Transcatheter aortic valve implantation and pre-procedural risk assesment
|
|
|
- Patience Armstrong
- 6 years ago
- Views:
Transcription
1 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France
2 Disclosures Relationship with companies who manufacture products used in the treatment of the subjects under discussion Relationship Manufacturer(s) Speaker's Honoraria Consultant (Advisory Board) Edwards Lifesciences Abbott, Medtronic Saint Jude Medical,Valtech
3 General comments on TAVI Pre-procedural risk assessment and indications for TAVI Pre-procedural risk assessment and feasibility of TAVI Conclusions


4 The Devices for TAVI Medtronic CoreValve TAV Edwards SAPIEN THV CE mark 2007 CE mark 2007 > patients treated
5 Procedural complications in SOURCE XT Events Results (N = 2706) Aborted Procedures - % 0.6 Unable to Cross Native Valve - % 0.04 Conversion to Surgery - % 0.4 Annular Dissection - % 0.4 Coronary Occlusion - % 0.4 SAPIEN-in-SAPIEN (Bailout) - % 1.1 Valve Embolization - % 0.7 Cardiac Tamponade - % 0.5 (Wendler ; EuroPCR 2012)
6 Clinical outcome at 30 Days ADVANCE Transfemoral N=1015 SOURCE Transfemoral N = 1694 SOURCE Transapical N = 906 All-cause Mortality (%) Any Stroke (%) Aortic regurgitation 2/4(%) Myocardial Infarction (%) New Pacemaker (%) Vascular Complication Major (%) Renal Failure with Temporary Dialysis) (%) Major Bleeding (%) (Bauernschmidt ; EuroPCR 2012)
7 Follow-up after TAVI (Webb. Circulation 2009;119; )
 Heart Failure Non Cardiac 88 (49.")
 Myocardial Infarction 6 (13.3%) 21 (23.9%) Renal Failure 11 (12.5%) 18 (39.")
 of non-cardiac cause Other* 8 (17.8%) Stroke 9 (10.2%) (Thomas et al.")
8 Impact of comorbidities on life expectancy Causes of death ALL 179 (30 days to 1 Year) in the Source Registry Cardiac 45 (25.1%) Heart Failure Non Cardiac 88 (49.2%) Pulmonary*** Unknown 46 (25.7%) Sudden Death 1038 patients (TAVI using Sapien valve) 28 (62.2%) Myocardial Infarction 6 (13.3%) 21 (23.9%) Renal Failure 11 (12.5%) 18 (39.1%) Unknown 18 (39.1%) Half of death were Endocarditis 3 (6.7%) Cancer 10 (11.4%) Other 10 (21.7%) of non-cardiac cause Other* 8 (17.8%) Stroke 9 (10.2%) (Thomas et al.circulation 2011;124:425-33) Gastrointestinal 5 (5.6%) Other** 32 (36.4%)


9 Predictors of 1-year death after TAVI Non cardiac Age Logistic EuroSCORE STS Score COPD Chronic Kydney D. Diabetes Prior stroke Carotid stenosis Dyslipidemia HTN Cardiac PHT NYHA Class IV Acute pulm.oedema CAD Severe MR M Valvuloplasty Procedural Moderate/ severe AR Major vascular compl Stroke Kidney injury Experience Transapical
10 General comments on TAVI Pre-procedural risk assessment and indications for TAVI Pre-procedural risk assessment and feasibility of TAVI Conclusions



 With")
11 The «Heart Team» SURGEONS CARDIOLOGISTS Anesthesiologists Other specialists: Geriatricians Treatment of Aortic Stenosis Imaging specialists (Echo, CT, MRI) With expertise in the treatment of valve disease
12 ESC/EACTS Guidelines for the Management of Valvular Heart Disease European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
13 Essential questions in the evaluation of a patient for valvular intervention Is valvular heart disease severe? Does the patient have symptoms? Are symptoms related to valvular disease? What are patient life expectancy and expected quality of life? Do the expected benefits of intervention (versus spontaneous outcome) outweigh its risks? What are the patient's wishes? Are local resources optimal for planned intervention? European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
14 Risk scores in valve surgery Good discrimination (low vs. high risk) C-index But poor calibration (predicted vs. observed risk) Predicted Observed 0 STS Add. Euroscore Log. Euroscore Ambler (Dewey et al. JTCS 2008;135:180-7) (Brown et al. JTCS 2008;136:566-71) Euroscore II Better calibration but no specific data in high-risk patients (Nashef et al. Eur J Cardiothorac Surg 2012;41:734-45)
15 Risk scores in PARTNER Contra indication for surgery (Partner B) 358 patients Logistic Euroscore: 28% STS score: 12% (Leon et al. N Engl J Med 2010;363: ) High-risk for surgery but operable (Partner A) 699 patients Logistic Euroscore: 29% STS score: 12% (Smith et al. N Engl J Med 2011;364: )
16 Risk factors not Captured in the Traditional Risk Scores Liver disease/cirrhosis Porcelain aorta Chest irradiation Chest wall deformities Oxygen dependence Neurocognitive dysfunction Frailty..




