not less than 3cm in length and 4cm in diameter. The challenges for TEVAR in the arch include conformability of the stent graft, endoleak and retrograde dissection occurrence, he said. He then alluded to a recent publication in the Journal of Vascular Surgery from Paola De Rango et al that analysed total aortic arch reconstruction in a contemporary comparison of current open and endovascular repair. De Rango et al entered endovascular and open arch procedures performed from 2007 to 2013 into a prospective database and then retrospectively analysed the data. Endovascular repair (proximal landing zones 0 1), with or without a hybrid adjunct, was selected for patients who were sicker but who had a fit anatomy. Operations involving coverage of left subclavian artery only (zone 2 proximal landing) and open hemiarch replacement were excluded. As reported in the journal, the authors concluded that despite the older age and a higher comorbidity profile in patients with challenging aortic arch disease who were suitable and selected for endovascular arch repair, no significant differences were detected in perioperative and four-year outcomes compared with the younger patients undergoing open arch total repair. Cao concluded by saying: The endovascular approach is a valid alternative to open surgery for all patients, when morphologically feasible. A safer proximal landing zone with longer coverage of the ascending aorta may be the key for long-term durability and to prevent retrograde dissection. Branched stent grafts might be useful in avoiding arch manipulations and decreasing the risk of major adverse events, he said. Greenhalgh then commented that the audience might like to have some idea of the expected mortality associated with both the open and endovascular methods in the case of a 70-year-old patient with an ascending dilating disease process in which the valve becomes incompetent. Mortality is 3% with open repair and 10% with endovascular repair, the audience learned. He further commented on the resurgence of the classification of aneurysmal disease: The starting point seems to be aneurysmal disease. We are seeing comments on syphilitic, fusiform and saccular aneurysms and this is beginning to look like an old surgical textbook, he commented. In a debate, Hans-Henning Eckstein, Munich, Germany, argued against the motion The heyday of open aortic surgery is over to garner majority support that open repair still had a valid place in the treatment of the ascending aorta and aortic arch. He persuaded 65% of the delegates to vote against the motion. Frank Veith, New York, USA, spoke for the motion.

9
10

 secondary interventions and more adjuncts associated with")
11 June 2015 Abdominal aorta Going off-label to use EVAR in necks less than 10mm in length can be sensible, says CX audience 11 The Charing Cross Symposium (28 May 1 April, London, UK) audience voted 70% against the motion that EVAR is not sensible for any abdominal aortic aneurysm with a neck length less than 10mm. Stephen Cheng (Hong Kong) spoke for the motion, while Jan Blankensteijn (Amsterdam, The Netherlands) sounded-off against the motion. Making his case, Cheng said that even with new devices, there are more early complications, more late complications, more (difficult) secondary interventions and more adjuncts associated with short-neck endovascular aneurysm repair. On the other hand, his opponent maintained that in selected cases of infrarenal neck length <10mm, Any of the current infra/transrenal devices can be used with or without endoanchors for enhancement, adding that even if it comes with a moderately increased risk of type Ia endoleak, it balances against downsides of FEVAR, CHIMPS, or against open repair (if FEVAR is not an option). Discussing the outcome of the debate and the audience s strong position against the motion, Blankensteijn said, I think people understand that things are not absolute and clearly we know that by staying within instructions for use you get better results. The instructions for use are guidelines that the graft manufacturer has set forth to ensure safe application of the device. We as surgeons need to decide what we can and cannot do with these products. Treating outside the instructions for use with an infrarenal device can be defended if the use of a fenestrated stent graft does not make sense or if it is considered too risky. Then I would suppose that an infrarenal device (for instance Gore Excluder) preserves all the options juxtarenally, so if this fails, you still have the option to use a fenestrated cuff or go higher up. The debate took place during a session on procedures for challenging infrarenal abdominal aortic necks. The answer lies in the neck While presenting the morphology findings from the IMPROVE trial, Robert Hinchliffe, London, UK, drew attention to the independent association between neck length and mortality. Only aortic neck length is significantly associated (inversely) with 30-day mortality both for open repair Treating outside the instructions for use with an infrarenal device can be defended if the use of a fenestrated stent graft does not make sense or if it is considered too risky. Jan Blankensteijn Stephen Cheng (p<0.001) and overall (p=0.007). The shorter the neck, the higher the mortality after open repair (and EVAR). With long necks, the 30-day mortality from EVAR and open repair is similar (and this is consistent with the results of the AJAX and ECAR trials), he said. Hinchliffe added that a short aneurysm neck was the commonest reason for a patient being unsuitable for conventional EVAR of ruptured abdominal aortic aneurysms. The results also explain in part why observational studies, which cherry pick longnecked aneurysms for EVAR leaving all the short necked aneurysms for open repair, always show that mortality is lower after EVAR. The morphology findings could also explain the worse outcomes in women as short aneurysm necks are especially common in women. In the future, new, widely available endovascular strategies for treating short necked ruptured aneurysms are needed and the results following rupture should report juxta-renal and infra-renal aneurysms separately, Hinchliffe said. Aneurysm morphology indicates whether a patient with ruptured abdominal aortic aneurysm is eligible for EVAR and may influence the outcome of both EVAR and open surgical repair, he concluded. Stick to the instructions for use Timothy Resch, Malmö, Sweden, enforced the point that the outcome of EVAR is excellent if we stick to the instructions for use and hostile sealing zone anatomy affects the outcome of EVAR negatively both in the short and long term regardless of the device that you use. Resch explained that 10 20% of EVAR patients have necks <15mm, and these short infrarenal necks are predictive of initial technical failure, with increased incidence of early and late type I endoleak and increased use of intraoperative adjunctive procedures, where the long-term outcome is impaired and endoleaks, migration and late rupture are common. Referring to a contemporary meta-analysis of 12,000 patients treated with modern devices, 3,039 patients with hostile necks saw an increase in 30-day mortality, intraoperative adjuncts, 30-day migration and an increase in type I endoleak at 30 days and one year. Further, in the ANCHOR registry, Resch noted, a regression and ROC analysis was used to try to find predictive factors for type Ia endoleak which showed that the diameter of the neck correlates with poor outcome, as does the anatomic neck length. This actually provides some solid data for calculating the risk in the individual patient, he said. So one option of course in these short juxta/ pararenal aneurysms is to seal higher above and use the fenestrated and incorporate the visceral arteries in your repair. Does that solve the problem of the proximal endoleaks? Again, it depends on how you use the graft, Resch suggested. Making a case from some of his own data and that of a study at the Cleveland Clinic, USA, he said, We found no cases with proximal type I endoleaks during long-term follow-up of these patients. So maybe this is the solution for everything using it in the right context. In a larger series from the Cleveland Clinic analysing over 900 patients with fenestrated grafts, indeed there was a 2.8% incidence of late type Ia endoleak occurring in a steady fashion over time and almost half after a year post-operatively. Looking at the risk factor in that series, what they identified again was a poor sealing zone, just as you would in an infrarenal neck and more that 10% was diameter change and they also found that the sealing zone was much more unstable in the juxtarenal vs. more proximal aorta. So from the clinical perspective, we have learned from that and we now place more fenestrations on the graft to reach a healthy sealing zone, which in our series, combined with the series from Lille with 300 patients, resulted in a higher placement of the endograft than we initially did without affecting the operative mortality or the one-year outcome, he reported.
12
 Peripheral Arterial Controversies session.")

13 June 2015 Bioresorbable scaffolds are the only complete solution for the superficial femoral artery The use of bioresorbable scaffolds is the only complete solution for the superficial femoral artery, argued Andrew Holden, Auckland, New Zealand, in a Charing Cross Symposium (28 April 1 May, London, UK) Peripheral Arterial Controversies session. Peripheral intervention 13 Presenting an update on the Stanza programme, Holden told delegates that the ideal treatment strategy for superficial femoral artery disease has been the source of much research, discussion and controversy. An endovascular device should provide vessel support acutely to manage dissection and recoil, include an anti-restenosis strategy and preferably leave nothing behind when no longer needed. A bioresorbable drug-eluting scaffold potentially fulfils these requirements, he explained. The programme employed the Stanza platform (480 Biomedical) a flexible, self-expanding stent design with full resorption in about 12 months. Holden summarised the development of the Stanza scaffold, the first part of which the STANCE first-in-man trial allowed assessment of stent parameters such as precise positioning and deployment, excellent radial resistive force with minimal residual stenosis and satisfactory resorption. Two sub-studies in the STANCE trial allowed original validation of important imaging modalities by independent core laboratories. One sub-study analysed the accuracy of quantitative vessel analysis of magnetic resonance angiography (MRA) compared to the gold standard catheter angiography. A second sub-study compared cross sectional luminal area evaluation using MRA and optical coherence tomography (OCT). This comprehensive analysis, Holden explained, confirms MRA is an effective method to assess the vessel lumen non-invasively after treatment with a bioresorbable scaffold. The study showed 100% scaffold delivery success, good scaffold apposition verified by OCT and angiography, and acute performance similar to metal stents. Holden noted that OCT is a vital tool in the assessment of bioresorbable scaffolds, as it allows investigators to identify scaffold encapsulation during healing and resorption. Using OCT Holden was also able to create 3D reconstructions of the vessel, allowing him to detect any scaffold fractures and show that at six months the scaffold demonstrated chronic strength to prevent vessel recoil. The drug-eluting version of the Stanza platform is currently being assessed in the SPRINT clinical trial. Holden told attendees that the biggest challenge has been to define appropriate and extended drug release Andrew Holden kinetics to deal with the inflammation associated with scaffold resorption. This has been achieved with the drug eluting version of Stanza. Currently, there is ongoing recruitment and evaluation in this trial, as well as several examples with medium-term follow-up. In one such case study, pre-implant the patient had 88% stenosis, which fell to just 2% residual stenosis following the implant. Similarly, in the second case that Holden presented, the pre-implant stenosis figure was 92%, falling to 0% following the implantation of Stanza. Both of these case studies were evaluated with MRA and OCT to confirm the outcomes. Following DEFINITIVE AR results, CX audience shows support for atherectomy before drug-coated balloon use Twelve-month results from the randomised, multicentre DEFINITIVE AR pilot study suggest that there is a benefit to adding directional atherectomy in long and calcified lesions prior to using a drug-coated balloon in comparison to the use of a drug-coated balloon alone. After the presentation of the results at the Charing Cross Symposium, 77% of the audience voted in favour of pretreatment of superficial femoral artery lesions before drug-coated balloon use. This is the first time the CX audience has shown support for atherectomy. Data from the trial were presented by Thomas Zeller, Bad Krozingen, Germany, who is a study principal investigator alongside Gunnar Tepe, Rosenheim, Germany. DEFINITIVE AR was designed to assess the effect of treating a lesion with directional atherectomy (Medtronic/Covidien s SilverHawk or TurboHawk plaque excision systems) followed by a paclitaxel-coated balloon (Bayer HealthCare s peripheral paclitaxel-coated angioplasty catheter with Paccocath Technology), collectively referred to as DAART (directional atherectomy + anti-restenotic therapy), in order to generate early hypotheses for further research in this therapy area. Claudicants (Rutherford category 2 4) with 7 15cm superficial femoral and/or popliteal lesions were randomised 1:1 to either DAART (n=48) or to the paclitaxel-coated balloon alone (n=54). Patients with severely calcified lesions were as signed to a non-randomised registry arm and were treated with DAART (n=19). Baseline patient and lesion characteristics did not differ between the DAART and drugcoated balloon arms. Technical success, defined as 30% residual stenosis following the protocol-defined treatment at the target lesion, was significantly higher in the DAART arm vs. the drugcoated balloon arm (89.6% vs. 64.2%, p=0.004). According to Zeller, there were significantly fewer flow-limiting dissections reported in patients treated with DAART vs. drug-coated balloon alone (2% vs 19%, p=0.01). Technical success in the DAART registry group was 84.2% and incidence of flowlimiting dissections was 0%. At 12 months, stenosis in the randomised groups was 33.6±17.7% for the DAART arm vs. 36.4±17.6% for the drug-coated balloon arm. Duplex ultrasound patency (PSVR 2.4, without target lesion revascularisation) was 93.4% for the DAART arm and 89.6% for the drug-coated balloon arm. Angiographic patency ( 50% stenosis and without target lesion revascularisation) was 82.4% in the DAART arm and 71.8% in the drug-coated balloon arm. In the DAART cohort lesions with a residual stenosis <30% post atherectomy did show a trend towards better angiographic patency at one year (94.1% vs. 68.8%). This rigorously performed pilot study suggests an added benefit for DAART over drugcoated balloons alone in long Thomas Zeller and calcified lesions. Further investigation in larger, prospective, statistically-powered randomised trials is warranted. Patients will be followed out to 24 months to assess durability of the results, Zeller said. For the first time, CX voters Continued on page 14

14 14 Updates June 2015 Cardinal Health binding offer to acquire Cordis is accepted Cardinal Health has announced that its 1 March 2015 binding offer to acquire Johnson & Johnson s Cordis business for US$1.944 billion in cash was formally accepted. The offer was accepted after consultations with relevant works councils and trade unions. The transaction is expected to close in the United States and key non-us countries towards the end of 2015, subject to regulatory clearances and other customary closing conditions. Headquartered in Fremont, California, USA, Cordis had annual sales in calendar year 2014 of approximately US$780 million, split almost evenly between cardiology and endovascular products. While the USA is the largest single market, 70% of total sales come from outside the US. Cordis international presence includes operations in more than 50 countries, including China, Japan, Germany, Italy, France, the United Kingdom, and Brazil. Cardinal Health noted in its March announcement that the acquisition of Cordis was a significant step forward in its cardiovascular strategy. The Cordis acquisition follows a sequence of strategic moves for Cardinal Health in the areas of cardiology, wound management and orthopaedics. The company is helping customers standardise around mature medical devices, while bringing them innovative solutions in supply chain management, inventory optimisation, and work flow tools and data to support the most effective management of the patient. Spectranetics accelerates investment in Stellarex drug-coated balloon for below-theknee disease Spectranetics is accelerating investments in the Stellarex drug-coated balloon angioplasty platform for treatment of below-the-knee disease. The company estimates this will represent a US$150 million market opportunity by Spectranetics estimates that treatment of below-the-knee disease will become a meaningful segment of the global market for drug-coated balloons, representing a potential market opportunity of US$150 million. The company anticipates the global market for drug-coated balloons to reach between US$700 million and US$1 billion over the next seven years. Spectranetics is targeting CE mark approval for the Stellarex platform in the second half of Wound healing is always a concern in the treatment of BTK disease. Robust patency and coating stability with minimal flaking is critical in those situations, said William Gray, Columbia University Medical Center, New York, USA. The Stellarex drug-coated balloon was designed to optimise drug delivery to the treatment site while minimising downstream drug loss through the unique coating formula and manufacturing process. The unique coating coupled with the strong clinical data on the Stellarex drug-coated balloon platform set the stage for an ideal application in treatment of belowthe-knee disease. The acceleration of the investment in the programme is expected to represent an incremental US$5 6 million of product development, regulatory and clinical expense in The company expects to commence enrolment in an investigational device exemption (IDE) clinical trial in the USA in mid The commencement of the IDE trial is conditioned upon receipt of regulatory approval from the FDA. Following DEFINITIVE AR results, CX audience shows support for atherectomy before drug-coated balloon use Continued from page 13 also showed their support for atherectomy, but as a pre-treatment to the use of drug-coated balloons as described in the DEFINITIVE AR trial or as a pre-treatment to the use of stents. Zeller explained that Drug-coated balloons add benefit to the endovascular approach to treat femoropopliteal disease but that there are still limitations such as recoil, calcium and dissections. Previous research has shown that circumferential calcification is a negative predictor for successful outcome with drug-coated balloon angioplasty. Directional atherectomy is one of the most interesting pretreatment plaque modulating or plaque removing options available, after cutting or scoring balloons have been shown not to be very effective at this. The removal of ex-centric plaque and calcified plaque serves to reduce the problem of early recoil that limits the use of drug-coated balloon angioplasty outcome, he said. Zeller also noted that the large majority vote favouring the use of atherectomy as a pretreatment was akin to a mandate to the industry to support large-scale randomised controlled trial to prove this concept. In previous years, atherectomy had failed to elicit CX voter backing as a treatment option in the superficial femoral artery. In 2014, 57% of the audience voted no to the motion I would use atherectomy for some superficial femoral artery lesions. In 2013, 68% voted against atherectomy is the answer for the superficial femoral artery technology. This year s vote shows that there is increasing support for atherectomy as a pre-treatment option rather than a definitive treatment and that the technique is clearly currently in favour of being used prior to drug-coated balloon or stents in order to reduce the risk of thrombosis. A member of the audience asked whether atherectomy should be the first option for isolated popliteal lesions considering there was a desire to leave nothing behind. Zeller, responding, said that it was frequently observed that isolated popliteal lesions were focal calcified lesions and for that indication, he considered atherectomy an excellent first option followed by angioplasty or stenting. However, if we are talking about evidence to support this, there is none, he clarified. In the treatment of in-stent restenosis, removal of plaque is probably key Jos van den Berg, Lugano, Switzerland, presented the long term follow-up of a combination therapy using excimer laser photoablation and drug-coated balloons for in-stent restenosis at the Charing Cross Symposium (28 April 1 May, London, UK). A prospective cohort of 14 patients with clinically relevant (Rutherford 3 6) in-stent restenosis that were treated with excimer laser photoablation (Spectranetics) and drug-coated balloons and a follow-up of at least 12 months was evaluated. Mean age was 78±6.5 years (range 67 88). The mean lesion length treated was 133.2±107.2mm (range mm). The mean time to occurrence of restenosis after initial treatment was 8.6±4.7 months (range 2 18 months). Technical success was 100%. In two cases distal embolisation occurred, and it was treated successfully by endovascular means. No other periprocedural major adverse events occurred. All patients were available for clinical follow-up and 12 patients were available for duplex follow-up. At a mean follow-up of 27.9±13.2 months (range months) one target lesion revascularisation was seen (at three years after the in-stent restenosis treatment). In the patients with critical limb ischaemia (n=7) no major amputations were needed. Twelve patients had duplex control (mean follow-up 28±12.5 months; range months). Binary restenosis (>50%) was seen in one case (at 36 months; same patient as target lesion revascularisation). A 25 50% stenosis was seen in four patients (mean follow-up 35.2 months; range 31 41). In seven patients no signs of neointimal hyperplasia were demonstrated (mean follow-up 21 months; range 10 42). Van den Berg concluded that in the treatment of instent restenosis, removal of plaque is probably key. There is a growing body of evidence that by adding drug-coated balloon angioplasty to photoablation, results that compare favourably to those of standard angioplasty, cutting-balloon angioplasty or debulking alone can be achieved. Randomised trials are needed to define the role this combine therapy in the treatment of in-stent restenosis further, he said. EXCITE ISR Another experience assessing the use of laser atherectomy in in-stent restenosis had its results presented by Craig Walker at New Cardiovascular Jos van den Berg Horizons (NCVH; May, New Orleans, USA). Twelve-month data from the EXCITE ISR trial show that laser atherectomy with balloon angioplasty is more effective than angioplasty alone for femoropopliteal in-stent restenosis, demonstrating continued durability at 12 months. The data showed that treatment using Turbo- Tandem (Spectranetics) resulted in significantly less residual stenosis and need for bailout stenting, and 92.9% procedural success rate vs. 81.7% with angioplasty alone (p<0.01). The primary safety endpoint, major adverse events rates at 30 days, was 5.4% vs. 20.8% with angioplasty alone (p<0.001), and the primary efficacy endpoint, freedom from target lesion revascularisation through six months, was 78.3% vs. 58.9% with angioplasty alone (p=0.002). Excimer laser atherectomy with adjunctive angioplasty was associated with a 43% reduction in target lesion revascularisation through 12 months (p=0.005). EXCITE ISR (Excimer laser randomized controlled study for treatment of femoropopliteal in-stent restenosis) is a multicentre, prospective randomised trial. In July 2014, Spectranetics received FDA 510(k) indication for Turbo-Tandem and Turbo-Elite to treat in-stent restenosis. The trial was designed to enrol a maximum of 318 subjects at up to 40 sites, randomised 2:1 treatment to control with predetermined statistical analyses at 200, 250 and 300 enrolled patients. In 2014, Spectranetics announced success of the trial based on achieving highly significant statistical superiority in both safety and efficacy among 252 patients.
15
 was 80.3% at 24 months.")