17 Subjective assessment of frailty Eye-ball test Severe frailty Frailty Flexibility

18 Objective assessment of frailty Katz Index of Activities of Daily Living How many of these activities do you require help? 1. Bathing 2. Dressing 3. Toileting 4. Transferring 5. Continence 6. Feeding Score 0 or 1 (Dependence vs. Independence) Total score <4: positive for frailty
19 SURTAVI model «Top ten» Risk factors Significant CAD Frailty Left Ventricular dysfunction Neurological dysfunction Pulmonary disease Peripheral vascular disease Renal disease Redo cardiac surgery Pulmonary hypertension Diabetes mellitus (Van Mieghem,EuroIntervention 2012 Online March 2012)
20 SURTAVI model Low risk Intermediate risk High risk 70 yrs, < 2 risk factors 75 yrs, no risk factors 70 yrs, 2 or 3 risk factors 75 yrs, 1 or 2 risk factors 80 yrs, 1 risk factor 70 yrs, > 3 risk factors 75 yrs, > 2 risk factors 80 yrs, > 1 risk factor (Van Mieghem,EuroIntervention 2012 Online March 2012)
21 The Model for the Prediction of the Risk of TAVI Simple score based on a limited number of variables Inclusion of indices of functional and/or cognitive capacities Specific evaluation in valve patients Elaborated from a broad spectrum of operative risks External validation in high- and low-volume centers Updated on a regular basis Consider specific model for high-risk patients (Rosenhek et al. Eur Heart J 2011, e-pub March )

22 Working group recommendations Currently available risk scores should not be used as an isolated decision tool but as part of an integrated approach, which includes complete clinical evaluation, reference to local resources and surgical results, and the preferences of the patient and their family. Risk scores are not a substitute for clinical experience in the management of patients with VHD.
23 ESC/ EACTS Guidelines for the Management of Valvular Heart Disease «In the absence of a perfect quantitative score, the risk assessment should mostly rely on the clinical judgement of the heart team in addition to a combination of scores» European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
24 Indications for transcatheter aortic valve implantation Class Level TAVI should only be undertaken with a multidisciplinary heart team including cardiologists and cardiac surgeons and other specialists if necessary. TAVI should only be performed in hospitals with cardiac surgery on-site. I C I C TAVI is indicated in patients with severe symptomatic AS who are not suitable for AVR as assessed by a heart team and who are likely to gain improvement in their quality of life and to have a life expectancy of more than 1 year after consideration of their comorbidities. TAVI should be considered in high risk patients with severe symptomatic AS who may still be suitable for surgery, but in whom TAVI is favoured by a heart team based on the individual risk profile and anatomic suitability. I IIa B B European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
25 Management of severe aortic stenosis Severe AS Symptoms No Yes LVEF < 50% No Yes Contraindication for AVR No Physically active No Yes Exercice test Symptoms or fall in blood pressure below baseline Yes No High risk for AVR No Yes Yes Short life expectancy No Yes Presence of risk factors and low/intermediate individual surgical risk TAVI Med Rx No Yes AVR Re-evaluate in 6 months AVR or TAVI European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
26 General comments on TAVI Pre-procedural risk assessment and indications for TAVI Pre-procedural risk assessment and feasibility of TAVI Conclusions

27 Contraindications for transcatheteter aortic valve implantation Absolute contraindications Absence of a heart team and no cardiac surgery on the site. Appropriateness of TAVI, as an alternative to AVR, not confirmed by a heart team. Clinical Estimated life expectancy < 1 year. Improvement of quality of life by TAVI unlikely because of comorbidities. Severe primary associated disease of other valves with major contribution to the patient s symptoms that can be treated only by surgery. Anatomical Inadequate annulus size (< 18 mm, > 29 mm). Thrombus in the left ventricle. Active endocarditis. Elevated risk of coronary ostium obstruction (asymmetric valve calcification, short distance between annulus and coronary ostium, small aortic sinuses). Plaques with mobile thrombi in the ascending aorta, or arch. For transfemoral/subclavian approach: inadequate vascular access (vessel size, calcification, tortuosity). Relative contraindications Bicuspid or non-calcified valves. Untreated coronary artery disease requiring revascularization. Haemodynamic instability. LVEF < 20%. For transapical approach: severe pulmonary disease, LV apex not accessible. European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).

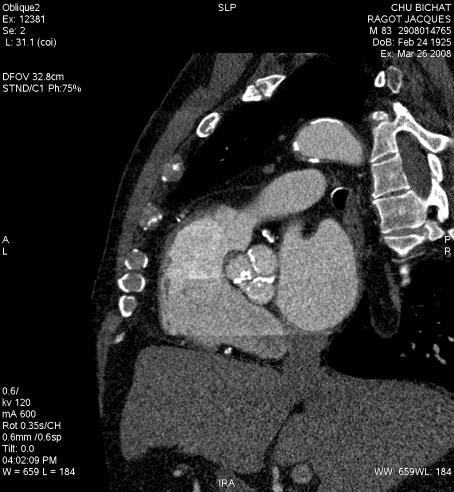

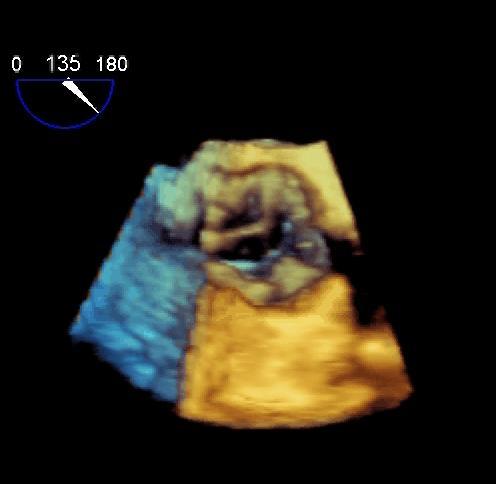
28 Multi-Modality screening of the aortic root before TAVI Echo/CT/MRI? Measurement of aortic annulus Calcium distribution Aortic root
 Operator experience The choice of the type and size of the prosthesis should be multifactorial Coli et and al.")
29 Predictors of aortic regurgitation (Edwards SAPIEN) Detaint et al. JACC Interv 2009;2:82107 Cover Index (TEE) Operator experience The choice of the type and size of the prosthesis should be multifactorial Coli et and al. also take into account other factors such as : Circulation Patient s 2009;120:S982 size and gender, Heigth of coronary ostia, Aortic root calcification Degree of valve calcification (TEE) Asymmetry of valve calcification (TEE) Delgado et al. Circulation 2009;120;S957 Annulus size (MSCT) Degree of valve calcification (MSCT)





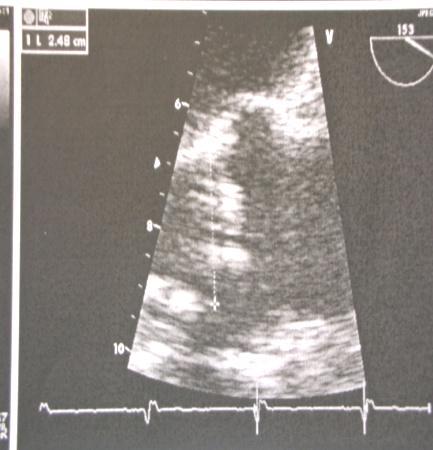
30 Other contraindications LV apical thrombus Contrast echo, MSCT Dynamic subaortic Obstruction Echocardiography Severe organic MR is a contraindication but functional MR is not


 Tortuosity Choice of the")
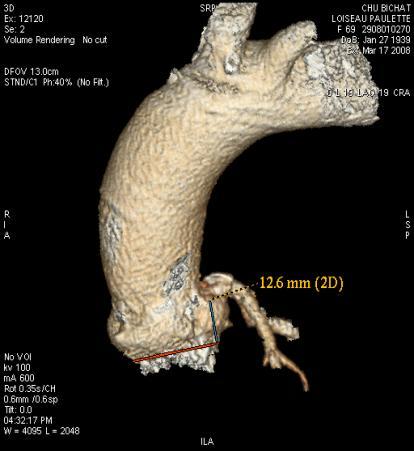
31 Vascular access Conventional angio + MSCT Sagittal + transversal views Judgement based on the combination of : Minimal diameters 18 Fr: 6mm 22 Fr: 7mm 24 Fr: 8mm Calcification (grading) Tortuosity Choice of the approach

32 Coronary artery disease Decision based on Clinical presentation Location of lesions Myocardium at risk Suitability for PCI Options TAVI + medical Rx PCI pre > per TAVI Reconsideration of surgery Give up any intervention
33 Left ventricular dysfunction BAV as a Bridge? TAVI? Cardiac assist for pts in Shock? (Clavel. Circulation 2010;122: )