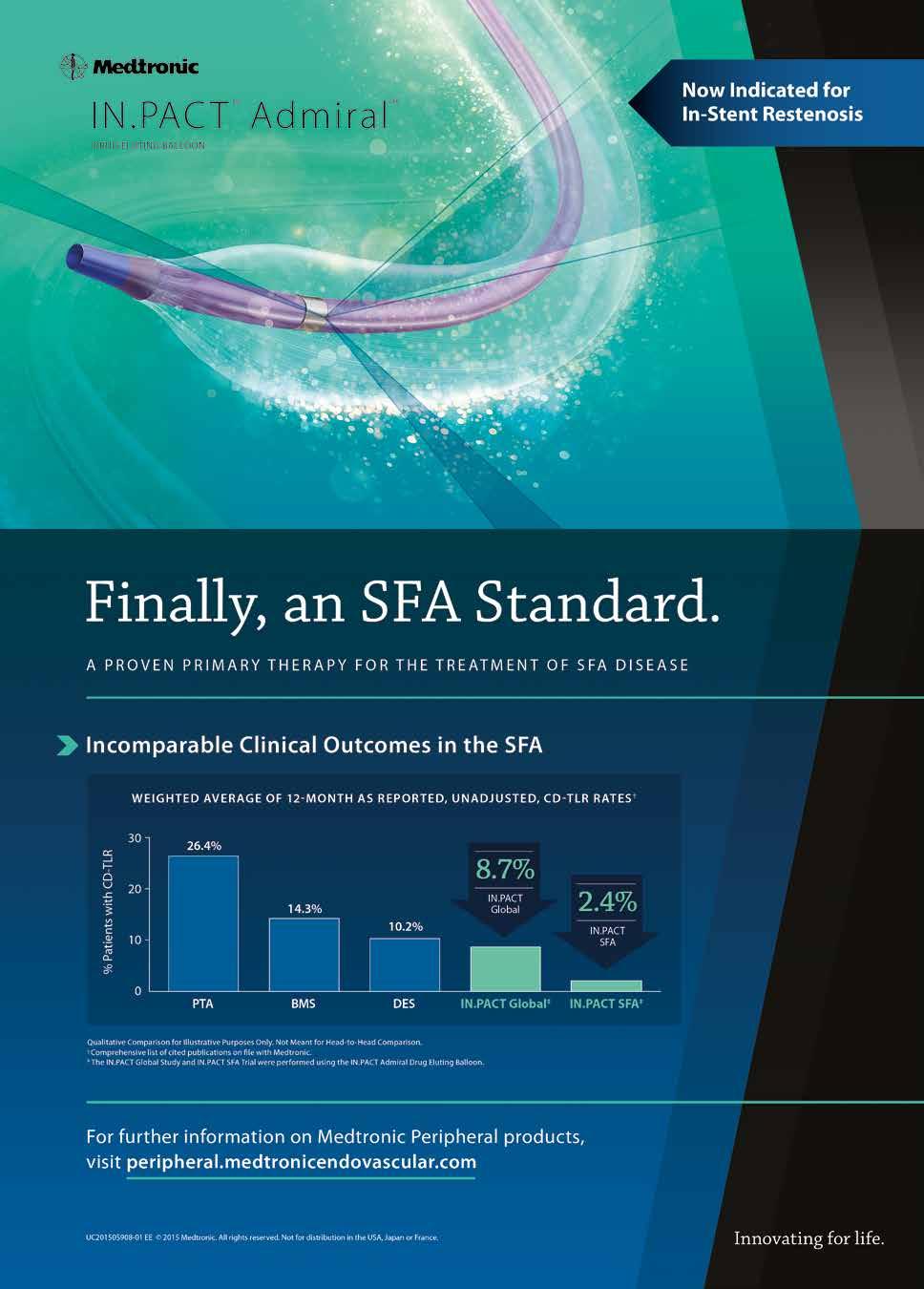
16 16 Peripheral intervention June 2015 ILLUMENATE FIH two-year results presented at Charing Cross 2015 At the Charing Cross Symposium (28 April 1 May, London, UK), Stephan Duda, Berlin, Germany, presented the results of the 24-month ILLUMENATE first-in-human study. These showed that the primary patency rate (as measured by Duplex Core lab evaluation) was 80.3% at 24 months. At 12-months, the primary patency rate was 89.5%. freedom from clinically-driven The target lesion revascularisation rate (as determined by the clinical events committee adjudication) was 85.8% at 24 months and it was 90% at 12 months, Duda said. In the study, researchers evaluated Stellarex in 50 patients with 58 lesions in a cohort that required predilatation with an uncoated balloon before the inflation of the drug-coated balloon. The mean age of the cohort was 69 years. The mean age of patients was 69±9.3 years; Thirty four per cent of patients had diabetes and 80% had hypercholesterolemia; 86% were Rutherford class 3 at baseline; the mean lesion length was 7.2cm; nearly 14% had severe calcification and the mean stenosis at baseline was 75%. The vessel patency was associated with a significant and sustained functional improvement as resulted by the walking impairment questionnaire and by the treadmill test patient subset. There were no cardiovascular deaths or amputations reported throughout the 24-month followup schedule in this cohort, demonstrating the high safety profile, Duda said. He continued: This study demonstrates the safety and efficacy of Stellarex for the treatment of femoropopliteal disease up to two years. The primary patency of 89.5% and 80.3% match the highest benchmark of reported rates at one- and two-years respectively. There is also significant functional benefit observed with improved walking distance, observed up to two years. Duda told Vascular News: Stellarex employs a nextgeneration manufacturing technology and coating formulation. This combination allows for an effective dose of paclitaxel to be transferred to the treatment site using a low drug dose density of 2µg/ mm 2. Pre-clinical work has shown this coating results in high coating stability with limited drug loss and an effective amount of drug in the arterial wall through 28 days. There is a robust clinical programme for Stellarex that is actively underway and will include up to 1,300 patients in five studies, Duda concluded. CX 2015 voting At the Charing Cross Symposium, delegates heard about the Leaving nothing behind concept with presentaitons on the status of drug-coated balloons, cost-effectiveness, vessel preparation and results update from the main trials studying devices currently on the market. The audience heard that the randomised controlled trial data for drug-coated balloons are mostly based on short lesions and 57% voted no to the question, Is drug-eluting balloon technology likely to be a successful standalone treatment for the majority of medium and long length superficial femoral artery lesions? Also at CX, Gunnar Tepe, Rosenheim, Germany, presented 12-month results of the IN.PACT SFA clinical trial, and Dierk Scheinert, Leipzig, Germany, spoke about the Levant 2 randomised trial assessing the performance of the Lutonix drug-coated balloon (Bard). Longer lesions Presented for the first time at EuroPCR 2015 (19 22 May, Paris, France) during a Hot Line session, new clinical data from two different studies show that the IN.PACT Admiral drugcoated balloon from Medtronic successfully treated long lesions in the superficial femoral and popliteal arteries. Dierk Scheinert, University- Hospital Leipzig, Leipzig, Germany, presented 12-month results for 157 patients enrolled in the IN.PACT Global study s long lesion imaging cohort. The average lesion length in this subset was 26.4±8.61cm nearly three times longer than the average lesion length of 8.9±5.07cm included in the randomised controlled IN.PACT SFA trial. The IN.PACT Admiral drugcoated balloon (DCB) received approval from the FDA in December 2014 for percutaneous transluminal angioplasty, after pre-dilatation, of de novo or restenotic lesions up to 18cm in length in native superficial femoral or popliteal arteries with reference vessel diameters of 4 7mm. It received the CE mark in 2009 for angioplasty in patients with obstructive disease of peripheral arteries a broader indication that does not specify lesion length or reference vessel diameter. The 157 patients from the IN.PACT Global Study s long Stephan Duda Dierk Scheinert lesion imaging cohort had a total of 164 lesions of at least 15cm in length. In addition to long lesion length, they also featured other challenging characteristics: 71.8% had calcified lesions, 60.4% had total occlusions and 41% had diabetes. Despite these challenges, The results [for long lesions] are remarkably consistent with those from similar studies of the IN.PACT Admiral drugcoated balloon, irrespective of lesion length. treatment with the IN.PACT Admiral DCB delivered good outcomes at 12 months, including a 6% rate of clinicallydriven target lesion revascularisation and primary patency of 91.1% according to Kaplan Meier analysis at 360 days post-procedure. Scheinert also highlighted key safety data in his presentation specifically, 94% freedom from major adverse safety events and no major target limb amputations through 12-month follow-up. For patients with peripheral arterial disease in the lower extremities, long lesions pose a notoriously difficult treatment challenge, said Scheinert, who is an investigator in the IN.PACT Global Study. That is why the 12-month results in this long-lesion subset are so impressive. The results are also remarkably consistent with those from similar studies of the IN.PACT Admiral drugcoated balloon, irrespective of lesion length. The IN.PACT Global Study has enrolled more than 1,500 patients at 64 sites worldwide to characterise the performance of the IN.PACT Admiral DCB in the context of routine clinical practice. The IN.PACT Global Study s imaging cohort consists of three sub-groups, each with at least 150 patients: de novo in-stent restenosis; long lesions (at least 15cm); and chronic total occlusions (at least 5cm). All patients in the imaging cohort were required to undergo duplex ultrasound at 12-months post-procedure and at the time of a reintervention (if one occurred) to assess for patency. Outcomes for patients in the in-stent restenosis and chronic total occlusion subgroups are expected to be presented at medical meetings over the next 12 months, as are two-year results from the IN.PACT SFA trial, including the economic outcomes analysis. The other study of the IN.PACT Admiral DCB s performance in long lesions presented at EuroPCR 2015, the DEB SFA-LONG Study, was conducted at six sites in Italy and enrolled 105 patients with an average lesion length of 25.2cm. The 12-month results were presented by Antonio Micari, Maria Cecilia Hospital, Palermo, Italy, and were consistent with those from the long-lesion subset of the IN.PACT Global Study s imaging cohort. Using the same definitions, the CD-TLR rate in this independent, multicentre Italian study was 4%, and primary patency was 89.3% according to Kaplan Meier analysis at 360 days post-procedure.
17
18

19 June 2015 Opinion 19 From hopeful trainee to accomplished vascular specialist COMMENT & ANALYSIS It is difficult for a vascular surgeon of yesteryear to comment constructively for the benefit of a vascular trainee of today. Why is that? It is because the subject of the management of a vascular disease has changed so much over the decades, writes Roger Greenhalgh. The content of this article was also subject of a talk at the Porto Vascular Conference 2015, Porto, Portugal. The most important thing for a vascular trainee to recognise is the inevitability of the change of the subject of vascular management over the years of practice. It is important to recognise at an early stage that what is learned at the time of qualification for practice independently will not be what is required to be known during the years of responsibility for managing patients. The trainee of today must prepare himself or herself for the inevitability of the need to learn new techniques for the better to treat the patient of tomorrow. What is learned at the stage of training is simply not going to be enough for the whole of the lifetime to practise at the highest level. Such is evident over the last 20 years. After a period of vascular management which could only be described as the DeBakey era, open surgery was the way to correct heart and heart vessel problems. The Mecca of vascular surgery was Houston, Texas, for the simple reason that Doctor Michael DeBakey dominated the field. His associates Denton Cooley and Stanley Crawford, among others, helped the DeBakey group to pioneer virtually every technical advance. DeBakey himself assisted physiologists to ROGER GREENHALGH create the pump that became the heart-lung machine. This gave birth to the whole possibility of open heart surgery. Every procedure on the heart or the vessels became possible to perform under general anaesthesia. The techniques became more advanced, cardiac transplantation was performed in thousands and most parts of the aorta from the heart onwards were replaced by constructions reminiscent of a road junction. Stanley Crawford was outstanding in creating the so-called elephant trunk operation. He simply stopped the patient s heart by cooling it down, tilted the patient so the blood to the brain would not encourage air bubbles to go to the brain and block future circulation. Because of the cold, the brain was preserved. Stanley and his team would replace aortic disease from the heart onwards, sometimes with the aortic valve, connecting all of the vessels on the way and then warmed the patient up. The heart would start, the vessels would pulsate and the patient would be closed. The whole was rather like opening a can of beans. The patient represented the can and the surgeon was like a can opener. Every vessel that required to be corrected was seen. This was the height of the DeBakey era. Trainees therefore had to learn all of these techniques. In addition, they had to learn operations to correct carotid artery disease and venous disease, including most commonly varicose veins, all done under general anaesthesia. It would be inappropriate to attribute all of the advances to Houston. Certainly this would not be the case. An input in example is from Portugal and another from Argentina. In the late 1920s, Reynaldo dos Santos, professor of Surgery in Lisbon, performed the first arteriogram. In the same city, in the late 1940s, his son Cid dos Santos performed the first thromboendarterectomy of a femoral artery. Cid was a fairly junior surgeon and, asked to remove the clot, took half of the artery wall with it and by pure chance performed an endarterectomy. This became a useful technique of arterial reconstruction for several decades. So just about every form of vascular reconstruction can be performed by open surgery. And then the endovascular revolution struck! The first warning was from Charles Dotter. He favoured angioplasty but the idea did not catch on. Many years later Andreas Grüntzig of Switzerland used a balloon to perform percutaneous transluminal angioplasty and with it the endovascular reconstruction of the arterial system became possible. Thomas Fogarty had already used a balloon to remove clots to do lesser surgical procedures. Then the ultimate strike occurred. At the Charing Cross meeting in 1990 Julio Palmaz described the use of his Palmaz stent to trap the Dacron tube inside an abdominal aortic aneurysm. This was the first procedure the Western world had heard about by Parodi, Palmaz and Barone. From that moment, it was clear that vascular surgery was going to change. Indeed, it did. The last 25 years have seen a revolution of the type which vascular surgery has never experienced before and never will again. The subject of the management of vascular disease is now a multidisciplinary one. Reconstructions can be performed by multiple techniques. Endovascular reconstruction of the whole of the aortic tree, the carotid system and every artery in the body can now be performed. If an embolus goes to the brain, neurovascular radiologists can go and fish it out. The need to open the head for neurosurgery is less. The need to open the chest in terms of thoracic surgery is almost zero. Times have changed. What does this mean for the vascular trainees of today? It means that in the next 30 years there will be huge change just as there has been in the last 30 years and the 30 years before that. It should not come as a surprise. It should be understood that it will occur as night follows day. This is by far the most important message a vascular surgeon can give to the next generation of vascular specialists. There will not be vascular surgeons in the future as there have been in the past. There will be vascular specialists able to reconstruct the vascular system in the very best way according to patient needs. In addition to that, there will need to be an understanding of the very disease process, of why arteries become diseased or dilated and why veins become thrombosed or varicose. The disease process itself will need to be understood and in understanding that, medical management will eventually take over from even the lesser invasive methods of today. In conclusion, trainees of today, please stand by for change in the future. Be ready for it. Let it not come as a surprise. Roger Greenhalgh is emeritus professor of Surgery, Imperial College, London, UK, head of the Imperial College Vascular Surgery Research Group. He is also editorin-chief of Vascular News News in brief Philips and AMC aim to improve care for diabetic patients with severe foot complications Royal Philips and Academic Medical Center (AMC), Amsterdam, The Netherlands, have announced the collaboration in a European multicentre study to investigate a new diagnostic technique targeting immediate assessment of the results of minimally-invasive treatment for diabetic foot and critical limb ischaemia. The study will start in the summer with final results expected in This could be a paradigm shift in our approach to critical limb ischaemia, said Jim Reekers, from AMC, whose team have been testing the new technology and have collected observational data from over 100 cases. If we can predict the effect of treatment immediately after revascularisation, then we will have a head start in developing a pro-active care plan for the patient s recovery at home, instead of a more reactive approach. The first observations using the new diagnostic technique are consistent and promising, and have already provided valuable insights into many pending questions regarding critical limb ischaemia. In collaboration with AMC, Philips is developing a new technology to analyse perfusion angiography images and obtain quantitative information on blood flow in the capillaries in the foot. Philips software assesses subtle physiological changes in the perfusion level. The image can be constructed from a standard digital subtraction angiography performed using an AlluraXper FD20 system, meaning that no additional patient exposure to radiation or contrast agent is needed. The generated perfusion image shows the physiological perfusion state as a colour-coded display. From this information a graphic representation can be obtained, which contains important information about the functioning of the microcirculation. Cordis launches Outback Elite re-entry catheter At this year s Charing Cross Symposium, Cordis launched the Outback Elite re-entry catheter, an enhanced version of the Outback re-entry catheter that received the CE mark in April. According to the company, Outback Elite provides more control and precision and includes additional features to enable re-entry into the most complex lesions whilst facilitating positioning and delivery. Amongst the new features of Outback Elite are single-handed torque and deployment the torque control is located closer to the needle actuator and the longer handle provides a more efficient slider mechanism a robust nitinol cannula for re-entry in very complex lesions and a lubricious hydrophilic coating to help delivery. The Outback Elite is available in a 120cm shaft length as the previous catheter but is also being launched with an 80cm shaft length indicated for ipsilateral antegrade or iliac procedures. The new size offers the advantage of having less shaft length to handle outside of the patient, increasing precision on the re-entry site.



 in light of plans for the first-in-man implant.")
20 20 Updates June 2015 Dragons slayed by new dialysis graft technology In the tradition of the CX Innovation Showcase, the highly-anticipated Dragons Den did not disappoint in 2015 with presentations of 15 new and innovative ideas from physician-inventors from all over the world. With much to consider after two hours of impressive presentations, Jeffrey Lawson (Durham, USA) came out on top, winning over the Dragons and gaining the most votes in his favour for his dialysis graft technology. Lawson spoke to Vascular News about his technology stating, It is a novel dialysis graft that is meant to protect patients when their dialysis graft needs to be cannulated by a sharp needle. You can only cannulate the graft or the blood-flowing portion safely and reliably that is the nature of the innovation. In terms of progress, Lawson reported that animal testing with the device has been done and a very mature prototype design has been developed. Further, he said New graft that his team has met with the US Food and Drug Administration (FDA) in light of plans for the first-in-man implant. Commenting on the value of the Dragons Den, Lawson said, It is a wonderful opportunity, and it is fun. It is also really good to see other people s technology making progress. Speaking to Vascular News, course director and chairman, Stephen Greenhalgh said, The feedback I received from the Dragons was that this year saw the most wide-ranging, innovative group of presentations that we have ever had at Charing Cross, and based on Jeffrey Lawson (standing, second from right) with the Dragons Den judges voting results where varying presentations received recognition from the individual Dragons it shows how closely fought it was. Speaking of the future of the CX Dragons Den, Greenhalgh added, I just want to ensure that Charing Cross always provides a platform for early stage innovation. Honourable mention was also given to Peter Philips (Didcot, UK) for his ideal compression stocking; Tim Chuter (San Francisco, USA) for his Inchworm balloon; and Lindsay Machan (Vancouver, Canada) for his uniform pressure non-straightening angioplasty balloon. Popliteal aneurysm should continue to be treated with open repair, say 75% of CX voters During a debate on the management of popliteal aneurysms at the Charing Cross Symposium, 75% of delegates voted against the motion Popliteal aneurysm should be treated by endovascular means. The motion was debated by Martin Bjӧrck, Uppsala, Sweden, who spoke against, and Michele Antonello, Padua, Italy, who spoke in favour. A relatively rare condition occurring in 1% of men aged years, popliteal aneurysm is difficult to study. There are only a small number of patients and the choice of treatment remains controversial. Given the risk of negative outcomes associated with the condition, including severe ischaemic manifestations secondary to embolisation and thrombosis, rupture, and compression of adjacent veins and nerves, proactive and adequate treatment is of great importance. Because it is associated with rupture, the most obvious criterion for intervention is size. However, rupture only occurs in 2% of surgical patients and the risk of thrombosis and embolisation the most frequent severe event is not entirely dependent on the size of the aneurysm. The question of a conservative or open approach to treat this condition has been raised before. Fifty years ago it was decided that an aggressive approach was preferable to a conservative one due to the higher risk of amputation in emergency cases with the conservative approach, though exactly what patient criteria would justify intervention has remained controversial. With the proliferation of endovascular techniques, this debate has once again come to the fore. Two specialists gave their opinions on the current treatment options for the condition. Open repair The speakers explained that the technique of vein inlay for the repair of an aneurysm with a posterior approach was presented in 1947 and became popular during the 50s. The medial approach, with bypass and proximal and distal ligation of the popliteal aneurysm was first described in 1968, and has since become (and remains) the most common treatment. The posterior approach was reevaluated and regained popularity following reports of aneurysmal sack growth, due to endoleak, with the medial approach. Comparison between the two techniques is difficult, as the medial approach when the aneurysm extends into the superficial femoral artery, above the adductor canal (Hunter s canal), whereas the former cannot. Evaluations that have taken these aspects into account have not shown any significant differences in patency rates. As such, the choice between the two Martin Björck Michele Antonello approaches is largely based on the extent of the aneurysm and surgeon preference. Long-term results of open surgery are well documented, with a recent study presenting five-year primary and secondary patency rates of 88% and 96% respectively, in a cohort of patients in whom only 57% were asymptomatic. Other publications have confirmed the results of good long-term patency and limb salvage. Mortality and morbidity have also been shown to be low with open repair. In a registry of 2,962 patients, endovascular treatment was not associated with any benefit in mortality or cost but was associated with more reinterventions. A high rate of occlusions (more than 20%) within two years has been reported after endovascular repair, leading to reinterventions with thrombolysis or bypass surgery in 65% of patients (15/23). Bjӧrck told delegates, Open surgery is the gold standard for definite repair of popliteal aneurysm. Preoperative thrombolysis can improve outflow and results. Whenever possible, use an interposition vein graft with the posterior approach. Endovascular stent graft treatment for popliteal aneurysm is experimental and should not be offered patients outside of trials, other than in compassionate cases. Continuing, Bjӧrck suggested that although endovascular repair is a tempting alternative to open repair for surgeons because of its simplicity, knowledge of which clinical situations are best suited to the approach is scarce. Data for long-term durability with the endovascular approach were also said to be lacking, as were data regarding how much the results of endovascular differ to open surgery for acute ischaemia. Bjӧrck concluded, and 75% of CX voters agreed, that Open repair remains the first-line choice for repair of a popliteal aneurysm in the absence of further studies and data. Endovascular repair Endovascular options now dominate most areas of vascular surgery. In recent years, results for endovascular repair have accumulated. Most concern asymptomatic popliteal aneurysms, however, and the number of legs treated in each study varies there has only been one randomised study comparing open and endovascular approaches (30 legs) and long-term data are scarce. Short-term results of endovascular repair are comparable with open repair, when asymptomatic patients are operated on, although even in this situation operations with vein grafts have better results. Overall these studies report primary patency rates at one year of 75 93% and secondary patency rates of more than 90%. Despite high two-year secondary patency rates, a large proportion of patients (10 51%) were lost to follow-up in these studies. In this setting we can really obtain optimal results in term of limb-salvage and patency rate, explained Antonello. I believe that open repair and endovascular treatment for popliteal aneurysm must be considered not as one against the other, but as two solutions to solve at a problem. In countries where an endovascular approach is used for popliteal aneurysms, the number of procedures has increased. A registry of 290 centres in the USA and Canada the Vascular Quality Initiative reports an increase in endovascular repairs from 34.8% in 2010 to 47.6% in In the Vascunet collaboration, popliteal aneurysm repair could be identified in eight countries for comparison and the proportion of endovascular repair varied from 35% in Australia to 0% in Switzerland, Finland and Iceland. According to Bjӧrck, We have introduced a new treatment without having proper evaluation of long-term results. Many patients are being treated experimentally. However, Antonello disagreed, arguing that given time and with appropriate use, endovascular can challenge open repair. He said, With appropriate indication endovascular treatment for popliteal aneurysm is comparable results to open repair, especially in terms of limb salvage and prevention in aneurysm growth with a less invasive approach it is the future. During the voting, the majority of delegates backed Bjӧrck against the motion.

21
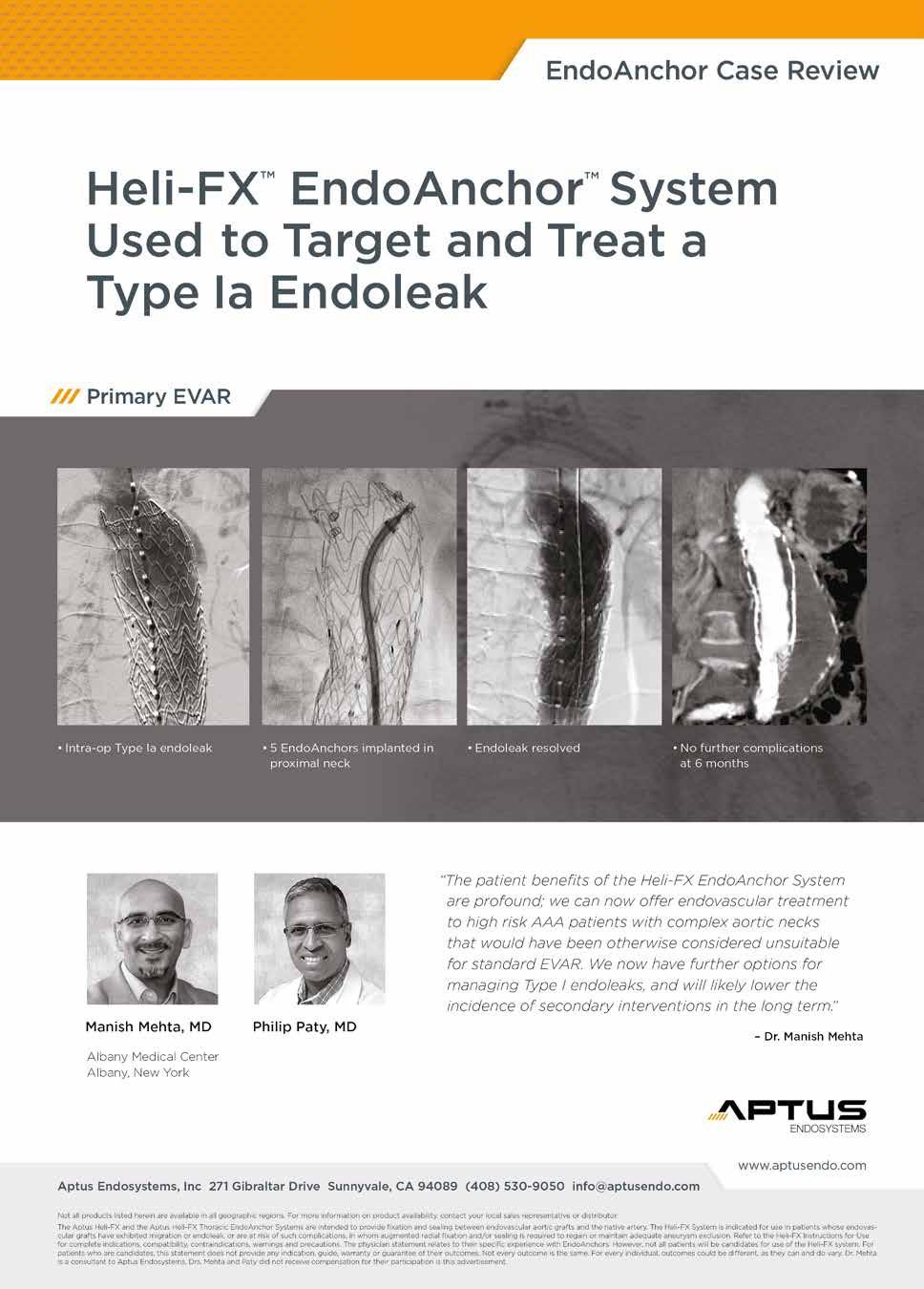
22

23 June 2015 Companies announce new round of renal denervation randomised trials Following the results of SYMPLICITY HTN-3, which failed to show benefit of renal denervation in resistant hypertension patients, Medtronic announced in April the initiation of the SPYRAL HTN clinical trial programme, studying renal denervation in uncontrolled hypertension. Also in April, Boston Scientific announced the initiation of the REDUCE-HTN: REINFORCE, a randomised, sham-controlled study designed to demonstrate the effects of the Vessix renal denervation system by minimising variability and factors that may have affected results in SYMPLICITY HTN-3. Like Boston Scientific, Medtronic stated that the two global studies of the SPYRAL HTN programme have been designed to address the confounding factors encountered in SYMPLICITY HTN-3, including medication, patient population and procedural variability, to ensure the clinical potential of the therapy is evaluated. Physicians in both studies announced by Medtronic will perform renal denervation with Medtronic s nextgeneration renal denervation technology, composed of the 6F-compatible, multielectrode Symplicity Spyral catheter and Symplicity G3 radiofrequency generator. The Symplicity Spyral catheter and G3 generator are investigational in the USA and Japan. The principal investigators for the two global studies are Michael Böhm, University of Saarland in Homburg/ Saar, Germany; David Kandzari, Piedmont Heart Institute in Atlanta, USA; Kazuomi Kario, Jichi Medical University School of Medicine in Tochigi, Japan; and Raymond Townsend, University of Pennsylvania, USA. The SPYRAL HTN programme includes two global, prospective, randomised, sham-controlled trials conducted simultaneously to investigate the impact of renal denervation both in the absence of and in the presence of antihypertensive medications. The SPYRAL HTN-OFF MED and SPYRAL HTN-ON MED studies will each include approximately 100 patients with moderate- to high-risk hypertension, as opposed to the severe, treatment resistant population studied in SYMPLCITY HTN-3. These studies will be conducted at approximately 20 centres in the USA and other countries. The SPYRAL HTN-OFF MED study is designed to isolate the effect of renal denervation on blood pressure reduction. Similar to the traditional design of antihypertensive pharmaceutical clinical trials, this approach was recommended by both the FDA and the global clinical community. Separately, the SPYRAL HTN-ON MED study will evaluate the effect of renal denervation on blood pressure in the presence of antihypertensive medication. Unlike the SYMPLIC- ITY HTN-3 trial, which enrolled patients with very high blood pressure that was not controlled despite an average of five antihypertensive medications at maximum tolerated dosages, the SPYRAL HTN-ON MED study requires patients who, despite use of drugs from three of the most common classes of medications prescribed for hypertension, do not achieve adequate blood pressure control. These drugs are not required to be prescribed at maximum tolerated medication dosages, a factor which may have contributed to variability in patient adherence and the large number of medication changes during SYMPLICITY HTN-3. Additionally, adherence will be closely monitored and there will be a focus on Updates 23 ambulatory blood pressure monitoring to ensure consistency between both arms of the on- and off-medication studies. Based on the outcomes of these two initial studies of the SPYRAL HTN programme, Medtronic will evaluate next steps for a pivotal study to support a pre-market application submission to the FDA and Shonin submission in Japan. Vessix sham-controlled study The first patient in the REDUCE-HTN: REINFORCE study was enrolled at Cardiology P.C. at Princeton Baptist Medical Center in Birmingham, USA, by Farrell Mendelsohn (site principal investigator) and referred by Michael Wilensky. Boston Scientific has received an investigational device exemption (IDE) for the study from the FDA. The REDUCE-HTN: REINFORCE study will enrol 100 patients. The primary efficacy assessment is the mean reduction in average 24-hour ambulatory systolic blood pressure at eight weeks post randomisation. First results may be obtained in the first half of According to Boston Scientific, the Vessix system is a differentiated and advanced renal denervation system using a multielectrode bipolar catheter designed to reduce procedural variability. It features a 30-second treatment time and an over-the-wire, balloon-based approach familiar to most cardiac and vascular specialists. Previous results of renal denervation studies have been affected by a focus on patients with the difficult-to-define condition of treatment-resistant hypertension, made even more complex by uncertainties regarding their use of hypertension medications, says Michael Weber, co-principal investigator, SUNY Downstate College of Medicine, New York, USA. We need to find clarity, and we believe this innovative study design will enable us to do so. Three-year results of the INNOVATION study confirm earlier very promising findings The INNOVATION study found that the rate of freedom proximal type I endoleaks and the rate of freedom from reintervention in patients who underwent endovascular aortic aneurysm repair (EVAR) with the Incraft (Cordis) device was, respectively, 100% and 95%, at three years. In this interview, Vascular News speaks to Giovanni Pratesi (Florence, Italy) who presented the data at the Charing Cross Symposium (28 April 1 May, London, UK) about Incraft and the three-year results. How does the Incraft stent graft differ from other EVAR devices? It is a new-generation stent graft system with unique features that have been specifically designed to overcome the limitations of current stent grafts. For example, the ultra-low profile integrated delivery system (14F OD) offers excellent navigational opportunities in challenging access vessels. Additionally, the micrometric deployment system allows for accurate placement either at proximal and distal attachment site. Bilateral in-situ length adjustment, up to 3cm, permits you to customise every implant on the single patient anatomy. Therefore, the Incraft system, according to the few-fits-most concept, is able to cover a large spectrum of anatomies with only 23 product codes, four main bodies and 19 iliac limbs. What are the main results of the INNOVATION study at three years? The three-year results of the INNOVATION study have confirmed the very promising one- and two-year outcomes of the study. These data show, at three years, the device is associated with 100% freedom from type Ia Giovanni Pratesi and III endoleaks, stent-graft migrations, and device- or procedure-related major adverse events. They also show that the rate of limb patency is 97.8%, with only one case of limb occlusion. Other findings from the three-year data indicate that there is a significant reduction in mean aortic aneurysm diameter, up to 15 mm, compared with two-year data, a freedom from sac increase of 95.6% and freedom from stent fractures of 97.7%. Core lab analysis has identified two cases of aneurysm sac enlargement both associated with a persistent type II endoleak and one case of stent fracture, but these events did not appear to have any clinical consequences. What other data were included in your presentation? I specifically addressed endograft durability and anatomical preservation in my analysis of the Innovation study. Data from core lab analysis have confirmed the excellent stent graft stability that has already been observed during follow-up. A median proximal migration of 2mm was observed at three-year compared with the one-month computed tomography (CT) scan. The same result was achieved in terms of distal migration with a median change of 1.1mm and 2mm on the right and left side respectively, compared with the one-month CT scan. Aortic neck diameter, neck angulation and iliac artery diameter, compared with one-month CT scan, were analysed at three years to review endograft influence on anatomic changes during follow-up. The observed 1mm proximal neck dilatation and 2mm iliac artery dilatation, combined with the 0.6 degree changes for infrarenal neck angulation and 2.4 degree for suprarenal neck angulation, confirmed the excellent stent graft conformability to the preoperative anatomy. What were the main take-home messages from your presentation? These data confirm the very promising earlier outcomes of Incraft stent graft system and add new evidence regarding its effectiveness in terms of anatomy preservation with a 100% freedom from both proximal aortic neck and iliac dilatation, and from proximal supra- and infrarenal aortic neck angulation changes.

24 24 Interview June 2015 Profile Janet Powell After obtaining a PhD in Biophysics in London, UK, Janet Powell, professor of Vascular Biology & Medicine at Imperial College, London, studied medicine in the United States, before returning to the UK where she completed clinical training in pathology, specialising in cardiovascular risk. In this interview, Powell tells why the cause and management of abdominal aortic aneurysms are her major research interest and speaks about her early career, her mentors, the IMPROVE randomised controlled trial, and also her interests outside medicine. How did you come to choose medicine as a career? And why pathology and cardiovascular risk? I was envious of the clinicians understanding of the integration of the physiology and pathophysiology of the body: only with such understanding and collaborative research can one obtain the evidence for improvements in patient care. So there always was a strong interest in pathophysiology. However, the choice of pathology, rather than an interventional speciality, was driven mainly by the need for work-family balance, since I had two small children at home throughout my training period. The choice of cardiovascular risk, or endocrinology, as a speciality allowed for continued patient contact and care. Who were your mentors and what advice from them do you still remember? Professor Donald Massaro, a pulmonary physician, who thought about pathophysiology in big pictures, was definitely a mentor. He was convinced that better science would lead to better clinical care. How did you develop your interest in vascular biology and clinical trials? I was interested in the pathophysiology of elastic tissues and working with Roger Greenhalgh, the aorta became the key vessel of interest. These horizons expanded after a sabbatical year at the Red Cross Laboratories in Amsterdam, where Jan van Mourik was a fantastic adviser. Science is based on experiments and evidence and I soon appreciated how randomised clinical trials were the best experiments to gain new evidence in clinical medicine and the best outcomes for patients. The cause and management of abdominal aortic aneurysms are your major research interests. How did it all begin and what was your first piece of work in this field? It began through my interest in the pathophysiology of elastic tissues. The first piece of work was a comparison of the concentration of acute phase reactants (including CRP) in the serum of patients with abdominal aortic aneurysm and patients with occlusive aortic atheromatous disease, pursuing evidence for the hypothesis that inflammation played an important role in the development of aortic aneurysms. The death of my father from aortic dissection sharpened my focus on degenerative disorders of the aorta. The one-year results of the IMPROVE randomised controlled trial were published in the European Heart Journal in April. How do you interpret the data and what does the trial add to the literature? The outcomes important to patients are not necessarily the same outcomes as those using to evaluate the success of treatments in clinical trials. Before we designed the trial, Rob Hinchliffe and I discussed with several patients and their families what they viewed as the most important outcomes to evaluate after aneurysm rupture. The focus was not on who lived and who died but on who came back home, how quickly and without any added disability. Accordingly, we started planning a trial using inhospital mortality as the primary outcome, with patient disposal and quality of life as secondary outcomes. In contrast, surgical reporting standards focus on 30-day mortality and to get the trial funded we had to use this as the primary outcome measure. Interestingly, our one-year results show that the patient-preferred outcomes are all better using an endovascular strategy, even though there was no significant survival advantage. In addition, the endovascular strategy appeared to be cost-effective. Through the trial we saw more and more centres becoming eligible to join the trial (ie. have credentialed experience in elective and emergency EVAR). Some of them were at an early stage of teamwork using emergency EVAR. So the question has been asked, did we do the trial too early? Of course not, if we had left it longer it might have been too late, with very experienced centres preferring EVAR. There was also the risk of surgeons losing equipoise by listening to the apples versus oranges comparisons from the likes of Frank Veith. The IMPROVE trial has shown how influential aortic neck length is in predicting mortality: the easy EVAR cases with long proximal aneurysm necks have low mortality after both EVAR and open repair, whilst those with short necks are predominantly treated with open repair and do much worse. So comparing observational data for emergency EVAR versus emergency open repair compares patients with long necks versus patients with short necks: apples and oranges. The results from emergency EVAR may improve with time and if so, this will be an added reason to encourage the wider use of emergency EVAR. Overall the current findings from IMPROVE lead to encouragement for the increasing use of endovascular repair. With survival of discharged patients being so good at one year, with so few delayed reinterventions, we need the three-year results to confirm or refute such encouragement. Critics often say a trial comparing EVAR and open repair for ruptured abdominal aortic aneurysms is not needed. How do you respond to criticism towards IMPROVE? Mainly with the fallacy of the apples and oranges comparison described earlier. In addition, we needed to know whether


25 June 2015 Interview 25 Fact File Science is based on experiments and evidence and I soon appreciated how randomised clinical trials were the best 'experiments' to gain new evidence in clinical medicine and the best outcomes for patients. organisational changes to provide more widespread emergency endovascular repair might be necessary. What piece of research are you most proud of and why? Anything that improves outcomes for patients, including all the randomised trials of abdominal aortic aneurysm management, as well as an early piece of pathology research which showed the importance of inflammation in the developing aneurysm a theme still being investigated by vascular biologists and evaluated in randomised trials. The rate of abdominal aortic aneurysm is falling. In your opinion, why is this happening? Do you see it as a continuous trend? This is largely due to the changes in smoking prevalence and practice. In men it appears to be a continuous trend but the same is not true in younger women. So in the future we might see the prevalence increasing in women. You are participating in the AARDVARK clinical trial, which is assessing the use of an ACE inhibitor in abdominal aortic aneurysms. What are your expectations with regards to the results of this trial and other potential medical therapy approaches for the condition? I wish that I was more optimistic but the RESCAN study suggests that single therapeutic agents are unlikely to have large enough effects on aneurysm growth. But wait and see, we shall have the results very soon. What advice do you usually give to young vascular surgeons starting their research careers? Do something you enjoy and believe in something that will enhance your standing beyond your research period eg. learning how to measure things properly, test new ideas and technologies, do a systematic review, assess the grey areas in vascular surgery. What is the most interesting paper you have come across recently? The ROX CONTROL HTN trial, using endovascular implantation of an arteriovenous coupler device to reduce blood pressure (Lancet 2015;385:1634). What are your interests outside of medicine? Outside of work, I spend time with my son, daughters, grandchildren and friends. I also enjoy trekking and maintenance of local area footpaths, growing my own vegetables (I have a large garden), bird-watching, contemporary cinema and theatre (last play seen was View from the Bridge, which was excellent I am an Arthur Miller fan). Also, I am a local school governor. So nothing very extraordinary! Professor of Vascular Biology & Medicine at Imperial College, London, UK Education BSc in Chemistry, 1968, Oxford, UK PhD in Biophysics, 1972, London, UK MD Medicine, 1981, University of Miami School of Medicine, USA FRCPath Pathology, specialising in cardiovascular risk Trials UK Small Aneurysm Trial POBBLE EVAR trials 1 and 2 IMPROVE AARDVARK Publications Cochrane reviews (2 published in 2012 with one 2014 update) 2011 ESVS guidelines for clinical practice relating to abdominal aortic aneurysm In total, more than 200 original papers listed in PubMed, including one in Nature and 3 in the New England Journal of Medicine Either chief investigator or a co-investigator on four Health Technology Assessment projects Journals Associate editor of the Arteriosclerosis, Thrombosis & Vascular Biology Editorial Board, Circulation Ex-associate editor of the European Journal of Vascular & Endovascular Surgery Award 2012, Life time achievement award, Vascular Society of Great Britain and Ireland
26 26 Updates June 2015 Early results for new carotid embolic protection systems reported at EuroPCR The CGuard embolic prevention system (InspireMD) has shown positive results in the PARADIGM study of all-comer carotid revascularisation patients, and the Wirion device (Allium Medical), has shown to be safe and effective in patients undergoing carotid stenting. Results for both systems were presented at EuroPCR (19 22 May, Paris, France). PARADIGM is a prospective evaluation of all-comer percutaneous carotid revascularisation in symptomatic and increased-risk asymptomatic carotid artery stenosis using CGuard mesh-covered embolic prevention stent system. The study indicated that the CGuard system is appropriate for use in an all-comer carotid revascularisation population and is associated with favourable angiographic and clinical outcomes. Principal investigator Piotr Musialek commented, Our experience with CGuard continues to be very positive. Evidence shows the device s applicability for use in an all-comer population with no major adverse cardiac or neurological events (MACNE) during the procedure and at 30 days. We were also pleased with CGuard s antiembolic performance as well as its flexibility. Impressively, we had a procedure success rate of 100%. During his clinical presentation from the 71 CGuard procedures in unselected all-comer patients in the PARADIGM evaluation, Musialek summarised: Stent system success and procedure success rate were 100% Periprocedural complications were 0%, and remained so at 30 days No MACNE occurred periprocedurally or at 30 days, by operator-independent neurologist and non-invasive cardiologist evaluation. Musialek stated, The system is unique in that it combines the most closed of the closed cell designs with the most open of the open cell designs, and concluded, Our experience indicates routine use of CGuard, which we believe presents a significant technological and clinical advancement, may form a new paradigm in carotid revascularisation. Wirion embolic filter safe and effective The positive 30-day results from 120 patients out of a planned 240 patient cohort at high risk for endarterectomy, who underwent carotid artery stenting using the Wirion embolic protection device (Allium Medical), were published in EuroIntervention and presented at EuroPCR 2015 (19 22 May, Paris, France). The data have shown that the Wirion embolic protection device in carotid artery stenting is safe and effective when compared to historical data in a population that includes high-risk patients. This early European experience from Alberto Cremonesi, Villa Maria Cecilia, Cotignola, Italy, and colleagues, using a novel guidewire-independent distal filter showed that the system is simple to use and highly rated by users. The ability to cross the lesion over a guidewire of choice and deploy the filter in the exact desired location creates a unique, natural and appealing advantage for all indications, the authors write in EuroIntervention. At EuroPCR 2015, Bernhard Reimers, Cardiology Department, Mirano Hospital, Mirano, Italy, presented the results. In March, the company announced the decision to stop recruiting additional patients in view of the successful compliance with all clinical trial objectives at this early stage. The Wirion embolic protection device is a rapid exchange pre-crimped distal filter system that can be used with any guidewire. It is a stent-like system in form and operation. The Wirion system is deployed after a guidewire of choice is positioned across the lesion in a standard fashion. Then, the Wirion standalone filter unit can be delivered, positioned and locked anywhere along the guidewire, resulting in smooth crossing of the lesion and optimal protection position along the artery. Wirion has received the CE mark and is at an advanced stage in the application for US FDA approval. One hundred and twenty patients who were high-risk for surgery were enrolled. The mean age of the cohort was 73.9 years, and 14 patients were symptomatic and 106 were asymptomatic. The lesions treated had an average stenosis of 84%. The 30-day composite primary endpoint of major cardiac and cerebrovascular events (MACCE) was 3.3%, with 0% death. Of these patients, one patient had contralateral stroke and a second patient had type 2 NSTEMI secondary to new untreated anaemia. Both were decided by the clinical event committee as non-procedure-related events. Only two patients (1.7%) experienced procedure-related events. The MACCE rate in the study was compared with an historical control group of high surgical risk patients showing significantly better performance. The device success rate was 99.2% and angiographic success was achieved in 97.5%, the authors write. News in brief Essential Medical announces successful additional clinical studies for Manta large bore vascular closure device Essential Medical has successfully completed additional clinical studies using its Manta 14F large bore vascular closure device, a vascular closure device designed to seal both 14F and 18F large bore femoral punctures. Manta 14F devices were successfully deployed in four patients, achieving immediate or rapid haemostasis following 14F balloon aortic valvuloplasty cases with excellent clinical, angiographic and haemodynamic (Duplex Ultrasound) results, said a company press release. All patients were successfully discharged the following day. The Manta devices were deployed in less than one minute, without pain or discomfort for the patients. Manta closes femoral arterial punctures made during cardiac catheterisation procedures such as transcatheter aortic valve replacement, balloon aortic valvuloplasty, and the endovascular treatment of abdominal aortic aneurysms. Manta utilises novel closure mechanics and can be deployed in less than 60 seconds with sealing components similar to the company s other closure device, X-Seal. The potential worldwide market for vascular closure products is approximately US$1bn. Large bore femoral access has been associated with significant morbidity including bleeding complications, the need for transfusions, increased hospital costs, patient discomfort and disability. Essential Medical believes that the Manta device has the potential to address all the aforementioned problems. This series, together with our successful patients with Manta 18F last November, provides the necessary confidence to proceed to a EU CEmarking study including both Manta sizes, commented Greg Walters, chief executive officer. We expect to enrol patients early this summer at sites in Vancouver, Rotterdam, Amsterdam and Milan. The company has also enrolled the first patients in a post-market study in Germany utilising its X-Seal smallbore closure devices. The company is conducting a 50-patient study as a requirement for X-Seal CE mark approval that was received in October Commercialisation of X-Seal is expected through a strategic partner once the study is complete. Shockwave Medical announces US$40m in funding for Lithoplasty system Shockwave Medical has announced US$40m in funding, coled by returning investor Sofinnova Partners and new investor Venrock, with the participation of RA Capital, Deerfield, Sectoral Asset Management, Ally Bridge Group, and two undisclosed large-cap strategic investors. Proceeds from the financing will be used for development of the company s Lithoplasty balloon catheters in peripheral, coronary and aortic valve applications. The company recently reported six-month follow-up results from the DISRUPT PAD trial, a 35-patient study of patients with calcified vascular stenosis of the superficial femoral artery (SFA) and popliteal artery treated with the Lithoplasty system. Data reported at the 37th Annual Charing Cross 2015 Symposium in London (28 April 1 May, London, UK) demonstrate safe and effective dilatation of calcified stenosis with no acute failures, favourable residual stenosis, no major device-related adverse events and no need for stent placement. Six-month durability was excellent with no need for retreatment and patency by duplex ultrasound of 83%. Shockwave Medical chief executive officer and co-founder Daniel Hawkins said, We believe the Lithoplasty system is uniquely suited to address substantial unmet needs in the treatment of patients with peripheral, coronary and aortic valve disease using a balloonbased approach that is inherently familiar to physicians. Our returning and new investors provide us the depth of resources and breadth of support needed to achieve our goal of changing the paradigm in the treatment of advanced cardiovascular disease. We were very impressed with the level of interest and the quality of the investor group that Shockwave was able to bring into this new funding round, with blue-chip financial investors as well as two major corporate investors, said Antoine Papiernik, managing partner of Sofinnova Partners. This is a tribute to the strength of the Lithoplasty technology as well as to the work that management has done to develop it to this stage.
.")

27 June 2015 Carotid arteries With a micromesh stent and its sustained antiembolic action we can solve limitations of carotid stenting 27 Micromesh stents and sustained antiembolic action to reduce cerebral embolisation may contribute to solving the remaining limitations of carotid stenting, according to Alberto Cremonesi (Cotignola, Italy). In a presentation during the Interventions for ascending and arch of the aorta session at the Charing Cross Symposium (28 April 1 May, London, UK), Cremonesi looked at the potential for micro-mesh to improve existing carotid artery stenting outcomes. He told delegates that the correct technique for performing a carotid artery stenting was to conduct a preprocedural evaluation for common carotid engagement, to select the correct stent and to select and manage an embolic protection device. Cremonesi said that it is already known that not all plaques are the same, and that carotid artery stenting and carotid endarterectomy are and will remain emboligenerating procedures. He told the audience that it is possible to give sustained anti-embolic over time with specific stents. When a poorly-selected stent is used for carotid artery stenting, intrastrut prolapse can occur resulting in post-procedural embolic events. The difficulty then, commented Cremonesi, is that lesions in the carotid arteries are often anatomically and morphologically very challenging. For this reason, plaque coverage can play an important role. The use of stenting strategies such as open cell, closed cell and hybrid geometry can be considered time honoured. Now, vascular specialists have access micromesh double layer carotid stents (Terumo, inspiremd and Gore), said Cremonesi, whose personal experience is with the Roadsaver carotid stent from Terumo. Cremonesi admitted that In terms of data, we do not have very much at the moment for the use of micromesh. Some data do exist from the CARENET all-comer trial, in which 30 patients saw very good outcomes without any neurological events up to five months follow-up. A further multicentre trial with 100 patients, CLEAR-ROAD, is also beginning, though Cremonesi said that he did not want to conclude anything about it yet. We are probably changing the paradigms in carotid artery stenting, because with these micromesh stents and their sustained antiembolic action, we can solve the remaining limitation of carotid stenting, concluded Cremonesi. Discussing his presentation with the audience, Cremonesi mentioned that two-thirds of the embolic complications are in the postprocedural phase. When session chairman Roger Greenhalgh asked about the cause for this later onset of complications, Cremonesi told him that it was due to the stent interacting with and cutting the plaque in the carotid artery, which can occur during the phase and even up to 48 hours later. Cremonesi made it clear that this problem is one of the carotid artery, rather than one associated with the aortic arch. Alberto Cremonesi

vascular graft is a rare but severe condition posing a serious clinical challenge.")



28 28 Aortic infection June 2015 Spiral saphenous vein reconstruction of the infected aorta: a strategy to adopt COMMENT & ANALYSIS Jan Heyligers and Patrick Vriens, Tilburg, The Netherlands, write about a technique using the great saphenous vein for the reconstruction of an infected aorta. The technique, defined as a see one, do one procedure, was presented at the Charing Cross Symposium in April. Infection of an aortic aneurysm or (endo)vascular graft is a rare but severe condition posing a serious clinical challenge. Percutaneous drainage and an antibiotic regimen may offer a temporary solution. However, radical surgical debridement and in situ autologous reconstruction are the cornerstones of long-term, infectionfree success. The Tilburg group has successfully introduced the spiral vein technique using the great saphenous vein to construct a tailor-made autologous neo-aorta in infected cases, with good and reproducible results. Background and implementation of the technique Infection of the aorta is a severe condition and a challenge to vascular specialists worldwide. The aorta has either been initially infected, or in most cases infected after surgical repair. Infection is seen in about 1 3% of cases after aortic aneurysmal repair, and morbidity and mortality are high. Patients may suffer from severe sepsis. CTA, PET scan analysis, guided puncture and culturing are obligatory for the definite diagnosis. Often an aortoenteric fistula is the underlying cause of the infected aneurysm (graft). Cultures can show various bacterial pathogens, both Gram negative and positive. Primary infection with Coxiella burnetii bacteria in patients with chronic Q fever is notorious in the southern part of The Netherlands. Leaving the infected aorta untreated can lead to death in up to 80% of cases. We first published our spiral vein technique in 2006 for a ruptured primary infected aneurysm. The patient did well and was on antibiotics for only three months after surgery. She survived more than eight years with no signs of reinfection. This initial success in a ruptured JAN HEYLIGERS PATRICK VRIENS Figure 2 case prompted us to further develop this innovative technique. In 2010, we published the results of five patients treated with spiral vein reconstruction of the infected aorta. The technical success of the procedure was 100% and 30-day survival 80%. These data were compared to a cohort of patients treated in our institution with the Glagett-Nevelsteen procedure, using the femoral vein. Our results with spiral vein were at least as good, but with less morbidity, as there is hardly any morbidity in harvesting the great saphenous vein. Furthermore, the Infection of the aorta remains a severe and challenging clinical condition and we continue to develop and improve innovative techniques to create the best outcomes for our patients. Figure 1 Figure 3 spiral vein technique allows for creating a conduit of any desired length and diameter. Other techniques, like replacement with impregnated grafts, xeno-grafts, extra-anatomical bypass or percutaneous drainage with life-time antibiotic regimen, do not totally eradicate infection and therefore are inferior to venous autologous replacement. Technique The great saphenous vein is harvested using longitudinal incisions in the leg. The vein is isolated and side branches are ligated using vicryl 4.0. The vein is then cut open longitudinally to create a ribbon that is wrapped around a tube of any desired size to create a neo-aorta. To calculate the length of vein that is needed, CTA reconstruction of the aorta is performed to measure the required length of the conduit. By using the formula 2πr (r = half of the diameter of the vein), the needed length of the vein can be calculated. The vein is then sutured around the tube using a non-absorbable monofilament 6.0 wire (eg. Vascufil or prolene) (Figure 1). In the meantime, a second team performs the abdominal phase. A midline laparotomy is performed and the infected aorta is exposed. After radical surgical removal of the infection and the infected graft, the constructed spiral vein is sutured in with a monofilament 4.0 wire using an inlay technique (Figure 2). Before closure the omentum is divided and brought to the neo-aorta in a retrocolonic fashion by an opening in the mesenterium (Figure 3). The spiral vein reconstruction is covered with omentum as an adjunct on the infected area. The abdomen is then closed in a conventional way. Antibiotics are continued up to three months after surgical repair, on the basis of pre- and perioperative culture results. Results The technique has been adopted by several other Dutch vascular centres. Up to now, 28 patients have been treated using this technique. The results were presented during the Charing Cross Symposium (28 April 1 May, London, UK) in the CX Innovation Showcase sessions. They were quite similar to the first five patients that were analysed and published in Of 28 patients (almost all male), 16 were treated for infection after aortic repair. We report technical feasibility of 100% in this series and a 30-day survival of almost 80%. The one-year survival is 69% and reinfection has not been seen with a median followup of nine months. No morbidity of the retrieval of the greater saphenous vein has been reported. Interestingly, followup CT scans have not shown dilatation of the spiral vein neo-aorta in any of the long-term surviving patients. A technique to adopt Infection of the aorta remains a severe and challenging clinical condition. We continue to develop and improve innovative techniques to create the best outcomes for our patients. Fortunately, aortic infection is a rare condition that vascular specialists (hopefully) hardly see in their daily practice. As the exposure is low for individual surgeons, this easy-to-adopt technique seems a solution for vascular surgeons all over the world. This is a see one, do one procedure. Every vascular surgeon is welcome to visit our website to see the spiral vein technique and bring it to their patients in need. Feel free to contact us and share your results. Jan Heyligers and Patrick Vriens are consultant vascular surgeons, Department of Vascular Surgery, Elisabeth TweeSteden Hospital, Tilburg, The Netherlands
29


 is a randomised trial designed to assess the performance of the")
30 30 Updates June 2015 Advertorial Fusion Bioline provides significant clinical benefit over standard eptfe femoropopliteal grafts Results from the FINEST randomised trial show that the Fusion Bioline vascular graft yields higher patency rates in lower limb bypasses in comparison with standard eptfe grafts at one year. Follow-up data from the study were published in the Journal of Vascular Surgery and also presented at the Charing Cross Symposium (28 April 1 May, London, UK). US principal investigator Alan B Lumsden, chair, Department of Cardiovascular Surgery, medical director, Methodist DeBakey Heart and Vascular Center, Houston, USA, presented the results on behalf of the FINEST investigators. He explained that FINEST (Comparison of safety and primary patency between Fusion vascular graft with Bioline and Exxcel Soft eptfe) is a randomised trial designed to assess the performance of the Fusion Bioline vascular graft from Maquet. Fusion Bioline graft is a combination of a heparin-coated eptfe graft with a Dacron outer layer glued together with polycarbonate urethane. Lumsden told delegates: Dacron has stood the test of time. It is extremely durable and thrombogenic, and therefore has been used in high flow vessels like the aorta and the iliacs. eptfe is less thrombogenic, dominates the lower prosthetic bypasses market, and has been further enhanced with the addition of heparin bonding on the luminal surface. The Fusion Bioline graft blends all these benefits: it is more thrombogenic, producing haemostasis in the suture line, provides the incorporation that has been demonstrated with Dacron, but using the antithrombogenic surface heparing-coated eptfe. He commented that the advantages of the bioline coating include the fact that heparin is immobilised on to the graft surface through covalent multipoint attachments, providing exceptional stability to the coating which may prolong the graft s performance. Heparin is also tightly bound to the albumin surface, allowing heparin to be flexible and extend into the blood flow to be clinically effective. The bioline coating makes the surface more hydrophilic and homogenous, and, in addition, the albumin reduces fibrinogen and platelet adhesions/aggregation. The technology has successfully been used for over 25 years within cardiopulmonary circuits, Lumsden said. Fusion Bioline The study enrolled 209 patients (25 sites) between May 2010 and June 2012, of which two thirds were enrolled in Europe and one third in the USA. Of the total of 207 patients treated, 203 were included in the efficacy analysis. In total, 103 patients were randomised to Fusion Bioline and 100 to the standard eptfe graft. The FINEST study included patients with claudication, rest pain and superficial ulcers, and the major inclusion criteria were requirement for femoropopliteal above- or below-the-knee bypass, proximal anastomosis on the most distal external iliac artery, common femoral artery or superficial femoral artery, and Rutherford category 1 5. Patients with previous bypass graft in the same limb were excluded from the trial. Patients presented with standard comorbidities, the majority had the proximal anastomosis in the common femoral artery (94% in the standard eptfe group and 96.1% in the Fusion Bioline group), and more than 85% had the distal anastomosis above the knee. Follow-up data from the study showed that Fusion Bioline continued to be superior to the standard eptfe graft at one year. At six months, the primary patency rate was 86.4% with Fusion Bioline vs. 70% with standard eptfe (p=0.006); at 12 months, primary patency was 76.5% for Fusion Bioline vs. 67% for standard eptfe (p=0.050). In terms of adverse events (reinterventions), the trial showed a lower rate (17.1%) with Fusion Bioline vs. 30.7% with the standard eptfe graft (p=0.033). Lumsden highlighted that the use of local haemostatic agent was double in the standard eptfe group (64%) than in the Fusion Bioline group (30.1%, p<0.0001). Time to suture hole haemostasis was shorter in the Fusion Bioline group (3.5 minutes) than in the standard eptfe group (11 minutes, p<0.001), even though the amount of haemostatic agent was higher in the standard eptfe group. He concluded the presentation stating that the FINEST study met its primary endpoint in its FDA IDE analysis that led to the approval of the graft in the USA. The Fusion Bioline heparin-coated vascular graft performs extremely well in femoropopliteal bypass procedures. We have seen that primary patency rates are improved with Fusion Bioline compared with those observed with the standard eptfe graft. Suture hole bleeding is substantially reduced with Fusion Bioline compared to standard eptfe graft. In summary, Fusion Bioline provides significant clinical benefits over standard eptfe femoropopliteal grafts, Lumsden said. Afshin Assadian, Vascular and Endovascular Surgery, Wilhelminenspital Vienna, Austria, an investigator in the FINEST trial, comments: The benefit of Fusion Bioline over standard eptfe in a randomised population is clear and an important piece of evidence. The benefit may be due to heparin, the physical properties of the graft, or a combination of both. The bottom line is that the Fusion Bioline graft performs significantly better than standard eptfe graft. Assadian notes that Fusion Bioline has the benefits of improving haemostasis and promoting tissue in-growth, and has axial compliance for better handling compared with standard eptfe grafts. He adds that the results of the FINEST trial reflect what he has experienced in his clinical practice. Because of the performance of the Fusion Bioline graft, we no longer use standard eptfe grafts, he says. APERTO study of paclitaxel-releasing balloon in haemodialysis access is initiated Cardionovum has announced the initiation of the APERTO study, a multicentre randomised postmarket study designed to compare the company s Aperto paclitaxel-releasing high-pressure shunt dilatation catheter with standard percutaneous transluminal angioplasty (PTA) in patients with stenosis in native haemodialysis fistulae or prosthetic haemodialysis grafts on the arm. The primary objective of this study is to compare the effectiveness of the Aperto dilatation catheter with standard PTA in haemodialysis access stenosis. The study will enrol 150 patients at up to 10 sites in The Netherlands and Belgium and is planned to be completed by May The primary endpoint is to compare the period of adequate functioning of the haemodialysis access, defined according to the NKF-DOQI criteria up to six months after the index procedure. The APERTO study is led by coordinating investigator professor Peter Pattynama, from Groene Hart Ziekenhuis in Gouda, The Netherlands. He commented, As the patency of the shunt is essential for the survival of the patients, Aperto cases the suppression of neo-intimal hyperplasia is the logical way to lower the frequency of the necessary shunt interventions and prolong overall haemodialysis shunt patency. With this study we would like to demonstrate an improvement of the primary patency of the access compared to the conventional PTA. According to Cardionovum, the Aperto catheter is a paclitaxel-releasing high-pressure balloon designed for the treatment of the complex restenotic and scarred haemodialysis shunt tissue. The device adds an antiinflammatory and anti-proliferative therapeutic effect to the conventional, purely mechanical angioplasty procedure.
31
.")

32 June 2015 Non-thermal endovenous technologies have comparable outcomes to those achieved with thermal technologies at one year Non-thermal, non-tumescent technologies to treat varicose veins were shown to have comparable short-term outcomes to those obtained with thermal technologies at the recent Charing Cross Symposium (28 April 1 May, London, UK). There is a vast array of technologies that can be used in the treatment of varicose veins including several thermal and non-thermal technologies. The important thing is not which the most appropriate treatment is, because very good results are achieved by using several of these, but the key is getting the right patients treated, getting the right reimbursement, and that is what we should focus on, the panel noted. The discussion also revealed that the most important long-term endpoints were quality of life coupled with reintervention rates. Further, the treatment of tributaries was highlighted as a way of reducing recurrence after thermal ablations and many experts said that concomitant phlebectomies were the way to improve outcomes for these technologies. While non-thermal technologies often emphasise that tumescent anaesthesia is not a requirement a factor that confers a clear benefit because it is less painful for patients in the short-term some presentations suggested that the outcomes of foam sclerotherapy, a nonthermal technology, can be improved by the addition of tumescence. This provided a contradiction of sorts: while some experts believed that the addition of tumescence to non-thermal technologies bettered outcomes and was justified because patients forget about the pain from tumescent anaesthesia, others noted that they would find the addition of tumescence to a non-thermal technology to be a suboptimal solution. Overall, the presentations provided delegates with the most important developments in both thermal and non-thermal technologies. Thermal techniques: Radiofrequency ablation Olivier Pichot, Grenoble, France, presented five-year data using the ClosureFast (Venefit) 7cm catheter system. Venefit is a sequential procedure with two cycles, at the termination of the greater saphenous vein (GSV). Echoguidance is mandatory at each step of the procedure: vein access, catheterisation, positioning and tumescent anaesthesia. The ClosureFAST study was conducted between April 2006 and March The investigators treated 295 limbs in 225 patients at eight centres in Europe. Most of the patients were females (74.5%) and most of them presented with CEAP clinical class 2 or 3. All veins treated were great saphenous veins. The early results showed technical success in all legs, and immediate vein occlusion was achieved in all patients, except one (99.7%) who presented delayed occlusion detected at three-month follow-up. Vein wall thickening was observed in all patients. At five years, the study was completed with 78.7% of the patients (236 legs in 177 patients), and the investigators observed great saphenous vein occlusion in 91.9% of the patients. In addition, 94.9% of patients were free from reflux. The great saphenous vein diameter, measured 3cm below the saphenous femoral junction, decreased from 5.8mm before treatment to 1.4mm at five years follow-up. In terms of anatomical failure during follow-up, we observed GSV blood flow in 25 patients, and reflux was presented in 15 of them. With regards to CEAP time course, between one year and three years varicose veins reappear and we saw an incidence of more than 30% of patients at five years. At five years, the Venous Clinical Severity Score (VCSS) decreased from 3.9 to 1.3. Complications and side effects were mild. At five years, only one patient presented with residual paraesthesia. We demonstrated the radiofrequency ablation with the Venefit procedure is efficient, safe and increases significantly immediate postoperative comfort for the patients. The five-year follow-up study demonstrates high durability of the once achieved great saphenous vein occlusion, and sustained improvement of clinical symptoms at long-term follow-up, Pichot said. Bipolar radiofrequency ablation Isaac Nyamekye, Worcester, UK, then spoke on the benefits of bipolar radiofrequency technology. During bipolar radiofrequency induced thermotherapy (RFITT, Olympus) the energy is delivered from the Celon Precision generator through the ProCurve applicator with its bipolar tip and there is an isolated segment between the two metallic parts defining the bipolarity. There are no randomised trials comparing the radiofrequency devices currently and we are undertaking such a trial at the moment. The Trial of Radiofrequency Thermo-ablation Treatments of Great Saphenous Varicose Veins is randomising patients to Venefit, RFITT or EVRF. Follow-up is by visual pain scores, duplex Olivier Pichot ultrasound assessment and quality of life questionnaires. The primary outcome is six-month ablation, and patients will be followed up with questionnaires at 12 months and hopefully, beyond, he said. In the absence of randomised data we looked at our results with the three devices in a retrospective study from our prospectively maintained database. Patients were matched for age, sex, vein length and diameter. We found that RFITT (5.4sec/cm) and Venefit (6.7sec/cm) took a significantly shorter time to perform than the monopolar device (9.1sec/cm). RFITT and Venefit also produced 100% truncal ablation at six weeks compared to 90% for the monopolar device. However, at the time the study was being performed it was the original monopolar setup that was being used, without a neutral pad electrode. We have noted that with the addition of the neutral pad electrode the monopolar device is better in terms of efficacy and this is being used in our randomised trial, he explained. Current published evidence comes mainly from series data. Early publications showed that Venefit had ablations from 94% to 97% compared to 89% for RFITT. But in 2013, Braithwaite and his group published a paper showing 92% ablation at six months for the RFITT system. This was for a large selection of operators with varying degrees of experience. In a subgroup in which operators had good experience using RFITT, they showed 98% ablation. We reported our data last year (Newman et al) also showing 98% ablation using the to and fro method. So RFITT can produce effective ablation in experienced hands, Nyamekye concluded. Monopolar radiofrequency the EVRF system Attila Szabo, Budapest, Hungary, reported that the monopolar radiofrequency system, EVRF (F Care Systems), provided high closure rates, and was easy Isaac Nyamekye to use, with the flexible 0.5cm catheter allowing treatment of more complex anatomies. The device is multitalented as we can treat small, medium and large veins with the same device, he noted. EVRF is not only for truncal veins but also for middle-size and large veins. The system has choice of different disposables adjusted to the size of the veins, Szabo explained. According to a study of EVRF for small veins conducted by Jean Marc Chardonneau, the percentage of recovery varies from 70% to 95% depending on the treated site. For mid-size veins, there is a small diameter catheter that can be inserted into the vein to apply local anaesthesia to treat these superficial veins from 1 4mm. It is also possible to treat smaller tributaries with this catheter. In our experience, we have treated 751 patients (73% females) between July 2011 and March Patient characteristics were very similar to those seen in other experiences with endovenous ablation devices. We had a 99% occlusion rate at one month, 97.2% at one year and 96.8% at three years. Patient satisfaction was high, pain scores were low, and quality of life improved after one month and one year, Szabo added. Laser Ian Chetter, Hull, UK, then examined new laser fibre technologies including jacket, tulip and radial fibres to state that the modifications in the fibres had resulted in maintaining efficacy (occlusion rates) and reducing the energy density required. This resulted in reduced bruising and pain, he noted. MOCA comes of age Alun Davies, London, UK, kicked off the section on non-thermal, non-tumescent techniques by making the case for mechanochemical ablation (MOCA) having come of age. MOCA (Clarivein, Vascular Continued on page 34

33


34 34 June 2015 Non-thermal endovenous technologies have comparable outcomes to those achieved with thermal technologies at one year Continued from page 32 Insights) combines mechanical endothelial damage using a rotating wire with the infusion of a liquid sclerosant. Heating of the vein and tumescent anaesthesia are not required and only local anaesthesia is utilised at the insertion site. Davies outlined the ideal endovenous device as one that provides a 100% occlusion rate, 100% patient satisfaction and durable results over a five to 10-year time horizon. By this definition, we do not have the ideal device as yet, he maintained. Davies emphasised that the 2013 UK National Institute for Health and Care Excellence (NICE) guidelines recommended a clear treatment hierarchy of endovenous thermal ablation that was followed by foam, and then followed by surgery. Similar recommendations came from the American Venous Forum with respect to clinical assessment, investigation and treatment hierarchy. In the UK, NICE has MOCA on a special measures, or interim regulatory arrangement before it can go on to become a fully recognised treatment, he said. On the point of tumescent anaesthesia, Davies said: You have inflicted pain on your patients if you have used tumescent anaesthesia. Obviously, the simplest nonthermal non-tumescent technology is foam sclerotherapy. If you make your own foam in the UK, it is inordinately inexpensive. There are also more expensive technologies such as Varithena (BTG), he added. Davies then showed a slide with data showing that the Clarivein device had been used in over 600 limbs and had showed high occlusion rates with no major adverse events. He then alluded to the multicentre, randomised trial comparing mechanochemical to radiofrequency ablation: the Venefit vs. ClariVein for varicose veins (VVCVV) trial. The primary outcome was pain during ablative procedure (but before tributary treatment) and the results showed that maximum pain was significantly less in MOCA compared to radiofrequency early on. By the time you get to six weeks, the quality of life data and occlusion data are the same, he noted. He further outlined that MOCA and glue were showing comparable short-term outcomes to radiofrequency or laser at one year with similar quality of life improvement and over 90% occlusion rates, which is comparable to any thermal techniques. Davies noted that while laser and radiofrequency had a risk of thermal damage to nerves, skin, surrounding tissue and paresthesia, ClariVein and VenaSeal did not. Similarly, ClariVein/VenaSeal do not require multiple injections of tumescent anaesthesia. With regard to anatomical suitability, radiofrequency and laser are for GSV and small saphenous vein (SSV), but are not ideal for SSV due to nerve thermal damage. ClariVein and VenaSeal are suitable for GSV, SSV and small veins down to the ankles. We do not have the ideal device as yet. [ ] None of these have a 100% patient satisfaction, 100% occlusion rate and 100% improvement in quality of life. But yes, MOCA has come of age and is a comparable technology to thermal techniques, Davies concluded. VariClose glue Kursat Bozkurt, Istanbul, Turkey, presented on glue ablation with VariClose (Biolas). He noted that the overall experience in Turkey, from over 200 centres, shows that 8,000 cases have been performed in 14 months and that the initial experience with the technology is good. More long-term data with glue are needed, Bozkurt said. He further added that since the endovenous programme begun in March 2005, there was now full reimbursement for endovenous procedures in the last five years. Bozkurt added that while the results obtained with current thermal techniques are good, the requirement of tumescent anaesthesia results in substantial post-interventional discomfort. Glue is used to treat great saphenous vein insufficiency and small saphenous vein insufficiency. Bozkurt went on to provide the results of the Turkish multicentre study of 181 patients with an average Venous Clinical Severity Score (VCSS) was 4.99±1.15 at baseline. The average length of the treated vein segment was 31.62±6.09cm. The results showed a 100% procedural occlusion rate. At the six-month follow-up, there was no total recanalisation observed. There were, however, five partial recanalisation observed and the total occlusion rate was 97.23%. Further, there was postoperative pain in 11 patients (6.07%) and five patients had phlebitis (2.76%). There was no venous thromboembolism and the average VCSS improved from 4.99±1.15 at baseline to 1.39±0.8 at six months. Citing the advantages of using VariClose, Bozturk noted that it was a continuous procedure with no need for tumescent anaesthesia. Cyanocrylate is easy to use compared to thermal ablation techniques and it eliminates nerve damage caused by thermal ablation. There is no need for the use of compression stockings; there are no skin lesions or burn marks after treatment; no need for operating room conditions and patients can return to work and daily routines immediately, he concluded. VenaSeal closure system Guido Lengfellner, Regensburg, Germany, then reported on the use of cyanoacrylate with the VenaSeal closure System (Medtronic) for the treatment of refluxing great saphenous vein. The system gained the CE mark in 2011 and FDA approval in Lengfellner made the point that typical cyanoacrylate was very brittle and hard after polymerisation. It has a low viscosity that means it moves easily can cause non-target embolisation and is slow to polymerise, he noted. However, VenaSeal is a formulated cyanoacrylate for venous application; it is soft and flexible after polymerisation and has a high viscosity so that it can be well controlled and fast polymerisation (30 seconds) upon contact with blood so there is no risk on non-target embolisation. Alluding to the evidence available to back the use of the system, Lengfellner Alun Davies emphasised the feasibility study that showed a three-year, 94.7% closure rate and the US pivotal, prospective, randomised trial VeClose, that demonstrated the safety and effectiveness of VenaSeal by showing noninferiority at three months to radiofrequency using ClosureFast. The trial demonstrated a 98.9% closure rate at six months. Longfellner also discussed the findings of the European multicentre study escope that set out to evaluate the safety, efficacy of VenaSeal for the treatment of refluxing GSV. The primary endpoint is duplex ultrasound closure without use of sedation, tumescent anaesthesia or compression stockings and the study showed closure rates at six months of 94.3% and at one year of 92.9%. Speaking with regard to his own experience he highlighted that there is great advantage to the absence of tumescence in that the procedure was almost painless, although Some patients had some minor pain in the first days after the intervention. Kursat Bozkurt Foam sclerotherapy Attilio Cavezzi, San Benedetto del Tronto, Italy, presented on ways to improve the outcomes of foam sclerotherapy. Foam sclerotherapy has proved to be effective, especially in terms of quality of life and we are obtaining similar results as with laser and radiofrequency at one and three years, but not with regard to occlusion rates. Since the beginning of our experience, we realised that blood was a problem for foam sclerotherapy. So we started to propose a couple of methods to improve the way we deliver foam and the way foam impacts the vein wall. Cavezzi and colleagues proposed that the usage of a long catheter, ultrasoundguided tumescence infiltration also in foam sclerotherapy and saphenous irrigation prior to foam delivery seem to improve the outcomes. He referred to data from a recent study from his group showing that clinical recurrence after foam sclerotherapy was 6% when no tumescence was used; it was 6% when tumescence was used with visual estimation, but no ultrasound-guidance and was 0% when ultrasound-guided tumescence was used. There was a significantly higher occlusion rate as determined by duplex ultrasound when ultrasound-guided tumescence was used when compared to the group in whom no tumescence was used. Further, there were significantly higher occlusions in the ultrasound-guided tumescence group when compared to the group receiving tumescence under visual estimation. It seems that tumescence works, he said. A combination of catheter foam sclerotherapy of the saphenous trunk including perisaphenous tumescence infiltration and saphenous irrigation, with concomitant phlebectomy of the varicose tributaries was shown to achieve clinical recurrence rates of 0% at one, six, 12 and 18 months. At one and six months, the occlusion rate was 100%. Later at 12 and 18 months, it was 93.6% and 86.6%, respectively. There were four recanalised GSV and two showing reflux after 18 months as determined by duplex ultrasound, Cavezzi said. Foam phlebectomy Michael Cummings, St Louis, USA, spoke about the techniques and outcomes of foam phlebectomy. Synchronised ablation and phlebectomy have been shown to improve early quality of life and have prolonged improvement in clinical status. By far and large, this is preferred by patients, Cummings noted. We see that foam sclerotherapy is fast, safe and effective, and on the downside associated with painful lumps, staining and potential embolic phenomena. On the other hand, ambulatory phlebectomy is safe, effective and has no lumps, but is time consuming, associated with more patient discomfort and is not necessarily appropriate for all veins, Cummings explained. Why not combine both and create a foam phlebectomy? An advantage would be the ability to treat a complete range of varicosities and avoid the limitations of either procedure, with some concern of spillage of foam into the soft tissues. It turns out that there are some unexpected advantages such as better sclerotherapy, potentially safer sclerotherapy, easier phlebectomy and fewer bleeding problems, he said. With foam and tumescence, we get compressed veins, better wall contact and less foam is needed for the procedure and that can be removed after it has time to dwell, Cummings explained. Foam phlebectomy offers better foam sclerotherapy due to better wall contact, use of less foam, removal of foam and needs less microthrobectomy. It also offers a better ambulatory phlebectomy because you can use ultrasound guidance for difficult varicosities, and if you do miss a vein during phlebectomy, it can be treated ultrasoundguided foam sclerotherapy and there is less bleeding, he said.
35 CONTROVERSIES CHALLENGES CONSENSUS VASCULAR & ENDOVASCULAR CHALLENGES Update See you in APRIL 2016 TUESDAY FRIDAY OLYMPIA GRAND LONDON UNITED KINGDOM EDUCATION INNOVATION EVIDENCE Like CX Symposium Follow
 Lugli explained that what is important in IVUS")

36 36 June 2015 IVUS is essential in obstruction treatment According to Marzia Lugli (Modena, Italy) the use of intravascular ultrasound (IVUS) is essential during obstruction treatment in deep veins. During the talk The value of IVUS in planning and deployment of deep venous stents at the Charing Cross Symposium (28 April 1 May, London, UK) Lugli explained that what is important in IVUS examination is that real-time images are provided. She said that the role of deep vein evaluation by IVUS is well known, as well as the role that IVUS plays in vein obstruction treatment, especially in obstruction detection and confirmation, in procedure planning and stent deployment, and in postoperative monitoring of the procedure. Lugli maintained, however, that the role of IVUS in post-thrombotic syndrome detection is probably not essential because in secondary obstruction all the other imaging techniques (ultrasound, venography, magnetic resonance imaging, computed tomography) provide sufficient morphological data to confirm postthrombotic deep vein wall damage. Alternatively, in primary obstruction, IVUS can be considered essential in providing a safe diagnosis and confirmation of stenosis, because sometimes the other imaging procedures seem not able to confirm without any doubt non-thrombotic iliac vein lesions, Lugli clarified. She added that during the procedure of obstruction treatment, IVUS should also be considered essential. It is an important tool that may give us important Marzia Lugli information, for example, about obstruction confirmation. Given that frequently the veins are flattened, IVUS allows us to understand exactly the shape of the vein and allows us to take a morphological degree of the stenosis. It is much better in the vein to rely on the area instead of the diameter and to have the Data must be relevant to facilitate changes in acute deep vein thrombosis treatment At the Charing Cross Symposium 2015, Ander Cohen, St Thomas Hospital, London, UK, stated that venous specialists must establish a valid evidence base to facilitate changes in the management of acute deep vein thrombosis. My conclusions are simple, he told the audience. Collect relevant data outcome and patient related data; collect it religiously regularly and with a format; collect it consistently try and get it at the same times and in the same format; and collect data for a long time. It is all about preparation. Given the lack of consensus on treating acute deep vein thrombosis and post-thrombotic syndrome, conducting relevant clinical research in this area is difficult. Cohen noted that randomised trials are complex in such a fast moving area. The large number of interventions and population differences mean that it is difficult to compare trial data. For this reason, Cohen believes that observational studies are extremely important. He stressed that in designing a trial, researchers must think about how their data can be used and shared. You can look at things such as risk factor adjustment and propensity scores. Some of the ideas that we have had are time to surgery as a variate for outcomes, as people are on the waiting lists for different amounts of time, he said. He suggested that delegates measure the person's time at risk which gives an indication of how long possibility to calculate the real rate of the degree of stenosis, Lugli said. During operative planning, on the other hand, Lugli maintained that it is much more important to understand where the landing zones are and the length of the segment to be stented. Using IVUS at this time of the procedure, Lugli explained, the approximate location of the reference healthy vessel and the landing zone can be verified by passing the lesion completely. We can in fact detect the reference vein area and calculate the stent measurements, obtaining a much more precise procedure, she said. Adding to that, Lugli used the example of nonthrombotic iliac vein lesions, such as in May-Thurner syndrome, where the proximal landing zone is very important, as is the confluence of the iliocaval system. She said that IVUS during stent deployment is essential, as well as the crossing point with the internal and external artery that can sometimes be neglected by the more common procedures. Also, in iliofemoral post-thrombotic syndrome, Lugli said that IVUS can be used to check for residual stenosis which is one of the factors that can limit the successful outcome in the long term. Using IVUS in this situation, we can understand exactly if the extension of the stent has been correct, she explained. Lugli reported that at her centre, based on over 300 cases of endovascular treatment of chronic outflow obstruction, IVUS is routinely applied. The reasons are: we have a precise stenosis location and extension, we have a precise stent sizing and deployment, we have significant reduction of the contrast dye and we have quicker procedures. It is for these reasons that despite the fact that this device is quite expensive, it is an adjunctive cost when compared to the procedures that are performed without IVUS. We therefore at present prefer to apply it routinely, she concluded. it takes them to get better from the time you see them, and you can see the effect of surgery over time. We need the failure rates, intervention rates and long-term follow up. Cohen suggested that, as well as demographic, surgical and follow-up data, surgeons should look at risk factors. He noted that baseline data are vital, and that collection of patient history, using the Villalta scale, quality of life (QOL) measures, and questionnaires such as the Veines QOL, were also important for any data set. He then outlined risk factors, some strongly associated with acute deep vein thrombosis and others less so. Obesity, female gender, age and the presence of varicose veins are risk factors with the strongest association, but Cohen suggested the inclusion of factors that are not strongly associated such as minor injury or previous surgery. From our studies, even factors such as liver disease, diabetes and varicose veins are associated with more ulceration. He stressed that by collecting more data like these, a study becomes more relevant and ultimately more useful. We need to get the right data, collect it religiously, collect data for a long time on all patients and be prepared, said Cohen in closing. I would urge you to work together to develop a common protocol so that data can be used in a useful way. Instead of talking about my experience we should talk about our experience.
37

38 38 Market watch June 2015 Product News Medtronic to develop stent graft for thoracoabdominal aneurysms under patent license agreement with Sanford Health Medtronic announced on 14 April 2015 that it plans to develop a stent graft system for less invasive treatment of thoracoabdominal aortic aneurysms under an exclusive patent license agreement with South Dakota-based Sanford Health. A concept for the novel system, which was described in the November 2014 issue of the Journal of Vascular Surgery, is currently being studied (NCT ) under a physician-sponsored (PS) investigational device exemption (IDE) recently approved by the US Food and Drug Administration (FDA). Sanford Health vascular surgeon Patrick Kelly, the physician sponsor of the PS IDE, developed the concept for the system and has since collaborated with Medtronic to manufacture devices based on the concept. Sanford Health holds the intellectual property covered by the exclusive patent license agreement with Medtronic. Medtronic plans to study the system in collaboration with physicians at several medical centres, including Kelly at Sanford Health, starting in the near future and subsequently to commercialise it after obtaining the required regulatory approvals. David Pearce, president of Sanford Research, believes this type of translational research is important to his organisation s mission. Our culture at Sanford Health and at Sanford Research is one that supports the problemsolving innovation that is needed to bring medical advancements to market and to patients. Dr Kelly s ingenuity is providing a treatment option to patients who may not be eligible for any other approach for repairing their aneurysm, Pearce said. Kelly added: Taking the complex and making it simple has long been our goal for the treatment of thoracoabdominal aneurysms. Working with Medtronic could eventually place our solution in the hands of vascular surgeons around the world to help patients facing a life-threatening condition. We hope that this will have a major impact on the treatment of one of the most challenging disease processes to face our specialty. TAAA stent graft system CE mark for Magellan10F robotic catheter Hansen Medical has announced that the company s Magellan 10F robotic catheter has received the CE mark for use in the peripheral vasculature. Achieving this milestone allows the company to market the Magellan 10F robotic catheter in Europe and other countries that require the CE mark. The Magellan 10F robotic catheter is the latest addition to the family of robotic catheters used with the Magellan robotic system. According to Hansen Medical, the 10F catheter allows for independent, robotic control of the distal tips of two telescoping catheters (an outer guide and an inner leader catheter). The guide catheter has a 10F outer diameter, and features the largest inner lumen (7F) in the Magellan catheter family, which enables delivery of therapeutic devices through the robotic catheter in a broader range of endovascular procedures. The Magellan 10F robotic catheter is an important advance for intravascular robotics and the Magellan robotic system, says Thomas Nolte, director of the Vascular Center at the Heart & Vascular Center in Bad Bevensen, Germany. The larger inner lumen will enable physicians to precisely deliver therapeutic devices through a stable, robotic catheter platform in many more vascular procedures. In particular, many complex endovascular aneurysm repairs and lower extremity arterial revascularisations involve delivery of stents, balloons or other devices requiring a 7F catheter inner lumen. The Magellan robotic system is an advanced technology that drives Magellan robotic catheters and guide wires during endovascular procedures. Magellan is designed to offer procedural predictability, control, and catheter stability to physicians as they navigate through the blood vessels and deliver therapy. Magellan s remote workstation allows physicians to control robotic catheters and guide wires while seated away from the radiation field, potentially reducing physicians radiation exposure and procedural fatigue. Medtronic initiates US launch of HawkOne directional atherectomy system Medtronic has initiated the US launch of the HawkOne directional atherectomy system. The HawkOne system can be used to treat all plaque morphologies in patients with peripheral arterial disease, including patients who have plaque blockages that have become severely calcified. Medtronic says that the HawkOne system enables operators to treat severe calcium more efficiently, and the technology design improves lesion engagement. In benchtop testing, the system was able to treat calcified lesions up to two times more effectively than the TurboHawk device. I use directional atherectomy in my practice because of its ability to achieve luminal gain and restore patency, said Mark Fugate, University Surgical Associates, Chattanooga, USA, who performed the first case in the USA with the HawkOne system. The HawkOne system s improved crossability and efficient calcium cutting will further enable our ability to effectively and efficiently treat practically any patient with peripheral arterial disease. A Medtronic press release states that the HawkOne system s design also streamlines procedural efficiency, with improved crossing and cleaning capabilities. Its lower crossing profile improves sheath deliverability and allows physicians to cross challenging lesions more predictably. The HawkOne system has been enhanced with a preloaded cleaning tool, which improves cleaning time by up to 55% when compared to the TurboHawk high efficiency cutter. In the cath lab, we are always looking for new technologies that effectively treat the disease, while improving efficiency, said Louis Lopez, St Joseph Hospital, Fort Wayne, USA. I was very impressed with the significant improvements of the device s crossing and cleaning capabilities. Medtronic s directional atherectomy portfolio also includes the TurboHawk and SilverHawk systems and is backed by more than 15 peer-reviewed studies. Recently published data from the DEFINITIVE LE study in the Journal of American College of Cardiology, Cardiovascular Interventions demonstrated 95% limb salvage in patients with critical limb ischaemia and 78% overall patency in claudicant patients at 12 months following treatment with directional atherectomy. Nitiloop announces 510(k) clearance for NovaCross microcatheter for support of guidewire access Nitiloop has received FDA clearance for its first product, NovaCross, which is intended to be used in conjunction with a guidewire to access discrete regions of the coronary or peripheral vasculature. NovaCross functions both as a competent supporting microcatheter and as a premium low profile microcatheter on its own. NovaCross gains its supportive characteristic through the use of a unique operator-controlled Nitinol scaffold and an extendable segment, both located at its distal end. In addition to the recent FDA clearance, the company reported successful results from a first in human European multicentre study which looked at NovaCross ability to cross chronic total occlusions (CTO) in the coronary vasculature. The device was successfully used in 22 patients, half of whom had undergone a prior failed CTO attempt. NovaCross enabled crossing of the CTO in its entirety in 82% of cases. At 30 days after the procedure, there were no reports of any major adverse cardiac event. The company is currently conducting a pivotal trial in order to be cleared for a CTO indication in the coronary vasculature. Furthermore, the first patient has been successfully enrolled in the company s first-in-human trial to evaluate the safety and efficacy of NovaCross in the peripheral vasculature, with a focus on below-theknee procedures. Chanan Schneider, chief executive officer of Nitiloop, commented, We are very excited at receiving FDA clearance, which represents an important first milestone for the company. We are encouraged by the positive results from the European multicentre study on NovaCross safety and efficacy in coronary CTOs, and look forward to replicating them in our pivotal study and first in human in the below the knee segment within the coming months.
39



40 Download the vascularnews app vascularnews vascularnews vascularnews BIBAPublishing Sponsored by vascularnews by Sponsored Sponsored by BIBAPublishing BIBAPublishing BIBAPublishing Sponsored by Get vascular news anywhere, anytime! vascularnews The VN app has the latest news from the and endovascular world. vascularnews vascularnews The app also brings opinion articles, videos, profiles and events straight to your iphone, ipad or Android. ipad and iphone FREE DOWNLOAD Visit the Apple App Store, Google play or scan the barcodes using your smartphone, or visit to download the VN app Sponsored by BIBAPublishing


41 June 2015 Market watch 41 Product News FDA grants premarket approval for Enroute transcarotid stent system Silk Road Medical has announced that the company has received premarket approval (PMA) from the FDA for the Enroute transcarotid stent system. The Enroute transcarotid stent is the first carotid stent that is introduced and implanted into the carotid artery through a direct common carotid access point to enable a safe and more direct approach to carotid artery stenting. The Enroute transcarotid stent is indicated for use in high surgical risk patients and is intended to be used in conjunction with Silk Road Medical s Enroute transcarotid neuroprotection system (NPS), which recently received 510(k) clearance by the FDA. Together the Enroute transcarotid NPS and stent system enables a novel hybrid procedure called transcarotid artery revascularisation (TCAR), which combines surgical principles of neuroprotection with a less invasive stenting procedure. The Enroute transcarotid NPS is a first in class system used to directly access the common carotid artery and initiate high rate temporary blood flow reversal to protect the brain from stroke while delivering and implanting the Enroute transcarotid stent. The Enroute transcarotid stent was developed pursuant to a license with Cordis Corporation and leverages the micromesh design and long-term durability of the Cordis Precise carotid stent that was clinically proven in tens of thousands of patients across multiple clinical trials including SAPPHIRE, CASES-PMS and SAPPHIRE Worldwide. The Enroute transcarotid stent has a shorter delivery system optimised for transcarotid access and was recently trialed by leading European physicians. TCAR allows us to avoid potential stroke hazards at the aortic arch while placing a stent under robust flow reversal which simulates the superb neuroprotection of carotid endarterectomy, commented Ralf Kolvenbach, chief of Vascular Surgery at Augusta Hospital, Dusseldorf Catholic Hospital Group, Germany. With the Enroute transcarotid stent we now have a dedicated, ergonomic stent platform for TCAR that combines the control afforded by transcarotid access with the stent s visibility under X-ray, allowing for confident, precise stent placement. The US FDA PMA was based in part on data collected from a subset (52) of 141 high surgical risk patients in the ROADSTER study who were treated with the Cordis Precise PRO RX stent system and the Enroute transcarotid NPS. Technical success was 100% (52/52) and the major adverse event (MAE) rate at 30 days was 1.9% consisting of a single minor stroke, comparable to the overall ROAD- STER results of 3.5% MAE and 1.4% stroke. Enroute EverFlex peripheral stent delivers sustained patency in long, complex lesions The EverFlex self-expanding peripheral stent system from Medtronic has been proven to provide sustained patency in the treatment of long, complex lesions in the superficial femoral and popliteal arteries, according to the three-year results of the DURABILITY II study, which are reported in Catheterization and Cardiovascular Intervention. EverFlex is a nitinol stent system that expands to a predetermined diameter to re-open stenotic regions of the superficial femoral artery and proximal popliteal arteries that supply blood to the legs. Narrowing of these arteries is associated with peripheral arterial disease. DURABILITY II is the first controlled study to focus on treating long, complex lesions, and to specifically test the use of a single nitinol stent in the superficial femoral artery, said Krishna J Rocha-Singh, chief scientific officer, Prairie Heart Institute, Springfield, USA. After 36 months, the durable patency and low fracture rates support the validity of a single stent strategy. DURABILITY II, a prospective, multicentre, nonrandomised, single-arm study, enrolled 287 patients at 44 centres in the USA and Europe. The mean lesion length was 8.9cm and included 48.1% occluded arteries with 43.2% severely calcified lesions. Subjects were followed annually for three years with independent ultrasound core lab adjudicated duplex ultrasound to determine stent patency, radiograms of the stented extremity to assess stent fractures and ankle brachial indices. Duplex ultrasound-assessed patency (PSVR <2.0) rate at three years was 60%; freedom from loss of primary patency was significantly higher for lesions <=8cm at 71%, compared to lesions >8cm at 50.5% (p=0.0001). The three year freedom from target lesion revascularisation was 70%. The three-year stent fracture rate was 0.9%. Gore Excluder iliac branch endoprosthesis registered in Australia and New Zealand The Gore s Excluder iliac branch endoprosthesis, a fully engineered system (Gore designed iliac branch and internal iliac components) intended for endovascular treatment of common iliac artery aneurysms or aortoiliac aneurysms, has been included on the Australian Register of Therapeutic Goods. The first patient procedures in Australia were successfully completed by vascular surgeons Steven Dubenec, head of Department of Vascular Surgery at Royal Prince Alfred Hospital, Sydney, and Jack Loa, at Macquarie University Hospital, Sydney. This new device used in conjunction with Gore Excluder abdominal aortic aneurysm endoprosthesis components to isolate the common iliac artery from systemic blood flow and preserve blood flow in the external iliac and internal iliac arteries is built on Gore s technology platform and designed using the same durable, expanded polytetrafluoroethylene (eptfe) graft. Based on the design of the Excluder device, this system provides a wide treatment range and long-term durability, which is extremely important for optimal clinical success, said Dubenec. The pre-cannulated branch and bi-femoral delivery elements of the Excluder support the ease of use of this device. The system provides a treatment range of mm for the internal iliac arteries, and a treatment range of mm for the external iliac arteries. The delivery profile of the loaded catheter allows the use of a 16F introducer sheath for the iliac branch component, and a 12F flexible, reinforced introducer sheath for the internal iliac component. Cardiovascular Systems receives FDA clearance for new peripheral Diamondback device Cardiovascular Systems has received FDA clearance for the new 4F 1.25 Solid Diamondback 360 peripheral orbital atherectomy system for the treatment of peripheral artery disease. Specifically, the clearance covers the company s 145cm-long: New 1.25mm Diamondback 360 Solid Crown, 4F sheath compatible; and Modified 1.25mm Diamondback 360 Micro Crown, 4F sheath compatible. The Diamondback Peripheral 145cm systems are available in two crown designs, the 1.25mm Solid Crown, and the 1.25mm Micro Crown. Both devices offer a smaller profile and a more flexible shaft for improved ease of use. Cardiovascular Systems new 4F compatible Diamondback devices are redefining interventional vascular medicine, said Cezar Staniloae, NYU Medical Center, USA. The use of smaller access sheaths has been shown to reduce procedure times, enable quicker patient recovery, and result in fewer procedural complications from bleeding, providing additional procedural benefits to patients and physicians in addition to expanding physicians treatment options. According to Cardiovascular Systems, the company believes that millions of patients with peripheral arterial disease may benefit from treatment with orbital atherectomy utilising the Stealth 360 and Diamondback 360 systems, minimally invasive catheter systems. These systems use a diamond-coated crown, attached to an orbiting shaft, which sands away plaque while preserving healthy vessel tissue a critical factor in preventing reoccurrences. Balloon angioplasty and stents have significant shortcomings in treating hard, calcified lesions. The company believes that stents are prone to fractures and high recurrence rates, and treatment of hard, calcified lesions often leads to vessel damage and suboptimal results. Diamondback
42
 graft.")
43 June 2015 Research 43 Clinical News Spiral Flow Spiral Flow arteriovenous graft shows substantial improvement in patency over current standard of care Vascular Flow Technologies has announced the presentation of independent study results demonstrating substantially better primary patency rates for its Spiral Flow arteriovenous graft than for polytetrafluoroethylene (PTFE) graft. The study was presented at the Vascular Access Society meeting (15 18 April, Barcelona, Spain) and showed 18-month primary patency rates of 72% for Spiral Flow arteriovenous graft, compared to 36.7% for PTFE grafts, which are the current standard of care. Investigator Wolfgang Hofmann, of the Department of Vascular Surgery, Feldkirch General Hospital, Austria, who presented his data and analysis commented: The results are more than satisfactory, particularly as the patients receiving Spiral Flow grafts were negatively selected. The study compared primary patency rates for 15 patients receiving Spiral Flow arteriovenous grafts with a consecutive series of 87 patients receiving PTFE grafts. Spiral Flow arteriovenous grafts were only used if, according to pre-operative duplex mapping, patients were not suitable for any type of autologous fistula. Follow-up consisted of duplex mapping every three months, and additional duplex scanning if there was suspicion of impending shunt failure. Of the 15 patients receiving Spiral Flow arteriovenous grafts, there were four shunt occlusions, of which two were managed by thrombectomy. Primary patency at 18 months for Spiral Flow arteriovenous grafts, calculated by Kaplan Meier, was 72%, secondary patency was 85.5%. The study results provide strong support for the premise of Vascular Flow s Spiral Flow technology. Spiral Flow grafts are designed to encourage a spiral laminar flow within the graft, which replicates the natural flow in blood vessels. This reduces turbulence at the distal (venous) end of the graft, so reducing shear stress, endothelial activation and platelet activation that precede thrombus formation at the distal anastomosis. The study used duplex mapping to confirm the presence of spiral flow in the grafts. Hofmann commented: We have long known that prosthetic graft failure is a normal tissue response to an abnormal flow environment. It was particularly gratifying to see that changing the flow pattern at the venous anastomosis improves the patency of the graft. Medtronic starts clinical study of Endurant Evo AAA stent graft system Medtronic has began a clinical study to evaluate the safety and effectiveness of the Endurant Evo abdominal aortic aneurysm (AAA) stent graft system, an investigational medical device designed to expand the applicability of EVAR. Based on the Endurant platform, the Endurant Evo AAA stent graft system features an evolved design that aims to simplify the implant procedure and increase patient customisation options. The study s two principal investigators Gilbert R Upchurch, chief of Vascular and Endovascular Surgery at the University of Virginia in Charlottesville, USA, and Hence Verhagen, chief of Vascular Surgery at Erasmus Medical Center in Rotterdam, The Netherlands collaboratively performed the first implant of the low-profile device at the University of Virginia, USA. They were assisted by Saher Sabri, an assistant professor from University of Virginia s Division of Interventional Radiology. The patient, a 56-year-old man, had an abdominal aortic aneurysm with a 5.05cm diameter. The first clinical use of the Endurant Evo AAA stent graft system went well, said Upchurch, the study s US principal investigator. Insertion and deployment were simple and straightforward. Verhagen, the study s European principal investigator, added: The Endurant Evo AAA stent graft system has a variety of design features that have the potential to make endovascular repair of abdominal aortic aneurysms an option for more patients. That potential is what is most exciting to me about this study. The study will enrol 140 patients with infrarenal abdominal aortic or aortoiliac aneurysms at up to 30 sites in the USA and Europe. All study patients will be treated with the Endurant Evo AAA stent graft system. The study s primary safety endpoint is defined as the proportion of subjects experiencing a major adverse event within 30 days post-implantation; its primary effectiveness endpoint is defined as the proportion of subjects with both technical success at the time of the index procedure and treatment success at 12 months post-implantation. Clinical evidence from the study will be used to seek regulatory approvals required to commercialise the Endurant Evo AAA stent graft system in the USA and other markets around the world. The Endurant Evo AAA stent graft system includes the following design features: A 3F reduction in profile facilitates vascular access In situ sizing with a three-piece system and adjustable limb length simplifies pre-case planning and reduces inventory An enhanced delivery system eliminates the tip-recapture step and incorporates an integrated flush port for contrast injection Smaller leg diameters and helical limb stents expand patient applicability in tight distal aortas and tortuous iliac arteries Multiple aortic body lengths and a larger range of limb lengths and diameters improve patient customisation. As an investigational medical device, the Endurant Evo AAA stent graft system may only be used in the current clinical study, which has been approved by the FDA and similar European regulatory bodies. Intact Vascular s Tack system first-inman results published Intact Vascular has announced the publication of the first clinical experience with supporting preclinical data in the Journal of the American College of Cardiology: Cardiovascular Interventions. The article Early experimental and clinical experience with a focal implant for lower extremity post-angioplasty dissection, reveals the potential of the Tack endovascular system for the repair of arterial dissections following percutaneous transluminal angioplasty. The first-in-human safety and feasibility study with one-year follow up was performed at two sites in Asunción, Paraguay (Santa Clara Hospital and The Italian Hospital). Eleven patients with 15 treated ischaemic limbs were enrolled. The 25 treated lesions covered the thigh to the ankle: eight in the superficial femoral artery, seven in the popliteal artery, and 10 in the tibial artery. Six of the lesions were occlusions and 19 were stenoses. The number of Tacks implanted per patient averaged 3.4. Successful dissection repair was achieved at all the lesion sites with the placement of the Tack implant, as determined by angiography. The key endpoints at 12-month follow up included: 100% repair of dissection flaps 12 month patency rates: 5% for superficial femoral artery and popliteal vessels; 3% for superficial femoral artery, popliteal and tibial vessels; and 0% for only tibial vessels No limb loss No implant migration One target lesion revascularisation and death occurred, not related to the device or procedure. Peter A Schneider, vascular surgeon at Kaiser Hospital in Honolulu, USA, and chief medical officer of Intact Vascular, said, This early clinical experience highlights the potential for a new paradigm in treating peripheral arterial disease that minimises the metal we leave behind, helps heal the trauma associated with angioplasty, and preserves future treatment options for patients. Balloon angioplasty is the most commonly performed peripheral intervention used in peripheral arterial disease. However, suboptimal results frequently occur due to tissue dissection resulting from dilating the artery to restore blood flow. If left untreated, acute or late complications can occur, resulting in re-intervention, tissue loss, or amputation. Stents are currently used to treat dissections; however, stents were not designed to address dissections. Stents involve the implantation of significant amounts of metal, and induce chronic injury and inflammation as a result of applying too much chronic outward force to the vessel wall. Stents permanently alter the structural quality of the artery and limit future treatment options. The Tack endovascular system has been designed to: leave minimal foreign material in the artery, apply a low outward force on the arterial wall and allow spot treatment only where needed. To minimise exchanges and increase procedural efficiency, the Tack endovascular delivery catheter contains multiple self-expanding nitinol Tacks. The system is designed to optimise angioplasty by repairing vessel wall dissections, while allowing the artery to maintain its natural configuration. MicroPort begins Minos abdominal aortic stent graft pre-market study MicroPort Endovascular has announced that 18 patients have now been enrolled in a pre-market clinical study to assess the efficacy and safety of the company s Minos ultra-low profile abdominal aortic stent graft system to treat infrarenal abdominal aortic aneurysms. The pre-market clinical study is a multicentre, open-label, prospective, non-randomised study that will enrol up to 130 abdominal aortic aneurysm patients in 15 centres in China. Up until now, the Minos system has had an especially effective sealing effect, said the study s principal investigator, Weiguo Fu, head of the Department of Endovascular Surgery at Fudan University Zhongshan Hospital in Shanghai, China. Its ultra-low profile design allows physicians to employ this less invasive procedure for many patients, especially those with smaller vasculature who might otherwise be ineligible for endovascular aneurysm repair. The stent graft of the Minos system features laser-cut hooks on the bare stent and strong but flexible limbs achieving a stable and upright position in the aorta, in order to reinforce the lower part of the aorta and to effectively exclude an aneurysm. The system is indicated for endovascular treatment of abdominal aortic aneurysms, with the outer diameter of the integrated delivery system ranging from 14 16F. MicroPort said it believes that the ultra-low profile nature of the Minos system represents an innovation in the field, providing patients and physicians with a less invasive treatment approach and a more durable efficacy for the treatment of abdominal aortic aneurysms.

44


45 June 2015 Companies 45 Industry News Lombard Medical closes US$26m debt facility with Oxford Finance Lombard Medical has entered into a US$26m secured term loan facility with Oxford Finance. Lombard Medical received US$11m in proceeds from the loan at closing on 24 April The company has the option of drawing another US$10m after achieving a specific near-term revenue milestone, with a final US$5m becoming available after reaching an additional revenue target. Simon Hubbert, chief executive officer of Lombard Medical, commented, This facility from Oxford solidifies our balance sheet and significantly extends our cash runway by providing non-dilutive capital to support key growth initiatives necessary for our successful global launch of Aorfix, as well as continued development of other innovative new products. Lombard Medical s Aorfix is an endovascular stent graft with global approvals to treat patients with aortic neck angulations up to 90 degrees. This is often a feature of complex abdominal aortic aneurysm anatomies. Contego Medical closes US$5.6 million in series B funding Contego Medical has announced the completion of a US$5.6 million series B financing round led by Hatteras Venture Partners. The round also included Mountain Group Partners, Lookout Capital and Medical Mutual. Contego Medical s portfolio of angioplasty balloons and stents embodying the Integrated Embolic Protection filter platform represents a breakthrough technology, which we believe will help endovascular interventionalists reduce the risk of stroke and other procedural complications, says Doug Reed, general partner of Hatteras Venture Partners. Doug Reed will be joining Contego Medical as a board member. The company will use the funds to continue to grow its leadership, sales and engineering teams and to develop several new and innovative products with its next-generation Integrated Embolic Protection platform. The Paladin device and other devices under development address a multi-billion dollar market, and have the potential to become standards of care in their respective target treatment areas as the combination devices are designed to simplify procedures, improve outcomes and offer cost-effective solutions. We are excited to partner with Hatteras Venture Partners as we continue to expand and commercialise our portfolio of products, says Ravish Sachar, founder and chief executive officer of Contego Medical. Hatch Medical brokers sale of Novotek abdominal aortic aneurysm stent-graft patent portfolio Hatch Medical has successfully brokered the sale of Novotek Innovation s novel intellectual property portfolio for endovascular repair of abdominal aortic aneurysms. The undisclosed purchase price consisted of a combined cash and stock payment. It has been a pleasure to represent Novotek, a UKbased company, through this transaction. The Novotek platform will help resolve the many critical issues associated with today s endovascular aneurysm repair technologies, stated Steve Hvozda, principal at Hatch Medical. Peter Harris, vascular surgeon and director of Novotek, added, We are pleased to have had the expertise and assistance of Hatch Medical to successfully negotiate a suitable transaction that recognises the potential value of these innovations. Jotec E-xtra Design Engineering reaches 1,600 implants Jotec has announced that more than 1,600 customised implants have now been released and implanted since the company launched the E- xtra Design Engineering in Of these, almost 70% were individual solutions to treat complex thoracoabdominal disease and around 30% for juxtarenal treatment. Most of the implantations were performed in Europe, Canada, Brazil and Russia. In a press release, Jotec stated that, based on its core competences and technologies, the company provides physicians with custom-made endovascular products. This allows treatment of vessel anatomies which cannot be treated by existing standard products. Jotec also said it offers the possibility of patient-specific therapeutic solutions for the aortic arch, thoracoabdominal aorta down to the common iliac arteries. Jotec stated that, starting from the sketch and in close cooperation with the physician-dedicated Jotec product specialists as well as the engineers, sophisticated therapeutic strategies and appropriate implants for the treatment of complex aortic diseases are created. Fenestrations, scallops or multiple branches as well as tapered or reversed tapered designs are possible. Beyond that, the support from Jotec is also guaranteed up to the implantation in the operating theatres. Jotec has set up a workflow to ensure the delivery of the final custom-made product in 18 working days only. This allows prompt treatment of patients which before had to wait several months. More information: www. jotec-extradesign.com
46 46 Congresses June 2015 Calendar of events Vascular News team June SVS Vascular Annual Meeting Chicago, USA McCormick Place West W June SITE International Symposium on Endovascular Therapeutics and Congress of the CELA Society (Endovascular Surgeons for Latin America) Barcelona, Spain Palau de Congressos de Catalunya E secretariat@sitesymposium. org W July BSET British Society of Endovascular Therapy Stratford upon Avon, UK Walton Hall Hotel W July 16th European Venous Forum Annual Meeting St Petersburg, Russia Holiday Inn Moskovskye Vorota E admin@ europeanvenousforum.org W www. europeanvenousforum.org August International Union of Phlebology (UIP) Chapter Meeting: Seoul UIP 2015 Seoul, South Korea E 2015uip@intercom.co.kr W September XXII European Chapter Congress of the International Union of Angiology Budapest, Hungary E secretariat@angiology.org W September International Society for Vascular Surgery Athens, Greece The Athens Hilton Hotel W September DGG Annual Meeting of German Society of Vascular Surgery Münster, Germany Messe und Congress Centrum Halle Münsterland GmbH September ESVS Annual Meeting Porto, Portugal Alfândega Congress Centre E esvs_porto2015@mcigroup.com W September Canadian Society for Vascular Surgery Annual Meeting 2015 Victoria, Canada September Association for Vascular Access Dallas, USA Gaylord Texan W September CIRSE 2015 Lisbon, Portugal E info@cirse.org W September IDEAS Interdisciplinary Endovascular Aortic Symposium Lisbon, Portugal W E info@cirse.org October European Symposium on Vascular Biomaterials ESVB 2015 Strasbourg, France Palais des Congres/PMC W October 6th EVF HOW Krakow, Poland Holiday Inn E admin@ europeanvenousforum.org W www. europeanvenousforum.org October 2015 Chinese Chapter of the International Union of Angiology (CCC-IUA) Beijing, China Beijing Meiquan Gong Hotel E lizhaoxw@sina.com 2 5 November VIVA Vascular Interventional Advances Las Vegas, USA Wynn Las Vegas W November Vascular Society of Great Britain & Ireland Annual Scientific Meeting 2015 Bournemouth, UK E office@vascularsociety.org. uk W November VEITHsymposium New York, USA Hilton New York W November XXXI Congreso Andaluz Sociedad Andaluza de Angiologia y Cirurgia Vascular Seville, Spain W December ASVS 2015 Asian Society for Vascular Surgery Bangkok, Thailand Plaza Athenee, Royal Meridien E asvs2015@gmail.com W January 2016 CACVS Paris, France Marriott Rive Gauche & Conference Centre W January 2016 LINC Leipzig, Germany Trade Fair Leipzig W 31 January 4 February 2016 ISET 2016 International Symposium on Endovascular Therapy Hollywood, USA Diplomat Resort & Spa Hollywood W April 2016 Charing Cross Symposium Vascular & Endovascular Challenges Update London, UK Olympia Grand E info@cxsymposium.com W Editor-in-chief: Roger Greenhalgh Publisher: Roger Greenhalgh Head of Publishing: Marcio Brito Editor: Marcio Brito marcio@bibamedical.com Editorial contribution: Amanda Nieves David Brennan Dawn Powell Urmila Kerslake Design: David Reekie Layout: Tim Parker Advertising: Lauren Isola lauren@bibamedical.com Subscriptions: Sue Couch subscriptions@bibamedical.com Please contact the Vascular News team with news or advertising queries Tel: +44 (0) Published by: BIBA Medical, 526 Fulham Road, Fulham, London, SW6 5NR, UK Tel: +44 (0) Printed by: Buxton Press Reprint requests and all correspondence regarding the newspaper should be addressed to the editor at the above address. BIBA Medical Ltd, 2015 All rights reserved. Write to us! If you have comments on this issue or suggestions for upcoming editions write to marcio@bibamedical.com Sign up for a free subscription Please visit Make sure you get your copy of Vascular News Next issue September 2015
47
48
EndoVascular Aneurysm Sealing (EVAS) with Nellix
 with Nellix") 1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
1 2 EndoVascular Aneurysm Sealing (EVAS) with Nellix Designed to seal entire aneurysm with contained biostable polymer Non-modular design with complete fixation Expands endovascular patient eligibility
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Treatment options of late failures of EVAS. Michel Reijnen Rijnstate Arnhem The Netherlands
 Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment
 Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
Challenges with Complex Anatomies Advancing Care in Endovascular Aortic Treatment Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Aortic Center Maimonides Medical Center Brooklyn,
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE
 MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
MODERN METHODS FOR TREATING ABDOMINAL ANEURYSMS AND THORACIC AORTIC DISEASE AAA FACTS 200,000 New Cases Each Year Ruptured AAA = 15,000 Deaths per Year in U.S. 13th Leading Cause of Death 80% Chance of
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Development of a Branched LSA Endograft & Ascending Aorta Endograft
 Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
Development of a Branched LSA Endograft & Ascending Aorta Endograft Frank R. Arko III, MD Sanger Heart & Vascular Institute Carolinas Medical Center Charlotte, North Carolina, USA Disclosures Proximal
The Auckland Experience with the Nellix EVAS System. Andrew Holden, MBChB, FRANZCR
 The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
Durable outcomes. Proven performance.
 Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
Durable outcomes. Proven performance. GORE EXCLUDER AAA Endoprosthesis GORE EXCLUDER Iliac Branch Endoprosthesis GORE EXCLUDER AAA Endoprosthesis The most-studied* EVAR stent graft designed for durable
RETROGRADE BRANCH. Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery
 RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
RETROGRADE BRANCH Gustavo S. Oderich MD Professor of Surgery Director of Endovascular Therapy Division of Vascular and Endovascular Surgery FACULTY DISCLOSURE Consulting* Cook Medical Inc., WL Gore Research
No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital
 No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital Disclosures Andrew Holden, MBChB, FRANZCR No financial investment to disclose Investigator
No Neck Is Needed! Treat the Aneurysm Instead! Andrew Holden, MD Associate Professor of Radiology Auckland City Hospital Disclosures Andrew Holden, MBChB, FRANZCR No financial investment to disclose Investigator
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES
 CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
CUSTOM-MADE SCALLOPED THORACIC ENDOGRAFTS IN DIFFERENT HOSTILE AORTIC ANATOMIES A SERIES OF THREE CASE REPORTS Joel Sousa Department of Department of Angiology and Vascular Surgery Hospital S. João, Porto,
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients
 ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
ENCORE, a Study to Investigate the Durability of Polymer EVAR with Ovation A Contemporary Review of 1296 Patients The Ovation System is approved to treat infrarenal abdominal aortic aneurysms and is not
THE THE MORE MORE NATURAL APPROACH TO OPTIMAL FIT
 THE THE MORE MORE NATURAL APPROACH Natural Approach TO Optimal Fit TO OPTIMAL FIT Conformability without Compromise THE STANDARD IN Conformability AND Designed for flexibility and conformability in tortuous
THE THE MORE MORE NATURAL APPROACH Natural Approach TO Optimal Fit TO OPTIMAL FIT Conformability without Compromise THE STANDARD IN Conformability AND Designed for flexibility and conformability in tortuous
Title. Different arch branched devices are available, is morphology the. main criteria of choice? Ciro Ferrer, MD
 Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Different arch branched devices are available, is morphology the Title main criteria of choice? Ciro Ferrer, MD Vascular Surgery Unit Sapienza University of Rome Disclosure Speaker name: Ciro Ferrer Proctoring/speaking
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry
 Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
Bilateral use of the Gore IBE device for bilateral CIA aneurysms and a first interim analysis of the prospective Iceberg registry Michel MPJ Reijnen, MD, PhD Department of Vascular Surgery, Rijnstate Hospital
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
FLEXIBLE, BALOON EXPANDABLE
 EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft
 MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
MEDICAL Reimbursement Guide Zenith Fenestrated AAA Endovascular Graft Disclaimer: The information provided herein reflects Cook s understanding of the procedure(s) and/or device(s) from sources that may
Current State of Thoracic Branch Devices and Ongoing Clinical Trials
 Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
Current State of Thoracic Branch Devices and Ongoing Clinical Trials Hiroo Takayama, MD, PhD Associate Professor of Surgery Director of Cardiovascular Institute Co-Director of Aortic Center NY Presbyterian/Columbia
My personal experience with INCRAFT in standard and challenging cases
 My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
My personal experience with INCRAFT in standard and challenging cases G Pratesi, MD Vascular Surgery University of Rome Tor Vergata giovanni.pratesi@uniroma2.it Disclosure Speaker name: Giovanni Pratesi,
EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes?
 D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
D. Böckler Department of Vascular and Endovascular Surgery University Hospital Heidelberg EVAR Revision Setting - How can Heli-FX EndoAnchors improve the outcomes? Disclosures Speaker name: Dittmar Böckler
Durability of The Endurant Stent-Graft through 5 Years
 Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
Durability of The Endurant Stent-Graft through 5 Years Michel S. Makaroun MD Co-Director, UPMC Heart and Vascular Institute Professor and Chair, Division of Vascular Surgery University of Pittsburgh School
EVAS using Nellix in my practice Where are we today?
 EVAS using Nellix in my practice Where are we today? Prof. dr. Michel MPJ Reijnen Department of Vascular Surgery, Rijnstate Hospital Arnhem Faculty of Science and Technology, University of Twente The Netherlands
EVAS using Nellix in my practice Where are we today? Prof. dr. Michel MPJ Reijnen Department of Vascular Surgery, Rijnstate Hospital Arnhem Faculty of Science and Technology, University of Twente The Netherlands
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs
 How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
How to select FEVAR versus EVAR + endoanchors in short-necked AAAs Jean-Paul P.M. de Vries, Richte C.L. Schuurmann St. Antonius Hospital Nieuwegein, The Netherlands 21st Critical Issues Congress Nuernberg,
Hostile Neck During EVAR, The Role Of Endoanchores
 Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Hostile Neck During EVAR, The Role Of Endoanchores Samer Koussayer, MD, FACS, RVT Prof, Al Faisal University Section Head and consultant Vascular & Endovascular Surgery Division King Faisal Specialist
Conflicts of Interest. When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Summary. Infrarenal EVAR for short necks 2y postop
 When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
When and Why Complex EVAR in Tx of juxta/suprarenal AAA? Tim Resch MD Vascular Center Skane University Hospital Conflicts of Interest COOK Medical - Consulting, Speakers Bureau, IP, Research support Medtronic
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany
 Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Type 1a Endoleak in hostile neck anatomies: Endoanchor can fix it! D. Böckler University Hospital Heidelberg, Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts
Co-Conveners: Nadia Wise (Adelaide) and Conor Marron (Adelaide) VASCULAR SOCIETY OF INDIA AND RARE VASCULAR DISORDERS (Combined with: Nursing)
 and Conor Marron (Adelaide) VASCULAR SOCIETY OF INDIA AND RARE VASCULAR DISORDERS (Combined with: Nursing)") VASCULAR Co-Conveners: Nadia Wise (Adelaide) and Conor Marron (Adelaide) SATURDAY 17 AUGUST 8:30am - 10:00am VASCULAR SOCIETY OF INDIA AND RARE VASCULAR DISORDERS (Combined with: Nursing) Carotid body
VASCULAR Co-Conveners: Nadia Wise (Adelaide) and Conor Marron (Adelaide) SATURDAY 17 AUGUST 8:30am - 10:00am VASCULAR SOCIETY OF INDIA AND RARE VASCULAR DISORDERS (Combined with: Nursing) Carotid body
Aortic stents, types, selection, tricks in deployment.
 Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Aortic stents, types, selection, tricks in deployment. Hamdy Soliman.M.D,FSCAI Consultant of Cardiology&Head of Endovascular Unit National Heart Institute Endovascular Treatment of Thoracic Aortic Aneurysms
Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft?
 Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft? Chang Shu, M.D., Ph.D Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS
Aortic Arch pathology options: Open,Hybrid, fenestration, Chimney or branched stent-graft? Chang Shu, M.D., Ph.D Vascular Surgery Center National Center for Cardiovascular Diseases. Fuwai Hospital, CAMS
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Neurological Complications of TEVAR. Frank J Criado, MD. Union Memorial-MedStar Health Baltimore, MD USA
 ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
ISES Online Neurological Complications of Frank J Criado, MD TEVAR Union Memorial-MedStar Health Baltimore, MD USA frank.criado@medstar.net Paraplegia Incidence is 0-4% after surgical Rx of TAAs confined
EVAS Sealing Technology: The new paradigm in AAA therapy
 June 2016 EDUCATIONAL SUPPLEMENT EVAS Sealing Technology: The new paradigm in AAA therapy This educational supplement has been supported by an unrestricted educational grant from Endologix MM1398 Rev 01
June 2016 EDUCATIONAL SUPPLEMENT EVAS Sealing Technology: The new paradigm in AAA therapy This educational supplement has been supported by an unrestricted educational grant from Endologix MM1398 Rev 01
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium. Thomas Zeller, MD
 The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
The Role of Lithotripsy in Solving the Challenges of Vascular Calcium Thomas Zeller, MD 1 1 Disclosure Speaker name: Thomas Zeller... I have the following potential conflicts of interest to report: X X
Indications for use. Contraindications within the United States
 Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Indications for use Indications within the United States The GORE TAG Thoracic Endoprosthesis is intended for endovascular repair of all lesions of the descending thoracic aorta, including: Isolated lesions
Final Results of the Feasibility Study for the Drug-coated Chocolate Touch PTA balloon. (The ENDURE Trial)
") Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Final results of the feasibility study for the drug-coated Chocolate Touch PTA balloon of of femoropopliteal Femoropopliteal lesions lesions: (The ENDURE Trial) Final Results of the Feasibility Study for
Taming The Aorta. David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA
 Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Taming The Aorta David Minion, MD Program Director, Vascular Surgery University of Kentucky Medical Center Lexington, Kentucky, USA Faculty Disclosure Consulting: Endologix, Cook 1 Objectives Review the
Abdominal and thoracic aneurysm repair
 Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Abdominal and thoracic aneurysm repair William A. Gray MD Director, Endovascular Intervention Cardiovascular Research Foundation Columbia University Medical Center Abdominal Aortic Aneurysm Endografts
Percutaneous Approaches to Aortic Disease in 2018
 Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
Percutaneous Approaches to Aortic Disease in 2018 Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network Case 78 year old F Lower CP and upper
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft
 Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft Frank R. Arko III, MD Professor of Cardiovascular Surgery Director, Endovascular Surgery Co-Director, Aortic Institute Carolinas Medical
Early Clinical Results with the Valiant Mona LSA Branch Stent-Graft Frank R. Arko III, MD Professor of Cardiovascular Surgery Director, Endovascular Surgery Co-Director, Aortic Institute Carolinas Medical
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
Exceptions to the Rules: Abdominal and Thoracic Aneurysms
 Exceptions to the Rules: Abdominal and Thoracic Aneurysms Jason Bayne MD, FRCSC Vascular Surgery Jewish General Hospital Assistant Professor, Program Director McGill University Objectives Risk factors
Exceptions to the Rules: Abdominal and Thoracic Aneurysms Jason Bayne MD, FRCSC Vascular Surgery Jewish General Hospital Assistant Professor, Program Director McGill University Objectives Risk factors
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Talent Abdominal Stent Graft
 Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Talent Abdominal with THE Xcelerant Hydro Delivery System Expanding the Indications for EVAR Treat More Patients Short Necks The Talent Abdominal is the only FDA-approved device for proximal aortic neck
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Influence of patient selection and IFU compliance on outcomes following EVAS
 Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
Influence of patient selection and IFU compliance on outcomes following EVAS LUNCH SYMPOSIUM LINC 2017 Jan MM Heyligers, MD, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg,
Optimizing Accuracy of Aortic Stent Grafts in Short Necks
 Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Optimizing Accuracy of Aortic Stent Grafts in Short Necks Venkatesh Ramaiah, MD, FACS Medical Director Arizona Heart Hospital Director Peripheral Vascular and Endovascular Research Arizona Heart Institute
Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry
 University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
University of Milan Thoracic Aortic Research Center Performance of the conformable GORE TAG device in Type B aortic dissection from the GORE GREAT real world registry Santi Trimarchi, MD, PhD Associate
Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan
 The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
The Gore GREAT Registry: Update about a real life data collection Santi Trimarchi, MD, PhD Vascular Surgeon Thoracic Aortic Research Center, Director IRCCS Policlinico San Donato University of Milan Disclosures
COMPLICATIONS OF TEVAR
 COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
COMPLICATIONS OF TEVAR P. Bergeron, A.Petrosyan, F.Markatis, T.Abdulamit, J.-C. Trastour IMAD CONGRESS 2010 Liège Belgium BACKGROUND Stentgrafting is a recognized treatment for TAA & TAD and has been proposed
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
Ovation. Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic
 Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Ovation Sean Lyden, MD Department Chair, Vascular Surgery Cleveland Clinic Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
STROKE PREVENTION IN AORTIC ARCH PROCEDURES
 5 th Aortic Live Symposium STROKE PREVENTION IN AORTIC ARCH PROCEDURES RICHARD GIBBS IMPERIAL VASCULAR UNIT LONDON Disclosure Speaker name:richard Gibbs... I have the following potential conflicts of interest
5 th Aortic Live Symposium STROKE PREVENTION IN AORTIC ARCH PROCEDURES RICHARD GIBBS IMPERIAL VASCULAR UNIT LONDON Disclosure Speaker name:richard Gibbs... I have the following potential conflicts of interest
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
Lessons learned from Ch-EVAR for the treatment of. Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly
 Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad).
.") Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular therapy for Ischemic versus Nonischemic complicated acute type B aortic dissection (catbad). AS. Eleshra, MD 1, T. Kölbel, MD, PhD 1, F. Rohlffs, MD 1, N. Tsilimparis, MD, PhD 1,2 Ahmed Eleshra
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial
 Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
Endovascular Therapy vs. Open Femoral Endarterectomy Rationale and Design of the Randomized PESTO Trial Prof. Thomas Zeller, MD Department Angiology Clinic for Cardiology and Angiology II University Heart-Center
RadRx Your Prescription for Accurate Coding & Reimbursement Copyright All Rights Reserved.
 Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
Interventional Radiology Coding Case Studies Prepared by Stacie L. Buck, RHIA, CCS-P, RCC, CIRCC, AAPC Fellow President & Senior Consultant INDICATION: Abdominal aortic aneurysm. INTERVENTIONAL RADIOLOGIST:
European Experience with a New Thoracic Device. D.Böckler University Hospital Heidelberg Germany
 European Experience with a New Thoracic Device D.Böckler University Hospital Heidelberg Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts of interest to report:
European Experience with a New Thoracic Device D.Böckler University Hospital Heidelberg Germany Disclosures Speaker name: Dittmar Böckler I have the following potential conflicts of interest to report:
Objective assessment of current stent grafts: which graft for which lesion. Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France
 Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
Objective assessment of current stent grafts: which graft for which lesion Ludovic Canaud, MD, PhD Pierre Alric, MD, PhD Montpellier, France Conflict of interest: none 1 Introduction Different diseases
Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU)
") October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
October 6, 2017 Important Update to Field Safety Notice Nellix EndoVascular Aneurysm Sealing System Updated Instructions for Use (IFU) Dear Physician, This notification is to provide you with further information
DISCLOSURES ISOLATED DTA LESION? TYPE B DISSECTIONS TREATMENT OPTIONS
 Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
Endovascular Repair of Aortic Arch Pathologies; What is available/possible in the U.S. in 2018? Kaiser Permanente Endovascular Symposium 6/2/18 Sukgu M Han, MD, MS Assistant Professor of Clinical Surgery
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Is a Stent or Scaffold Necessary in The SFA?
 1 2 3 Is a Stent or Scaffold Necessary in The SFA? Stents were developed to optimize acute results after angioplasty Specifically, stents are universally accepted to manage flow limiting dissections and
1 2 3 Is a Stent or Scaffold Necessary in The SFA? Stents were developed to optimize acute results after angioplasty Specifically, stents are universally accepted to manage flow limiting dissections and
New Data to Shape the Era of Drug Elution in Peripheral Interventions
 New Data to Shape the Era of Drug Elution in Peripheral Interventions William A. Gray MD Director of Endovascular Services Columbia University Medical Center New York Lower Extremity Endovascular - Interventions
New Data to Shape the Era of Drug Elution in Peripheral Interventions William A. Gray MD Director of Endovascular Services Columbia University Medical Center New York Lower Extremity Endovascular - Interventions
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty
 TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
TOBA II 12-Month Results Tack Optimized Balloon Angioplasty William Gray, MD System Chief, Cardiovascular Division Main Line Health, Philadelphia, PA Dissection: The Primary Mechanism of Angioplasty Lesions
Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type 1b Endoleak following an EVAR for Ruptured AAA
 Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Hindawi Case Reports in Vascular Medicine Volume 2017, Article ID 4931282, 5 pages https://doi.org/10.1155/2017/4931282 Case Report Early and Late Endograft Limb Proximal Migration with Resulting Type
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device
 Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Endovascular Repair of Aortic Arch/Thoracic Aneurysms: Bolton RelayBranch Device Luis A. Sanchez MD Gregorio A. Sicard Distinguished Professor of Surgery & Radiology Chief, Section of Vascular Surgery
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA
 Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Which Stent Is Best for Various Femoropopliteal Anatomy? 2018 Pacific Northwest Endovascular Conference June 15-26, 2018 Seattle, WA Brian DeRubertis, MD, FACS Associate Professor of Surgery UCLA Division
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Is EVAS a proper choice in women?
 Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
Is EVAS a proper choice in women? CACVS 2018 Jan MM Heyligers, PhD, FEBVS Consultant Vascular Surgeon Elisabeth TweeSteden Hospital Tilburg The Netherlands Disclosures Consultant for Endologix DEVASS =Dutch
SANGER HEART & VASCULAR INSTITUTE
 VASCULAR SURGERY & MEDICINE PROGRAM GUIDE SANGER HEART & VASCULAR INSTITUTE Vascular Surgery & Medicine Program Guide About Us...1 Vascular Surgery & Medicine...3 Comprehensive Aortic Disease Management...5
VASCULAR SURGERY & MEDICINE PROGRAM GUIDE SANGER HEART & VASCULAR INSTITUTE Vascular Surgery & Medicine Program Guide About Us...1 Vascular Surgery & Medicine...3 Comprehensive Aortic Disease Management...5
I have the following financial relationships to disclose:
 Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
Novel Approaches to Endovascular Management of Aortic Aneurysms Rodney A White, MD Medical Director, Vascular Services MemorialCare Heart & Vascular Institute Long Beach Memorial Hospital Long Beach, California
CAUTION: The Nellix EndoVascular Aneurysm Sealing System is an investigational device. Limited by federal (or United States) law to investigational
 law to investigational") Safety and Effectiveness Results of the Nellix System IDE Pivotal Trial for Endovascular Aneurysm Sealing PRESENTED BY: Jeffrey P. Carpenter, MD National Principal Investigator Professor and Chairman,
Safety and Effectiveness Results of the Nellix System IDE Pivotal Trial for Endovascular Aneurysm Sealing PRESENTED BY: Jeffrey P. Carpenter, MD National Principal Investigator Professor and Chairman,
Klinikum Rosenheim Department of Diagnostic and Interventional Radiology
 Klinikum Rosenheim Department of Diagnostic and Interventional Radiology Is Directional Atherectomy (Silverhawk Or Turbohawk) With DEB, Better Than DEB Alone: Based On The DEFINITIVE AR RCT: 1-Year Results
Klinikum Rosenheim Department of Diagnostic and Interventional Radiology Is Directional Atherectomy (Silverhawk Or Turbohawk) With DEB, Better Than DEB Alone: Based On The DEFINITIVE AR RCT: 1-Year Results
GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 2018 Abstract. Section I GORE TAG Device Clinical experience. Section II Conformable
 GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 08 Abstract This annual clinical update provides a review of the ongoing experience with the GORE TAG Thoracic Endoprosthesis There have
GORE TAG Thoracic Endoprosthesis ANNUAL CLINICAL UPDATE SEPTEMBER 08 Abstract This annual clinical update provides a review of the ongoing experience with the GORE TAG Thoracic Endoprosthesis There have
Endovascular Branched Aortic Arch Repair
 Houston Aortic Symposium 2018 Endovascular Branched Aortic Arch Repair Nimesh D. Desai MD PhD Associate Professor of Surgery, University of Pennsylvania Co-Director, Penn Thoracic Aortic Surgery Program
Houston Aortic Symposium 2018 Endovascular Branched Aortic Arch Repair Nimesh D. Desai MD PhD Associate Professor of Surgery, University of Pennsylvania Co-Director, Penn Thoracic Aortic Surgery Program
Toward Total Endovascular Therapy of the Aorta. Adam W. Beck, MD. Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy
 Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Toward Total Endovascular Therapy of the Aorta Adam W. Beck, MD Associate Professor of Surgery Division of Vascular Surgery and Endovascular Therapy University of Alabama at Birmingham Disclosures Grant
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice
 Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Aortic Neck Issues Associated Clinical Sequelae/Implications for Graft Choice Eric Verhoeven, MD, PhD, A. Katsargyris, MD Department of Vascular and Endovascular Surgery, Paracelsus Medical University,
Improving Endograft Durability with EndoAnchors
 Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Improving Endograft Durability with EndoAnchors William D. Jordan, Jr., M.D. John E. Skandalakis Chair in Surgery Professor and Chief Division of Vascular Surgery and Endovascular Therapy Emory University
Endovascular Ascending Repair: Is This the Next Frontier?
 Endovascular Ascending Repair: Is This the Next Frontier? The 11 th Houston Aortic Symposium Session II: Ascending Aorta/Aortic Dissection (Proximal) February 15, 2018 Michael D. Dake, M.D. Thelma and
Endovascular Ascending Repair: Is This the Next Frontier? The 11 th Houston Aortic Symposium Session II: Ascending Aorta/Aortic Dissection (Proximal) February 15, 2018 Michael D. Dake, M.D. Thelma and
A New EVAR Device for Infrarenal AAAs
 A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
A New EVAR Device for Infrarenal AAAs Peter Nelson, MD, MS Assistant Professor of Surgery MM0203 Rev. 01 Current U.S. EVAR Devices Anatomical Fixation Proximal Fixation Powerlink - Endologix Excluder WL
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System
 Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
Introducing the GORE TAG Conformable Thoracic Stent Graft with ACTIVE CONTROL System K. Oikonomou Department of Vascular Surgery Regensburg University Disclosures W.L. Gore & Associates Sponsored Presentation
14F OD Ovation Abdominal Stent Graft System
 14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
14F OD Ovation Abdominal Stent Graft System 2 Year Results from the European Study Dierk Scheinert, MD Center for Vascular Medicine Angiology and Vascular Surgery Park Hospital Leipzig, Germany Disclosure
Development of Stent Graft. Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection.
 Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Development of Stent Graft Kato et al. Development of an expandable intra-aortic prothesis for experimental aortic dissection. ASAIO J 1993 The New England Journal of Medicine Downloaded from nejm.org
Endo-Bentall: Fact or Fiction?
 Endo-Bentall: Fact or Fiction? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Surgical Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures Bolton Cook Cryolife Edwards Gore
Endo-Bentall: Fact or Fiction? Eric E. Roselli, MD Chief, Adult Cardiac Surgery Surgical Director, Aorta Center Heart and Vascular Institute, Cleveland Clinic Disclosures Bolton Cook Cryolife Edwards Gore
Nellix Endovascular System: Clinical Outcomes and Device Overview
 Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Nellix Endovascular System: Clinical Outcomes and Device Overview Jeffrey P. Carpenter, MD Professor and Chief, Department of Surgery CAUTION: Investigational device. This product is under clinical investigation
Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK
 Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK Disclosure I have the following potential conflicts of interest to report Consultant, proctor and paid speaker for Vascutek UK
Dr Peter Bungay Derbyshire Vascular Services Royal Derby Hospital Derby UK Disclosure I have the following potential conflicts of interest to report Consultant, proctor and paid speaker for Vascutek UK
Ascending Aorta: Is The Endovascular Approach Realistic?
 Ascending Aorta: Is The Endovascular Approach Realistic? Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosures Research-grants, travelling, proctoring speaking-fees,
Ascending Aorta: Is The Endovascular Approach Realistic? Tilo Kölbel, MD, PhD University Heart Center Hamburg University Hospital Eppendorf Disclosures Research-grants, travelling, proctoring speaking-fees,