34 Bicuspid valves Case by case decision annulus: shape/diameter amount/distribution of Ca specific valve design?
35 Conclusions Pre-procedural risk / benefit assessment is crucial in the performance of TAVI A dedicated Heart Team should determine the indications for TAVI and thereafter the feasibility of the procedure All of this relies on a comprehensive evaluation of cardiac and extra-cardiac conditions, combining clinical assessment, multimodality imaging and other investigations if needed Further research is needed on risk stratification models for AVR and TAVI, evaluating mortality and functional results
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Heart Team For TAVI Who and How?
 2 nd TAVI Summit 2012, Seoul Corea Heart Team For TAVI Who and How? Alain Cribier, MD, Charles Nicolle Hospital University of Rouen, France Disclosure Edwards Lifesciences Consultant Training / proctoring
2 nd TAVI Summit 2012, Seoul Corea Heart Team For TAVI Who and How? Alain Cribier, MD, Charles Nicolle Hospital University of Rouen, France Disclosure Edwards Lifesciences Consultant Training / proctoring
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII
 Bichat hospital University Paris VII") When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
Results of Transapical Valves. A.P. Kappetein Dept Cardio-thoracic surgery
 Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
Results of Transapical Valves A.P. Kappetein Dept Cardio-thoracic surgery Rotterda am, The Netherlands 2002 FIM 2003 2005 2006 2010 THV THV Cribier-Edwards Edwards Edwards Sapien Sapien XT Bovine pericardium
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Aortic valve implantation using the femoral and apical access: a single center experience.
 Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Aortic valve implantation using the femoral and apical access: a single center experience. R. Hoffmann, K. Brehmer, R. Koos, R. Autschbach, N. Marx, G. Dohmen Rainer Hoffmann, University Aachen, Germany
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval?
 Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Edwards Transcatheter AVR: Have the Outcomes Changed after CE Approval? Update from PARTNER EU and SOURCE Registries T. Lefèvre Disclosure Statement Cardiologist Interventional cardiologist 1 st PABV in
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI)
") Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Incorporating the intermediate risk in Transcatheter Aortic Valve Implantation (TAVI) Larry S. Dean, MD, MSCAI Past President SCAI Professor of Medicine and Surgery University of Washington School of Medicine
Transcatheter Aortic Valve Implantation. SSVQ November 23, 2012 Centre Mont-Royal 15:40
 Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Transcatheter Aortic Valve Implantation SSVQ November 23, 2012 Centre Mont-Royal 15:40 Nicolo Piazza MD, PhD, FRCPC, FESC, FACC McGill University Health Center German Heart Center Munich 1 First-in-Human
Alec Vahanian,FESC, FRCP (Edin.) Bichat Hospital University Paris VII, Paris, France
 Bichat Hospital University Paris VII, Paris, France") Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Future Percutaneous Therapies for Mitral Valve Disease (Mitraclip,percutaneous annuloplasty and transcatheter valve implantation) Will they reach the TAVI s success? Alec Vahanian,FESC, FRCP (Edin.) Bichat
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
The Role of Imaging in Transcatheter Aortic Valve Implantation
 The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
The Role of Imaging in Transcatheter Aortic Valve Implantation Helmut Baumgartner Westfälische Wilhelms-Universität Münster Division of Adult Congenital and Valvular Heart Disease Department of Cardiovascular
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D.
 Charles T. Klodell, M.D.") Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Valve Replacement without a Scalpel Transcatheter Aortic Valve Replacement (TAVR) Charles T. Klodell, M.D. Professor, Thoracic and Cardiovascular Surgery University of Florida klodell@surgery.ufl.edu Disclosures
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre
 TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
TAVI: The Real Deal? Marc Pelletier, MD Head, Department of Cardiac Surgery New Brunswick Heart Centre Disclosure St. Jude Medical: Consultant and Proctor Edwards Lifesciences: Proctor Medtronic: Research
1-YEAR OUTCOMES FROM JOHN WEBB, MD
 1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
1-YEAR OUTCOMES FROM JOHN WEBB, MD ON BEHALF OF THE SAPIEN 3 INVESTIGATORS UNIVERSITY OF BRITISH COLUMBIA VANCOUVER, CANADA Potential conflicts of interest Speaker's name: John Webb I have the following
Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia
 Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Transcatheter Transapical Aortic Valve Implantation Prince Sultan Cardiac Center Experience Riyadh, Saudi Arabia Ahmed Elwatidy, MD,PhD, FRCS S Kassab, MD,S Ahmari, MD, H Amri, MD, H Ismail, MD, A Calafiori,
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY)
") Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
Peri-operative results and complications in 15,964 transcatheter aortic valve implantations from the German Aortic valve RegistrY (GARY) Thomas Walther, Christian W. Hamm, Gerhard Schuler, Alexander Berkowitsch,
Aortic Valve Stenosis and TAVR: Putting it all together.
 Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Aortic Valve Stenosis and TAVR: Putting it all together. Maria L. Held, MSN CNS Valve Clinic Coordinator at The Cleveland Clinic Alliance of Cardiovascular Professionals April 14 th, 2018 Brief Anatomy
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee
 - 5 important lessons learnt from HK experiences Michael KY Lee") Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
2/28/2010. Speakers s name: Paul Chiam. I have the following potential conflicts of interest to report: NONE. Antegrade transvenous transseptal route
 Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
Transcatheter Aortic Valve Implantation Asian perspective Speakers s name: Paul Chiam Paul TL Chiam MBBS, MRCP, FACC I have the following potential conflicts of interest to report: NONE Consultant National
TAVI: Nouveaux Horizons
 TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI: Nouveaux Horizons EUAPI580i 432HQ14NP02353 Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Objectifs Les recommandations Le TAVI en chiffre La
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital
 TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
TAVI: 10 Years After the First Case Low-Risk and High-Risk Patients What are the Limits? Dr Bernard Prendergast DM FRCP FESC John Radcliffe Hospital Oxford I have financial relationships to disclose Honoraria
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients?
 After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
After PARTNER 2A/S3i and SURTAVI: What is the Role of Surgery in Intermediate-Risk AS Patients? Vinod H. Thourani, MD Professor of Surgery and Medicine Emory University Disclosure Statement of Financial
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Update on Percutaneous Therapies for Structural Heart Disease. William Thomas MD Director of Structural Heart Program Tucson Medical Center
 Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Update on Percutaneous Therapies for Structural Heart Disease William Thomas MD Director of Structural Heart Program Tucson Medical Center NCVH 2014- Tucson Disclosure of Financial Interest Research: Stock
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea
 Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Surgical AVR: Are there any contraindications? Pyowon Park Samsung Medical Center Seoul, Korea Contents Decision making in surgical AVR in old age Clinical results of AVR with tissue valve Impact of 19mm
Prof. Dr. Thomas Walther. TAVI in ascending aorta / aortic root dilatation
 Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
Prof. Dr. Thomas Walther TAVI in ascending aorta / aortic root dilatation nn AorticStenosis - Guidelines TAVI and aortic aneurysm? Few data published. EJCTS 2014;46:228-33 TAVI and aortic aneurysm? Few
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
Transcatheter Aortic Valve Implantation Management of risks and complications
 Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
Transcatheter Aortic Valve Implantation Management of risks and complications TAVI Summit, Seoul, Korea, Spetember 3rd, 2011 Alain Cribier University of Rouen, France Complications of TAVI Depending on
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSAPICAL AORTIC VALVE REPAIR
 TRANSAPICAL AORTIC VALVE REPAIR Mauro ROMANO M.D. Department of Cardio-Vascular Surgery Institut Cardiovasculaire Paris Sud Institut Hospitalier Jacques Cartier MASSY FRANCE romano.mauro@orange.fr Treatment
TRANSAPICAL AORTIC VALVE REPAIR Mauro ROMANO M.D. Department of Cardio-Vascular Surgery Institut Cardiovasculaire Paris Sud Institut Hospitalier Jacques Cartier MASSY FRANCE romano.mauro@orange.fr Treatment
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR
 TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
TAVR in Intermediate Risk Populations /Optimizing Systems for TAVR Saibal Kar, MD, FACC, FAHA, FSCAI Professor of Medicine Director of Interventional Cardiac Research Smidt Heart Institute, Cedars-Sinai
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients?
 Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Is TAVI ready for prime time in: - Intermediate risk patients? - Low risk patients? Didier TCHETCHE, MD. Clinique PASTEUR, Toulouse, France, Conflicts of interest: -Consultant for Edwards LifeSciences
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS
 Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
Establishing the New Standard of Care for Inoperable Aortic Stenosis THE PARTNER TRIAL COHORT B RESULTS E D W A R D S T R A N S C A T H E T E R H E A R T V A L V E P R O G R A M T H E P A R T N E R T R
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Bernard De Bruyne, MD, PhD Cardiovascular Center Aalst OLV-Clinic Aalst, Belgium
 Medium Term Survival and Functional Status in Patients with Severe Aortic Stenosis Treated by Transcatheter Aortic Valvular Implantation in the PARTNER EU Trial Bernard De Bruyne, MD, PhD Cardiovascular
Medium Term Survival and Functional Status in Patients with Severe Aortic Stenosis Treated by Transcatheter Aortic Valvular Implantation in the PARTNER EU Trial Bernard De Bruyne, MD, PhD Cardiovascular
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients:
 Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
Transcatheter Aortic Valve Replacement with a Self-Expanding Prosthesis or Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 1-Year Results from the SURTAVI Clinical Trial Nicolas M. Van
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Appropriate Use of TAVR - now and in the future. A Surgeon s Perspective. Neil Moat Royal Brompton Hospital, London, UK
 Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Appropriate Use of TAVR - now and in the future A Surgeon s Perspective Neil Moat Royal Brompton Hospital, London, UK Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner
Interventional procedures guidance Published: 26 July 2017 nice.org.uk/guidance/ipg586
 Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Transcatheter aortic valve implantation for aortic stenosis Interventional procedures guidance Published: 26 July 17 nice.org.uk/guidance/ipg586 Your responsibility This guidance represents the view of
Transcatheter Aortic Valve Replacement
 Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Transcatheter Aortic Valve Replacement Jesse Jorgensen, MD Medical Director, Cardiac Catheterization Laboratory Greenville Health System Greenville, South Carolina, USA January 30, 2016 Aortic Stenosis
Vinod H. Thourani, MD, FACC, FACS
 Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
Considering SAVR in the TAVR era: Surgical Implications of TAVR Vinod H. Thourani, MD, FACC, FACS Professor of Cardiothoracic Surgery and Medicine Chief of Cardiothoracic Surgery, Emory Hospital Midtown
3 years after introduction of TAVI in QEH. Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong
 3 years after introduction of TAVI in QEH Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong HA Convention 2014 Introduction Aortic Stenosis most common valvular heart disease
3 years after introduction of TAVI in QEH Michael KY Lee On Behalf of QEH TAVI Heart Team Queen Elizabeth Hospital Hong Kong HA Convention 2014 Introduction Aortic Stenosis most common valvular heart disease
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Transcatheter Aortic Valve Implantation (TAVI)
") Transcatheter Aortic Valve Implantation (TAVI) QEH Registry A Multidisciplinary Team Approach Michael KY Lee 1, LK Chan 1, KC Chan 1, KT Chan 1, SF Chui 1, HS Ma 1, CY Wong 1, CS Chiang 1, P Li 1, CB Lam
Transcatheter Aortic Valve Implantation (TAVI) QEH Registry A Multidisciplinary Team Approach Michael KY Lee 1, LK Chan 1, KC Chan 1, KT Chan 1, SF Chui 1, HS Ma 1, CY Wong 1, CS Chiang 1, P Li 1, CB Lam
Transcatheter aortic valve implantation for aortic stenosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Transcatheter aortic valve implantation for aortic stenosis Aortic stenosis occurs when the aortic valve
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Transcatheter aortic valve implantation for aortic stenosis Aortic stenosis occurs when the aortic valve
The Role of TAVI in high-risk and normal-risk Patients
 The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
The Role of TAVI in high-risk and normal-risk Patients Joachim Schofer Hamburg University Cardiovascular Center and Department for percutaneous treatment of structural heart disease Albertinen Heart Center
Dr. Jean-Claude Laborde
 Medtronic CoreValve Experience Alternative Access (Subclavian) and Technology Evolution of the Medtronic CoreValve TAVI System Dr. Jean-Claude Laborde Glenfield Hospital, Leicester, U.K. St George Hospital,
Medtronic CoreValve Experience Alternative Access (Subclavian) and Technology Evolution of the Medtronic CoreValve TAVI System Dr. Jean-Claude Laborde Glenfield Hospital, Leicester, U.K. St George Hospital,
Dr.ssa Loredana Iannetta. Centro Cardiologico Monzino
 Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Dr.ssa Loredana Iannetta Centro Cardiologico Monzino Bicuspid aortic valve BAV is the most common congenital cardiac anomaly. Estimated incidence is 2% in general population. 4:1 male predominance. Frequency
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know?
 Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
Pre-procedural CT angiography for Transcatheter Aortic Valve Implantation: What a Radiologist Needs to Know? E O Dwyer, C O Brien, I Murphy, C Shortt, O Buckley Department of Radiology, AMNCH, Dublin,
TAVI Versus Suturless Valve In Intermediate Risk Patients
 TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy
 TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
TAVR today: High Risk, Intermediate Risk Population, and Valve in Valve Therapy Alan Zajarias, MD FACC Structural Interventional Fellowship Director Associate Professor Medicine Cardiovascular Division
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Transcatheter Aortic Valve Implantation Anaesthetic Prespectives
 Transcatheter Aortic Valve Implantation Anaesthetic Prespectives Dr Simon Chan Consultant Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 11 Oct 2014 Aortic Stenosis Prevalence
Transcatheter Aortic Valve Implantation Anaesthetic Prespectives Dr Simon Chan Consultant Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 11 Oct 2014 Aortic Stenosis Prevalence
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Aortic Stenosis: Open vs TAVR vs Nothing
 Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Aortic Stenosis: Open vs TAVR vs Nothing Wilson Y. Szeto, MD Associate Professor of Surgery Surgical Director, Transcatheter Cardio-Aortic Therapies Associate Director, Thoracic Aortic Surgery Division
Indication, Timing, Assessment and Update on TAVI
 Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Indication, Timing, Assessment and Update on TAVI Swedish Heart and Vascular Institute Ming Zhang MD PhD Interventional Cardiology Structure Heart Disease Conflict of Interest None Starr- Edwards Mechanical
Complications after TAVI: VARC Definitions, Frequency and Management Considerations Patrick W. Serruys, Nicolo Piazza,
 Complications after TAVI: VARC Definitions, Frequency and Management Considerations Patrick W. Serruys, Nicolo Piazza, Nicolas M. Van Mieghem, Yoshinobu Onuma, Martin B. Leon TCT-AP 2011 April 27 th, 2011
Complications after TAVI: VARC Definitions, Frequency and Management Considerations Patrick W. Serruys, Nicolo Piazza, Nicolas M. Van Mieghem, Yoshinobu Onuma, Martin B. Leon TCT-AP 2011 April 27 th, 2011
Transcatheter aortic valve implantation (TAVI): an example of how to organise a TAVI programme
: an example of how to organise a TAVI programme") original article Transcatheter aortic valve implantation (TAVI): an example of how to organise a TAVI programme J M ten Berg R Heijmen As the population ages, aortic valve stenosis becomes more prevalent.
original article Transcatheter aortic valve implantation (TAVI): an example of how to organise a TAVI programme J M ten Berg R Heijmen As the population ages, aortic valve stenosis becomes more prevalent.
Embolic Protection Devices for Transcatheter Aortic Valve Replacement
 Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
Embolic Protection Devices for Transcatheter Aortic Valve Replacement James M. McCabe, MD Medical Director, Cardiac Cath Lab University of Washington Seattle, WA Disclosures Proctoring and honoraria for
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Successful Transfemoral Edwards Sapien Aortic. Valve Implantation in a Patient with Previous. Mitral Valve Replacement
 Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
Advanced Studies in Medical Sciences, Vol. 2, 2014, no. 1, 37-45 HIKARI Ltd, www.m-hikari.com http://dx.doi.org/10.12988/asms.2014.31213 Successful Transfemoral Edwards Sapien Aortic Valve Implantation
Emergency TAVI: Does It Exist? Is the Risk Higher?
 Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
Emergency TAVI: Does It Exist? Is the Risk Higher? Gerald Yong MBBS (Hons) FRACP FSCAI Interventional Cardiologist Royal Perth Hospital Western Australia APCASH 12 October 2014 Disclosure Statement of
When Should We Consider TAVI. (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea
? Pyowon Park Samsung Medical Center Seoul, Korea") When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
When Should We Consider TAVI Procedure in Korea (Surgeon s Viewpoint)? Pyowon Park Samsung Medical Center Seoul, Korea Aortic Stenosis in Korea Rapidly increasing valve disease in Korea Still low incidence
Corrado Tamburino, MD, PhD
 Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Paravalvular leak: acceptable or not Corrado Tamburino, MD, PhD Full Professor of Cardiology, Director of Postgraduate School of Cardiology Chief Cardiovascular Department, Director Cardiology Division,
Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015
 Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015 Disclosures Research grants from: SFC, FFC, FRM, Servier Lectures: Novar,s, Daichii Sankyo Follow-up after TAVI Randomized
Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015 Disclosures Research grants from: SFC, FFC, FRM, Servier Lectures: Novar,s, Daichii Sankyo Follow-up after TAVI Randomized
Percutaneous Management of Severe AS in Octagenarians. Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington
 Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Percutaneous Management of Severe AS in Octagenarians Phillip Matsis FRACP FCSANZ Interventional Cardiologist Wakefield Heart Centre Wellington May 2017 Outline Aetiology of AS Natural History of AS Assessment
Le TAVI pour tout le monde?
 Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Le TAVI pour tout le monde? Thierry Lefèvre Institut Cardiovasculaire Paris Sud, Massy Disclosure Statement of Financial Interest I currently have, or have had over the last two years, an affiliation or
Complicanze durante TAVI. Brambilla Nedy IRCCS Policlinico San Donato
 Complicanze durante TAVI Brambilla Nedy IRCCS Policlinico San Donato 0 2 4 6 9 11 14 16 22 26 31 33 37 43 52 61 69 78 87 93 106 113 121 151 171 186 201 225 267 283 294 311 349 502 515 709 1007 Number of
Complicanze durante TAVI Brambilla Nedy IRCCS Policlinico San Donato 0 2 4 6 9 11 14 16 22 26 31 33 37 43 52 61 69 78 87 93 106 113 121 151 171 186 201 225 267 283 294 311 349 502 515 709 1007 Number of
> 1200 Patients
 > 1200 Patients 2002-2008 2008 Transfemoral (n=628) Transapical (n=457) Antegrade N=59 Retrograde N=569 TRAVERCE n=172 RECAST n = 24 REVIVE II n = 106 REVIVAL II n =40 Early First in Man irevive n = 22
> 1200 Patients 2002-2008 2008 Transfemoral (n=628) Transapical (n=457) Antegrade N=59 Retrograde N=569 TRAVERCE n=172 RECAST n = 24 REVIVE II n = 106 REVIVAL II n =40 Early First in Man irevive n = 22
How to Prevent Thromboembolic Complications in TAVI
 How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
How to Prevent Thromboembolic Complications in TAVI PETER WENAWESER, MD Swiss Cardiovascular Centre, University Hospital, Bern, Switzerland Potential Conflicts of Interest Proctoring and lecture fees from
New York Valves Patient focused evidence-based approach. New York City: 6 December Antonio Colombo
 New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
New York Valves 2018 Patient focused evidence-based approach New York City: 6 December 2018 Antonio Colombo Speaker 7 EMO GVM Centro Cuore Columbus Milan, Italy No conflicts to report Vascular complications
An Update on the Edwards TAVR Results. Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St.
 An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
An Update on the Edwards TAVR Results Zvonimir Krajcer, MD Director, Peripheral Intervention Texas Heart Institute at St. Luke s Hospital Disclosures On the speaker s bureau for Endologix, TriVascular,
Dr Winnie Sze-Wun Chan. Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong
 Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Dr Winnie Sze-Wun Chan Cardiac Team Deputy Team Head Department of Radiology and Imaging Queen Elizabeth Hospital Hong Kong Why? Is CT reliable? How to perform the CT study? How to interpret the CT study?
Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update
 Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update T. Lefèvre Natural History of Aortic Stenosois 100 Latent period Survival (%) 80 60 40 20 Symptoms Average Age Death 0 40 50
Percutaneous Aortic Valve Implantation. Core-Valve and Cribier-Edwards Update T. Lefèvre Natural History of Aortic Stenosois 100 Latent period Survival (%) 80 60 40 20 Symptoms Average Age Death 0 40 50
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital,
 Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Transcatheter aortic valves in aortic regurgitation Gry Dahle Dept of Cardiothoracic- and vascular surgery Rikshospitalet, Oslo University Hospital, Oslo, Norway Aortic regurgitation Prevalence in Framingham
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of Medicine Harvard Medical School
 Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Aortic Stenosis: Current State of Percutaneous Therapies, Emerging Technologies and Future Directions Igor Palacios, MD Director of Interventional Cardiology Massachusetts General Hospital Professor of
Transcatheter Valve Replacement: Current State in 2017
 Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Transcatheter Valve Replacement: Current State in 2017 Marc A. Sintek MD Assistant Professor of Medicine Interventional Cardiology Cardiovascular Division Washington University in St. Louis Missouri ACP
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators